
Back and Forth on Sustainable Development: A Focus on Healthcare Organisations




1
Department of Economics and Management, University of Ferrara, Via Voltapaletto 11, 44121 Ferrara, Italy
2
Department of Management, University of Bergamo, Via dei Caniana 2, 24127 Bergamo, Italy
*
Author to whom correspondence should be addressed.
Sustainability 2022, 14(9), 4958; https://0-doi-org.brum.beds.ac.uk/10.3390/su14094958
Submission received: 8 March 2022
/
Revised: 13 April 2022
/
Accepted: 15 April 2022
/
Published: 20 April 2022
(This article belongs to the Special Issue Sustainability Management in the Healthcare Sector)
Abstract
:The sustainability of healthcare systems represents a relevant target of the 2030 Sustainable Development Goals Agenda. Nevertheless, academic research has neglected to study healthcare systems when focusing on the transition toward sustainable healthcare. This study addresses this gap by investigating the implementation of the sustainable development (SD) principle in the Italian healthcare system, in light of international and national institutional discourses on SD. A questionnaire-based survey has been directed to the General Directors (GDs) of government-funded healthcare orgsanisations to investigate their perceptions about the SD principle applied to healthcare, their strategic planning for SD, their implemented projects for sustainability and the intellectual capital factors that influence the latter’s implementation. The study was conducted in two waves: a first survey was administered in 2016, with a second one in 2021. We used content analysis to identify the potential differences emerging over time in GDs’ perceptions in light of the changes in the institutional discourse; we then assessed the differences over time in the perceived contribution of intellectual capital factors to the implementation of sustainability actions. Results show a substantial decrease in strategic planning for sustainability, as well as in the volume of sustainability projects implemented, as organisations were found to be less involved in implementing SD strategies and projects in 2021 than in 2016. Policies at the country level have mainly focused on balancing cost containment with quality targets, leaving the environmental dimension of sustainability and its connection with healthcare with limited guidelines. Regarding intellectual capital factors, organisational culture and technologies are increasingly perceived as enablers of SD; nevertheless, further studies are needed to deepen their effective contribution to sustainable healthcare.
1. Introduction
Healthcare sustainability is becoming a more and more relevant target to achieve in our society, not only considering the need to implement responsive healthcare services while increasing the efficiency of healthcare organisations (HCOs), but also considering that implementing environmental strategies can contribute to healthier environments and lives and generate important cost-benefits for healthcare systems [1].
Sustainable development (SD) has been defined as the “development that meets the needs of the present without compromising the ability of future generations to meet their own needs” [2]. This definition applied to the healthcare context has meant the optimisation of the use of resources in order to improve the quality of healthcare and to provide better outcomes. Nevertheless, this misleading cycle that sees economic and financial sustainability as sufficient conditions to guarantee the viability of healthcare systems has been criticised, as it neglects sustainability as a wicked issue in complex adaptive systems, such as the healthcare ones [3,4,5,6,7,8,9]. Consequently, the main label attributed to SD has been related to austerity measures to recover efficiency [10], to the detriment of other dimensions of sustainability, such as social, political and environmental sustainability [3]. Furthermore, the meaning of sustainable healthcare, along with interventions that may support sustainability of the healthcare systems in the long run, is difficult to define, as are performance measures aimed at tracking the effectiveness of such interventions [3]. However, scholars have tried to conceptualise SD applied to the healthcare setting. In this regard, sustainable healthcare encompasses several dimensions, such as the economic, social, political and environmental ones, so that healthcare policy makers need to balance them in decision making, considering their potential trade-offs [3,11]. In this regard, the pioneering attempt to define sustainable healthcare dates back to the work of Jameton and McGuire [12], who argue that sustainable healthcare systems should balance the needs of (i) people (patients and healthcare professionals) with (ii) economic concerns and (iii) environmental costs. This definition of sustainable healthcare can also be found in more recent studies, i.e., [11], where it has been applied to the design of innovations in the healthcare setting [13]. Other studies suggested several frameworks to operationalise SD in healthcare, including objectives of corporate social responsibility, patients and employees’ satisfaction, lean thinking applied to healthcare service provision, quality management and accreditation, facilities management to reduce hospitals’ environmental impact, etc. (see [14,15]).
From the 1992 Rio Conference on Sustainable Development, steps have been made to renovate countries’ commitment toward the achievement of a climate-neutral society, including in healthcare. Among others, the Paris Agreement in 2015 [16], where 196 countries participating at the COP21 from all over the world committed to achieve voluntary targets related to greenhouse gas emissions (i.e., the “Nationally Determined Contributions”) and report on this progress. COP26 was then held in Glasgow in 2021 with the aim of verifying countries’ factual engagement in the reduction of emissions and to update their plans to mitigate climate change.
In 2018, the WHO and the United Nations recognised that to achieve the Sustainable Development Goals (SDGs) Agenda, people, skills and resources should be integrated in one single approach emphasising the complementarity of objectives. To address this perspective, a process was launched at the global level by 12 multilateral health, development and training agencies and humanitarian organisations, aimed at developing the Global Action Plan for Healthy Lives and Well-being for All (GAP) and promoting the One Health approach. The Plan aimed at strengthening collaboration between organisations operating in the field of sustainability and accelerating the progress of the countries towards the SDGs Agenda, with a specific focus on health (Goal 3 of the SDGs). While these organisations recognised that health systems’ governance models all over the world were changing to set intersectoral policies, action planning for sustainability was still confined to sectoral interventions, especially in healthcare. As a result, international institutions have mobilised to set roadmaps and guidelines to promote the SDGs’ achievement. For instance, the SDGs Roadmap signed by all WHO European Member States in 2017 proposed an action framework to help institutions and healthcare providers to embrace the challenge of sustainability and report their progress in line with the SDGs agenda: this framework is called the 4EA approach, and it is composed of four building blocks—engage, align, accelerate and account—that aim at coordinating interventions in the field of sustainable healthcare [17].
A systemic and systematic effort at sustainable healthcare is, however, still far from realisation. Indeed, when empirical research is considered, the transition toward sustainable healthcare is mainly characterised by the implementation of single projects by healthcare providers, denoting the lack of strategic planning for sustainability. In addition, sustainability related to healthcare systems as a whole is not investigated. For instance, Kruk et al. [18] found that interventions toward sustainability were pursued with the aim to change healthcare providers’ behaviour, with limited effect in terms of performance and scalability. As argued by the authors, “because health systems are complex adaptive systems that function at multiple interconnected levels, fixes at the micro-level (i.e., healthcare provider or clinic) alone are unlikely to alter the underlying performance of the whole system” [18] (p. e1197). In this regard, structural reforms that can consider the overall health system were suggested, and studies focusing on the performance of sustainable healthcare systems are of wide interest and deserve much investigation [18]. Challenges related to the sustainability of healthcare systems remain linked to the provision of high quality, safe and effective healthcare, as well as the reduction in the environmental impact of HCOs trough the promotion of environmentally friendly hospitals [5]. As a remedy, policies focusing on the interconnectedness between health and the environment have been envisaged by scholars [19]. Addressing the call of these scholars and in light of the WHO roadmaps focusing on the need to develop the One Health approach as well as international policies aimed at sustainable healthcare systems, this paper aims at examining whether the attempts made by the Italian healthcare system to embrace the SD principle have demonstrated achievements over time. In this sense, this study represents an update of a previous survey published in 2017 by Cavicchi and Vagnoni [20] about sustainability in Italian HCOs. Thus, this paper aims at investigating to what extent the SD discourse, stemming from the institutional context, was characterising GDs’ perceptions in sustainable healthcare and to what extent SD was operationalised in Italian HCOs through dedicated actions, comparing the years 2016 and 2021. In addition, potential levers that could contribute to sustainable development implementation in Italian HCOs were examined, comparing the years 2016 and 2021. These levers relate to the Sustainability Intellectual Capital framework that has been applied elsewhere in Cavicchi and Vagnoni’s study [20].
To achieve the paper’s objectives, a questionnaire-based survey has been directed to the General Directors of government funded HCOs to investigate their perceptions about the SD principle applied to healthcare, their strategic planning for SD, their implemented actions and the intellectual capital (IC) factors that influence the latter’s implementation. For the purposes of this study, the questionnaire was designed in 2016 and conducted in two waves: the first wave was administered in 2016 and the second one in 2021. To compare the results of the two waves and to identify differences over time, we used both qualitative and quantitative methods of analysis, and read the results in light of the political context and relevant literature in the field.
2. Action Planning for Sustainability in Healthcare Systems
Cavicchi and Vagnoni [20] conducted a survey of Italian HCOs to investigate action planning for sustainability in the Italian healthcare system in light of the approved National Strategy of Sustainable Development. Indeed, the Italian National Strategy of Sustainable Development was born in 2017, thanks to a strong concertation process (started at the beginning of 2016) between government institutions and the representatives of the main stakeholders’ categories to define targets to achieve the 2030 SDGs Agenda. The strategy provided several targets for the healthcare sector, such as improving the access to health services; strengthening staff training; enacting prevention mechanisms to counteract health emergencies; relaunching public health functions. The Strategy recognised that the link among the conditions of the ecosystem, social wellbeing and economic prospects was essential for the development of the territory and for infrastructural policies, so that targets were set considering such interconnectedness.
The study of Cavicchi and Vagnoni [20], in this regard, analysed the perceptions of General Directors (GDs) of the total population of the Italian HCOs about the implementation of the sustainability principle in their organisations, to understand whether the international and national discourse on sustainability that was rising in those years was developing new ways of thinking in GD mindsets. The results revealed the GDs’ awareness of the SD principle in the healthcare sector, and their tendency to consider the economic, social and environmental dimensions in their decision making, coherently with the triple bottom line approach [12,21]. The need to achieve a balance between the quality and efficiency of the care services played a pivotal role for sustainable healthcare and was mainly reflected in their propensity to integrate the economic and social considerations in decision making. The environmental sensitivity was also improving but with limited connections to the other sustainability dimensions. While a half of the HCOs declared to have inserted SD goals within their strategic plans, action planning for sustainability was mainly related to the implementation of single projects. Action planning mainly included: the rational use of natural resources; prevention through the promotion of sustainable lifestyles; green purchases; projects for health and safety in the workplace; sustainable management of waste; etc. These results were in line with a national context in which the Sustainable Development Strategy had just been outlined and with the emanation of the 2030 SDGs Agenda. However, more recent studies have confirmed the single projects’ implementation approach in other contexts as well. For instance, Kruk et al. [18] found that most interventions for sustainable primary healthcare, as discussed by the literature in the period 2008–2017, were focusing on the micro-level, in the interface between the HCOs and its users, targeting individual users, facilities and the health workers as the main recipients of actions. In this regard, how health systems as a whole coordinate sustainable action planning deserves more investigation. At the same time, it has to be acknowledged that the degree of sustainability implementation by a HCO depends on its level of maturity, leadership and management commitment [22,23].
Based on the above, we stated the following research questions:
RQ1: How did GDs perceive the SD principle over time?
RQ2: To what extent did GDs operationalise the SD principle in their HCOs over time?
RQ3: To what extent did HCOs’ plans and projects take into account SD over time?
3. Intellectual Capital to Promote Sustainability in Healthcare Organisations
Scholars have focused on the role of IC to promote the transition of HCOs toward SD; research in this direction has gained momentum starting from 2017 [24], when studies started to address the role of IC to the achievement of the SDGs agenda in public sector organisations.
Focusing on the literature on sustainability in healthcare, a Sustainability Intellectual Capital Model for HCOs has been proposed by Cavicchi and Vagnoni [20], to get a whole picture of the intangible and tangible assets that can enact the sustainability transition. This model responded to the call for management frameworks integrating IC as a driver of sustainability, consistent with previous literature [25], which, however, neglected the healthcare sector as a study setting despite the relevancy of sustainability in this sense [12].
IC has been mainly related to three components—human, structural and relational capital [26,27,28] with a focus on the factors within those components that are needed to promote the shift to environmental sustainability [29] based on [30] and [31,32,33].
The Sustainable Intellectual Capital in HCOs model [20] consistently enclosed the three components and provided an overview of the related factors:
- (a)
- (b)
- Structural capital dealt with the organisational culture around sustainability, the leadership support and the presence of dedicated organisational structures to manage sustainability [41]; the open and collaborative environment to foster interdisciplinary projects [42]; organisational capabilities (clinical possibilities) [43]; specific organisational structures [44]; managerial philosophies aimed at resource efficiency; time to be dedicated to sustainability projects; and change management capabilities [39,40,45];
- (c)
- Relational capital included collaboration with and support from territorial stakeholders at different levels of planning [46,47,48,49] and involving different actors such as non-profit organisations, firms, communities, universities and others. This could help the acquisition of elements needed to address challenges [50].
The model has been mainly tested in the Italian healthcare sector, revealing that synergies among the capitals can promote the implementation of sustainability in HCOs; among the factors, the ICT and advanced technologies played a pivotal role in action planning for sustainability. The contribution of IC assets to sustainable healthcare was also confirmed by Cavicchi [51], who found social capital as well as technologies to be enablers of environmental and medical projects aimed at increasing patients’ involvement in disease management. Technologies has been discussed to potentially improve the patients’ access to healthcare services, to reduce errors and to optimize internal processes [52,53]. Another study [54] found that green human resources practices are correlated with sustainability performance in HCOs. Academic research has also revealed barriers related to the implementation of sustainability projects due to the lack of specific assets’ development: for instance, the lack of organisational commitment to environmental issues represents one of the main barriers in environmental projects’ implementation in HCOs [55]. On the contrary, budget constraints as well as difficulties evaluating the impact of such initiatives are not considered as relevant barriers to promote environmental initiatives for sustainable healthcare [55]. Nevertheless, enablers of sustainability in HCOs have been shown to be the incorporation of SD principle in their organisational culture, strategy, performance management and structures [56].
Based on the above premise, we aimed at responding to the following research question:
RQ4: To what extent did the GDs’ perception of IC assets as levers of sustainable healthcare change in the timeframe 2016–2021?
4. Materials and Methods
A questionnaire to be directed to Italian public HCOs was prepared in 2016 [20]. The setting was considered interesting as Italy experienced the design and implementation of a sustainability strategy at the national level in those years.
Based on Floyd and Fowler [57], the questionnaire was pre-tested at the time in a focus group with academics with expertise in surveys in healthcare. It was then tested with general directors (GDs) of three HCOs before being administered and re-tested in 2021 with two other general directors of two HCOs to ensure the topic was still relevant to the audience.
Based on the survey’s aims, all the government-funded HCOs populating the Italian context were considered, including local health authorities (LHAs), independent hospitals (IHs and university hospitals (UHs).
Two surveys were administrated in two separate periods: the first round of the questionnaire was submitted at the end of 2016 by mail, while the round second came at the end of 2021, using the Qualtrics package.
The organisations were identified based on Ministry of Health public databases; then, two of the researchers collected the general directors’ names and addresses and the questionnaires were expressly mailed to them. The data collection processes were performed in both 2016 and 2021 to ensure that changes in organisations’ top management were detected.
The sample involved almost the total population of Italian public HCOs with juridical autonomy (as issued by the Legislative Decree 502/1992 [58]). Thus, the sample included 122 LHAs and 83 IHs and UHs in 2016, for a total of 205 HCOs; in 2021, the sample included 99 LHAs and 104 IH and UHs, for a total number of 203. As a process of mergers has characterised the Italian healthcare system during the last few years, the population has clearly changed in terms of dimension.
Invitation to fill in the questionnaire was directed to HCOs’ GDs, as they are responsible for the organisations’ strategy [59]. GDs are appointed by the Regions for five-year mandates; they are in charge of managing the organisations and fulfilling health goals through an efficient resource management, aligned with regional health plans.
Follow-ups were conducted both in 2016 and 2021, aiming at increasing the overall response rate [60].
In 2016, 31 organisations answered the questionnaire, for a total response rate of 15%; in 2021, 14 organisations responded (total response rate of about 7%). None of the HCOs involved in 2016 responded to the survey in 2021, so that the two samples are not superimposable.
The questionnaire (reported in Appendix A) was composed of four sections: the first was centred on the investigation of GDs’ perspectives on the principle of SD and the meaning they attributed to it in healthcare. In this sense, the questionnaire included two open questions: “What meaning do you attribute to the principle of ‘sustainable development’?” and “In your opinion, what does the concept of sustainable development in HCOs refer to, or what does it translate into in this context?”. The second section investigated whether the organisation had or had not adopted a sustainability plan (permanently adopted, in progress, pending approval, not approved) and whether it adopts or not an approach in individual projects or programs for implementing SD initiatives (yes or no). Further, an additional section centred on the initiatives HCOs put in place to increase organisations’ sustainability: in this sense, respondents were given a list of major key project actions based on sustainability from the healthcare literature [39,50,61], among them: sustainable use of resources (energy, water, etc.), sustainable canteen/catering, equal opportunities, health and safety for the hospital’s population, sustainable transport, public procurement, waste management, promotion of sustainable lifestyles, prevention of drug use, personalised and eco-friendly treatments, eco-compatibility of health facilities, economic and financial sustainability. The fourth section refers to the “Sustainable Intellectual Capital for HCOs” model [20]. In this sense, GDs were asked to rate the extent to which a series of factors pertaining to the model could contribute to the implementation of sustainability projects on a five-point Likert scale. The reliability of the scale was assessed through Cronbach’s alpha [62] using SPSS software package, with satisfactory results (α = 0.879).
Data analysis was performed in multiple ways. GDs’ responses in 2016 and 2021 concerning their perception of sustainability and its meaning in the healthcare sector were analysed through NVivo software. In particular, the autocoding function was performed to identify the main themes emerging from the data, following an inductive approach to content analysis. This supported the comparison of the perceptions of GDs at different times and the discussion of potential differences in light of the evolution of the institutional context.
Then, descriptive statistics were employed to explore the state of implementation of sustainability plans in 2016 and 2021, the adoption of programs/projects to increase organisations’ sustainability, and the types of initiatives organised by the respondents at the time of investigation. Lastly, differences in the two periods concerning GDs’ perspective on the contribution of IC factors to the implementation of sustainability projects were analysed through a Mann–Whitney U test using SPSS software package [63,64]. Aimed at comparing the means of the two data collections, the authors firstly checked for the normality of distributions and the homogeneity of variances through Shapiro–Wilk and Levene’s tests. Having assessed the non-normal distribution of variables, the authors implemented the Mann–Whitney U test as a non-parametric method. Consistent with the test assumptions, the two samples are random and independent and the scale of measurement is ordinal (as mentioned before).
5. Results
As from Table 1, the respondents in 2016 mainly pertained to LHAs (n = 23; 74.2%), while in 2021 they pertained to UH and IH (n = 6; 42.9%) and LHAs (n = 5; 35.7%). The organisations were predominantly located in the North of Italy in 2016 (n = 23; 74.2%), while in the 2021 analysis, they were mainly located in both the Centre (n = 7; 50.0%) and the North (n = 6; 42.9%).
5.1. The Meaning of Sustainable Development in Healthcare
GDs were initially asked to provide their perspectives concerning the meaning they attribute to the principle of SD. The NVivo analysis allowed for the detection of some differences in the way GDs defined sustainable healthcare.
From the definitions provided by GDs at the time of the survey conducted in 2016, it was possible to identify four main themes: (i) the integration between the social and economic dimensions of sustainability in the provision of care services, (ii) the optimisation in the use of resources to allow future generations to satisfy their health needs, (iii) the development of technologies to improve the quality of care, (iv) the principle of environmental protection.
Concerning the integration of the social and economic dimensions of sustainability in the provision of care services, it was argued:
“SD is a socio-economic model of development that must be designed to balance the increasingly complex and specific healthcare demand with the organisational and financial constraints imposed by the system: development must be operationalised through actions that produce results in terms of quality and of efficiency but also in terms of social equity.”(LHA1)
Once again:
“SD is a process of change that makes the exploitation of resources, the direction of investments, the orientation towards technological development consistent with future health needs as well as with the current ones.”(LHA2)
Environmental protection was mainly recognised as a general principle that characterised the institutional context in which HCOs operated. As argued:
“It is a process of improvement based on available resources, which directs the flow of investments according to technological and social development in line with current needs, but also with the future ones, in compliance with universally recognised environmental protection principle.”(IH1)
Considering definitions of sustainable healthcare from respondents of the 2021 survey, a major awareness on the topic of environmental protection was growing. In fact, three main themes emerged prominently: (i) the link between environmental protection and the use of resources, (ii) the need to balance the provision of healthcare services foreseen by law and the use of resources, (iii) the quality of life through balancing environmental protection with economic development.
As argued:
“In the health sector, it means being able to guarantee the fair and complete provision of healthcare services foreseen by law within a framework of limited resources. I think there may also be an environmental dimension, linked to the use of resources in terms of decreasing the environmental impact.”(LHA3)
“We apply the SD principle promoting environmental stewardship behavior that is aimed at eliminating the waste of resources”(LHA4)
“Economic development that respects the environment, aimed at improving the quality of life.”(UH1)
Apart from definitions still focusing on the balance between the quality of care and the financial resources available to provide care services, the recent investigation allowed for noticing an increase in the GDs’ awareness of the environmental dimension of sustainability in healthcare. From one side, that awareness was mainly routed toward the reduction of waste to free financial resources and improve the economic performance of HCOs. From the other side, it was also recognised that environmental protection is relevant for the quality of life of people, in a certain sense, trying to connect the environmental dimension of SD with the social one.
5.2. The Operationalisation of the Sustainable Development Principle
GDs also gave their perspective on the operationalisation of the SD principle in their organisations.
In 2016, this was mainly related to actions linked to (i) the prevention activities and (ii) the reduction in the environmental impact of care facilities. For instance, a respondent argued:
“We are promoting actions aimed at improving community health also through the promotion of sustainable lifestyles.”(UH2)
Other GDs recognised the relevance of the three dimensions of sustainability in daily practices, and stated:
“Actions aimed at reducing waste have been launched as a part of the strategy, and have been operationalised through SMART objectives. We have applied the principles of recycling and reuse in our practice, we have promoted renewable energy sources utilisation. Great importance has also been attributed in our planning to human resources: this in terms of safety at work, equal opportunities and training to allow the full professional development of staff members.”(LHA5)
The above themes also emerged in 2021 from the perceptions of GDs showing a major focus on the redesign of the internal business processes. These include: (i) the implementation of lean management, (ii) the reduction in environmental impact projects and (iii) the promotion of actions related to the social sustainability sphere.
“The revision of the internal business processes can reduce waste, the use of drugs and medical devices. It can also facilitate home care. By introducing new services or simplifying others, we can contribute to improve the health and the psycho-physical well-being of patients.”(LHA5)
Again:
“To act in a sustainable manner, it is therefore necessary to act on the care paths and processes (lean management), and human resources (skills management).”(UH3)
“In a broad sense, our actions can range from energy consumption choices that have a lower environmental impact to improve services to patients and comply with economic sustainability principle.”(UH4)
5.3. Sustainability Plan, Projects/Programmes and Action Adoption
Concerning the adoption of a formalised sustainability strategy through a sustainability plan (Table 2), results reported differences in their levels of implementation. Specifically, while in 2016, HCOs with formalised sustainability plans were 45.2% (n = 14), in 2021, these are 35.7% (n = 5) of respondents. However, more organisations presented progress in their processes (21.4% in 2021 compared to 3.2% in 2016), although, in absolute terms, this number refers to three compared to one organisation. Further, respondents in 2016 presented a tendency to develop sustainability plans, given the proportion of respondents reporting a pending approval (19.4%; n = 6), while this has not been confirmed in 2021, where only one respondent reported such a situation. Lastly, an increasing number of organisations do not present adopted sustainability plans. Specifically, in 2021, 35.7% (n = 5) of the respondents reported that a sustainability plan has not been adopted, compared to 32.3% of 2016.
Most respondents in the two periods reported they had adopted projects or programs for sustainability (Table 3), but with a decreasing trend on the timeline. In fact, the number of HCOs implementing projects or programs was higher in 2016 compared to 2021 (83.8% vs. 78.6%), with an increase in the proportion of organisations that did not implement such programs (14.3% in 2021, compared to 12.9% in 2016).
Concerning the SD actions implemented by HCOs, all the respondents in 2016 and all except 1 in 2021 reported being engaged in at least 1 sustainability initiative among the 12 proposed in the questionnaire. In 2016, HCOs performed n = 6.7 initiatives on average (std.dev. = 3.1), while in 2021, they performed n = 4.0 on average (std.dev. = 3.1). In 2016, 1 respondent reported that the managed organisation implemented all initiatives, while 3 HCOs’ GDs reported the implementation of 11 initiatives out of 12, and an additional 3 reported 10 initiatives out of 12. In 2021, none of the respondents implemented all the initiatives, while one reported the organisations had implemented 11 out of 12 initiatives.
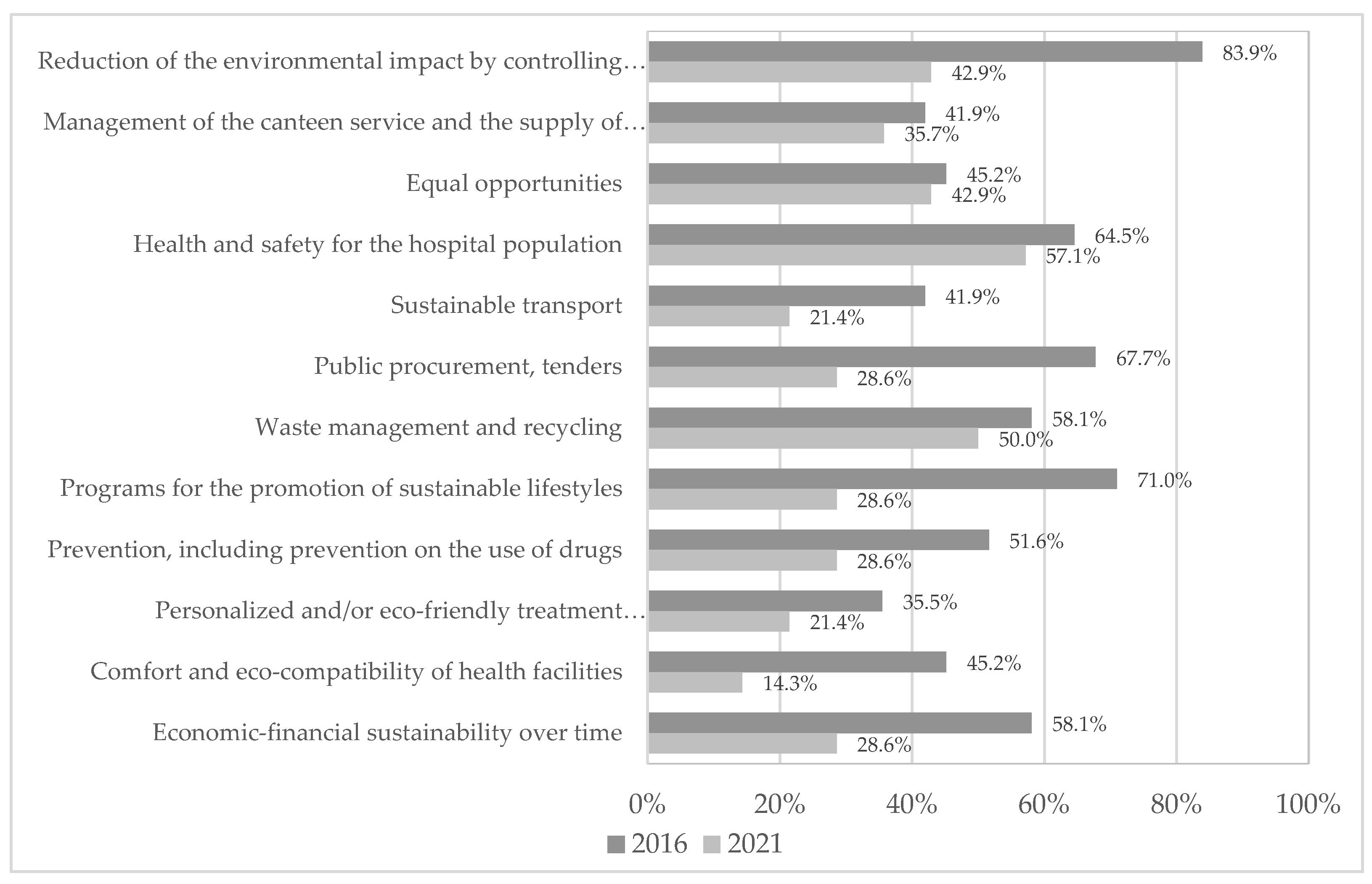
The types of initiatives that HCOs presented are reported in Figure 1; for each action, the proportion of responses for the total number of respondents in the year is reported. As it can be noted, there emerges a shared tendency for HCOs to reduce the number of initiatives carried out towards SD. While in 2016, the most pursued action concerned the reduction in the environmental impact, which was performed by 83.9% of respondents, in 2021, the proportion of respondents in this sense dropped to 42.9%. Again, more than two thirds of HCOs in 2016 promoted sustainable lifestyles (71.0%) or addressed SD while paying attention to public procurement and tenders (67.7%). In 2021, the most pursued initiative referred to ensuring the health and safety of the hospital population (57.1%), followed by waste management and recycling (50.0%). The least pursued initiatives in 2016 were related to the management of the canteen service and food supply and to sustainable transport (41.9%). In 2021, the least performed activities refer to the comfort and eco-compatibility of healthcare facilities (14.3%), followed by sustainable transport and personalised/eco-friendly treatments (21.4% each).
5.4. IC Factors and Sustainability
Table 4 reports mean values and standard deviations concerning GDs’ answers on the factors based on the Sustainable Intellectual Capital for HCOs model presented in Section 3 to support the implementation of sustainability initiatives. As it can be noted, for both periods, all factors’ means are above the mean value of 2.5 on the 5-points Likert scale, so that all the factors are considered relevant for pursuing sustainability initiatives.
For all the factors (except “Collaboration and support of local stake-holders”) mean values in 2021 are higher than those reported in 2016. The highest value in 2016 refers to “Search for internal efficiency” (mean = 3.79; std.dev. = 0.902) and “Collaboration between strategic management and employees; active participation” (mean = 3.52; std.dev. = 1.151), and the lowest mean values are reported with regards to “Structural factors” (mean = 2.66; std.dev. = 1.233) and “Presence of sustainability skills dictated by specific university training and learning projects” (mean = 2.67; std.dev. = 1.295). This latter factor has also been appointed in 2021 as the least contributive to sustainability initiatives (mean = 2.92; std.dev. = 1.498), together with “Collaboration and support of local stakeholders” (mean = 3.00; std.dev. = 0.913). Conversely, most contributive factors are related to “Search for internal efficiency” (as in 2016, mean = 4.00; std.dev. = 0.816) and “Organisational culture” (mean = 4.08; std.dev. = 0.862).
To test whether the differences reported above were significant, the Mann–Whitney U test was performed using the SPSS.
As shown in Table 4, the analysis reported significant differences between the groups for only two factors. In particular, the use of ICT and technological innovation as a factor for implementing sustainability actions differs significantly (2-tailed sig. = 0.039), with a higher mean in 2021 (mean = 4.00, std.dev. = 0.816 versus mean = 3.35, s.d. = 0.877). Further, a significant difference (2-tailed sig. = 0.043) emerged concerning organisational culture, whose role was rated higher again in 2021 (mean = 4.08, std.dev. = 0.862 versus mean = 3.47, std.dev. = 0.973).
6. Discussion
From the analysis of the GDs’ perceptions, sustainable healthcare has been conceptualised considering the three dimensions of sustainability as reported in policy and academic frameworks. In this regard, sustainability can be met when the social, economic and environmental dimensions are incorporated in decision making. Results revealed that the GDs’ awareness of the relevance of the environmental dimension increased in the second-wave survey in 2021. The conceptual view of sustainable healthcare did not change, as mainly ascribable to the integration of the social dimension (the quality and affordability of care) with the economic dimension (budgets available from government funding), and to the integration between the environmental dimension (the reduction in the use of natural resources) and the economic one (mainly related to saving and the reduction in waste). In 2021, however, the sustainability definitions started to consider the relevance of environmental protection principles for the peoples’ quality of life. When considering the operationalisation of the SD principle, perceptions of GDs revealed similarities between the two survey results, as actions were connected to the three pillars of the triple bottom line.
However, when looking at the statistical results, a decrease in the implementation of formalised sustainability plans emerges, in terms of adoption, progress or pending approval. Consistently, a minor proportion of HCOs implemented programs and projects for sustainability. A reduction in the proportion of HCOs implementing SD actions can also be noted (6.7 on average for each HCO in 2016 versus 4.0 on average in 2021). In this sense, HCOs in 2021 tended to address minor sustainability initiatives compared to the situation surveyed five years before. The focus also changed, from an attention to reducing the environmental impact and the promotion of sustainable lifestyles, to the health and safety of the hospital population and waste management and recycling.
Concerning the relevance of IC factors to support the implementation of sustainability initiatives, few differences emerge between the two surveys. In particular, a significant difference is highlighted concerning the use of ICT and technological innovation and the role of organisational culture, which were higher in 2021, emphasising the increasing relevance of such factors in more recent times to pursue sustainability initiatives. This is in line with studies that identify ICT and organisational culture as potential enablers of the healthcare transition toward sustainability [20,36,51,52,56]. Despite the Italian National Strategy on Sustainable Development that was set in 2017 to define guidelines for the achievement of the 2030 SDGs Agenda, it has never been translated into direct interventions in the national and regional health systems (the macro and meso levels) to promote the integration of the three dimensions of sustainability (environmental, social and economic) in decision making. In fact, healthcare policies promoted during this time were mainly oriented to guarantee the financial sustainability of the healthcare systems, this being a dominant discourse in the Italian healthcare setting [10,51]. As argued, in Western European Countries, austerity measures aimed at containing health expenditures and responding to the effects of the financial crisis have been mainly pursued to recover efficiency and to use resources for short-term interventions to increase economic growth; in turn, the label of “sustainability” attributed to these measures has led to considerations of sustainability as a resource constraint healthcare systems must comply with, at the expense of the welfare provided to the citizens risking impoverishment of their health status [3,65]. In this perspective, innovation needs to be sustained without incremental or dedicated resources due to cost containment targets; however, the latter did not discourage HCOs from the adoption of environmental innovations [55] to sustain the environmental dimension of SD. Consequently, most of the projects undertaken at the HCO level (the micro level) in the field of sustainability were voluntary initiatives and depended largely on the single sensitivity of regions and HCOs’ GDs [51]. As a result, despite awareness on SD topics being identified in both the waves of the survey, different commitments to sustainable projects were found. This result is in line with the literature [22,23] arguing that SD implementation depends on the level of maturity of the HCOs’ sustainability orientation, leadership and management.
7. Conclusions
The study has aimed at discussing the extent to which the SD principle has entered the strategic planning of HCOs and has impacted their strategic actions and processes. With reference to RQ1, both the waves of the survey identified a general awareness of GDs for the principle of SD in healthcare; as for the operationalisation of SD (RQ2), GDs emphasised the relevance of the balancing of the economic and social dimensions of the triple bottom line applied to healthcare, and of the environmental and economic dimensions. In 2021, references to the principle of environmental protection and its impact on quality of life started to characterise GDs’ discourses. Nevertheless, as from the findings addressing RQ3, in 2021, the HCOs were found to be less involved in implementing SD strategies and projects than in 2016. Considering IC factors that can enhance sustainability planning in HCOs, consistent with RQ4, in 2021, ICT and technological innovations along with organisational culture were perceived as more relevant than in 2016. The study allows for sensing some changes in terms of SD implementations during the last five years; these appear to be consistent with the country’s policies and actions undertaken in terms of sustainability in the national healthcare system.
This study contributes to filling the gap in the literature about SD in healthcare from the HCOs’ perspective, highlighting both the role of the factors enhancing the implementation of sustainability actions and, more in depth, the role of the IC and staff’s capabilities to that end.
Furthermore, this paper may contribute to the healthcare field’s practise to raise the discussion—among practitioners and local policy makers—of the state of SD penetration in the HCO’s strategy and actions. This might raise the debate about the contribution of the SD’s strategy to the improvement of the HCO’s overall performance and of the relationship between the organisations and their stakeholders. In addition, this paper emphasizes the importance of raising organisational culture and exploiting ICT potentialities to support sustainability actions, as those factors gained increasing attention over time.
Further studies are needed to investigate the operationalisation of the SD principle in other countries and care settings (for instance private healthcare providers) to extend our knowledge on healthcare systems’ progress toward the SDGs Agenda and to promote the dissemination of best practices. In addition, following the investigation of the differences over time concerning the relevance of IC factors for SD, the results emphasize the importance of additional research exploring the reasons underlying GDs’ perceptions through qualitative approaches. Therefore, further qualitative research (e.g., comparative case studies) is recommended to deepen the understanding regarding the extent to which IC factors play a role in SD. Furthermore, considering the emerging importance of digital technologies (artificial intelligence, machine learning, telemedicine, etc.) in healthcare settings, additional qualitative and quantitative research is needed to understand whether these assets are currently applied for the improvement of healthcare pathways with a view to sustainability, and what factors can affect their implementation.
Author Contributions
Conceptualisation, C.C., E.V. and C.O.; methodology, C.C. and C.O.; validation, E.V.; formal analysis, C.C. and C.O.; writing—original draft preparation, C.C. and C.O.; writing—review and editing, E.V.; supervision, E.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy reasons.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
The questionnaire
| What meaning do you attribute to the principle of “sustainable development”? | |||||
| | |||||
| In your opinion, what does the concept of sustainable development in healthcare organisations refer to, or what does it translate into in this context? | |||||
| | |||||
| Does the organisation have an action plan for sustainable development? By plan we mean the performance plan or programmatic plan, or in general a planning process that is formalised in a strategic document | |||||
| |||||
| Does the organisation adopt an approach for individual projects/programs for the implementation of sustainable development initiatives? | |||||
| |||||
| If sustainable development actions have been adopted, with respect to which areas have they been implemented? | |||||
| |||||
| To what extent do you believe that the following factors may have favoured the adoption of sustainable development actions? | |||||
| 1 (Not at all) | 2 | 3 | 4 | 5 (Completely) | |
| Organisational culture | ○ | ○ | ○ | ○ | ○ |
| Availability of financial resources | ○ | ○ | ○ | ○ | ○ |
| Search for internal efficiency | ○ | ○ | ○ | ○ | ○ |
| Collaboration between strategic management and employees; active participation | ○ | ○ | ○ | ○ | ○ |
| Presence of sustainability skills dictated by specific university training and learning projects | ○ | ○ | ○ | ○ | ○ |
| Adoption of change management practices (ability to readjust organisational practices, flexibility, etc.) | ○ | ○ | ○ | ○ | ○ |
| Push the organisation to use ICT and technological innovation | ○ | ○ | ○ | ○ | ○ |
| Leadership support and presence of dedicated structures | ○ | ○ | ○ | ○ | ○ |
| Time | ○ | ○ | ○ | ○ | ○ |
| Collaboration and support of local stakeholders | ○ | ○ | ○ | ○ | ○ |
| Structural factors | ○ | ○ | ○ | ○ | ○ |
References
- Naranjo-Gil, D. The Role of Management Control Systems and Top Teams in Implementing Environmental Sustainability Policies. Sustainability 2016, 8, 359. [Google Scholar] [CrossRef] [Green Version]
- United Nations. Our Common Future–Brundtland Report; Oxford University Press: Oxford, UK, 1987. [Google Scholar]
- Borgonovi, E.; Adinolfi, P.; Palumbo, R.; Piscopo, G. Framing the shades of sustainability in health care: Pitfalls and perspectives from Western EU countries. Sustainability 2018, 10, 4439. [Google Scholar] [CrossRef] [Green Version]
- Rouse, W.B. Health Care as a Complex Adaptive System: Implications for Design and Management. Bridge 2008, 38, 17–25. [Google Scholar]
- McDaniel, R.R.; Lanham, H.J.; Anderson, R.A. Implications of complex adaptive systems theory for the design of research on health care organizations. Health Care Manag. Rev. 2009, 34, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Berwick, D.M.; Nolan, T.W.; Whittington, J. The Triple Aim: Care, Health, and Cost. Health Aff. 2008, 27, 759–769. [Google Scholar] [CrossRef] [Green Version]
- Maarse, H.; Jeurissen, P.; Ruwaard, D. Concerns over the Financial Sustainability of the Dutch Healthcare System; IFO Institute, Center for Economic Studies: Munich, Germany, 2013. [Google Scholar]
- Kessler, R.; Glasgow, R.E. A Proposal to Speed Translation of Healthcare Research into Practice: Dramatic Change is Needed. Am. J. Prev. Med. 2011, 40, 637–644. [Google Scholar] [CrossRef]
- Waddock, S. The Wicked Problems of Global Sustainability Need Wicked (Good) Leaders and Wicked (Good) Collaborative Solutions. J. Manag. Glob. Sust. 2013, 1, 91–111. [Google Scholar] [CrossRef]
- Nuti, S.; Noto, G.; Ruggieri, T.G.; Vainieri, M. The challenges of hospitals’ planning & control systems: The path toward public value management. Int. J. Environ. Res. Public Health 2021, 18, 2732. [Google Scholar]
- Osorio-González, C.S.; Hegde, K.; Brar, S.K.; Avalos-Ramírez, A.; Surampalli, R.Y. Sustainable Healthcare Systems. In Sustainability: Fundamentals and Applications; Surampalli, R., Zhang, T., Kumar Goyal, M., Brar, S., Tyagi, R., Eds.; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2020; pp. 375–396. [Google Scholar]
- Jameton, A.; McGuire, C. Toward sustainable health-care services: Principles, challenges, and a process. Int. J. Sustain. High. 2002, 3, 113–127. [Google Scholar] [CrossRef]
- Barbero, S.; Pallaro, A. Systemic Design for Sustainable Healthcare. Des. J. 2017, 20 (Suppl. 1), S2473–S2485. [Google Scholar] [CrossRef] [Green Version]
- Marimuthu, M.; Paulose, H. Emergence of sustainability based approaches in healthcare: Expanding research and practice. Procedia Soc. Behav. Sci. 2016, 224, 554–561. [Google Scholar] [CrossRef] [Green Version]
- Al Jaberi, O.A.; Hussain, M.; Drake, P.R. A framework for measuring sustainability in healthcare systems. Int. J. Healthc. Manag. 2017, 13, 276–285. [Google Scholar] [CrossRef]
- United Nations. 2015. Available online: https://unfccc.int/sites/default/files/english_paris_agreement.pdf (accessed on 5 March 2022).
- Menne, B.; Aragon de Leon, E.; Bekker, M.; Mirzikashvili, N.; Morton, S.; Shriwise, A.; Tomson, G.; Vracko, P.; Wippel, C. Health and well-being for all: An approach to accelerating progress to achieve the Sustainable Development Goals (SDGs) in countries in the WHO European Region. Eur. J. Public Health 2020, 30 (Suppl. 1), i3–i9. [Google Scholar] [CrossRef] [PubMed]
- Kruk, M.E.; Gage, A.D.; Arsenault, C.; Jordan, K.; Leslie, H.H.; Roder-DeWan, S.; Adeyi, O.; Barker, P.; Daelmans, B.; Doubova, S.V.; et al. High-quality health systems in the Sustainable Development Goals era: Time for a revolution. Lancet Glob. Health 2018, 6, e1196–e1252. [Google Scholar] [CrossRef] [Green Version]
- Molero, A.; Calabrò, M.; Vignes, M.; Gouget, B.; Gruson, D. Sustainability in healthcare: Perspectives and reflections regarding laboratory medicine. Ann. Lab. Med. 2021, 41, 139–144. [Google Scholar] [CrossRef]
- Cavicchi, C.; Vagnoni, E. Does intellectual capital promote the shift of healthcare organizations towards sustainable development? Evidence from Italy. J. Clean. Prod. 2017, 153, 275–286. [Google Scholar] [CrossRef]
- Elkington, J. Cannibals with Forks: The Triple Bottom Line of Twenty-First Century Business; Capstone: North Mankato, MN, USA, 1997. [Google Scholar]
- Chiarini, A.; Vagnoni, E. Environmental sustainability in European public healthcare: Could it just be a matter of leadership? Leadersh. Health. Serv. 2016, 29, 2–8. [Google Scholar] [CrossRef]
- Cosimato, S.; Vona, R. Circular economy strategies for healthcare sustainability: Some insights from Italy. In Sima Management Conference Proceedings; University of Pisa—Sant’Anna School of Advanced Studies: Pisa, Italy, 2020. [Google Scholar]
- Secundo, G.; Ndou, V.; Del Vecchio, P.; De Pascale, G. Sustainable development, intellectual capital and technology policies: A structured literature review and future research agenda. Technol. Forecast. Soc. Change 2020, 153, 119917. [Google Scholar] [CrossRef]
- Mertins, K.; Orth, R. Intellectual capital and the triple bottom line: Overview, concepts and requirements for an integrated sustainability management system. In Proceedings of the 4th European Conference on Intellectual Capital, ECIC 2012, Helsinki, Finland, 23–24 April 2012; pp. 516–526. [Google Scholar]
- Edvinsson, L.; Malone, M.S. Intellectual Capital—Realizing Your Company’s True Value by Finding its Hidden Roots; Harper Business: New York, NY, USA, 1997. [Google Scholar]
- Sveiby, K.E. The New Organizational Wealth: Managing and Measuring Knowledge—Based Assets; Berrett-Koehler: San Francisco, CA, USA, 1997. [Google Scholar]
- Cañibano, L.; Sánchez, P.; Garcia-Ayuso, M.; Chaminade, C. (Eds.) Meritum. In Guidelines for Managing and Reporting on Intangibles; Fundación Airtel Móvil: Madrid, Spain, 2002; pp. 1–30. [Google Scholar]
- Chen, Y. The positive effect of green intellectual capital on competitive ad-vantages of firms. J. Bus. Ethics 2008, 77, 271–286. [Google Scholar] [CrossRef]
- Bontis, N. Managing organisational knowledge by diagnosing intellectual capital: Framing and advancing the state of the field. Int. J. Technol. Manag. 1999, 18, 433–462. [Google Scholar] [CrossRef]
- Johnson, W.H. An integrative taxonomy of intellectual capital: Measuring the stock and flow of intellectual capital components in the firm. Int. J. Technol. Manag. 1999, 18, 562–575. [Google Scholar] [CrossRef]
- Yahya, N.A.; Arshad, R.; Kamaluddin, A. Measuring green intellectual capital in Malaysian environmentally sensitive companies. In Proceedings of the International Conference on Advances in Social Science, Economics & Human Behavior. Institute of Research Engineers and Doctors, Kuala Lumpur, Malaysya, 8–9 March 2014; pp. 1–5. [Google Scholar]
- Lopez-Gamero, M.D.; Zaragoza-Saez, P.; Claver-Cortes, E.; Molina-Azorín, J.F. Sustainable development and intangibles: Building sustainable intellectual capital. Bus. Strategy Env. 2011, 20, 18–37. [Google Scholar] [CrossRef]
- Pinzone, M.; Guerci, M.; Lettieri, E.; Redman, T. Progressing in the change journey towards sustainability in healthcare: The role of ‘Green’ HRM. J. Clean.Prod. 2016, 122, 201–211. [Google Scholar] [CrossRef]
- Rich, C.R.; Singleton, J.K.; Wadhwa, S.S. Sustainability for Healthcare Management. A Leadership Imperative; Routledge: Oxon, UK, 2013. [Google Scholar]
- Ramirez, B.; West, D.J.; Costell, M.M. Development of a culture of sustain-ability in health care organizations. J. Health Organ. Manag. 2013, 27, 665–672. [Google Scholar] [CrossRef]
- Rogers, B.; McCurdy, L.E.; Slavin, K.; Grubb, K.; Roberts, J.R. Children’s environmental health faculty champions initiative: A successful model for integrating environmental health into pediatric health care. Environ. Health Perspect. 2009, 117, 850–855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarriot, E.G.; Winch, P.J.; Ryan, L.J.; Bowie, J.; Kouletio, M.; Swedberg, E.; LeBan, K.; Edison, J.; Welch, R.; Pacque, M.C. A methodological approach and framework for sustainability assessment in NGO-implemented primary healthcare programs. Int. J. Health Plann. Manag. 2004, 19, 23–41. [Google Scholar] [CrossRef]
- Schroeder, K.; Thompson, T.; Frith, K.; Pencheon, D. Sustainable Healthcare; John Wiley & Sons: Oxford, UK, 2012. [Google Scholar]
- Weisz, U.; Haas, W.; Pelikan, J.M.; Schmied, H. Sustainable hospitals: A socio-ecological approach. GAIA Ecol. Perspect. Sci. Soc. 2011, 20, 191–198. [Google Scholar] [CrossRef] [Green Version]
- Ramirez, B.; Oetjen, R.M.; Malvey, D. Sustainability and the health care manager: Part I. Health Care Manag. 2011, 30, 133–138. [Google Scholar] [CrossRef]
- Kira, M.; Lifvergren, S. Sowing the seeds for sustainability in work systems. In Sustainability and Human Resource Management; Ehnert, I., Harry, W., Zink, K.J., Eds.; Springer: Berlin, Germany, 2014; pp. 57–81. [Google Scholar]
- Lifvergren, S.; Huzzard, T.; Docherty, P. A development coalition for sustainability in healthcare. In Creating Sustainable Work Systems: Developing Social Sustainability; Docherty, P., Kira, M., Shani, A.B.R., Eds.; Routledge: Oxford, UK, 2008; pp. 261–290. [Google Scholar]
- Pinzone, M.; Lettieri, E.; Masella, C. Sustainability in healthcare: Combining organizational and architectural levers. Int. J. Eng. Bus. Manag. 2012, 14, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Balcezak, T.; D’Aquila, R.; DeVito Indiveri, C. WorkSMART at Yale-new haven hospital: A program to eliminate waste and improve efficiency. Sustain. J. Rec. 2014, 7, 260–268. [Google Scholar] [CrossRef]
- Frumkin, H.; Hess, J.; Luber, G.; Malilay, J.; McGeehin, M. Climate change: Thepublic health response. Am. J. Public Health 2008, 98, 435–445. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, C.; McKinley, D. New approaches to pollution prevention in the healthcare industry. J. Clean. Prod. 2008, 16, 734–742. [Google Scholar] [CrossRef]
- Passerini, K.; Wu, D. The new dimensions of collaboration: Mega and intelligent communities, ICT and wellbeing. J. Knowl. Manag. 2008, 12, 79–90. [Google Scholar] [CrossRef]
- Ryan-Fogarty, Y.; O’Regan, B.; Moles, R. Greening healthcare: Systematic implementation of environmental programmes in a university teaching hospital. J. Clean. Prod. 2016, 126, 248–259. [Google Scholar] [CrossRef] [Green Version]
- Gerwig, K. Greening Health Care: How Hospitals Can Heal the Planet; Oxford University Press: Oxford, UK, 2014. [Google Scholar]
- Cavicchi, C. Healthcare sustainability and the role of intellectual capital: Evidence from an Italian regional health service. J. Intellect. Cap. 2017, 18, 544–563. [Google Scholar] [CrossRef]
- Turcu, C.E.; Turcu, C.O. Internet of things as key enabler for sustainable healthcare delivery. Procedia Soc. Behav. Sci. 2013, 73, 251–256. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, T.; Shirahada, K. Toward a sustainable healthcare service system in a limited resource context: Case study of Bangladesh rural advancement committee’s healthcare system. Int. J. Healthc. Manag. 2019, 12, 97–105. [Google Scholar] [CrossRef]
- Mousa, S.K.; Othman, M. The impact of green human resource management practices on sustainable performance in healthcare organisations: A conceptual framework. J. Clean. Prod. 2020, 243, 118595. [Google Scholar] [CrossRef]
- Pinzone, M.; Lettieri, E.; Masella, C. Proactive environmental strategies in healthcare organisations: Drivers and barriers in Italy. J. Bus. Ethics 2015, 131, 183–197. [Google Scholar] [CrossRef]
- Boone, T. Organizing for sustainability: Exploratory analysis of the healthcare industry. In Sustainable Supply Chains; Boone, T., Jayaraman, V., Ganeshan, R., Eds.; Springer: New York, NY, USA, 2012; pp. 37–48. [Google Scholar]
- Floyd, J.; Fowler, J. Survey Research Methods; Sage publications, Inc.: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Italian Parliament. Legislative Decree 30 December 1992, n. 502. Riordino della Disciplina in Materia Sanitaria, a Norma dell’Articolo 1 della Legge 23 Ottobre 1992, n. 421; Italian Parliament: Rome, Italy, 1992. [Google Scholar]
- Swayne, L.E.; Duncan, W.J.; Ginter, P.M. Strategic Management of Health Care Organization; Jossey Bass: San Francisco, CA, USA, 2008. [Google Scholar]
- Millar, M.M.; Dillman, D.A. Improving response to web and mixed-mode surveys. Public Opin. Q. 2011, 75, 249–269. [Google Scholar] [CrossRef] [Green Version]
- Pelikan, J.M.; Krajic, K.; Dietscher, C. The health promoting hospital (HPH): Concept and development. Patient Educ. Couns. 2001, 45, 239–243. [Google Scholar] [CrossRef]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef] [Green Version]
- Cramer, D. Fundamental Statistics for Social Science; Routledge: London, UK; New York, NY, USA, 1998. [Google Scholar]
- Field, A. Discovering Statistics Using SPSS (and Sex, Drugs and Rock’n’Roll), 3rd ed.; Sage: Los Angeles, CA, USA, 2009. [Google Scholar]
- Borgonovi, E.; Compagni, A. Sustaining universal health coverage: The interaction of social, political, and economic sustainability. Value Health 2013, 16, S34–S38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Proportion of organisations implementing sustainable development actions in 2016 and 2021.
Figure 1.
Proportion of organisations implementing sustainable development actions in 2016 and 2021.


{kind=link}
Table 1.
Respondents’ characteristics in 2016 and 2021.
| 2016 (n = 31) | 2021 (n = 14) | |
|---|---|---|
| Organisation type | ||
| Local health authority | 23 | 5 |
| Independent hospital | 5 | 3 |
| University hospital | 3 | 6 |
| Location | ||
| North | 23 | 6 |
| Centre | 2 | 7 |
| South | 6 | 1 |
Table 2.
Implementation of sustainability plans, number of respondents and percentage.
| 2016 (n = 31) | 2021 (n = 14) | |||
|---|---|---|---|---|
| Count | Percentage | Count | Percentage | |
| Permanently adopted | 14 | 45.2% | 5 | 35.7% |
| In progress (approved and awaiting implementation) | 1 | 3.2% | 3 | 21.4% |
| Pending approval | 6 | 19.4% | 1 | 7.1% |
| Not approved | 10 | 32.3% | 5 | 35.7% |
Table 3.
Implementation of programs/projects for sustainability.
| 2016 (n = 31) | 2021 (n = 14) | |||
|---|---|---|---|---|
| Count | Percentage | Count | Percentage | |
| Yes | 26 | 83.9% | 11 | 78.6% |
| No | 4 | 12.9% | 2 | 14.3% |
| No answer | 1 | 3.2% | 1 | 7.1% |
Table 4.
Mean values, standard deviations and Mann–Whitney U test of factors’ contribution to sustainable development actions.
Table 4.
Mean values, standard deviations and Mann–Whitney U test of factors’ contribution to sustainable development actions.
| 2016 | 2021 | Mann-Whitney U Test | Z | 2-Tailed Sig. | |||
|---|---|---|---|---|---|---|---|
| Factors | Mean | Std. Dev. | Mean | Std. Dev. | |||
| Organisational culture | 3.47 | 0.973 | 4.08 | 0.862 | 122.500 | −2.023 | 0.043 |
| Availability of financial resources | 3.50 | 0.938 | 3.77 | 1.235 | 155.500 | −1.089 | 0.276 |
| Search for internal efficiency | 3.79 | 0.902 | 4.00 | 0.816 | 166.500 | −0.632 | 0.528 |
| Collaboration between strategic management and employees; active participation | 3.52 | 1.151 | 3.64 | 1.027 | 163.000 | −0.224 | 0.822 |
| Presence of sustainability skills dictated by specific university training and learning projects | 2.67 | 1.295 | 2.92 | 1.498 | 176.500 | −0.502 | 0.616 |
| Adoption of change management practices | 3.30 | 0.988 | 3.33 | 1.155 | 178.000 | −0.058 | 0.953 |
| Push the organisation to use ICT and technological innovation | 3.35 | 0.877 | 4.00 | 0.816 | 126.000 | −2.068 | 0.039 |
| Leadership support and presence of dedicated structures | 3.34 | 1.010 | 3.77 | 0.725 | 146.000 | −1.235 | 0.217 |
| Time | 2.90 | 1.076 | 3.08 | 0.760 | 173.000 | −0.800 | 0.424 |
| Collaboration and support of local stakeholders | 3.10 | 1.155 | 3.00 | 0.913 | 186.000 | −0.247 | 0.805 |
| Structural factors | 2.66 | 1.233 | 3.23 | 0.927 | 141.000 | −1.342 | 0.180 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Cavicchi, C.; Oppi, C.; Vagnoni, E. Back and Forth on Sustainable Development: A Focus on Healthcare Organisations. Sustainability 2022, 14, 4958. https://0-doi-org.brum.beds.ac.uk/10.3390/su14094958
AMA Style
Cavicchi C, Oppi C, Vagnoni E. Back and Forth on Sustainable Development: A Focus on Healthcare Organisations. Sustainability. 2022; 14(9):4958. https://0-doi-org.brum.beds.ac.uk/10.3390/su14094958
Chicago/Turabian StyleCavicchi, Caterina, Chiara Oppi, and Emidia Vagnoni. 2022. "Back and Forth on Sustainable Development: A Focus on Healthcare Organisations" Sustainability 14, no. 9: 4958. https://0-doi-org.brum.beds.ac.uk/10.3390/su14094958
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.