
Linking Lean Adoption and Implementation in Healthcare to National Cultures

 , , and
, , and
Abstract
:1. Introduction
- RQ1: Is the adoption level of Lean in healthcare similar in Finland and Mexico?
- RQ2: What are the similarities and differences between the introduction of Lean healthcare in Finland and Mexico?
- RQ3: What are the similarities and differences between the levels of integration of Lean healthcare in Finland and Mexico?
- RQ4: What are the similarities and differences between the benefits of Lean healthcare in Finland and Mexico?
- RQ5: What are the similarities and differences between the factors enabling and preventing successful Lean implementations in healthcare in Finland and Mexico?
2. Literature Review
2.1. Lean Healthcare in Scandinavian and Latin American Countries
2.2. Finnish and Mexican Cultures
2.3. Lean and National Cultures
3. Materials and Methods
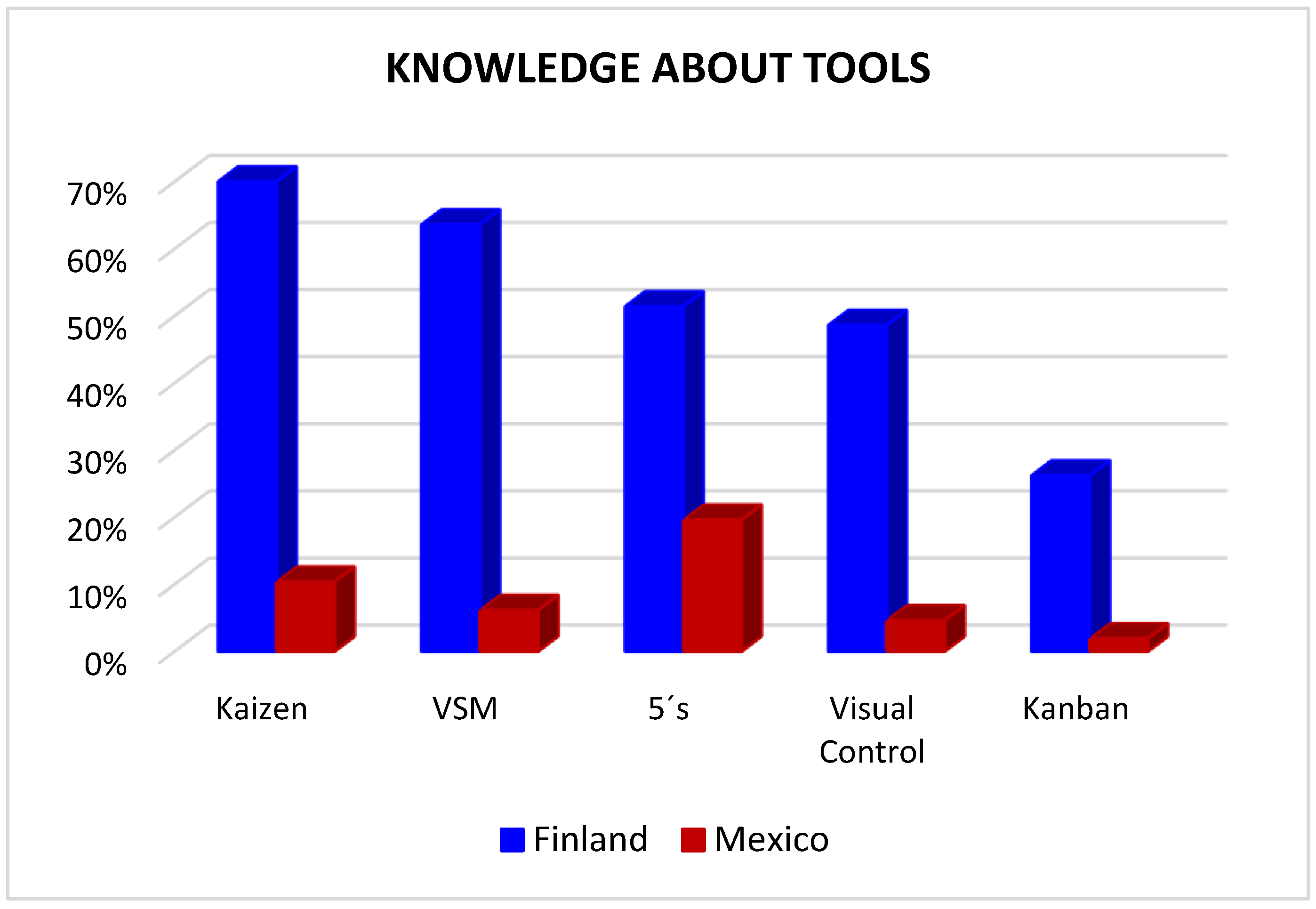
- RQ1 focuses on the level of Lean adoption in healthcare, and it includes questions: (1) ongoing Lean projects, (4) familiarity with Lean tools, and (5) areas with the largest impact.
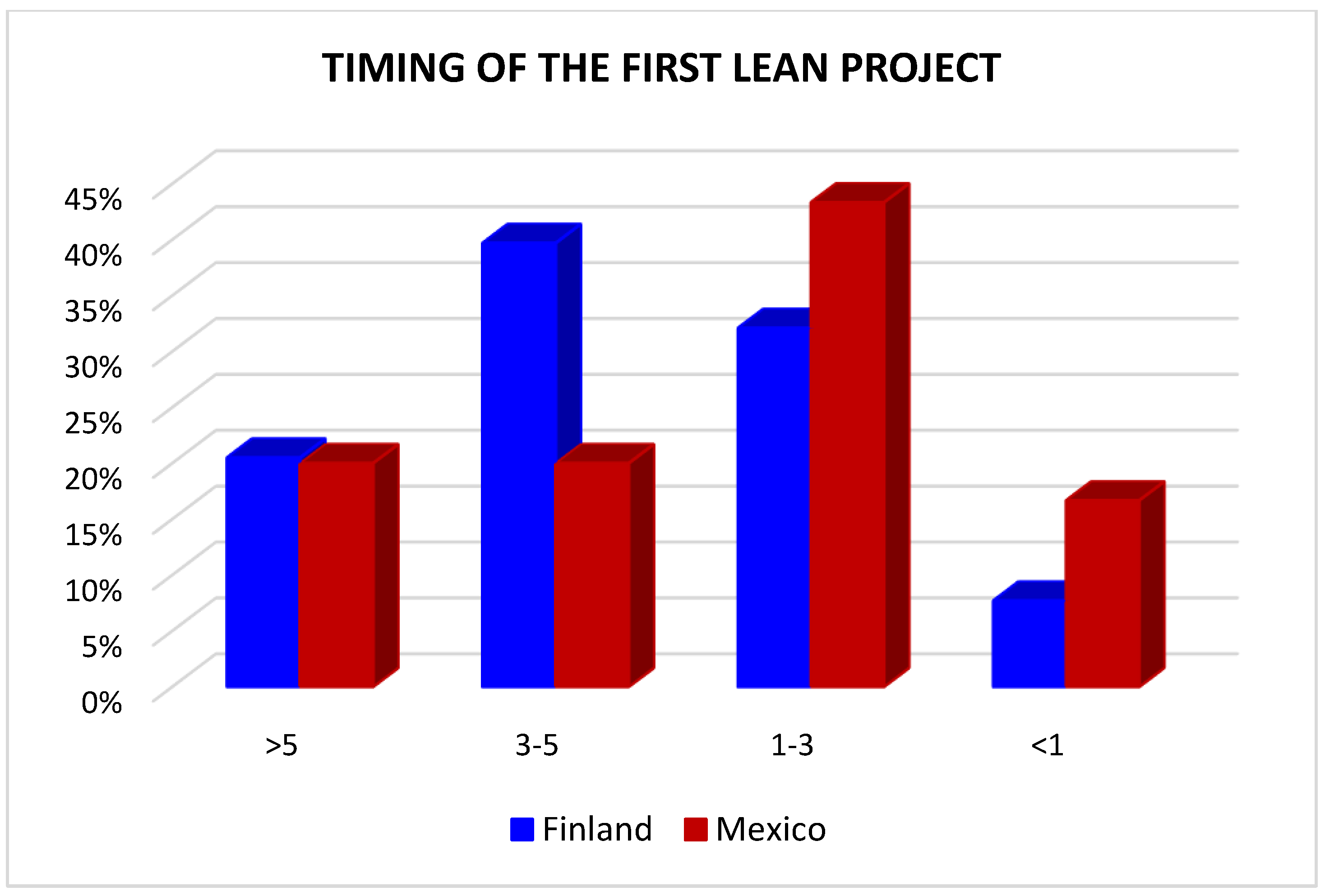
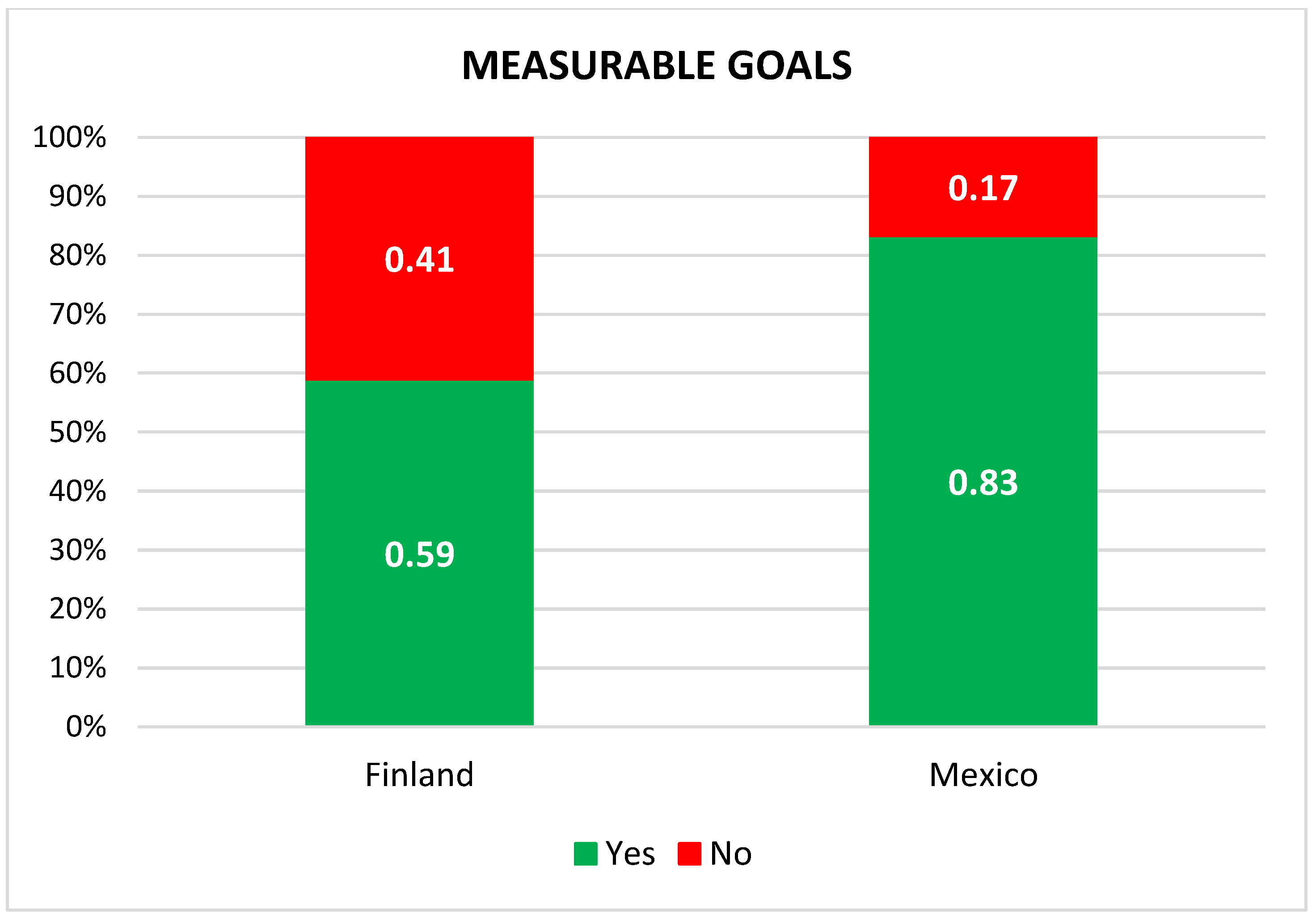
- RQ2 focuses on how Lean was introduced, and it includes questions: (6) timing of the first project, (7) initial reason for Lean, (8) who introduced Lean, and (16) definition of measurable goals.
- RQ3 focuses on how Lean is carried out and integrated, and it includes questions: (9) internal Lean expert and (10) his background, (11) number of Lean projects, (12) current the level of integration of Lean in the system, and (13) what tools are being used.
- RQ4 focuses on the benefits brought by implementing Lean, and it includes questions: (14) economic investment in Lean, (15) economic savings, (17) level of achievement, (18) success of Lean, and (19) main benefits. Note: although question 14 does not focus on benefits, it is relevant to assess the impact of question 15.
- RQ5 focuses on enabling factors and barriers for Lean, and it includes questions: (20) enabling factors, (21) disabling factors, (22) least supportive groups, and (23) reasons of resistance.
4. Results
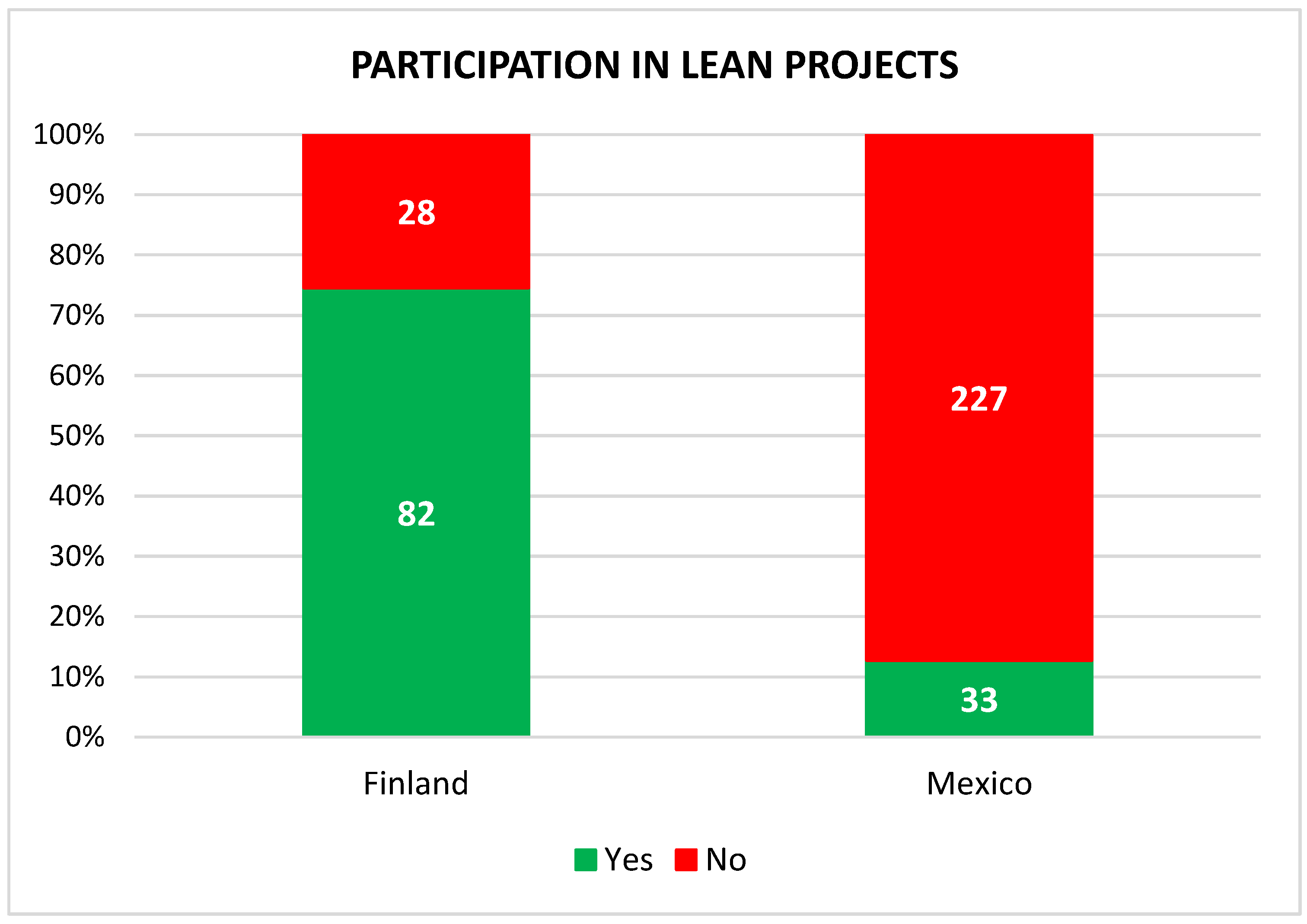
4.1. All Respondents
4.2. Participating Respondents
4.2.1. Starting the Initiative
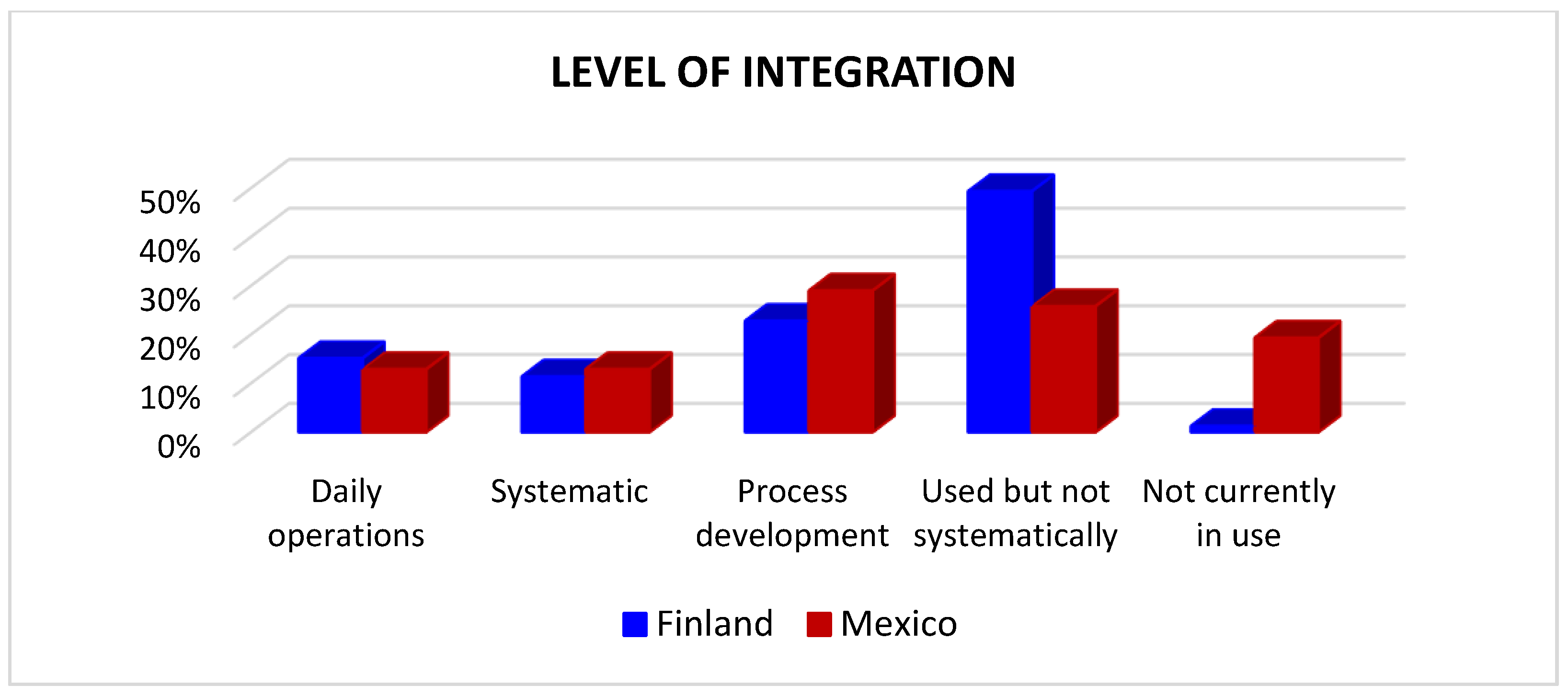
4.2.2. Integration
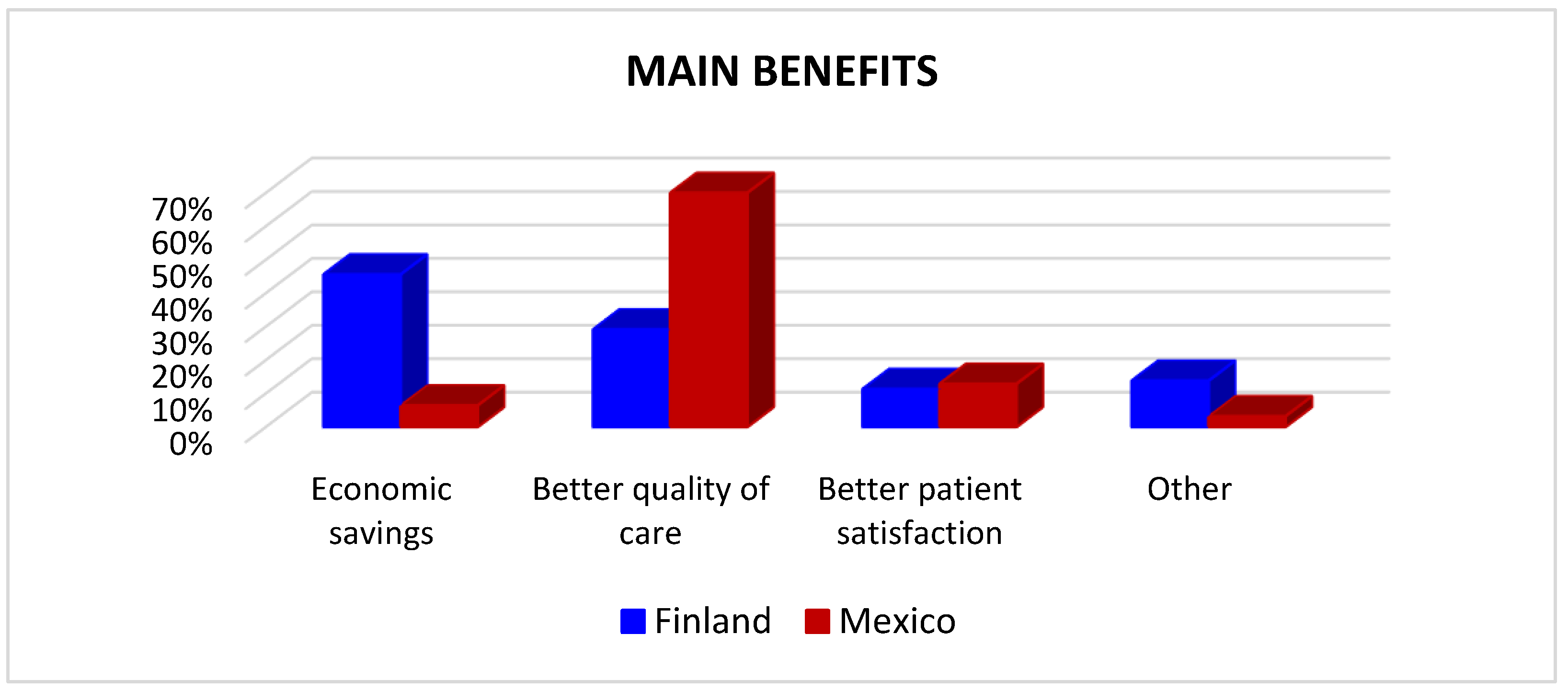
4.2.3. Benefits
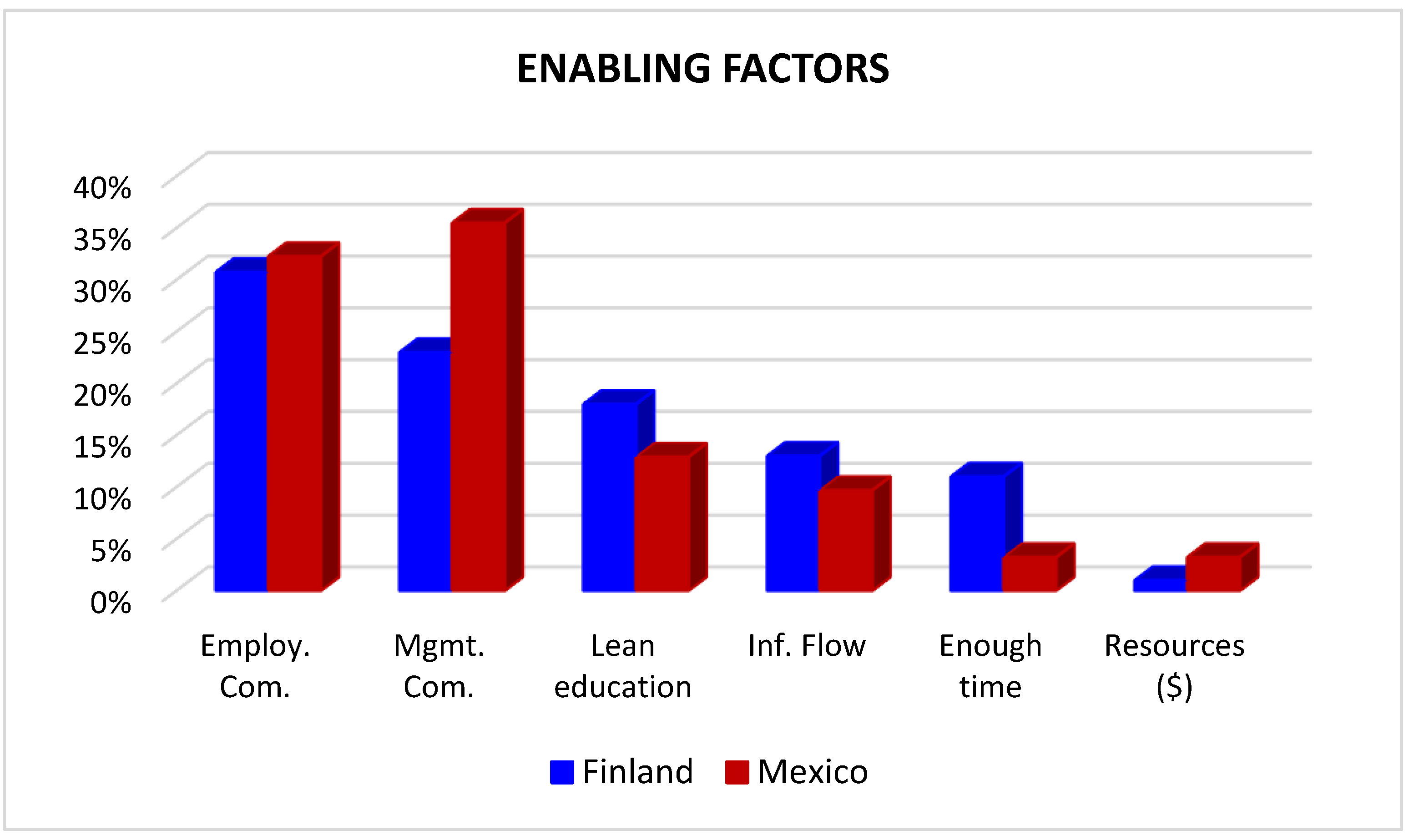
4.2.4. Factors
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- Do you have an ongoing (or have you had a) Lean project(s)?
- Yes
- No
- 2.
- Do you know what Lean thinking is?
- Yes
- No
- 3.
- Have you considered using Lean thinking in your organization?
- Yes
- No
- 4.
- What Lean tools do you know? (multiple)
- Value stream mapping
- Kaizen
- 5´s
- Kanban
- Visual control
- None of the above
- 5.
- In your opinion, where or in what healthcare functions does Lean thinking methodology have the greatest potential?
- Healthcare support functions (laundry, accounting, transportation, general administration, etc.)
- Healthcare functions indirectly involved in patient processes (pharmacy, laboratory, etc.)
- Patient processes / patient treatment processes
- Other.
- 6.
- When did you first launch a Lean project?
- More than five years ago
- 3–5 years ago
- 1–3 years ago
- Less than one year ago
- 7.
- What was the initial reason for initiating Lean in your organization? (only one)
- Financial saving/increasing productivity
- Better quality of care/few errors
- Better patient satisfaction
- Other.
- 8.
- Who introduced the first Lean project in your organization? (only one)
- Member of the front-line staff (nurse, physician, technician, etc.)
- Supervisor level (chief nurse, chief physician, etc.)
- Middle-management (nurse manager, physician manager)
- Executive level / top management
- Somebody outside your organization
- 9.
- Do you have a Lean expert in your organization?
- Yes
- No
- 10.
- What is his/her educational background for Lean?
- Lean education or certification
- Related formal education at a general university or university of applied sciences (process engineering, etc.)
- ‘Self-educated’ by means of literature, seminars and in practice
- ‘Practical’ learning (managing or taking part in Lean projects)
- N/A
- 11.
- How many Lean project have you had in your organization?
- More than 10
- 6–10
- 2–5
- One
- 12.
- In your opinion, how has Lean been implemented in your organization?
- Lean thinking is a part of our organization’s daily operations (management system and methodology)
- Lean thinking is systematic, but is not included as part of daily operations/ management (methodology)
- Lean thinking is part of process development (methodology)
- Lean thinking is used in our organization but not systematically
- Lean thinking has been used, but is not currently in use
- 13.
- What Lean methods have you used in your organization/unit? (multiple)
- Value stream mapping
- Kaizen
- 5´s
- Kanban
- Visual control
- 14.
- What is the amount of money invested in your Lean project(s)?
- More than $630,000 Mexican pesos—€30,000
- $336,000-$630,000 Mexican pesos—€16,000–30,000
- $105,000-$336,000 Mexican pesos—€5000–15,999
- Less than $105,000 Mexican pesos—€5000
- No money invested/done in daily work
- Unknown
- 15.
- What (if measured) is the amount of money saved with Lean project(s)?
- More than $10.5 million Mexican pesos—€500,000
- $5.2 million–$10.5 million Mexican pesos—€251,000–500,000
- $2.1 million–$5.2 million Mexican pesos—€101,000–250,000
- $1 million–$2.1 million Mexican pesos—€50,000–100,000
- Less than $1 million Mexican pesos—€50,000
- Unknown
- 16.
- Do you or did you require specific or measurable goals when initiating (when you initiated) your first Lean project?
- Yes
- No
- 17.
- Did your first project achieve its goals?
- Yes
- No
- 18.
- In your opinion, have Lean project(s) been successful in your organization?
- Yes
- No
- 19.
- What is the most important benefit that Lean thinking has brought to your organization?
- Economic savings/better productivity
- Better quality of care/fewer treatment errors
- Better patient satisfaction
- Other, what?
- 20.
- What were the enabling factors for Lean project?
- Committed management
- Committed employees
- Good financial resources
- Enough time for projects
- Lean education
- Good flow of information
- Other, what?
- 21.
- What were the disabling factors for Lean project?
- Lack of commitment of management
- Lack of committed employees
- Lack of financial resources
- Insufficient time for project
- Insufficient training in Lean
- Inappropriate flow of information
- Other.
- 22.
- Which professional group (if it can be specified) was the least supportive of your organization’s Lean project(s)?
- Nurses
- Physicians
- Other personnel involved in patient/treatment processes (including but not limited to healthcare assistants, lab technicians, etc.).
- Supervisors
- Middle management
- Executive management
- 23.
- What are (in your opinion) the reasons for resistance to Lean projects?
- Tired of development projects
- Lack of knowledge
- The will to maintain old ways to do things
- Discrepancies between professional groups
- Negative experiences from previous Lean initiatives
- Other.
Appendix B. Responses by Management vs. Workers Groups

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Count. | Mgm | Work | Mgm | Work | Mgm | Work | Mgm | Work | Mgm | Work | Mgm | Work | Mgm | Work | Mgm | Work |
| Yes | 50% | 24% | 46% | 14% | 56% | 38% | ||||||||||
| No | 50% | 76% | 54% | 86% | 44% | 62% | ||||||||||
| a | 43 | 41 | 12% | 12% | 12% | 10% | 54% | 37% | 15% | 25% | ||||||
| b | 49 | 53 | 10% | 15% | 31% | 27% | 34% | 47% | 15% | 26% | ||||||
| c | 42 | 64 | 75% | 70% | 37% | 44% | 8% | 10% | 21% | 18% | ||||||
| d | 18 | 15 | 3% | 2% | 20% | 19% | 4% | 5% | 33% | 21% | ||||||
| e | 31 | 33 | 17% | 10% | ||||||||||||
| Total Resp. | 103 | 267 | 54 | 197 | 48 | 186 | 102 | 263 | 73 | 84 | 49 | 59 | 48 | 61 | 48 | 61 |
| Q9 | Q10 | Q11 | Q12 | Q13 | Q14 | Q15 | Q16 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Count. | Mgm | Work | Mgm | Work | Mgm | Work | Mgm | Work | Mgm | Work | Mgm | Work | Mgm | Work | Mgm | Work |
| Yes | 71% | 59% | 66% | 66% | ||||||||||||
| No | 29% | 41% | 34% | 34% | ||||||||||||
| a | 23% | 19% | 13% | 12% | 20% | 10% | 23 | 24 | 8% | 7% | 0% | 0% | ||||
| b | 28% | 21% | 22% | 16% | 14% | 10% | 23 | 23 | 21% | 2% | 4% | 0% | ||||
| c | 40% | 38% | 52% | 40% | 18% | 30% | 21 | 32 | 10% | 4% | 2% | 3% | ||||
| d | 25% | 45% | 13% | 33% | 48% | 38% | 4 | 6 | 6% | 4% | 2% | 0% | ||||
| e | 20% | 26% | 0% | 12% | 14 | 12 | 23% | 18% | 8% | 3% | ||||||
| f | 31% | 65% | 84% | 93% | ||||||||||||
| Total Resp. | 49 | 59 | 40 | 42 | 46 | 58 | 50 | 60 | 48 | 61 | 48 | 55 | 50 | 58 | 50 | 58 |
| Q17 | Q18 | Q19 | Q20 | Q21 | Q22 | Q23 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Count. | Mgm | Work | Mgm | Work | Mgm | Work | Mgm | Work | Mgm | Work | Mgm | Work | Mgm | Work |
| Yes | 100% | 88% | 96% | 79% | ||||||||||
| No | 0% | 12% | 4% | 21% | ||||||||||
| a | 46% | 25% | 63% | 48% | 15% | 15% | 16% | 20% | 29% | 25% | ||||
| b | 32% | 52% | 75% | 66% | 29% | 23% | 49% | 43% | 41% | 46% | ||||
| c | 10% | 13% | 0% | 5% | 29% | 18% | 19% | 17% | 51% | 54% | ||||
| d | 12% | 10% | 25% | 21% | 58% | 45% | 8% | 7% | 18% | 20% | ||||
| e | 38% | 38% | 33% | 18% | 0% | 6% | 2% | 0% | ||||||
| f | 31% | 25% | 21% | 17% | 8% | 7% | 6% | 7% | ||||||
| g | 6% | 8% | 13% | 7% | ||||||||||
| Total Resp. | 31 | 41 | 47 | 57 | 50 | 60 | 48 | 61 | 48 | 60 | 37 | 54 | 49 | 61 |
References
- Brackett, T.; Comer, L.; Whichello, R. Do Lean Practices Lead to More Time at the Bedside? J. Healthc. Qual. 2013, 35, 7–14. [Google Scholar] [CrossRef]
- D’Andreamatteo, A.; Ianni, L.; Lega, F.; Sargiacomo, M. Lean in healthcare: A comprehensive review. Health Policy 2015, 119, 1197–1209. [Google Scholar] [CrossRef] [PubMed]
- Poksinska, B. The Current State of Lean Implementation in Health Care: Literature Review. Qual. Manag. Health Care 2010, 19, 319–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grout, J.R.; Toussaint, J.S. Mistake-proofing healthcare: Why stopping processes may be a good start. Busi Horiz 2010, 53, 149–156. [Google Scholar] [CrossRef]
- Barnas, K. ThedaCare’s business performance system: Sustaining continuous daily improvement through hospital management in a lean environment. Jt. Comm J. Qual. Saf. 2011, 37, 387–399. [Google Scholar] [CrossRef]
- Furman, C.; Caplan, R. Applying the Toyota Production System: Using a patient safety alert system to reduce error. Jt. Comm J. Qual. Saf. 2007, 33, 376–386. [Google Scholar] [CrossRef]
- Nelson-Peterson, D.L.; Leppa, C.J. Creating an environment for caring using lean principles of the Virginia Mason Production System. J. Nurs. Adm. 2007, 37, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Ben-Tovim, D.I.; Bassham, J.E.; Bolch, D.; Martin, M.A.; Dougherty, M.; Szwarcbord, M. Lean thinking across a hospital: Redesigning care at the Flinders Medical Centre. Aust. Health Rev. 2007, 31, 10–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben-Tovim, D.I.; Bassham, J.E.; Bennett, D.M.; Dougherty, M.L.; Martin, M.A.; O’Neill, S.J.; Sincock, J.L.; Szwarcbord, M.G. Redesigning care at the Flinders Medical Centre: Clinical process redesign using “lean thinking”. Med. J. Aust. 2008, 188, 27–31. [Google Scholar] [CrossRef]
- Burgess, N.; Radnor, Z. Evaluating Lean in healthcare. Int. J. Health Care Qual. Assur. 2013, 26, 220–235. [Google Scholar] [CrossRef]
- Woodnutt, S. Is Lean sustainable in today’s NHS hospitals? A systematic literature review using the meta-narrative and integrative methods. Int. J. Health Care Qual. Assur. 2018, 30, 578–586. [Google Scholar] [CrossRef]
- Graban, M. Lean Hospitals: Improving Quality, Patient Safety, and Employee Engagement, 3rd ed.; CRC Press: New York, NY, USA, 2016. [Google Scholar]
- Peimbert-García, R.E.; Matis, T.; Cuevas-Ortuño, J.; and Nucamendi-Guillen, S.M. Systematic Review of Literature on Lean and Six Sigma in Healthcare and Directions for Future Research. In Proceedings of the 10th International Conference on Industrial Engineering and Operations Management (IEOM), Dubai, UAE, 10–12 March 2020. [Google Scholar]
- Hofstede, G.; Hofstede, G.J. Culture and Organizations: Software of the Mind, 2nd ed.; McGrawHill: New York, NY, USA, 2005. [Google Scholar]
- Hofstede, G. Dimensionalizing cultures: The Hofstede model in context. Online Read. Psychol. Cult. 2011, 2, 1–8. [Google Scholar] [CrossRef]
- Kull, T.J.; Yan, T.; Liu, Z.; Wacker, J.G. The moderation of lean manufacturing effectiveness by dimensions of national culture: Testing practice-culture congruence hypotheses. Int. J. Prod. Econ. 2014, 153, 1–12. [Google Scholar] [CrossRef]
- Machado-Guimararâes, C.; Crespo de Carvalho, J. Lean Healthcare across Cultures: State-Of-The-Art. Am. Int. J. Contemp. Res. 2012, 2, 187–206. [Google Scholar]
- Erthal, A.; Marques, L. National culture and organisational culture in lean organisations: A systematic review. Prod. Plan. Control. 2018, 29, 668–687. [Google Scholar] [CrossRef]
- Jorma, T.; Tiirinki, H.; Bloigu, R.; Turkki, L. LEAN thinking in Finnish healthcare. Leadersh. Health Serv. 2016, 29, 9–36. [Google Scholar] [CrossRef] [PubMed]
- Peimbert-García, R.E.; Matis, T.; Beltran-Godoy, J.H.; Garay-Rondero, C.L.; Vicencio-Ortiz, J.C.; Lopez-Soto, D. Assessing the State of Lean and Six Sigma Practices in Healthcare in Mexico. Leadersh. Health Serv. 2019, 32, 644–662. [Google Scholar] [CrossRef]
- Statistics Finland. Health Expenditure and Financing. Available online: http://www.stat.fi/til/thkura/index_en.html (accessed on 4 March 2020).
- Finnish Institute for Health and Welfare Personnel in the Health Care and Social Welfare. Available online: https://thl.fi/en/web/thlfi-en (accessed on 5 March 2020).
- INEGI. National Institute of Statistics and Geography. Available online: https://en.www.inegi.org.mx (accessed on 6 March 2020).
- Womack, J.P.; Jones, D.T. Lean Thinking: Banish Waste and Create Wealth in Your Corporation, 2nd ed.; Free Press: New York, NY, USA, 2003. [Google Scholar]
- Costa, L.B.M.; Folho, M.G. Lean healthcare: Review, classification and analysis of literature. Prod. Plan. Control. 2016, 27, 823–836. [Google Scholar] [CrossRef]
- Henrique, D.B.; Filho, M.G. A systematic literature review of empirical research in Lean and Six Sigma in healthcare. Total Qual. Manag. Bus. Excell. 2020, 31, 429–449. [Google Scholar] [CrossRef]
- Tlapa, D.; Zepeda-Lugo, C.A.; Tortorella, G.L.; Baez-Lopez, Y.A.; Limon-Romero, J.; Alvarado-Iniesta, A.; Rodriguez-Borbon, M.I. Effects of lean healthcare on patient flow: A systematic review. Value Health 2020, 23, 260–273. [Google Scholar] [CrossRef] [Green Version]
- Khodambashi, S. Alignment of an intra-operating management process to a health information system: A Lean analysis approach. Pers. Ubiquitous Comput. 2015, 19, 689–698. [Google Scholar] [CrossRef]
- Savage, C.; Parke, L.; von Knorring, M.; Mazzocato, P. Does lean muddy the quality improvement waters? A qualitative study of how a hospital management team understands lean in the context of quality improvement. BMC Health Serv. Res. 2016, 16, 588–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulhassan, W.; Sandahl, C.; Westerlund, H.; Henriksson, P.; Bennermo, M.; Scharwz, U.T.; Thor, J. Antecedents and Characteristics of Lean Thinking Implementation in a Swedish Hospital: A Case Study. Qual. Manag. Health Care 2013, 22, 48–61. [Google Scholar] [CrossRef] [PubMed]
- Setijono, D.; Naraghi, A.M.; Ravipati, U.P. Decision support system and the adoption of lean in a Swedish emergency ward: Balancing supply and demand towards improved value stream. Int. J. Lean Six Sigma 2010, 1, 234–248. [Google Scholar] [CrossRef]
- Larsson, A.; Johansson, M.; Baathe, F.; Neselius, S. Reducing throughput time in a service organisation by introducing cross-functional teams. Prod. Plan. Control. 2012, 23, 571–580. [Google Scholar] [CrossRef]
- Mazzocato, P.; Holden, R.J.; Brommels, M.; Aronsson, H.; Backman, U.; Elg, M.; Thor, J. How does lean work in emergency care? A case study of a lean-inspired intervention at the Astrid Lindgren Children’s hospital, Stockholm, Sweden. BMC Health Serv. Res. 2012, 12, 28–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, K.; Nielsen, A.P.; Jacobsen, P. Implementing lean in surgery–lessons and implications. Int. J. Technol. Manag. 2012, 57, 4–17. [Google Scholar] [CrossRef]
- Andersen, H.; Røvik, K.A. Lost in translation: A case-study of the travel of lean thinking in a hospital. BMC Health Serv. Res. 2015, 15, 401–410. [Google Scholar] [CrossRef] [Green Version]
- Hasle, P.; Anders, P.N.; Edwards, K. Application of Lean Manufacturing in Hospitals—the Need to Consider Maturity, Complexity, and the Value Concept. Hum. Factor Ergon. Manuf. 2016, 26, 430–442. [Google Scholar] [CrossRef] [Green Version]
- Johannessen, K.A.; Alexandersen, N. Improving accessibility for outpatients in specialist clinics: Reducing long waiting times and waiting lists with a simple analytic approach. BMC Health Serv. Res. 2018, 18, 827–830. [Google Scholar] [CrossRef]
- Hihnala, S.; Kettunen, L.; Suhonen, M.; Tiirinki, H. The Finnish healthcare services lean management: Health services managers’ experiences in a special health care unit. Leadersh. Health Serv. 2018, 31, 17–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maijala, R.; Eloranta, S.; Reunanen, T.; Ikonen, T.S. Successful implementation of Lean as a managerial principle in health care: A conceptual analysis from systematic literature review. Int. J. Technol. Assess. Health Care 2018, 34, 134–146. [Google Scholar] [CrossRef]
- Ruohoaho, U.M.; Kokki, M.; Hirvonen, J.; Joukainen, S.; Aaltomaa, S.; Fraunberg, M.; Leinonen, V.; Reijula, J. Value stream map assessment of the extended day: 23h surgery model. Intell Build. Int. 2018, 1–15. [Google Scholar] [CrossRef]
- da Silva, I.B.; Seraphim, E.C.; Agostinho, O.L.; Lima, J.O.F.; Batalha, G.F. Lean office in health organization in the Brazilian Army. Int. J. Lean Six Sigma 2015, 6, 2–16. [Google Scholar] [CrossRef]
- Filho, M.G.; Boschi, A.; Rentes, A.F.; Thurer, M.; Bertani, T.M. Improving hospital performance by use of lean techniques: An action research project in Brazil. Qual. Eng. 2015, 27, 196–211. [Google Scholar] [CrossRef]
- Peimbert-García, R.E. Analysis and Evaluation of Reviews on Lean and Six Sigma in Healthcare. Qual. Manag. Health Care 2019, 28, 229–236. [Google Scholar] [CrossRef]
- Zepeda-Lugo, C.; Tlapa, D.; Baez-Lopez, Y.; Limon-Romero, J.; Ontiveros, S.; Perez-Sanchez, A.; Tortorella, G. Assessing the impact of lean healthcare on inpatient care: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 5609. [Google Scholar] [CrossRef] [PubMed]
- Peimbert-García, R.E.; Gutiérrez-Mendoza, L.M.; García-Reyes, H. Applying Lean Healthcare to Improve the Discharge Process in a Mexican Academic Medical Center. Sustainability 2021. Accepted for Publication. [Google Scholar]







| # | Definition | Finland | Mexico |
|---|---|---|---|
| 1 | Power distance is the extent to which the less powerful members expect and accept that power is distributed unequally. | Equal rights and hierarchy for convenience only | Hierarchical society |
| 2 | Individualism is the degree of interdependence a society maintains among its members. | Individualist society | Collectivistic society |
| 3 | Masculinity. High score (Masc.): Society is driven by competition and success. Low score (Fem.): Dominant values are caring for others and quality of life, which is a sign of success. | Feminine society | Masculine society |
| 4 | Uncertainty Avoidance is the extent to which the members of a culture feel threatened by ambiguous or unknown situations. | Preference for avoiding uncertainty | High preference for avoiding uncertainty |
| 5 | Long Term Orientation. Low score: Society prefers to maintain time-honored traditions and norms. High score: Society encourages thrift and efforts in modern education as a way to prepare for the future. | Normative | Normative |
| 6 | Indulgence is the extent to which people try to control their desires and impulses. Weak control is called “Indulgence” and strong control is “Restraint”. | Indulgent | Highly indulgent |
| Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Count. | FIN | MEX | FIN | MEX | FIN | MEX | FIN | MEX | FIN | MEX | FIN | MEX | FIN | MEX | FIN | MEX |
| Yes | 75% | 13% | 90% | 11% | 84% | 37% | ||||||||||
| No | 25% | 87% | 10% | 89% | 16% | 63% | ||||||||||
| a | 68 | 16 | 7% | 23% | 21% | 20% | 59% | 10% | 23% | 13% | ||||||
| b | 75 | 27 | 7% | 27% | 40% | 20% | 27% | 77% | 21% | 22% | ||||||
| c | 55 | 51 | 83% | 48% | 32% | 43% | 9% | 10% | 17% | 25% | ||||||
| d | 28 | 5 | 4% | 2% | 8% | 17% | 5% | 3% | 22% | 38% | ||||||
| e | 52 | 12 | 17% | 3% | ||||||||||||
| Total Resp. | 110 | 260 | 31 | 220 | 25 | 209 | 107 | 260 | 107 | 52 | 78 | 30 | 78 | 31 | 77 | 32 |
| Q9 | Q10 | Q11 | Q12 | Q13 | Q14 | Q15 | Q16 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Count. | FIN | MEX | FIN | MEX | FIN | MEX | FIN | MEX | FIN | MEX | FIN | MEX | FIN | MEX | FIN | MEX |
| Yes | 74% | 42% | 59% | 83% | ||||||||||||
| No | 26% | 58% | 41% | 17% | ||||||||||||
| a | 13% | 33% | 15% | 7% | 15% | 13% | 41 | 8 | 11% | 0% | 0% | 0% | ||||
| b | 14% | 42% | 20% | 13% | 11% | 13% | 37 | 9 | 15% | 0% | 3% | 0% | ||||
| c | 30% | 8% | 42% | 53% | 23% | 29% | 27 | 26 | 8% | 3% | 4% | 0% | ||||
| d | 26% | 17% | 23% | 27% | 49% | 26% | 8 | 2 | 6% | 3% | 1% | 0% | ||||
| e | 17% | 8% | 1% | 19% | 24 | 2 | 25% | 10% | 8% | 0% | ||||||
| f | 35% | 84% | 84% | 100% | ||||||||||||
| Total Resp. | 77 | 31 | 70 | 12 | 74 | 30 | 79 | 31 | 77 | 32 | 72 | 31 | 77 | 31 | 78 | 30 |
| Q17 | Q18 | Q19 | Q20 | Q21 | Q22 | Q23 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Count. | FIN | MEX | FIN | MEX | FIN | MEX | FIN | MEX | FIN | MEX | FIN | MEX | FIN | MEX |
| Yes | 100% | 81% | 88% | 82% | ||||||||||
| No | 0% | 19% | 12% | 18% | ||||||||||
| a | 46% | 6% | 23% | 35% | 9% | 6% | 20% | 16% | 21% | 3% | ||||
| b | 29% | 77% | 31% | 32% | 14% | 23% | 51% | 34% | 25% | 47% | ||||
| c | 11% | 13% | 1% | 3% | 12% | 23% | 10% | 31% | 36% | 31% | ||||
| d | 14% | 3% | 11% | 3% | 33% | 16% | 10% | 3% | 12% | 16% | ||||
| e | 18% | 13% | 13% | 23% | 3% | 3% | 1% | 0% | ||||||
| f | 13% | 10% | 13% | 3% | 5% | 13% | 5% | 3% | ||||||
| g | 3% | 3% | 5% | 6% | ||||||||||
| Total Resp. | 45 | 27 | 76 | 28 | 79 | 31 | 78 | 31 | 77 | 31 | 59 | 32 | 78 | 32 |
| Finland vs. Mexico | Mgmt. vs. Workers | |||||||
|---|---|---|---|---|---|---|---|---|
| Group | # | Question | Test | p-Value | Status | p-Value | Status | |
| All respondents | 1 | Ongoing Lean projects | p | 0.00 | ≠ | 0.00 | ≠ | |
| 4 | Familiarity w/Lean tools | Wilcoxon | 0.03 | ≠ | 0.03 | ≠ | ||
| 5 | Funct. w/greatest impact | X2 | 0.00 | ≠ | 0.55 | = | ||
| Participating respondents | Starting | 6 | Timing of the first project | X2 | 0.23 | = | 0.89 | = |
| 7 | Initial reason for Lean | X2 | 0.00 | ≠ | 0.22 | = | ||
| 8 | Who introduced Lean | X2 | 0.11 | = | 0.23 | = | ||
| 16 | Measurable goals | p | 0.03 | ≠ | 0.96 | = | ||
| Integration | 9 | Internal Lean expert | p | 0.00 | ≠ | 0.18 | = | |
| 10 | Background Lean expert | X2 | 0.04 | ≠ | 0.44 | = | ||
| 11 | No. of Lean projects | X2 | 0.48 | = | 0.13 | = | ||
| 12 | Lean integration | X2 | 0.78 | = | 0.16 | = | ||
| 13 | Use of Lean tools | Wilcoxon | 0.03 | ≠ | 0.42 | = | ||
| Benefits | 14 | Investment in Lean | - | - | NA | - | NA | |
| 15 | Economic savings | - | - | NA | - | NA | ||
| 17 | Achieving goals | p | 0.01 | ≠ | 0.01 | ≠ | ||
| 18 | Success of Lean | p | 0.46 | = | 0.00 | ≠ | ||
| 19 | Main benefits | X2 | 0.00 | ≠ | 0.045 | ≠ | ||
| Factors | 20 | Enabling factors | X2 | 0.39 | = | 0.97 | = | |
| 21 | Disabling factors | X2 | 0.09 | = | 0.94 | = | ||
| 22 | Least supportive groups | X2 | 0.40 | = | 0.77 | = | ||
| 23 | Reasons of resistance | X2 | 0.03 | ≠ | 0.95 | = | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peimbert-García, R.E.; Jorma, T.; Cárdenas-Barrón, L.E.; Nucamendi-Guillén, S.M.; García-Reyes, H. Linking Lean Adoption and Implementation in Healthcare to National Cultures. Sustainability 2021, 13, 8855. https://0-doi-org.brum.beds.ac.uk/10.3390/su13168855
Peimbert-García RE, Jorma T, Cárdenas-Barrón LE, Nucamendi-Guillén SM, García-Reyes H. Linking Lean Adoption and Implementation in Healthcare to National Cultures. Sustainability. 2021; 13(16):8855. https://0-doi-org.brum.beds.ac.uk/10.3390/su13168855
Chicago/Turabian StylePeimbert-García, Rodrigo E., Tapani Jorma, Leopoldo Eduardo Cárdenas-Barrón, Samuel M. Nucamendi-Guillén, and Heriberto García-Reyes. 2021. "Linking Lean Adoption and Implementation in Healthcare to National Cultures" Sustainability 13, no. 16: 8855. https://0-doi-org.brum.beds.ac.uk/10.3390/su13168855