
Family Welfare Expenditure, Contraceptive Use, Sources and Method-Mix in India

 ,
,  ,
,  ,
, 

Abstract
:1. Introduction
Indian Context
2. Materials and Methods
2.1. Data Sources
2.2. Empirical Strategy
2.2.1. Descriptive Analyses
2.2.2. Macro Data Analyses: Variables and Model Description
2.2.3. Microdata Analyses: Variables and Model Description
3. Results
3.1. FWE and its Share in Total PHE
3.2. Contraceptive Method-Mix
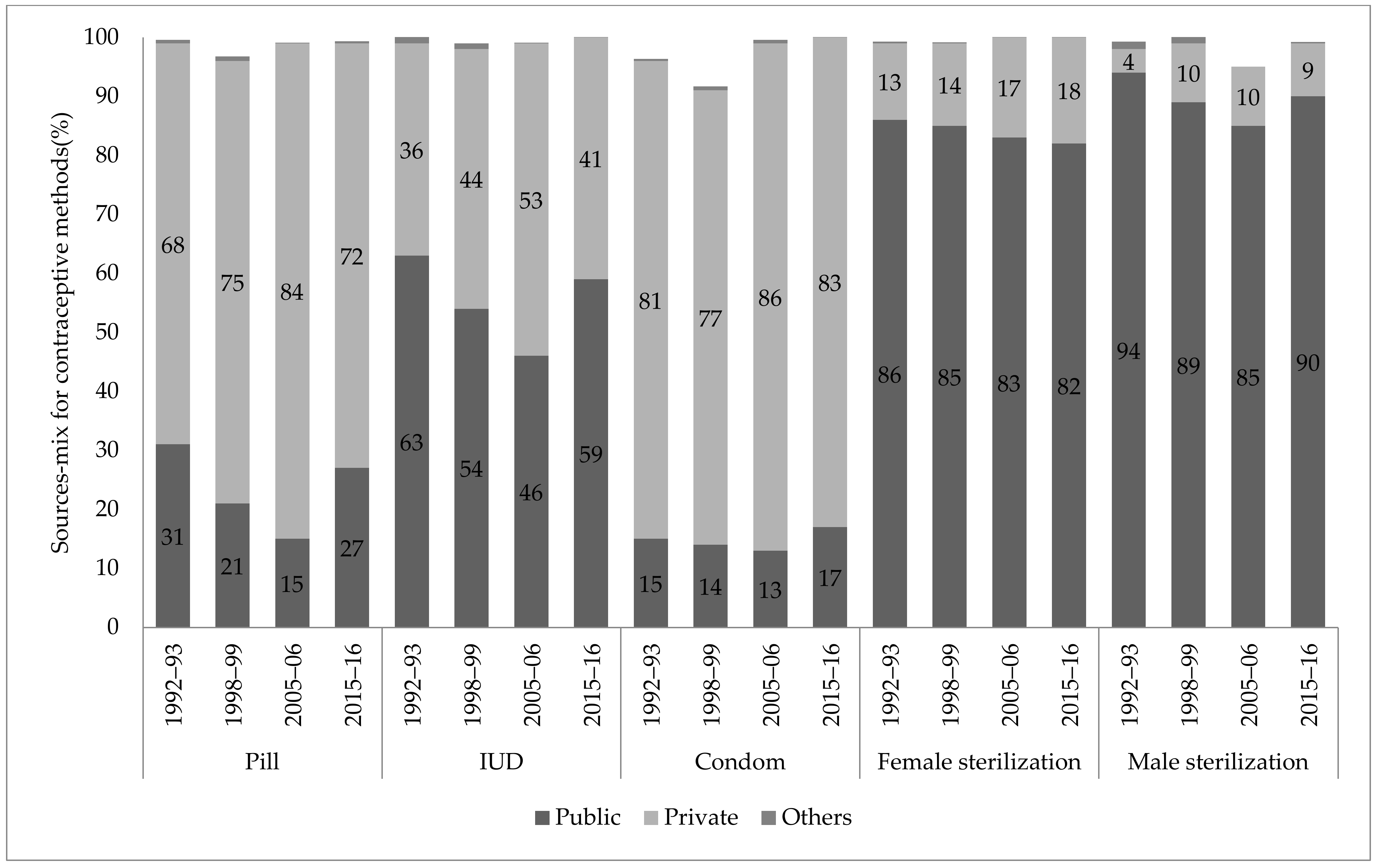
3.3. Sources of Contraceptive Methods
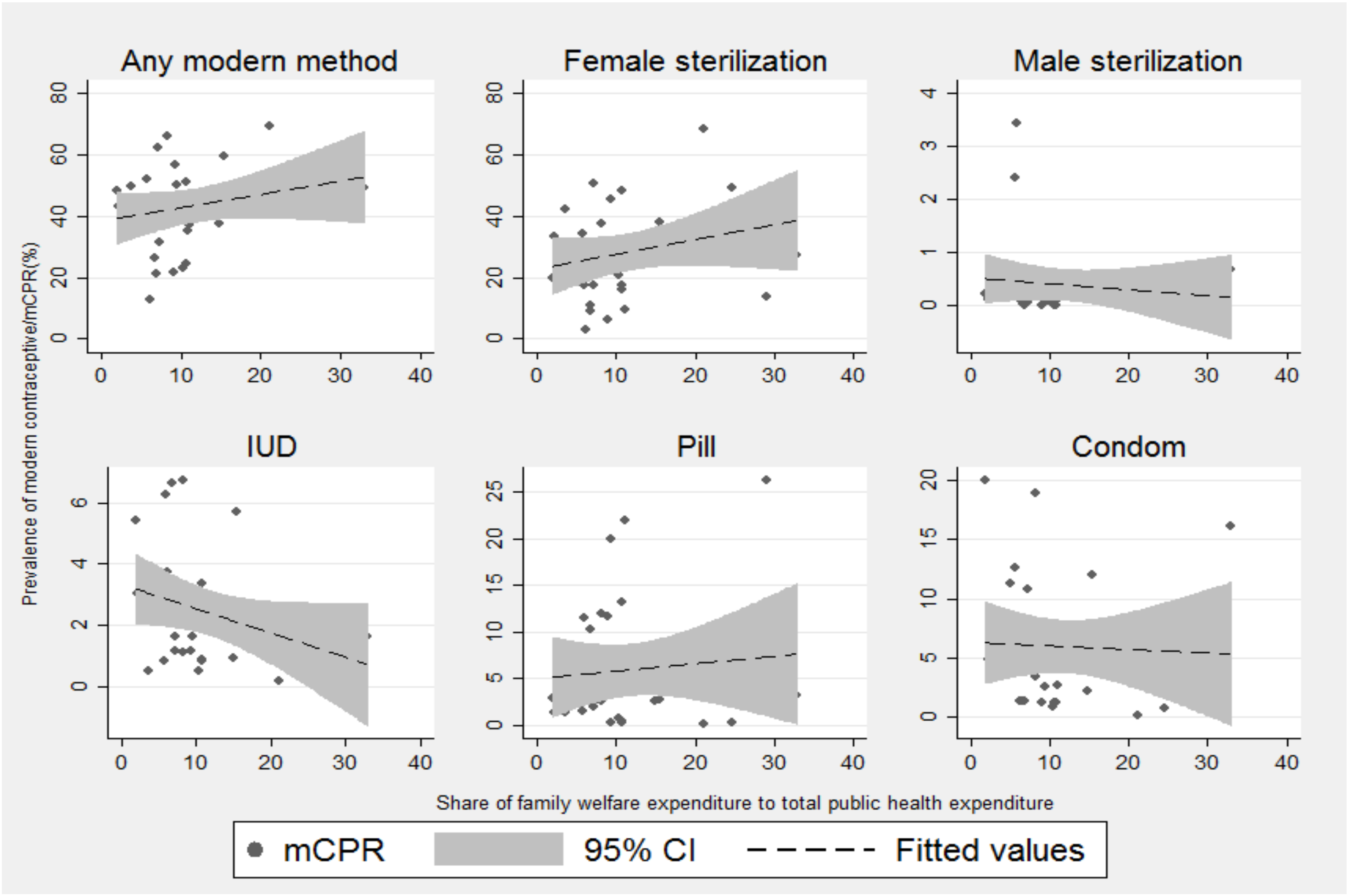
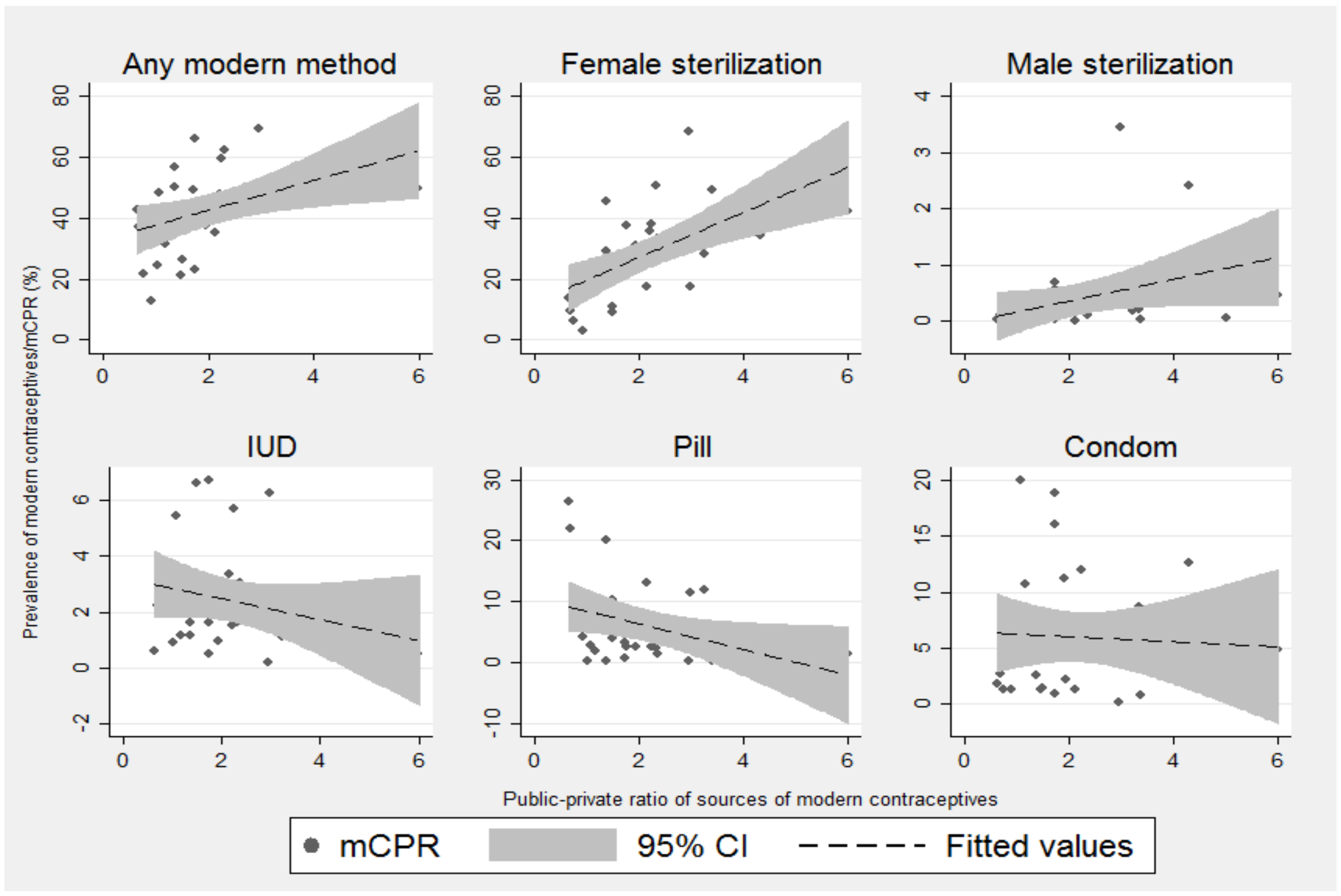
3.4. Correlation of FWE and PPR With Use of Modern Contraceptive Methods
3.5. The Effect of FWE on FP Use: Results From Panel Data Regression Analyses
3.6. Factors Associated with the Public Sector as the Source of Modern Contraception: Results from Binary Logistic Regression Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| State | Share of Family Welfare in Total Public Healthcare Expenditure | |||
|---|---|---|---|---|
| 1995–1996 | 1997–1998 | 2004–2005 | 2014–2015 | |
| India | 19.42 | 16.37 | 13.49 | 15.98 |
| Andhra Pradesh | 21.29 | 19.49 | 21.22 | 21.07 |
| Arunachal Pradesh | 3.19 | 4.60 | 4.6 | 6.68 |
| Assam | 16.69 | 12.78 | 17.11 | 11.04 |
| Bihar | 48.68 | 25.61 | 19.41 | 10.34 |
| Delhi | 6.67 | 3.65 | 1.26 | 1.93 |
| Goa | 2.6 | 3.66 | 2.77 | 2.18 |
| Gujarat | 16.19 | 15.30 | 14.01 | 10.7 |
| Haryana | 19.64 | 15.91 | 15.9 | 5.69 |
| Himachal Pradesh | 14.93 | 12.02 | 11.77 | 15.45 |
| Jammu & Kashmir | - | 8.72 | 9.28 | 14.88 |
| Jharkhand | - | - | - | 4.99 |
| Karnataka | 18.42 | 18.07 | 14.05 | 10.69 |
| Kerala | 14.7 | 14.13 | 14.06 | 9.38 |
| Madhya Pradesh | 17.24 | 15.42 | 12.5 | 8.99 |
| Maharashtra | 14.52 | 10.76 | 8.06 | 7.09 |
| Manipur | 15.62 | 14.09 | 14.85 | 3.64 |
| Meghalaya | 11.26 | 11.23 | 13.28 | 6.16 |
| Mizoram | 7.44 | 6.99 | 9.42 | 10.82 |
| Nagaland | - | 5.69 | 8.22 | 6.82 |
| Odisha | 23.11 | 20.08 | 20.53 | 8.18 |
| Punjab | 14.68 | 9.52 | 8.02 | 8.22 |
| Rajasthan | 20.22 | 20.97 | 18.77 | 31.27 |
| Sikkim | 12.81 | 12.32 | 11 | 5.89 |
| Tamil Nadu | 17.84 | 16.36 | 16.42 | 24.63 |
| Telangana | - | - | - | 26 |
| Tripura | 20.24 | 23.13 | 23.08 | 29.09 |
| Uttar Pradesh | 21.16 | 21.45 | 17.09 | 32.87 |
| Uttarakhand | - | - | - | 7.22 |
| West Bengal | 14.44 | 12.20 | 13.07 | 9.26 |
| Panel A | ||||||||||||
| States | Female Sterilization | Male Sterilization | IUD | |||||||||
| 1992-93 | 1998-99 | 2005-06 | 2015-16 | 1992-93 | 1998-99 | 2005-06 | 2015-16 | 1992-93 | 1998-99 | 2005-06 | 2015-16 | |
| All India | 67.4 | 70.8 | 66.3 | 67.2 | 8.5 | 3.9 | 1.8 | 0.5 | 4.6 | 3.4 | 3.2 | 2.9 |
| Andhra Pradesh | 81.1 | 88.4 | 92.9 | 98.2 | 14.1 | 7.3 | 4.4 | 0.8 | 1.2 | 1.1 | 0.7 | 0.3 |
| Arunachal Pradesh | 43.6 | 58.1 | 52.1 | 35.4 | 1.5 | 0.3 | 0.2 | 0.1 | 19.3 | 11.8 | 8.3 | 10.8 |
| Assam | 28.3 | 36.3 | 23 | 18.2 | 5.5 | 2.3 | 0.4 | 0.2 | 2.1 | 4.3 | 2.3 | 4.2 |
| Bihar | 74.9 | 78.2 | 69.8 | 86 | 5.8 | 4 | 1.8 | 0.2 | 2.3 | 2.2 | 1.8 | 2.1 |
| Delhi | 33.2 | 41.2 | 34.4 | 36.2 | 5.4 | 3.7 | 1.2 | 0.4 | 13 | 9.7 | 7.5 | 9.9 |
| Gujarat | 76.1 | 72.8 | 64.4 | 71.6 | 7.2 | 3.9 | 0.9 | 0.2 | 6.1 | 5.2 | 6.8 | 6.5 |
| Goa | 61.8 | 58.5 | 53.5 | 61.8 | 2.1 | 0.8 | 0.2 | 0 | 5.7 | 4 | 4.8 | 3.5 |
| Himachal Pradesh | 55.9 | 66.5 | 67.5 | 60.6 | 22.5 | 10.8 | 8.7 | 4.2 | 4.6 | 3 | 2.1 | 1.5 |
| Haryana | 59.9 | 62 | 60.3 | 59.7 | 10.1 | 3.4 | 1.1 | 0.9 | 6.4 | 5.7 | 7.4 | 8.9 |
| Jharkhand | ─ | ─ | 65.5 | 77 | ─ | ─ | 1.1 | 0.5 | ─ | ─ | 1.7 | 2.4 |
| Jammu & Kashmir | 51.2 | 57 | 50 | 42.5 | 8.9 | 5.5 | 4.9 | 0.7 | 5.6 | 6 | 5.1 | 5 |
| Karnataka | 83.5 | 88.3 | 90.3 | 93.8 | 3.1 | 1.1 | 0.3 | 0.1 | 6.5 | 4.7 | 4.9 | 1.6 |
| Kerala | 66 | 76.2 | 71 | 86.2 | 10.3 | 3.9 | 1.5 | 0.1 | 4.3 | 2.5 | 3.4 | 3.1 |
| Meghalaya | 45.4 | 32.1 | 39.1 | 25.5 | 2.9 | 0 | 0.4 | 0 | 10.6 | 16.3 | 6.2 | 8.7 |
| Maharashtra | 74.4 | 79.5 | 76.4 | 78.3 | 11.5 | 6.1 | 3.1 | 0.7 | 4.7 | 3.2 | 4.6 | 2.5 |
| Madhya Pradesh | 72.3 | 80.6 | 79.2 | 82.2 | 14.1 | 5.1 | 2.3 | 0.9 | 3.1 | 1.8 | 1.3 | 1 |
| Manipur | 31.2 | 37.2 | 16.6 | 13.2 | 8.4 | 3 | 1 | 0.4 | 19.3 | 17.6 | 11.1 | 15.8 |
| Mizoram | 82.8 | 78.4 | 71.6 | 49.3 | 0.2 | 0.2 | 0 | 0 | 9.5 | 9.3 | 8.2 | 9.5 |
| Nagaland | 48.9 | 40.6 | 33.3 | 34.1 | 0.8 | 0 | 0 | 0 | 15.8 | 25.3 | 17.5 | 25.1 |
| Orissa | 77.8 | 72.3 | 65.3 | 49.3 | 9.3 | 3.7 | 2 | 0.3 | 4.2 | 1.7 | 1.2 | 2 |
| Punjab | 53.7 | 43.9 | 48.7 | 49.5 | 4.2 | 2.4 | 1.9 | 0.7 | 10.7 | 9.2 | 8.7 | 8.9 |
| Rajasthan | 79.7 | 76.4 | 72.5 | 68.2 | 7.4 | 3.6 | 1.7 | 0.4 | 3.9 | 2.9 | 3.4 | 2.1 |
| Sikkim | ─ | 41.5 | 36.8 | 37.6 | ─ | 4.4 | 7.8 | 7.4 | ─ | 10.4 | 5.4 | 13.4 |
| Tamil Nadu | 75.4 | 86.7 | 89.6 | 92.9 | 3.9 | 1.5 | 0.7 | 0 | 7.1 | 4.7 | 3.4 | 3.5 |
| Tripura | 29.9 | 47 | 26.7 | 21.7 | 4.3 | 1.1 | 0.8 | 0 | 2.7 | 3.5 | 1.5 | 0.9 |
| Uttarakhand | ─ | ─ | 54.1 | 51.3 | ─ | ─ | 3 | 1.3 | ─ | ─ | 2.5 | 3.1 |
| Uttar Pradesh | 59 | 53.2 | 39.7 | 38.1 | 6.9 | 2.4 | 0.5 | 0.1 | 5.8 | 3.5 | 3.2 | 2.6 |
| West Bengal | 45.9 | 47.9 | 45.2 | 41.3 | 7.5 | 2.8 | 1 | 0.1 | 2.2 | 2.1 | 0.8 | 1.7 |
| Panel B | ||||||||||||
| States | Pill | Condom | Traditional methods | |||||||||
| 1992-93 | 1998-99 | 2005-06 | 2015-16 | 1992-93 | 1998-99 | 2005-06 | 2015-16 | 1992-93 | 1998-99 | 2005-06 | 2015-16 | |
| All India | 2.9 | 4.4 | 5.5 | 7.6 | 6 | 6.3 | 9.4 | 10.5 | 9.4 | 9.8 | 10.1 | 8.4 |
| Andhra Pradesh | 1 | 0.9 | 0.4 | 0.2 | 1.6 | 1.2 | 0.7 | 0.2 | 0.5 | 0.8 | 0.8 | 0.1 |
| Arunachal Pradesh | 13.7 | 20.5 | 19.2 | 32.3 | 3 | 1.9 | 6.7 | 4.5 | 17.3 | 6.2 | 9 | 7.9 |
| Assam | 6.4 | 14.6 | 18.2 | 42 | 4 | 4.1 | 4.2 | 5.2 | 46.7 | 33.7 | 35 | 22.9 |
| Bihar | 4.7 | 4 | 3.8 | 3.2 | 5.6 | 2.9 | 6.7 | 4 | 5.8 | 6.2 | 13.4 | 2.8 |
| Delhi | 4.8 | 6.3 | 6.7 | 5.3 | 34 | 27.4 | 34.8 | 36.5 | 8.9 | 10.7 | 9.8 | 6.8 |
| Gujarat | 2.1 | 2.6 | 3.9 | 2.9 | 3.6 | 5.9 | 9 | 10.4 | 4.6 | 8.9 | 11.5 | 4.5 |
| Goa | 1.5 | 1.9 | 3.1 | 1.3 | 8.2 | 10.3 | 16.2 | 26.9 | 19.1 | 20.3 | 13.8 | 4.7 |
| Himachal Pradesh | 0.9 | 1.9 | 3.9 | 2.7 | 9.1 | 7.4 | 16.1 | 22.2 | 6.3 | 9.5 | 1.7 | 6.2 |
| Haryana | 2.5 | 3.3 | 4.4 | 4.2 | 10.4 | 10.8 | 18.6 | 18.8 | 10.2 | 13.7 | 5.8 | 5 |
| Jharkhand | ─ | ─ | 10.6 | 6.4 | ─ | ─ | 7.8 | 5.4 | ─ | ─ | 10.7 | 5.7 |
| Jammu & Kashmir a | 2.7 | 6.7 | 8.9 | 10.9 | 11.9 | 9.8 | 15.4 | 19.7 | 18.7 | 13.2 | 9.3 | 13.3 |
| Karnataka | 0.9 | 1 | 1.7 | 0.9 | 2.4 | 1.8 | 3.3 | 2.5 | 3.2 | 2.7 | 1.1 | 0.4 |
| Kerala | 0.7 | 0.7 | 0.7 | 0.4 | 4.6 | 4.8 | 8.5 | 4.8 | 12.8 | 11.1 | 11.4 | 4.1 |
| Meghalaya | 11.6 | 22.1 | 20.2 | 47.9 | 2.4 | 6.2 | 10.3 | 5.3 | 7.6 | 18.1 | 13.2 | 5.3 |
| Maharashtra | 2.5 | 2.9 | 3.7 | 3.6 | 4.7 | 6.6 | 9.6 | 11 | 1.9 | 1.5 | 2.1 | 2.1 |
| Madhya Pradesh | 1.8 | 2.2 | 3 | 2.6 | 6 | 6.5 | 8.8 | 9.5 | 1.9 | 3 | 4.2 | 2.2 |
| Manipur | 6.8 | 5.7 | 10.9 | 17.9 | 3.5 | 3.4 | 8.6 | 5.7 | 28.9 | 29.9 | 31 | 29.8 |
| Mizoram | 4.7 | 9.3 | 17.7 | 37.4 | 1.2 | 1.6 | 2.8 | 3.6 | 1.4 | 1 | 0.3 | 0.1 |
| Nagaland | 16.5 | 8.4 | 15.8 | 15.1 | 16.5 | 5.8 | 9.4 | 5 | ─ | 18.2 | 16.1 | 12.1 |
| Orissa | 2.4 | 6.4 | 13.8 | 21 | 1.7 | 1.9 | 6.3 | 6 | 3.1 | 11.3 | 7.9 | 16 |
| Punjab | 3.7 | 4.6 | 4.6 | 3.3 | 15.2 | 20.6 | 24.5 | 24.9 | 11.9 | 17.9 | 8.1 | 8.7 |
| Rajasthan | 1.6 | 3.8 | 4.2 | 4 | 4.6 | 7.7 | 12.3 | 14.5 | 2.4 | 4.6 | 3.9 | 8 |
| Sikkim | ─ | 17.8 | 22.2 | 24.7 | ─ | 2.8 | 7.3 | 11.1 | ─ | 21.7 | 10.3 | 0.9 |
| Tamil Nadu | 1.1 | 0.6 | 0.3 | 0.4 | 3.2 | 2.9 | 3.7 | 1.6 | 7.4 | 3.1 | 1.7 | 0.9 |
| Tripura | 11.4 | 24.3 | 33.4 | 41.1 | 2.9 | 2.6 | 5.3 | 2.9 | 43.8 | 19.8 | 22.4 | 26.5 |
| Uttarakhand | ─ | ─ | 7.1 | 6.1 | ─ | ─ | 26.5 | 30.1 | ─ | ─ | 4.6 | 4.7 |
| Uttar Pradesh | 5 | 4.4 | 3.9 | 4.2 | 16.2 | 14.8 | 20 | 23.7 | 5.5 | 19.5 | 21.5 | 22.2 |
| West Bengal | 6.2 | 13.7 | 16.4 | 28.2 | 3.2 | 4.4 | 6.3 | 8.4 | 31.4 | 25.9 | 23.9 | 13.9 |
References
- Cleland, J.; Bernstein, S.; Ezeh, A.; Faundes, A.; Glasier, A.; Innis, J. Family planning: The unfinished agenda. Lancet 2006, 368, 1810–1827. [Google Scholar] [CrossRef]
- Canning, D.; Schultz, T.P. The economic consequences of reproductive health and family planning. Lancet 2012, 380, 165–171. [Google Scholar] [CrossRef]
- Joshi, S.; Schultz, T.P. Family planning and women’s and children’s health: Long-term consequences of an outreach program in Matlab, Bangladesh. Demography 2013, 50, 149–180. [Google Scholar] [CrossRef] [Green Version]
- Moreland, S. Egypt’s Population Program: Assessing 25 Years of Family Planning. Brief prepared for the US Agency for International Development. Available online: http://www.policyproject.com/abstract.cfm/2793 (accessed on 22 August 2021).
- United Nations. Contraceptive Use by Method 2019: Data Booklet (ST/ESA/SER.A/435); Department of Economic and Social Affairs, Population Division: New York, NY, USA, 2019. [Google Scholar]
- Bongaarts, J.; Cleland, J.; Townsend, J.W.; Bertrand, J.T.; Gupta, M.D. Family Planning Programs for the 21st Century; Population Council: New York, NY, USA, 2012. [Google Scholar]
- Bailey, M.J.; Malkova, O.; Norling, J. Do family planning programs decrease poverty? Evidence from public census data. CESifo Econ. Stud. 2014, 60, 312–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goli, S.; James, K.S.; Singh, D.; Srinivasan, V.; Mishra, R.; Rana, M.J.; Reddy, U.S. Economicreturns of family planning and fertility decline in India 1991–2061. J. Demogr. Econ. 2021, 1–33. [Google Scholar] [CrossRef]
- Jurczynska, K.; Moreland, S.; Sacher, S.; Bispo, S.; Corpuz, K. Modeling the Effects of Family Planning on the Sustainable Development Goals: Family Planning-Sustainable Development Goals Model Methodology and User’s Manual; USAID: Washington, DC, USA, 2018. [Google Scholar]
- Starbird, E.; Norton, M.; Marcus, R. Investing in family planning: Key to achieving the sustainable development goals. Glob. Health Sci. Pract. 2016, 4, 191–210. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.; Choi, Y.; Rimon, J.G.; Alzouma, S.; Gichangi, P.; Guiella, G.; Kayembe, P.; Kibira, S.P.; Makumbi, F.; OlaOlorun, F.; et al. Trends in contraceptive prevalence rates in sub-Saharan Africa since the 2012 London Summit on Family Planning: Results from repeated cross-sectional surveys. Lancet Glob. Health 2019, 7, e904–e911. [Google Scholar] [CrossRef] [Green Version]
- Rana, M.J.; Goli, S. Tracing long-term trajectories of contraceptive practice across 185 countries. PLoS ONE 2018, 13, e0205927. [Google Scholar]
- United Nations Population Fund. Press Statement. Family Planning: Empowering People, Developing Nations. 2017. Available online: https://www.unfpa.org/press/family-planning-empowering-people-developing-nations (accessed on 22 August 2021).
- Ayad, M.; Wilkinson, M.; McNiff, M. Sources of Contraceptive Methods; Macro International Inc.: Calverton, MD, USA, 1994. [Google Scholar]
- Footman, K.; Benova, L.; Goodman, C.; Macleod, D.; Lynch, C.A.; PennKekana, L.; Campbell, O.M.R. Using multi-country household surveys to understand who provides reproductive and maternal health services in low and middle-income countries: A critical appraisal of the Demographic and Health Surveys. Trop. Med. Int. Health 2015, 20, 589–606. [Google Scholar] [CrossRef]
- Peters, D.H.; Mirchandani, G.G.; Hansen, P.M. Strategies for engaging the private sector in sexual and reproductive health: How effective are they? Health Policy Plan. 2004, 19 (Suppl. S1), i5–i21. [Google Scholar] [CrossRef]
- Ross, J.; Keesbury, J.; Hardee, K. Trends in the contraceptive method mix in low- and middle-income countries: Analysis using a new "average deviation" measure. Glob. Health Sci. Pract. 2015, 3, 34–55. [Google Scholar] [CrossRef]
- Ensor, T.; Cooper, S.; Davidson, L.; Fitzmaurice, A.; Graham, W.J. The impact of economic recession on maternal and infant mortality: Lessons from history. BMC Public Health 2010, 10, 727. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.; Verhoeven, M.; Tiongson, E.R. Public spending on health care and the poor. Health Econ. 2003, 12, 685–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maruthappu, M.; Ng, K.Y.B.; Williams, C.; Atun, R.; Zeltner, T. Government health care spending and child mortality. Pediatrics 2015, 135, e887–e894. [Google Scholar] [CrossRef] [Green Version]
- Novignon, J.; Olakojo, S.A.; Nonvignon, J. The effects of public and private health care expenditure on health status in sub-Saharan Africa: New evidence from panel data analysis. Health Econ. Rev. 2012, 2, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gribble, J.N.; Jennings, V.; Nikula, M. Mind the gap: Responding to the global funding crisis in family planning. BMJ Sex. Reprod. Health 2004, 30, 155–157. [Google Scholar] [CrossRef] [Green Version]
- Goli, S.; James, K.S.; Singh, D.; Srinivasan, V. Road to family planning and RMNCHN related SDGs: Tracing the role of public health spending in India. Glob. Public Health 2020, 16, 546–562. [Google Scholar] [CrossRef]
- United Nations. Transforming Our World; The 2030 Agenda for Sustainable Development; United Nations: New York, NY, USA, 2015; Available online: https://sustainabledevelopment.un.org/post2015/transformingourworld (accessed on 28 December 2018).
- Abhiyan, W.N.T. Sustainable Development Goals: Agenda 2030; A Civil Society Report; Wada Na Todo Abhiyan: New Delhi, India, 2017. [Google Scholar]
- Muttreja, P.; Singh, S. Family planning in India: The way forward. Indian J. Med. Res. 2018, 148 (Suppl. S1), S1. [Google Scholar]
- New, J.R.; Cahill, N.; Stover, J.; Gupta, Y.P.; Alkema, L. Levels and trends in contraceptive prevalence, unmet need, and demand for family planning for 29 states and union territories in India: A modelling study using the Family Planning Estimation Tool. Lancet Glob. Health 2017, 5, e350–e358. [Google Scholar] [CrossRef] [Green Version]
- Arokiasamy, P.; Shekhar, C.; Srinivasan, K.; Goli, S. Family welfare program in India: Expenditure vs performance. Econ. Political Wkly. 2011, 46, 127. [Google Scholar]
- Srinivasan, K. Population Concerns in India: Shifting Trends, Policies, and Programs; SAGE Publishing: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Chaurasia, A.R. Contraceptive use in India: A data mining approach. Int. J. Popul. Res. 2014, 2014, 1–11. [Google Scholar] [CrossRef]
- Government of India. Family Welfare Program in India: Year Book 1991–1992; Ministry of Health and Family Welfare, Department of Family Welfare: New Delhi, India, 1993.
- International Institute for Population Sciences (IIPS); ICF. National Family Health Survey (NFHS-4), 2015–2016; IIPS: Mumbai, India, 2017. [Google Scholar]
- United Nations. World Population Day—Ban Ki Moon; Annual Health Survey Fact Sheet; United Nations: New York, NY, USA, 2012. [Google Scholar]
- Mohanty, S.K.; Mishra, S.; Chatterjee, S.; Saggurti, N. Pattern and correlates of out-of-pocket payment (OOP) on female sterilization in India, 1990–2014. BMC Women’s Health 2020, 20, 13. [Google Scholar] [CrossRef] [PubMed]
- Dixit, A.; Averbach, S.; Yore, J.; Kully, G.; Ghule, M.; Battala, M.; Begum, S.; Johns, N.E.; Vaida, F.; Bharadwaj, P.; et al. A gender synchronized family planning intervention for married couples in rural India: Study protocol for the CHARM2 cluster randomized controlled trial evaluation. Reprod. Health 2019, 16, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Johns, N.E.; Dixit, A.; Ghule, M.; Begum, S.; Battala, M.; Kully, G.; Silverman, J.; Dehlendorf, C.; Raj, A.; Averbach, S. Validation of the Interpersonal Quality of Family Planning Scale in a rural Indian setting. Contraception 2020, 2, 100035. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, M.R.; Dwivedi, L.K. Changes in contraceptive use and method mix in India: 1992–1992 to 2015–2016. Sex. Reprod. Healthc. 2019, 19, 56–63. [Google Scholar] [CrossRef]
- Raj, A.; Ghule, M.; Ritter, J.; Battala, M.; Gajanan, V.; Nair, S.; Dasgupta, A.; Silverman, J.G.; Balaiah, D.; Saggurti, N. Cluster randomized controlled trial evaluation of a gender equity and family planning intervention for married men and couples in rural India. PLoS ONE 2016, 11, e0153190. [Google Scholar] [CrossRef] [Green Version]
- Ranjan, M.; Mozumdar, A.; Acharya, R.; Mondal, S.K.; Saggurti, N. Intra-household influence on contraceptive use among married Indian women: Evidence from the National Family Health Survey 2015–2016. SSM Popul. Health 2020, 11, 100603. [Google Scholar] [CrossRef]
- Singh, P.; Singh, K.K.; Singh, A.; Pandey, A. The levels and trends of contraceptive use before first birth in India (2015–2016): A cross-sectional analysis. BMC Public Health 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Mozumdar, A.; Acharya, R.; Mondal, S.K.; Shah, A.A.; Saggurti, N. India’s family planning market and opportunities for the private sector: An analysis using the total market approach. Int. J. Health Plan. Manag. 2019, .34, 1078–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Government of India. Family Welfare Program in India: Year Book 1997–1998; Ministry of Health and Family Welfare, Department of Family Welfare: New Delhi, India, 1999.
- Government of India. Financial Management Report; Ministry of Health and Family Welfare: New Delhi, India. Available online: https://nhm.gov.in/index4.php?lang=1&level=0&linkid=354&lid=441 (accessed on 10 March 2019).
- International Institute for Population Sciences (IIPS). National Family Health Survey (NFHS I) 1992–1993; IIPS: Mumbai, India, 1995. [Google Scholar]
- International Institute for Population Sciences. National Family Health Survey (NFHS 2), 1998–1999; IIPS: Mumbai, India, 2000. [Google Scholar]
- International Institute for Population Sciences (IIPS); Macro International. National Family Health Survey NFHS–3, 2005–2006; IIPS: Mumbai, India, 2007; Volume II. [Google Scholar]
- Cameron, A.C.; Trivedi, P.K. Econometric models based on count data. Comparisons and applications of some estimators and tests. J. Appl. Econom. 1986, 1, 29–53. [Google Scholar] [CrossRef]
- Retherford, R.D.; Choe, M.K. Statistical Models for Causal Analysis; Wiley: New York, NY, USA, 1993. [Google Scholar]
- Cates, W.; Karim, Q.A.; El-Sadr, W.; Haffner, D.W.; Kalema-Zikusoka, G.; Rogo, K.; Petruney, T.; Averill, E.M.D. Family planning and the millennium development goals. Science 2010, 329, 1603. [Google Scholar] [CrossRef] [Green Version]
- Miller, G.; Babiarz, K.S. Family Planning: Program Effects (No. w20586); National Bureau of Economic Research: Cambridge, MA, USA, 2014. [Google Scholar]
- Srinivasan, K.; Shekhar, C.; Arokiasamy, P. Reviewing reproductive and child health programs in India. Econ. Political Wkly. 2007, 42, 2931–2939. [Google Scholar]
- Zavier, F.; Padmadas, S.S. Use of a spacing method before sterilization among couples in Kerala, India. Int. Fam. Plan. Perspect. 2000, 26, 29–35. [Google Scholar] [CrossRef] [Green Version]
- Basu, A.M. Family planning and the emergency: An unanticipated consequence. Econ. Political Wkly. 1985, 422–425. [Google Scholar]
- De Oliveira, I.T.; Dias, J.G.; Padmadas, S.S. Dominance of sterilization and alternative choices of contraception in India: An appraisal of the socioeconomic impact. PLoS ONE 2014, 9, e86654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agrahari, K.; Mohanty, S.K.; Chauhan, R.K. Socio-Economic Differentials in Contraceptive Discontinuation in India. SAGE Open 2016, 6, 2158244016646612. [Google Scholar] [CrossRef] [Green Version]
- Government of India. Annual Report; Ministry of Health and Family Welfare: New Delhi, India. Available online: https://mohfw.gov.in/sites/default/files/56324455632156323214.pdf (accessed on 20 November 2019).
- Shah, I.H.; Santhya, K.G.; Cleland, J. Postpartum and Post-Abortion Contraception: From Research to Programs. Stud. Fam. Plan. 2015, 46, 343–353. [Google Scholar] [CrossRef]
- Prusty R., K. Use of contraceptives and unmet need for family planning among tribal women in India and selected hilly states. J. Health Popul. Nutr. 2014, 32, 342–355. [Google Scholar] [PubMed]
- Johri, L.; Panwar, D.S.; Lundgren, R. Introduction of the Standard Days Method in CARE-Indias Community-Based Reproductive Health Programs; Institute for Reproductive Health, Georgetown University: Washington, DC, USA, 2005. [Google Scholar]
- United Nations Population Fund. Assessment of Contraceptive Social Marketing Programme; Ministry of Health and Family Welfare, Government of India: New Delhi, India, 2015. [Google Scholar]
- Jain, M.L.; Chauhan, M.; Talwar, B. Role of private sector in family planning programme in Rajasthan, India-a rapid assessment. Int. J. Community Med. Public Health 2017, 3, 869–874. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Jain, A.K.; Aruldas, K.; Mozumdar, A.; Shukla, A.; Acharya, R.; Ram, F.; Saggurti, N. Is economic inequality in family planning in India associated with the private sector? J. Biosoc. Sci. 2019, 52, 1–12. [Google Scholar] [CrossRef]
- Singh, P.; Singh, K.K.; Singh, P. Factors explaining the dominion status of female sterilization in India over the past two decades (1992–2016): A multilevel study. PLoS ONE 2021, 16, e0246530. [Google Scholar] [CrossRef] [PubMed]
- Rana, M.J.; Goli, S. The road from ICPD to SDGs: Health returns of reducing the unmet need for family planning in India. Midwifery 2021, 103, 103107. [Google Scholar] [CrossRef] [PubMed]
- James, K.S.; Goli, S. Demographic changes in India: Is the country prepared for the challenge. Brown J. World Aff. 2016, 23, 169. [Google Scholar]




| States | Total | Urban | Rural | Public/Private Ratio (2015–2016) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1992–1993 | 1998–1999 | 2005–2006 | 2015–2016 | 1992–1993 | 1998–1999 | 2005–2006 | 2015–2016 | 1992–1993 | 1998–1999 | 2005–2006 | 2015–2016 | Total | Urban | Rural | |
| All India | 79.0 | 76.0 | 69.8 | 68.7 | 62.4 | 60.1 | 55.6 | 56.7 | 87.0 | 83.2 | 77.6 | 75.5 | 2.2 | 1.3 | 3.1 |
| Andhra Pradesh | 78.1 | 78.5 | 76.6 | 74.7 | 61.8 | 64.9 | 67.2 | 64.7 | 85.6 | 83.4 | 81.0 | 78.9 | 2.9 | 1.8 | 3.7 |
| Arunachal Pradesh | 85.7 | 72.2 | 63.1 | 59.9 | 72.2 | 64.3 | 49.3 | 52.2 | 89.6 | 74.2 | 69.0 | 62.0 | 1.5 | 1.1 | 1.6 |
| Assam | 72.2 | 63.7 | 44.2 | 40.7 | 55.8 | 46.8 | 28.1 | 30.5 | 76.5 | 65.5 | 49.3 | 42.4 | 0.7 | 0.4 | 0.7 |
| Bihar | 76.1 | 76.9 | 53.4 | 63.1 | 55.0 | 56.0 | 39.5 | 51.3 | 83.7 | 80.9 | 56.9 | 65.5 | 1.7 | 1.0 | 1.9 |
| Chandigarh | — | — | — | 54.8 | — | — | — | 53.2 | — | — | — | 86.7 | 1.2 | 1.1 | 6.5 |
| Delhi | 45.2 | 51.9 | 43.9 | 51.8 | 45.2 | 50.8 | 42.0 | 51.8 | 46.2 | 63.7 | 65.7 | 60.7 | 1.1 | 1.0 | 1.5 |
| Gujarat | 75.5 | 72.0 | 70.6 | 70.0 | 63.6 | 52.2 | 53.8 | 53.7 | 82.3 | 86.7 | 83.5 | 82.0 | 2.4 | 1.2 | 4.6 |
| Goa | 72.0 | 68.3 | 58.9 | 50.5 | 62.7 | 62.8 | 51.9 | 50.8 | 80.7 | 72.9 | 69.3 | 48.9 | 1.0 | 1.0 | 0.9 |
| Himachal Pradesh | 90.6 | 91.7 | 84.6 | 81.0 | 75.2 | 68.4 | 61.3 | 66.2 | 92.6 | 94.2 | 87.2 | 82.4 | 4.3 | 2.0 | 4.7 |
| Haryana | 83.1 | 79.5 | 68.1 | 69.1 | 65.8 | 59.2 | 51.4 | 58.3 | 90.1 | 87.9 | 75.3 | 75.5 | 2.2 | 1.4 | 3.1 |
| Jharkhand | — | — | 57.4 | 65.5 | — | — | 47.4 | 50.9 | — | — | 63.7 | 71.3 | 1.9 | 1.0 | 2.5 |
| Jammu and Kashmir a | 81.1 | 68.5 | 57.9 | 65.5 | 62.8 | 60.7 | 52.3 | 60.3 | 86.2 | 72.0 | 61.2 | 68.7 | 1.9 | 1.5 | 2.2 |
| Karnataka | 83.4 | 85.3 | 82.1 | 83.3 | 68.9 | 70.7 | 69.0 | 73.4 | 90.9 | 93.3 | 89.8 | 89.6 | 5.0 | 2.8 | 8.8 |
| Kerala | 74.9 | 66.4 | 61.3 | 57.8 | 72.1 | 63.4 | 57.9 | 54.5 | 76.1 | 67.4 | 63.1 | 60.7 | 1.4 | 1.2 | 1.5 |
| Meghalaya | 68.2 | 47.3 | 42.5 | 42.9 | 58.5 | 33.5 | 40.7 | 44.1 | 73.5 | 61.8 | 44.1 | 42.6 | 0.8 | 0.8 | 0.7 |
| Maharashtra | 74.8 | 75.2 | 68.4 | 69.7 | 55.2 | 59.1 | 52.0 | 55.3 | 87.8 | 85.5 | 83.2 | 81.8 | 2.3 | 1.2 | 4.5 |
| Madhya Pradesh | 89.2 | 86.6 | 86.1 | 85.6 | 74.9 | 69.8 | 65.2 | 68.1 | 94.9 | 94.2 | 94.2 | 92.6 | 6.0 | 2.2 | 12.8 |
| Manipur | 82.3 | 76.9 | 51.4 | 47.6 | 80.4 | 69.7 | 43.4 | 43.2 | 83.7 | 81.7 | 55.4 | 50.4 | 0.9 | 0.8 | 1.0 |
| Mizoram | 90.6 | 81.0 | 83.9 | 67.9 | 87.4 | 72.8 | 80.5 | 59.9 | 94.0 | 92.8 | 88.6 | 79.1 | 2.1 | 1.5 | 3.9 |
| Nagaland | 70.7 | 57.7 | 47.2 | 59.7 | 68.9 | 59.5 | 40.9 | 52.6 | 71.6 | 56.8 | 51.4 | 64.6 | 1.5 | 1.1 | 1.8 |
| Orissa | 93.4 | 88.5 | 78.1 | 76.0 | 79.7 | 74.2 | 59.5 | 58.0 | 96.8 | 91.6 | 82.4 | 80.1 | 3.2 | 1.4 | 4.1 |
| Punjab | 77.1 | 64.3 | 61.4 | 63.7 | 62.7 | 40.3 | 43.5 | 52.1 | 83.1 | 75.2 | 70.7 | 71.2 | 1.8 | 1.1 | 2.5 |
| Rajasthan | 92.3 | 86.3 | 80.8 | 76.9 | 85.6 | 73.3 | 62.3 | 59.6 | 95.1 | 91.8 | 91.8 | 83.2 | 3.4 | 1.5 | 4.9 |
| Sikkim | — | 77.9 | 65.4 | 74.9 | — | 76.3 | 50.8 | 55.0 | — | 78.2 | 69.1 | 81.6 | 2.9 | 1.2 | 4.5 |
| Tamil Nadu | 78.0 | 73.6 | 72.0 | 77.2 | 63.3 | 65.0 | 65.7 | 70.8 | 85.8 | 78.9 | 77.4 | 84.0 | 3.4 | 2.4 | 5.3 |
| Tripura | 75.3 | 71.4 | 53.2 | 39.1 | 69.6 | 57.9 | 35.0 | 40.3 | 77.4 | 75.2 | 57.0 | 38.6 | 0.6 | 0.7 | 0.6 |
| Uttarakhand | — | — | 65.0 | 63.3 | — | — | 41.3 | 45.7 | — | — | 74.2 | 72.8 | 1.7 | 0.8 | 2.7 |
| Uttar Pradesh | 74.5 | 71.1 | 58.4 | 53.8 | 55.2 | 49.8 | 40.3 | 33.9 | 83.6 | 81.7 | 67.9 | 62.8 | 1.2 | 0.5 | 1.7 |
| West Bengal | 79.6 | 69.5 | 64.2 | 57.4 | 57.9 | 52.6 | 51.8 | 44.0 | 87.6 | 74.6 | 69.1 | 62.7 | 1.4 | 0.8 | 1.7 |
| Characteristic | Any Modern Contraceptives | Female Sterilization | ||||||
|---|---|---|---|---|---|---|---|---|
| 1992–1993 | 1998–1999 | 2005–2006 | 2015–2016 | 1992–1993 | 1998–1999 | 2005–2006 | 2015–2016 | |
| Wealth status | ||||||||
| Poorest | 90.2 | 92.3 | 87.6 | 82.0 | 96.1 | 96.1 | 95.4 | 92.5 |
| Poorer | 89.6 | 88.7 | 82.6 | 78.1 | 94.9 | 93.0 | 91.3 | 91.2 |
| Middle | 88.3 | 83.3 | 79.3 | 75.9 | 92.4 | 89.4 | 88.7 | 87.3 |
| Richer | 83.1 | 71.7 | 68.2 | 67.6 | 87.0 | 80.8 | 80.4 | 79.5 |
| Richest | 68.3 | 48.3 | 45.1 | 47.4 | 71.8 | 63.7 | 63.0 | 61.8 |
| Place of residence | ||||||||
| Urban | 62.4 | 60.1 | 55.6 | 56.7 | 78.9 | 74.5 | 73.6 | 71.9 |
| Rural | 89.0 | 83.2 | 77.6 | 75.5 | 92.1 | 89.4 | 87.5 | 87.0 |
| Education | ||||||||
| No education | 90.1 | 88.9 | 83.4 | 83.6 | 93.9 | 92.6 | 90.6 | 90.8 |
| Primary | 80.9 | 79.4 | 76.4 | 76.6 | 87.2 | 86.3 | 86.2 | 87.3 |
| Secondary | 61.5 | 63.7 | 57.1 | 61.6 | 79.7 | 75.3 | 72.6 | 75.7 |
| Higher | 28.2 | 33.4 | 22.7 | 30.4 | 65.3 | 51.2 | 42.8 | 45.3 |
| Indicators | Any Modern Method | Any Modern Method for Spacing | ||||||
|---|---|---|---|---|---|---|---|---|
| Model1 (Re) | Model 2 (Fe) | Model 3 (fe) | Model 4 (Fe) | |||||
| β | p-Value | Β | p-Value | Β | p-Value | β | p-Value | |
| Log of per capita FWE | −4.886 (2.544) | 0.055 | −2.446 (1.297) | 0.064 | ||||
| Share of FWE in PHE | 0.076 (0.133) | 0.565 | 0.118 (0.079) | 0.139 | ||||
| Under five mortality | −0.087 (0.057) | 0.126 | −0.040 (0.055) | 0.456 | −0.0006 (0.032) | 0.984 | 0.001 (0.033) | 0.979 |
| ANC (At least 4 visits) | 0.096 (0.080) | 0.229 | 0.087 (0.087) | 0.316 | 0.190 (0.051) | 0.000 | 0.195 (0.052) | 0.000 |
| Child marriages | −0.081 (0.089) | 0.358 | −0.351 (0.093) | 0.000 | 0.019 (0.053) | 0.721 | 0.022 (0.056) | 0.695 |
| Female literacy rate | 0.123 (0.103) | 0.229 | 0.081 (0.112) | 0.474 | 0.039 (0.063) | 0.534 | 0.035 (0.067) | 0.608 |
| Urban population | 0.043 (0.113) | 0.700 | 0.155 (0.220) | 0.483 | −0.093 (0.125) | 0.456 | −0.138 (0.131) | 0.298 |
| Sex ratio at Birth (SRB) | −0.007 (0.014) | 0.587 | 0.009 (0.013) | 0.480 | 0.012 (0.007) | 0.109 | 0.010 (0.008) | 0.194 |
| SC/ST population | −0.161 (0.082) | 0.048 | −0.080 (0.136) | 0.556 | 0.038 (0.077) | 0.615 | 0.034 (0.081) | 0.666 |
| Muslim population | −0.080 (0.126) | 0.522 | −0.108 (0.142) | 0.450 | 0.019 (0.080) | 0.805 | 0.021 (0.085) | 0.801 |
| Log of per capita NSDP | −25.775 (6.062) | 0.000 | −1.747 (3.611) | 0.630 | ||||
| Constant | 492.311 (302.593) | 0.104 | −1175.57 (654.710) | 0.077 | −214.91 (269.31) | 0.428 | −445.584 (390.115) | 0.258 |
| N | 102 | 102 | 102 | 102 | ||||
| sigma_u | 9.466 | 14.252 | 8.293 | 8.752 | ||||
| sigma_e | 5.661 | 5.156 | 3.023 | 3.072 | ||||
| rho | 0.736 | 0.884 | 0.882 | 0.890 | ||||
| Variables | OR | p-Value | (95% CI) |
|---|---|---|---|
| Type of contraceptive methods | |||
| Female sterilization | Ref. | ||
| Pill | 0.05 | 0.000 | (0.05 to 0.06) |
| IUD | 0.44 | 0.000 | (0.41 to 0.46) |
| Condom | 0.04 | 0.000 | (0.04 to 0.04) |
| Other | 0.10 | 0.000 | (0.08 to 0.11) |
| State | |||
| Andhra Pradesh | 0.26 | 0.000 | (0.23 to 0.28) |
| North East | 0.39 | 0.000 | (0.36 to 0.42) |
| Bihar | 0.12 | 0.000 | (0.11 to 0.13) |
| Chhattisgarh | 0.86 | 0.002 | (0.77 to 0.95) |
| Gujarat | 0.46 | 0.000 | (0.42 to 0.51) |
| Haryana | 1.00 | 0.927 | (0.91 to 1.08) |
| Himachal Pradesh | 2.34 | 0.000 | (2.06 to 2.65) |
| Jammu and Kashmir | 1.18 | 0.002 | (1.06 to 1.30) |
| Jharkhand | 0.18 | 0.000 | (0.16 to 0.19) |
| Karnataka | 0.57 | 0.000 | (0.52 to 0.62) |
| Kerala | 0.28 | 0.000 | (0.25 to 0.30) |
| Madhya Pradesh | 1.18 | 0.000 | (1.09 to 1.29) |
| Maharashtra | 0.52 | 0.000 | (0.48 to 0.57) |
| Delhi | 0.86 | 0.044 | (0.75 to 1.00) |
| Odisha | 0.97 | 0.467 | (0.88 to 1.06) |
| Punjab | Ref. | ||
| Rajasthan | 0.83 | 0.000 | (0.77 to 0.91) |
| Tamil Nadu | 0.39 | 0.000 | (0.36 to 0.42) |
| Uttar Pradesh | 0.35 | 0.000 | (0.32 to 0.38) |
| Uttarakhand | 1.02 | 0.769 | (0.92 to 1.12) |
| West Bengal | 0.46 | 0.000 | (0.42 to 0.51) |
| Telangana | 0.19 | 0.000 | (0.17 to 0.21) |
| Goa and UTs | 0.75 | 0.000 | (0.67 to 0.84) |
| Age of respondent (years) | |||
| 15–21 | Ref. | ||
| 22–34 | 1.07 | 0.058 | (1.00 to 1.15) |
| 35+ | 1.11 | 0.007 | (1.03 to 1.19) |
| Age at marriage (years) | |||
| <14 | Ref. | ||
| 15–19 | 0.96 | 0.025 | (0.92 to 0.99) |
| 20–24 | 0.87 | 0.000 | (0.84 to 0.91) |
| 25–29 | 0.92 | 0.012 | (0.86 to 0.98) |
| 30+ | 0.98 | 0.730 | (0.85 to 1.12) |
| Not reported | 1.33 | 0.000 | (1.23 to 1.44) |
| Place of residence | |||
| Urban | Ref. | ||
| Rural | 1.32 | 0.000 | (1.29 to 1.36) |
| Religion | |||
| Hindu | Ref. | ||
| Muslim | 0.70 | 0.000 | (0.67 to 0.73) |
| Other | 1.06 | 0.020 | (1.01 to 1.11) |
| Caste | |||
| Others | Ref. | ||
| SC | 1.35 | 0.000 | (1.30 to 1.39) |
| ST | 1.88 | 0.000 | (1.79 to 197) |
| OBC | 0.95 | 0.117 | (0.89 to 1.01) |
| Wealth Quintiles | |||
| Poorest | Ref. | ||
| Poorer | 0.80 | 0.000 | (0.77 to 0.84) |
| Middle | 0.68 | 0.000 | (0.64 to 0.71) |
| Richer | 0.49 | 0.000 | (0.47 to 0.52) |
| Richest | 0.27 | 0.000 | (0.26 to 0.29) |
| Respondent’s education | |||
| Illiterate | Ref. | ||
| Primary | 0.88 | 0.000 | (0.85 to 0.92) |
| Secondary | 0.68 | 0.000 | (0.66 to 0.70) |
| Higher | 0.37 | 0.000 | (0.35 to 0.39) |
| Occupation | |||
| Not working | Ref. | ||
| Working | 1.23 | 0.000 | (1.15 to 1.32) |
| Don’t know/ Not reported | 1.08 | 0.000 | (1.05 to 1.12) |
| Exposure to mass media | |||
| No | Ref. | ||
| Partial | 0.98 | 0.160 | (0.95 to 1.01) |
| Full | 1.05 | 0.041 | (1.00 to 1.10) |
| Constant | 20.62 | 0.000 | (18.25 to 23.30) |
| N | 228799 | ||
| Chi-square test | 96241.23 | ||
| P-value | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Misra, S.; Goli, S.; Rana, M.J.; Gautam, A.; Datta, N.; Nanda, P.; Verma, R. Family Welfare Expenditure, Contraceptive Use, Sources and Method-Mix in India. Sustainability 2021, 13, 9562. https://0-doi-org.brum.beds.ac.uk/10.3390/su13179562
Misra S, Goli S, Rana MJ, Gautam A, Datta N, Nanda P, Verma R. Family Welfare Expenditure, Contraceptive Use, Sources and Method-Mix in India. Sustainability. 2021; 13(17):9562. https://0-doi-org.brum.beds.ac.uk/10.3390/su13179562
Chicago/Turabian StyleMisra, Sheuli, Srinivas Goli, Md Juel Rana, Abhishek Gautam, Nitin Datta, Priya Nanda, and Ravi Verma. 2021. "Family Welfare Expenditure, Contraceptive Use, Sources and Method-Mix in India" Sustainability 13, no. 17: 9562. https://0-doi-org.brum.beds.ac.uk/10.3390/su13179562