Medical Electronic Prescription for Home Respiratory Care Services (PEM-CRD) at a Portuguese University Tertiary Care Centre (2014–2018): A Case Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Statistical Analysis
2.3. Ethical Approval
3. Results
3.1. Characterization of HRC Users
3.2. Evolution of HRC Users (2014–2018)
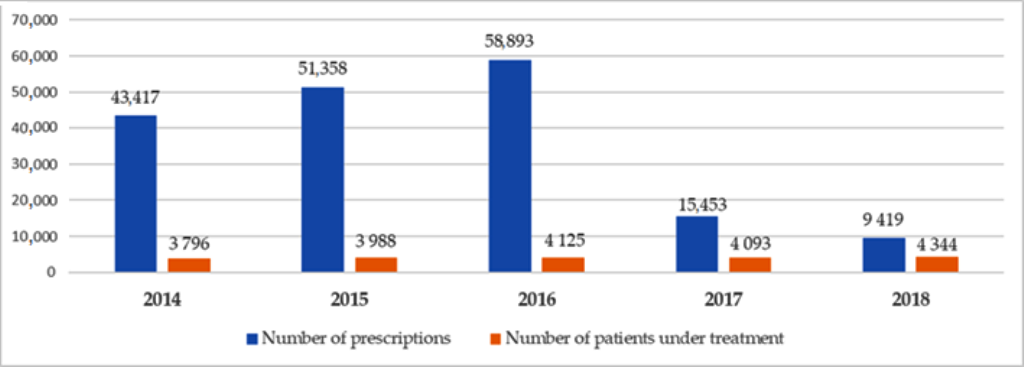
3.3. Evolution of HRC Prescriptions (2014–2018)
3.4. HRC Prescriptions and Users (2014–2018)
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Despacho n.º 9405/2014, de 21 de Julho. Ministério da Saúde-Gabinete do Secretário de Estado da Saúde. Diário da República n.º 138/2014, Série II de 2014-07-21. Available online: https://dre.pt/pesquisa/-/search/55028303/details/normal?p_p_auth=JvT5FiDw (accessed on 12 October 2020).
- Caneiras, C.; Jacome, C.; Mayoralas-Alises, S.; Ramon-Calvo, J.; Fonseca, J.A.; Diaz-Lobato, S.; Escarrabill, J.; Winck, J.C. Patient experience with home respiratory therapies in Portugal: It is time to move forward. Pulmonology 2019, 25, 311–312. [Google Scholar] [CrossRef] [PubMed]
- Adeloye, D.; Chua, S.; Lee, C.; Basquill, C.; Papana, A.; Theodoratou, E.; Nair, H.; Gasevic, D.; Sridhar, D.; Campbell, H.; et al. Global and regional estimates of COPD prevalence: Systematic review and meta-analysis. J. Glob. Health 2015, 5, 020415. [Google Scholar] [CrossRef] [PubMed]
- Wedzicha, J.A.E.C.-C.; Miravitlles, M.; Hurst, J.R.; Calverley, P.M.; Albert, R.K.; Anzueto, A.; Criner, G.J.; Papi, A.; Rabe, K.F.; Rigau, D.; et al. Management of COPD exacerbations: A European Respiratory Society/American Thoracic Society guideline. Eur. Respir. J. 2017, 49, 1600791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antunes, A.F.; Bárbara, C.; Gomes, E.M. Programa Nacional para as doenças respiratórias (2012–2016). Direção Geral da Saúde. 2013. Available online: https://www.dgs.pt/documentos-e-publicacoes/programa-nacional-para-as-doencas-respiratorias-2012-2016-pdf.aspx (accessed on 12 October 2020).
- Bárbara, C.; Jara, E.S. Programa Nacional Para as Doenças Respiratórias-Regras de Prescrição de Cuidados Respiratórios Domiciliários. Direção Geral da Saúde. 2015. Available online: https://comum.rcaap.pt/bitstream/10400.26/15280/1/i022038.pdf (accessed on 12 October 2020).
- Punjabi, N.M. The epidemiology of adult obstructive sleep apnea. Proc. Am. Thorac. Soc. 2008, 5, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Dretzke, J.; Moore, D.; Dave, C.; Mukherjee, R.; Price, M.J.; Bayliss, S.; Wu, X.; Jordan, R.E.; Turner, A.M. The effect of domiciliary noninvasive ventilation on clinical outcomes in stable and recently hospitalized patients with COPD: A systematic review and meta-analysis. Int. J. Chronic Obstruct. Pulm. Dis. 2016, 11, 2269–2286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miravitlles, M.; Vogelmeier, C.; Roche, N.; Halpin, D.; Cardoso, J.; Chuchalin, A.G.; Kankaanranta, H.; Sandstrom, T.; Sliwinski, P.; Zatloukal, J.; et al. A review of national guidelines for management of COPD in Europe. Eur. Respir. J. 2016, 47, 625–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escarrabill, J.; Tebe, C.; Espallargues, M.; Torrente, E.; Tresserras, R.; Argimon, J.; en nombre del equipo del Plan Director de las Enfermedades del Aparato Respiratorio y del Observatorio de Terapias Respiratorias. Variability in home mechanical ventilation prescription. Arch. Bronconeumol. 2015, 51, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Dybwik, K.; Tollali, T.; Nielsen, E.W.; Brinchmann, B.S. Why does the provision of home mechanical ventilation vary so widely? Chronic Respir. Dis. 2010, 7, 67–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Despacho n.º 9483/2014, de 22 de Julho. Ministério da Saúde-Gabinete do Secretário de Estado da Saúde. Diário da República n.º 139/2014, Série II de 2014-07-22. Available online: https://dre.pt/web/guest/pesquisa/-/search/55025906/details/normal?q=Despacho+n.%C2%BA%209483%2F2014 (accessed on 12 October 2020).
- Norma da Direção Geral da Saúde Nº 021/2011, Atualizada a 11/09/2015. Cuidados Respiratórios Domiciliários: Prescrição de Aerossolterapia por Sistemas de Nebulização. Direção-Geral de Saúde. 2015. Available online: https://nocs.pt/aerossolterapia-por-sistemas-de-nebulizacao-domicilio/ (accessed on 12 October 2020).
- Norma da Direção Geral da Saúde Nº 018/2011, Atualizada a 11/09/2015. Cuidados Respiratórios Domiciliários: Prescrição de Oxigenoterapia. Direção-Geral de Saúde. 2015. Available online: https://nocs.pt/oxigenoterapia-domiciliaria/ (accessed on 12 October 2020).
- Norma da Direção Geral da Saúde Nº 022/2011, Atualizada a 11/09/2015. Cuidados Respiratórios Domiciliários: Prescrição de Ventiloterapia e Outros Equipamentos. Direção-Geral de Saúde. Available online: https://nocs.pt/ventiloterapia-domiciliaria/ (accessed on 12 October 2020).
- Meen, T.H.; Matsumoto, Y.; Lee, K.H. Special Issue on Clinical Medicine for Healthcare and Sustainability. J. Clin. Med. 2020, 9, 2206. [Google Scholar] [CrossRef] [PubMed]
- Caneiras, C.; Jacome, C.; Mayoralas-Alises, S.; Ramon Calvo, J.; Almeida Fonseca, J.; Escarrabill, J.; Winck, J.C. Patient Experience in Home Respiratory Therapies: Where We Are and Where to Go. J. Clin. Med. 2019, 8, 555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sousa-Uva, A.; Jara, E.; Castelão, I.; De Almeida, A.B.; Pires Deveza, R.M.M.; Santos, R.; Mariz, S.; Almeida, J.; Moita, J.; Santos, A.C.; et al. Relatório de Situação Cuidados Respiratórios Domiciliários em Portugal. Comissão Nacional Para os Cuidados Respiratórios Domiciliários. 2010. Available online: http://nocs.pt/wp-content/uploads/2016/06/CNCRD_RELATORIO_BOAS_PRATICAS_12_03_2011vfinal.pdf (accessed on 12 October 2020).
- Despacho n.º 9309/2013, de 16 de Julho. Ministério da Saúde-Gabinete do Secretário de Estado da Saúde. Diário da República n.º 135/2013, Série II de 2013-07-16. Available online: https://dre.pt/web/guest/pesquisa/-/search/2783810/details/normal?q=Despacho+n%C2%BA%209309%2F2013+de+16+de+julho (accessed on 12 October 2020).
- Procedimento de Contratação Tendente à Celebração de Acordo Quadro Para a Area da Saúde com Vista à Prestação de Serviços de Cuidados Técnicos Respiratórios Domiciliários. CP 2017/100. Serviços Partillhados do Ministério da Saúde (SPMS). Available online: https://www.catalogo.min-saude.pt/CTAP/downloads/concursos/CE_2017_100_VF.PDF (accessed on 12 October 2020).
- Aldughayfiq, B.; Sampalli, S. Digital Health in Physicians’ and Pharmacists’ Office: A Comparative Study of e-Prescription Systems’ Architecture and Digital Security in Eight Countries. OMICS 2020. [Google Scholar] [CrossRef] [PubMed]
- Bhatta, L.; Leivseth, L.; Mai, X.M.; Henriksen, A.H.; Carslake, D.; Chen, Y.; Langhammer, A.; Brumpton, B.M. GOLD Classifications, COPD Hospitalization, and All-Cause Mortality in Chronic Obstructive Pulmonary Disease: The HUNT Study. Int. J. Chronic Obstruct. Pulm. Dis. 2020, 15, 225–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumeier, A.; Keith, R. Clinical Guideline Highlights for the Hospitalist: The GOLD and NICE Guidelines for the Management of COPD. J. Hosp. Med. 2020, 15, 240–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, P.B.; Rehal, S.; Arbane, G.; Bourke, S.; Calverley, P.M.A.; Crook, A.M.; Dowson, L.; Duffy, N.; Gibson, G.J.; Hughes, P.D.; et al. Effect of Home Noninvasive Ventilation With Oxygen Therapy vs Oxygen Therapy Alone on Hospital Readmission or Death After an Acute COPD Exacerbation: A Randomized Clinical Trial. JAMA 2017, 317, 2177–2186. [Google Scholar] [CrossRef] [PubMed]
- Mayoralas Alises, S.; Caneiras, C.; Diaz-Lobato, S. A telephone-based survey of current trends, habits and beliefs in patients receiving portable oxygen therapy in Madrid, Spain. ERJ Open Res. 2019, 5. [Google Scholar] [CrossRef] [PubMed]
- Lloyd-Owen, S.J.; Donaldson, G.C.; Ambrosino, N.; Escarabill, J.; Farre, R.; Fauroux, B.; Robert, D.; Schoenhofer, B.; Simonds, A.K.; Wedzicha, J.A. Patterns of home mechanical ventilation use in Europe: Results from the Eurovent survey. Eur. Respir. J. 2005, 25, 1025–1031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, G.P.; McArdle, N.; Dhaliwal, S.S.; Douglas, J.; Rea, C.S.; Singh, B. Patterns of use, survival and prognostic factors in patients receiving home mechanical ventilation in Western Australia: A single centre historical cohort study. Chronic Respir. Dis. 2018, 15, 356–364. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Year | 2014 | 2015 | 2016 | 2017 | 2018 | % Variation 2018/2014 | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of patients underHRC treatment 1 | 3796 | 3988 | 4125 | 4093 | 4344 | 14.4% | |||||
| Therapies | |||||||||||
| Nr. of therapies | 4297 | 4514 | 4715 | 4684 | 4952 | 15.2% | |||||
| Type and subtype of therapies 2 | |||||||||||
| Aerosol therapy | 450 | (10.5%) | 289 | (6.4%) | 245 | (5.2%) | 279 | (6.0%) | 194 | (3.9%) | −56.9% |
| Ventilation therapy | 2490 | (57.9%) | 2777 | (61.5%) | 2899 | (61.5%) | 2960 | (63.2%) | 3260 | (65.8%) | 30.9% |
| Oxygen therapy | 1263 | (29.4%) | 1334 | (29.6%) | 1445 | (30.6%) | 1316 | (28.1%) | 1383 | (27.9%) | 9.5% |
| Ventilation adjuvant | 45 | (1.0%) | 77 | (1.7%) | 80 | (1.7%) | 88 | (1.9%) | 66 | (1.3%) | 46.7% |
| Ambulation | 56 | (1.3%) | 183 | (4.1%) | 253 | (5.4%) | 260 | (5.6%) | 319 | (6.4%) | 469.7% |
| Short-term oxygen therapy | 184 | (4.3%) | 112 | (2.5%) | 148 | (3.1%) | 116 | (2.5%) | 110 | (2.2%) | −40.2% |
| Long-term oxygen therapy | 925 | (21.5%) | 929 | (20.6%) | 920 | (19.5%) | 802 | (17.1%) | 844 | (17.0%) | −8.8% |
| Palliative | 53 | (1.2%) | 33 | (0.7%) | 44 | (0.9%) | 50 | (1.1%) | 44 | (0.9%) | −17% |
| Other treatments | 94 | (2.2%) | 114 | (2.5%) | 126 | (2.7%) | 129 | (2.8%) | 115 | (2.3%) | 22.3% |
| Nr. of patients with 1 or more therapies | |||||||||||
| 1 type of therapy | 3508 | (92.4%) | 3682 | (92.3%) | 3813 | (92.4%) | 3771 | (92.1%) | 4026 | (92.7%) | 14.8% |
| 2 types of therapy | 257 | (6.8%) | 283 | (7.1%) | 284 | (6.9%) | 293 | (7.2%) | 288 | (6.6%) | 12.1% |
| 3 types of therapy | 28 | (0.7%) | 22 | (0.6%) | 26 | (0.6%) | 28 | (0.7%) | 27 | (0.6%) | −3.6% |
| 4 types of therapy | 3 | (0.1%) | 1 | (0.0%) | 2 | (0.0%) | 1 | (0.0%) | 3 | (0.1%) | 0.0% |
| Year | 2014 | 2015 | 2016 | 2017 | 2018 | % Variation 2018/2014 |
|---|---|---|---|---|---|---|
| Total of prescriptions | 43,417 | 51,358 | 58,893 | 15,453 | 9419 | −78.3% |
| Treatments: | ||||||
| Aerosol therapy | 4100 (9.4%) | 2245 (4.4%) | 3266 (5.5%) | 1022 (6.6%) | 468 (5.3%) | −88.6% |
| Other treatments | 895 (2.1%) | 1418 (2.8%) | 1418 (2.4%) | 373 (2.4%) | 226 (2.4%) | −74.7% |
| Oxygen therapy | 10,067 (23.2%) | 12,886 (25.1%) | 14,508 (24.6%) | 3539 (22.9%) | 2274 (24.1%) | −77.4% |
| Adjuvant vent. therapy | 393 (0.9%) | 714 (1.4%) | 977 (1.7%) | 252 (1.6%) | 115 (1.2%) | −70.7% |
| Ambulation | 332 (0.8%) | 1596 (3.1%) | 2381 (4.0%) | 651 (4.2%) | 503 (5.3%) | 51.5% |
| Short-term oxygen therapy | 853 (2.0%) | 557 (1.1%) | 781 (1.3%) | 236 (1.5%) | 131 (1.4%) | −84.6% |
| Long-term oxygen therapy | 8284 (19.1%) | 9834 (19.1%) | 10,060 (17.1%) | 2269 (14.7%) | 1404 (14.9%) | −83.1% |
| Palliative | 205 (0.5%) | 185 (0.4%) | 309 (0.5%) | 131 (0.8%) | 121 (1.3%) | −41.0% |
| Ventilation therapy | 28,355 (65.3%) | 34,809 (67.8%) | 39,701 (67.4%) | 10,519 (68.1%) | 6451 (68%) | −77.2% |
| Prescription type: | ||||||
| Initial | 28,172 (64.9%) | 23,912 (46.6%) | 6516 (11.1%) | 2045 (13.2%) | 1585 (16.8%) | −94.4% |
| Renewal | 14,747 (34.0%) | 26,316 (51.2%) | 51,195 (86.9%) | 12,983 (84.0%) | 7302 (77.5%) | −50.5% |
| Modification | 498 (1.1%) | 1130 (2.2%) | 1182 (2.0%) | 425 (2.8%) | 532 (5.6%) | 6.8% |
| Clinical context: | ||||||
| Hospital care | 26,709 (61.5%) | 25,701 (50.0%) | 32,375 (55.0%) | 8277 (53.6%) | 5426 (57.6%) | −79.7% |
| Primary care | 16,708 (38.5%) | 25,657 (50.0%) | 26,518 (45.0%) | 7176 (46.4%) | 3993 (42.4%) | −76.1% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alves, R.; Caneiras, C.; Santos, A.I.; Barbosa, P.; Cardoso, J.; Caseiro, P.; Vitorino, M.J.; Pereira, J.; Escoval, A. Medical Electronic Prescription for Home Respiratory Care Services (PEM-CRD) at a Portuguese University Tertiary Care Centre (2014–2018): A Case Study. Sustainability 2020, 12, 9859. https://0-doi-org.brum.beds.ac.uk/10.3390/su12239859
Alves R, Caneiras C, Santos AI, Barbosa P, Cardoso J, Caseiro P, Vitorino MJ, Pereira J, Escoval A. Medical Electronic Prescription for Home Respiratory Care Services (PEM-CRD) at a Portuguese University Tertiary Care Centre (2014–2018): A Case Study. Sustainability. 2020; 12(23):9859. https://0-doi-org.brum.beds.ac.uk/10.3390/su12239859
Chicago/Turabian StyleAlves, Ricardo, Cátia Caneiras, Ana Isabel Santos, Patricia Barbosa, João Cardoso, Paulo Caseiro, Maria João Vitorino, João Pereira, and Ana Escoval. 2020. "Medical Electronic Prescription for Home Respiratory Care Services (PEM-CRD) at a Portuguese University Tertiary Care Centre (2014–2018): A Case Study" Sustainability 12, no. 23: 9859. https://0-doi-org.brum.beds.ac.uk/10.3390/su12239859