
Applying Lean Healthcare to Improve the Discharge Process in a Mexican Academic Medical Center


Abstract
:1. Introduction
2. Literature Review
3. Materials and Methods
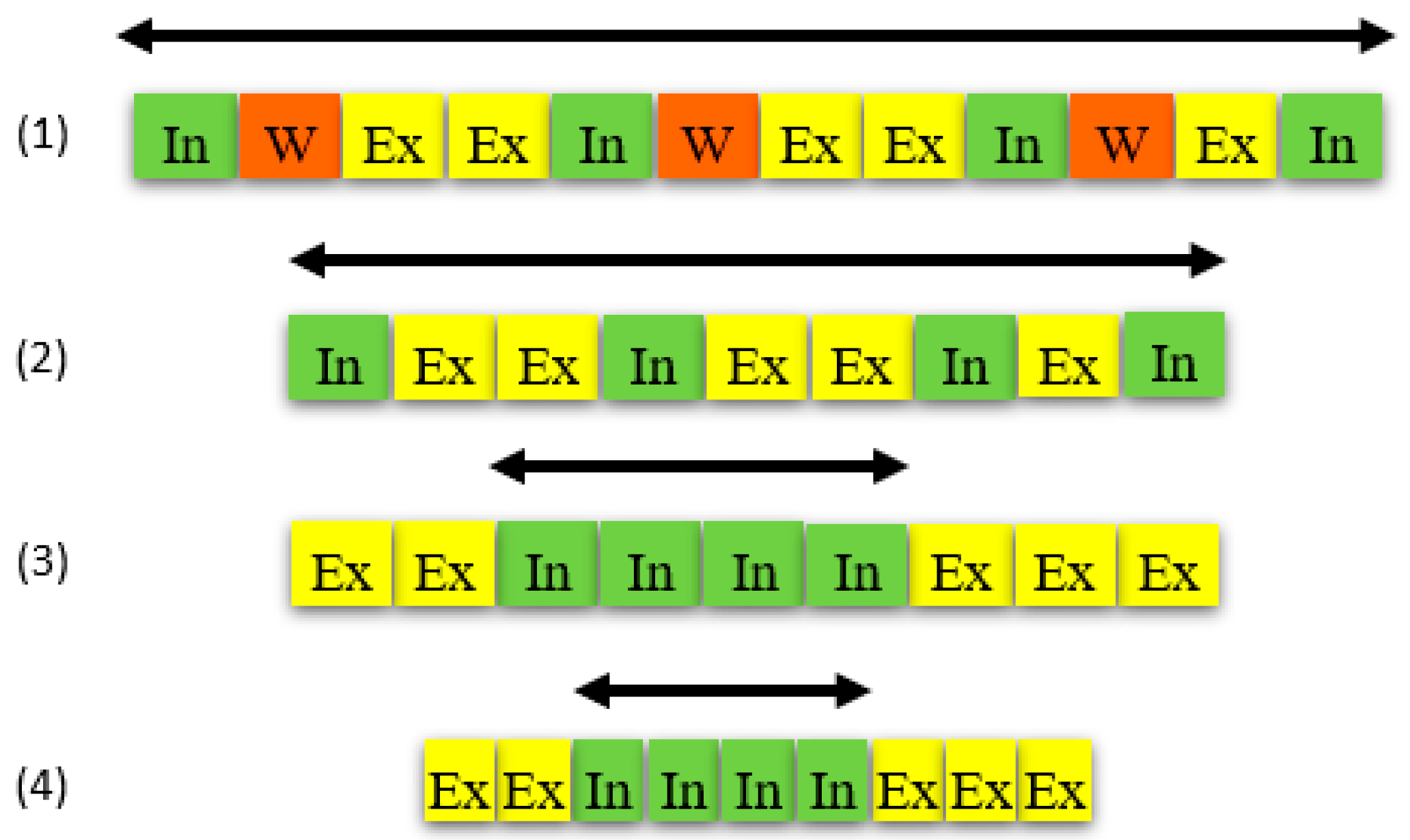
- Value-added external activities that can take place anytime but should occur before or after the process;
- Value-added internal activities that occur during the process and should be made external when possible;
- Non-value-added or waste activities that should be eliminated (or at least reduced).
- Identifying and separating internal, external, and wasteful activities.
- Eliminating wasteful activities.
- Converting internal to external activities.
- Streamlining all aspects of the process.
4. Results
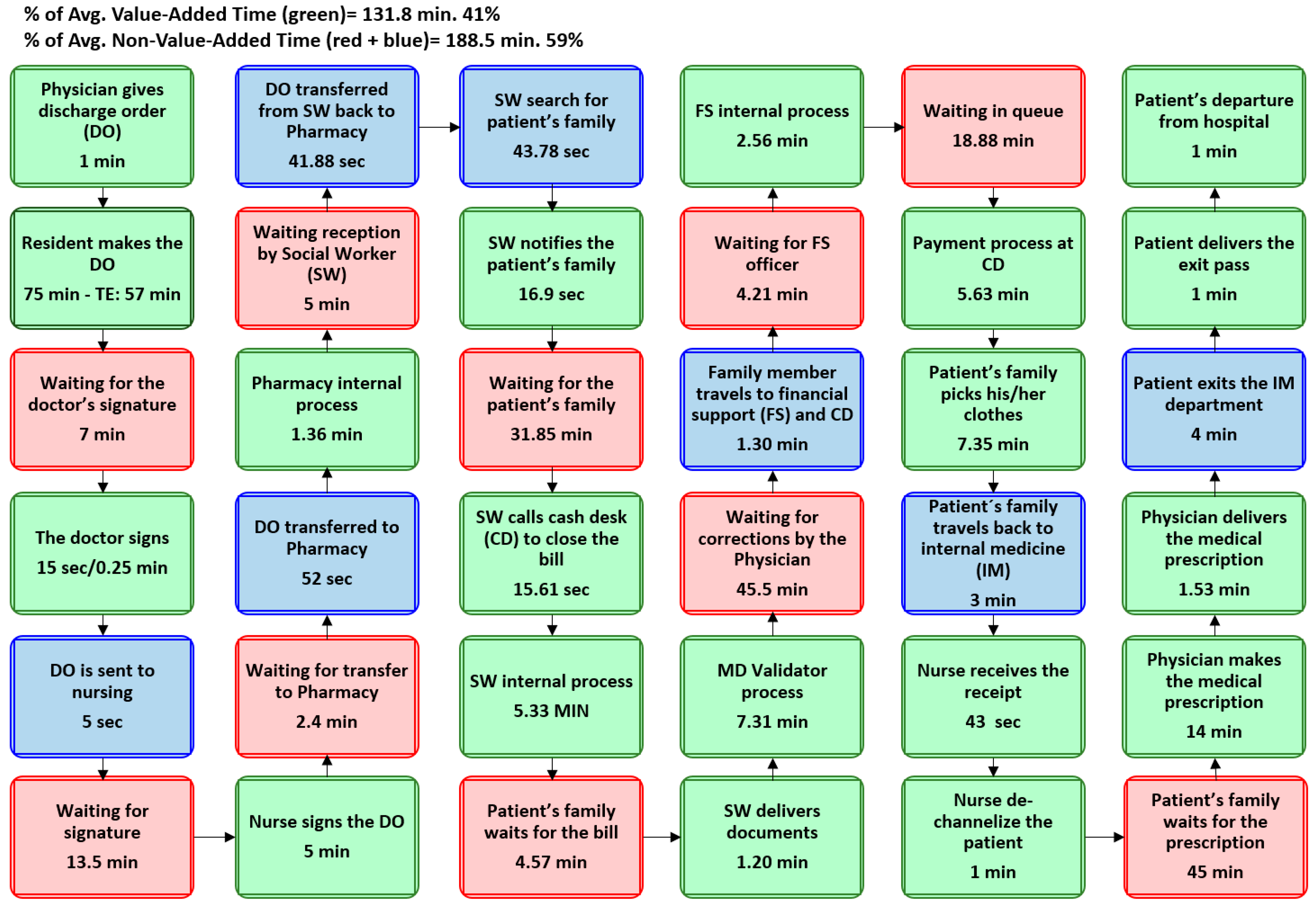
4.1. Diagnostic
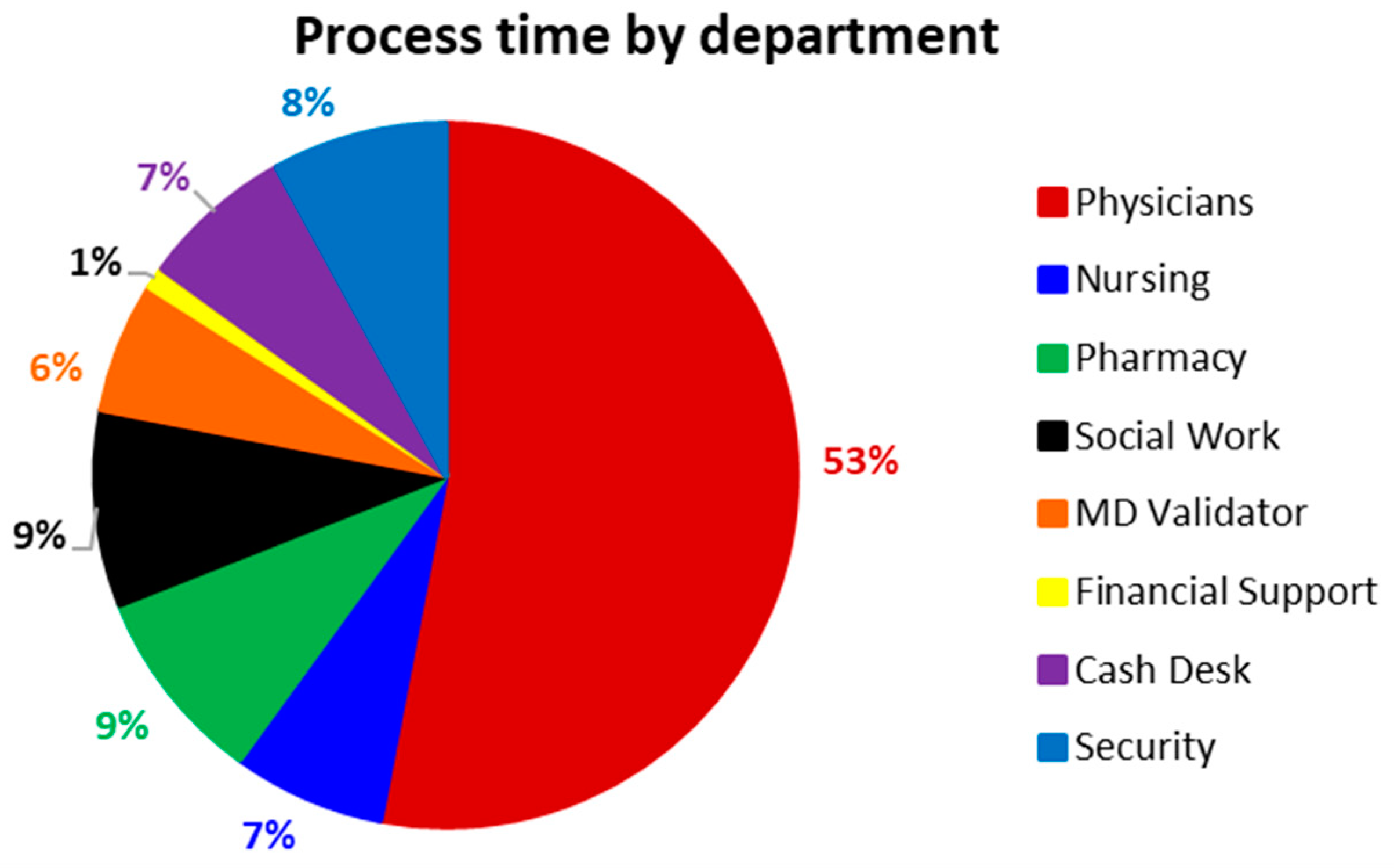
- Physicians, including residents, interns, and externs (third-year medical students).
- Nursing.
- Pharmacy.
- Social workers.
- Medicine department (MD) validators who check the coverage according to the public medical insurance called “seguro popular”.
- Financial support (if needed).
- Cash desk.
- Security
4.2. Analysis
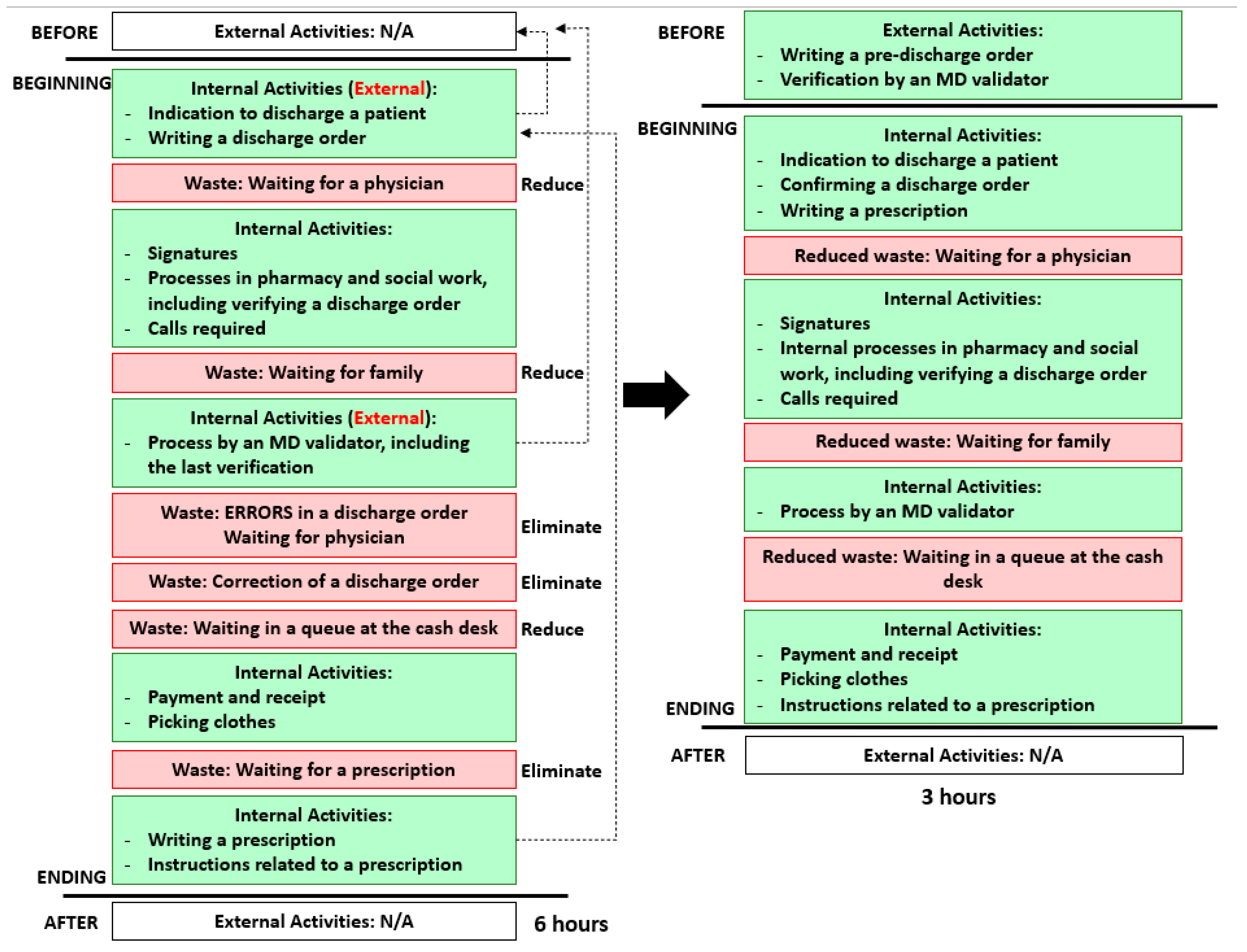
4.3. Improvement
- Eliminating wasteful activities: The main wastes are associated with the physician throughout the entire process. While the main concerns are the large number of errors found in DOs, their correction, and the long waiting times for the prescription, these also have an impact on the other sources of waste in a systemic way. These are reduced in the following step.
- Converting internal to external activities: Two key activities that are carried out during the process (internal) should occur before (external): pre-filling the DO, ideally the day before, and its pre-evaluation and fix by the MD validator early in the morning (first two dotted lines). This will reduce the number of defective orders, as well as the corresponding waiting times.
- Streamlining all aspects of the process: The prescription can be provided at the beginning of the process, along with the DO (third dotted line). This and the previous changes (step 3) eliminate rework and reduce waiting times, given that physicians and family members are still around during the morning (when required), and the cash desk is reached during the first working shift.
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brackett, T.; Comer, L.; Whichello, R. Do Lean Practices Lead to More Time at the Bedside? J. Healthc. Qual. 2013, 35, 7–14. [Google Scholar] [CrossRef]
- Graban, M. Lean Hospitals: Improving Quality, Patient Safety, and Employee Engagement, 3rd ed.; CRC Press: Boca Raton, FL, USA, 2016. [Google Scholar]
- Costa, L.B.M.; Folho, M.G. Lean healthcare: Review, classification and analysis of literature. Prod. Plan. Control 2016, 27, 823–836. [Google Scholar] [CrossRef]
- Peimbert-García, R.E.; Matis, T.; Cuevas-Ortuño, J.; Nucamendi-Guillen, S.M. Systematic Review of Literature on Lean and Six Sigma in Healthcare and Directions for Future Research. In Proceedings of the 10th International Conference on Industrial Engineering and Operations Management (IEOM), Dubai, United Arab Emirates, 10–12 March 2020. [Google Scholar]
- Da Silva, I.B.; Seraphim, E.C.; Agostinho, O.L.; Lima, J.O.F.; Batalha, G.F. Lean office in health organization in the Brazilian Army. Int. J. Lean Six Sigma 2015, 6, 2–16. [Google Scholar] [CrossRef]
- Godinho Filho, M.G.; Boschi, A.; Rentes, A.F.; Thurer, M.; Bertani, T.M. Improving hospital performance by use of lean techniques: An action research project in Brazil. Qual. Eng. 2015, 27, 196–211. [Google Scholar] [CrossRef]
- Peimbert-García, R.E.; Matis, T.; Beltran-Godoy, J.H.; Garay-Rondero, C.L.; Vicencio-Ortiz, J.C.; López-Soto, D. Assessing the state of lean and six sigma practices in healthcare in Mexico. Leadersh. Health Serv. 2019, 32, 644–662. [Google Scholar] [CrossRef]
- Ortíz-Barrios, M.A.; Escorcia-Caballero, J.P.; Sánchez-Sánchez, F.; De Felice, F.; Petrillo, A. Efficiency Analysis of Integrated Public Hospital Networks in Outpatient Internal Medicine. J. Med. Syst. 2017, 41, 163. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, K.C.; Does, R.J.M. Quality Quandaries: Lean Nursing. Qual. Eng. 2010, 23, 94–99. [Google Scholar] [CrossRef]
- Fischman, D. Applying Lean Six Sigma methodologies to improve efficiency, timeliness of care, and quality of care in an internal medicine residency clinic. Qual. Manag. Health Care 2010, 19, 201–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niemeijer, G.C.; Trip, A.; Ahaus, K.T.; Does, R.J.; Wendt, K.W. Quality in trauma care: Improving the discharge procedure of patients by means of Lean Six Sigma. J. Trauma Acute Care Surg. 2010, 69, 614–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Banna, M.A. Improving Patients Discharge Process in Hospitals by using Six Sigma Approach. World Acad. Sci. Eng. Technol. 2012, 6, 1378–1387. [Google Scholar]
- Udayai, K.; Kumar, P. Implementing Six Sigma to improve hospital discharge process. Int. J. Pharm. Sci. Res. 2012, 3, 4528–4532. [Google Scholar] [CrossRef]
- Vijay, S.A. Reducing and Optimizing the Cycle Time of Patients Discharge Process in a Hospital Using Six Sigma DMAIC Approach. Int. J. Qual. Res. 2014, 8, 169–182. [Google Scholar]
- McDermott, C.M.; Venditti, F.J. Implementing lean in knowledge work: Implications from a study of the hospital discharge planning process. Oper. Manag. Res. 2015, 8, 118–130. [Google Scholar] [CrossRef]
- Molla, M.; Warren, D.S.; Stewart, S.L.; Stocking, J.; Johl, H.; Sinigayan, V. A Lean Six Sigma Quality Improvement Project Improves Timeliness of Discharge from the Hospital. Jt. Comm. J. Qual. Patient Saf. 2018, 44, 401–412. [Google Scholar] [CrossRef] [PubMed]
- Zepeda-Lugo, C.; Tlapa, D.; Baez-Lopez, Y.; Limon-Romero, J.; Ontiveros, S.; Perez-Sanchez, A.; Tortorella, G. Assessing the Impact of Lean Healthcare on Inpatient Care: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 5609. [Google Scholar] [CrossRef]
- Womack, J.P.; Jones, D.T. Lean Thinking: Banish Waste and Create Wealth in Your Corporation, 2nd ed.; Free Press: New York, NY, USA, 2003. [Google Scholar]
- Peimbert-García, R.E. Analysis and Evaluation of Reviews on Lean and Six Sigma in Healthcare. Qual. Manag. Health Care 2019, 28, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Senna, P.; Gomes, A.; Monteiro, A.; Pinha, D. Study on Techniques and Tools Used in Lean Healthcare Implementation: A Literature Review. Braz. J. Oper. Prod. Manag. 2016, 13, 406–420. [Google Scholar] [CrossRef]
- Costa, L.B.; Filho, M.G.; Rentes, A.F.; Bertani, T.M.; Mardegan, R. Lean healthcare in developing countries: Evidence from Brazilian hospitals. Int. J. Health Plan. Manag. 2017, 32, 99–120. [Google Scholar] [CrossRef] [PubMed]
- Hamid, S.; Jan, F.A.; Rashid, H.; Jalali, S. Study of hospital discharge process viz a viz prescribed NABH standards. Int. J. Contemp. Med. Res. 2018, 5, H1–H4. [Google Scholar] [CrossRef]
- Chen, L.M.; Freitag, M.H.; Franco, M.; Sullivan, C.D.; Dickson, C.; Brancati, F.L. Natural history of late discharges from a general medical ward. J. Hosp. Med. 2009, 4, 226–233. [Google Scholar] [CrossRef]
- Breslin, S.E.; Hamilton, K.M.; Paynter, J. Deployment of Lean Six Sigma in care coordination: An improved discharge process. Prof. Case Manag. 2014, 19, 77–83. [Google Scholar] [CrossRef] [Green Version]
- Van Rossum, L.; Aij, K.H.; Simons, F.E.; van der Eng, N.; Ten Have, W.D. Lean healthcare from a change management perspective. J. Health Organ. Manag. 2016, 30, 475–493. [Google Scholar] [CrossRef]
- Henrique, D.B.; Filho, M.G. A systematic literature review of empirical research in Lean and Six Sigma in healthcare. Total Qual. Manag. Bus. Excell. 2020, 31, 429–449. [Google Scholar] [CrossRef]
- Gabow, P.A.; Goodman, P.L. The Lean Prescription: Powerful Medicine for Our Ailing Healthcare System; CRC Press: New York, NY, USA, 2014. [Google Scholar]
- Dillon, A.P.; Shingo, S. A Revolution in Manufacturing: The SMED System; CRC Press: New York, NY, USA, 1985. [Google Scholar]
- Meguerditchian, A.N.; Krotneva, S.; Reidel, K.; Huang, A.; Tamblyn, R. Medication reconciliation at admission and discharge: A time and motion study. BMC Health Serv. Res. 2013, 13, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Allen, T.T.; Tseng, S.H.; Swanson, K.; McClay, M.A. Improving the Hospital Discharge Process with Six Sigma Methods. Qual. Eng. 2009, 22, 13–20. [Google Scholar] [CrossRef]
- Kim, C.S.; Spahlinger, D.A.; Kin, J.M.; Coffey, R.J.; Billi, J.E. Implementation of Lean Thinking: One Health System’s Journey. Jt. Comm. J. Qual. Patient Saf. 2009, 35, 406–413. [Google Scholar] [CrossRef]
- Arbune, A.; Wackerbarth, S.; Allison, P.; Conigliaro, J. Improvement through Small Cycles of Change: Lessons from an Academic Medical Center Emergency Department. J. Healthc. Qual. 2015, 39, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.S.; Lukela, M.P.; Parekh, V.I.; Mangrulkar, R.S.; Del Valle, J.; Spahlinger, D.A.; Billi, J.E. Teaching internal medicine residents quality improvement and patient safety: A lean thinking approach. Am. J. Med. Qual. 2010, 25, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Weigel, C.; Suen, W.; Gupte, G. Using lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am. J. Med. Qual. 2013, 28, 392–399. [Google Scholar] [CrossRef]
- Stelson, P.; Hille, J.; Eseonu, C.; Doolen, T. What drives continuous improvement project success in healthcare? Int. J. Health Care Qual. Assur. 2017, 30, 43–57. [Google Scholar] [CrossRef]
- Hallam, C.R.A.; Contreras, C. Lean healthcare: Scale, scope and sustainability. Int. J. Health Care Qual. Assur. 2018, 31, 684–696. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Area | Total Staff Members | Staff Members per Shift | |
|---|---|---|---|
| First: 7 a.m.–2 p.m. | Second: 2 p.m.–9 p.m. | ||
| Interns | 7 | 5 | 2 |
| Externs | 30 | 27 | 3 |
| Residents | 7 | 5 | 2 |
| Nursing (men) | 11 | 6 | 5 |
| Nursing (women) | 6 | 3 | 3 |
| Social Workers | 2 | 1 | 1 |
| Pharmacy | 3 | 2 | 1 |
| MD Validators | 3 | 1 | 2 1 |
| Cash Desk | 4 | 3 1 | 1 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peimbert-García, R.E.; Gutiérrez-Mendoza, L.M.; García-Reyes, H. Applying Lean Healthcare to Improve the Discharge Process in a Mexican Academic Medical Center. Sustainability 2021, 13, 10911. https://0-doi-org.brum.beds.ac.uk/10.3390/su131910911
Peimbert-García RE, Gutiérrez-Mendoza LM, García-Reyes H. Applying Lean Healthcare to Improve the Discharge Process in a Mexican Academic Medical Center. Sustainability. 2021; 13(19):10911. https://0-doi-org.brum.beds.ac.uk/10.3390/su131910911
Chicago/Turabian StylePeimbert-García, Rodrigo E., Luis Meave Gutiérrez-Mendoza, and Heriberto García-Reyes. 2021. "Applying Lean Healthcare to Improve the Discharge Process in a Mexican Academic Medical Center" Sustainability 13, no. 19: 10911. https://0-doi-org.brum.beds.ac.uk/10.3390/su131910911