
Equitable City in an Aging Society: Public Transportation-Based Primary Care Accessibility in Seoul, Korea


1
Department of Urban Planning, Hanyang University, Seoul 04763, Korea
2
Department of Urban Planning and Engineering, Hanyang University, Seoul 04763, Korea
*
Author to whom correspondence should be addressed.
Sustainability 2022, 14(16), 9902; https://0-doi-org.brum.beds.ac.uk/10.3390/su14169902
Submission received: 4 July 2022
/
Revised: 4 August 2022
/
Accepted: 8 August 2022
/
Published: 10 August 2022
(This article belongs to the Special Issue Health in All: Global Health and Sustainable Development Goals)
Abstract
:The development of an equitable city has been the primary goal of recent urban planning. Whereas previous urban planning has addressed problems caused by urbanization and population growth, current urban planning must closely consider demographic changes such as an aging society. An aging population, characterized by an increased need for regular healthcare and a growing reliance on public transport, can pose a major challenge to equitable cities. Thus, it is necessary to scrutinize the medical and public transportation links in urban planning strategies to create a more equitable city in an aging society. This study analyzed primary care accessibility for older adults using public transportation in Seoul and considered whether it is socially and economically equitable. Primary care accessibility was derived using the modified 2SFCA model and the Seoul Public Transportation API and social equity was analyzed using the concentration index and concentration curve. The results showed that primary care accessibility of the elderly is related to public transportation mobility, medical facilities and the distribution of elderly populations, revealing both social and economic inequality. This analysis suggests the need for integrated urban planning for an equitable city in an aging society, with implications for efficient resource distribution.
1. Introduction
Equal access to public services such as medical facilities and public transportation is essential for creating equitable cities [1,2,3]. Indeed, this is a core principle in Habitat III (The United Nations Conference on Housing and Sustainable Urban Development), which establishes the global urban policy direction for the next two decades [4]. The New Urban Agenda, the result of Habitat III discussions, articulated the vision of “a city for all” and emphasized equal opportunities, rights, and freedom for all people within a city. The key themes of the New Urban Agenda include ensuring equal access to public goods and services and guaranteeing the mobility of vulnerable populations (such as older people and women). In addition, the Agenda specifies inequality, social exclusion, and poverty as significant obstacles to achieving this vision.
Recent global population aging may increase cities’ vulnerability to inequality and social exclusion. Globally, there will be 727 million people aged 65 and over in 2020, and this number is expected to more than double over the next 30 years. In particular, the old-age dependency ratio (65+/20–64) in 2050 is expected to increase dramatically in East Asian and European countries such as Japan (0.81), Korea (0.79), Spain (0.78), Greece (0.75), Italy (0.74), Portugal (0.71), Taiwan (0.71), and Hong Kong (0.71) [5].
In these countries, more targeted health plans and access to medical care are required. Moreover, the role of public transportation in mobility is even more important for the older population as car ownership decreases owing to safety and income restrictions. For example, in Hong Kong, dependence on public transit increased as the aging population intensified, with 93.6% of those aged 60 or older and 96.5% of those aged 80 or older [6]. Similarly, a German survey found that older people drive less and use more public transportation [7]. Seoul is a distinctive case as it has a 4 percent share of passenger cars among the elderly, which is low compared to the 24.5 percent share of the total population.
Particularly, an aging society emphasizes the importance of public services such as access to medical care and public transportation. However, older people’s growing dependence on public transit may lead to their social exclusion if there is an unequal distribution of public transit [8,9,10,11]. Social exclusion negatively affects an individual’s quality of life and social integration [12]. Therefore, policies to achieve an equitable city by improving the health and quality of life of vulnerable groups such as older adults, and creating appropriate activity opportunities, should support the equitable distribution of health and public transportation facilities [10].
This study aims to provide urban planning insights for creating a “city for all” in an aging society by focusing on medical care and public transportation. To simultaneously consider medical access and public transportation mobility, this study analyzes the primary care accessibility of elderly using public transit. Specifically, by finding the answers to the following research questions, we intend to obtain insights for inclusive cities. First, is the primary care accessibility of the elderly evenly distributed socially? To solve this question, this study analyzes the primary care accessibility of elderly individuals in Seoul using public transportation and compares this with accessibility for all age groups to determine whether there is some degree of inequality. Second, is the primary care accessibility of the elderly evenly distributed economically? By comparing the income level of the region with primary care accessibility, this study aims to analyze whether medical access is socially and economically equitable and provide policy implications for an equitable city.
2. Literature Review
2.1. Medical Accessibility
Access to primary healthcare facilities can be considered in terms of economic efficiency (medical utilization costs), acceptability (medical service satisfaction), availability (providing appropriate medical services), and geographical accessibility (traffic costs), among others [13]. In particular, geographical accessibility has potential for policy improvements, such as improving the physical accessibility of medical facilities. Therefore, numerous studies are being conducted regarding equity or spatial accessibility to healthcare [14,15]. The role of geographical distance in the interaction between medical access and health needs has also been emphasized [16,17,18].
Dai [19], for example, measured the residential segregation and access to healthcare facilities of Black Americans in Detroit using the 2SFCA (two-step floating catchment area), model. The results showed that living in areas with greater black segregation and poorer access to healthcare significantly increased the risk of a late diagnosis of breast cancer. Daly, et al. [20] also measured the spatial accessibility of older adults to primary care facilities using the E2SFCA (Enhanced two-step floating catchment area), model in Virginia. The researchers analyzed the correlation between spatial accessibility and avoidable hospitalization using regression analysis. The analysis showed that increased geographic access to primary care was associated with a lower risk of hospitalization among older people. Fortney, et al. [21] also found that access to healthcare facilities influences the availability of depression treatment services. In addition, if geographic access to primary care facilities is readily available, hospitalization for ambulatory care-sensitive conditions (ACSC) such as diabetes, hypertension, asthma, and heart failure may be reduced [20,22,23,24].
2.2. Equity
Equity, derived from the Latin aequitas, refers to justice by fairness, not by the routine application of rules [25]. In this sense, equity is not just a legal principle but an ethical/moral principle and comprehensively refers to the spirit and habits of right treatment [26,27]. Most importantly, the principle of equity means justice, and arguments about equity can only be based on justice [27].
Barry [28] described social justice as achievable via income and resource distribution based on individuals’ financial situation. Harvey also argued that social justice should imply just allocation [29]. As such, social justice has been described from various theoretical perspectives: liberal, utilitarian, social contract theory of justice, Marxist theory of justice, and communitarian justice. In particular, the political philosophy of the United States uses Rawls’ social contract theory of justice (1971) as the basis for its conceptualization of social equity [30]. In the social contract theory of justice, if society becomes unequal, equality in the allocation of basic rights and obligations to address inequality must be demanded. Socioeconomic inequality—for example, inequality in terms of property and power—can only be justified when all people, especially the least beneficiaries of society, are guaranteed the benefits that compensate for the inequality [29].
Therefore, Rawls suggests the principle of equality, in that no one can claim a particular advantage in the distribution of social values that meet human needs, and there is no reason to ignore certain damages inflicted on the individual. If some inequality exists in the social system that can improve the situation of all people compared to greater equality, Rawls persuasively presented that the “differential principle” should be justified and that such inequality should be allowed. Rawls further expanded the principles of equity that justify its contribution to the common good, with this contribution specifically focused on the poverty-stricken [29].
Equity based on the social contract theory of justice does not merely imply the same distribution but also the value judgment of distributive justice. Equity concerns whether the state of distribution is fair [31]. Vadrevu and Kanjilal [32] assessed medical equity in India by analyzing the relationship between economic circumstances and medical accessibility using E2SFCA analysis, the concentration curve, and the concentration index.
3. Materials and Methods
3.1. Study Area
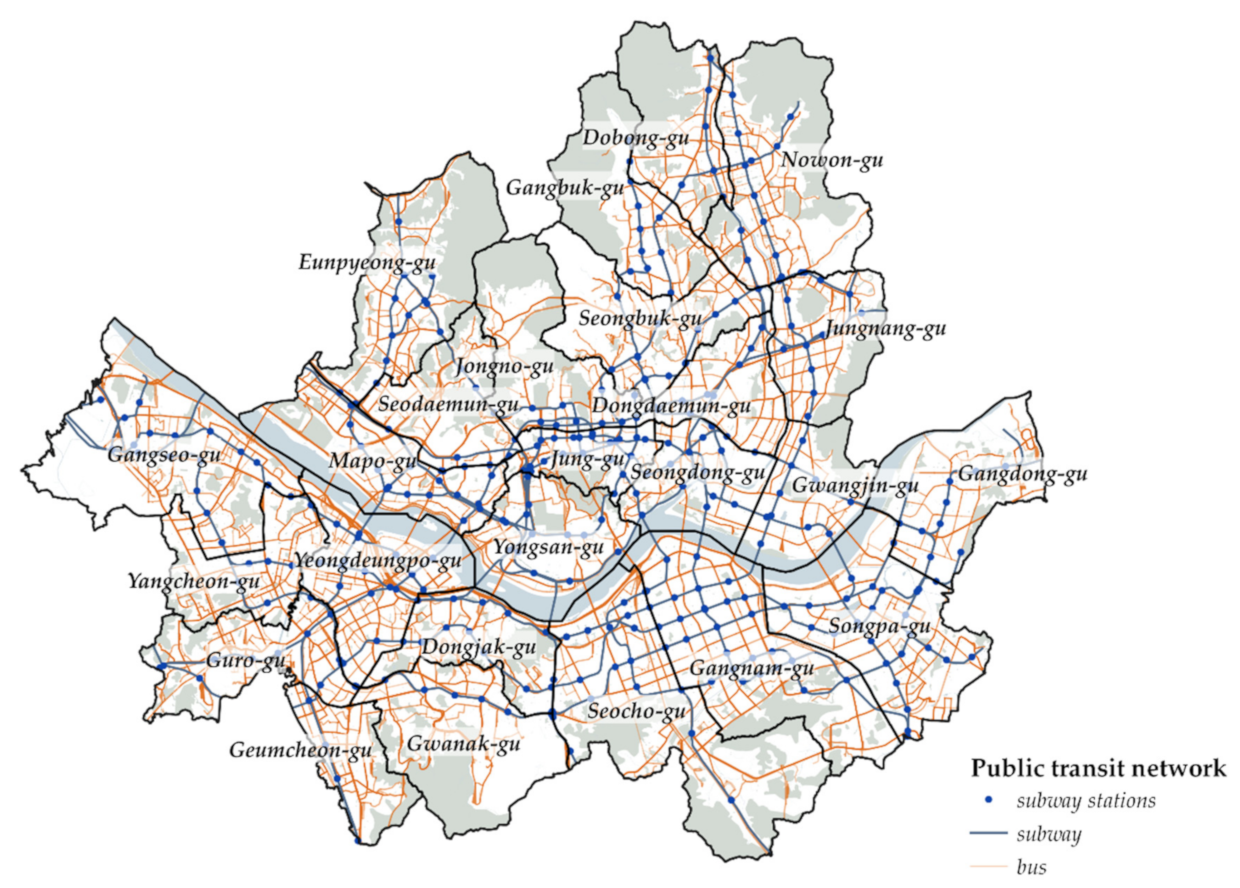
With about 9.6 million people residing within an area of 605.33 km2, Seoul has more than 10 subway lines and over 600 bus routes, making it relatively easy to use public transportation throughout the city (see Figure 1). In addition, Seoul’s share of public transit is 74% (2012), putting it at par with global cities that provide relatively good public transportation systems, such as Paris at 76.3% and Tokyo at 74.1% (2010). However, these numerical figures do not convey a true picture—there are many areas in Seoul with poor public transportation accessibility, and the level of public transport accessibility and mobility varies greatly by region. In particular, public transportation mobility in some suburbs of Seoul is less than half that of automobile mobility [33].
As for Seoul’s population characteristics, the proportion of the population aged 65 and over is 15.4% as of 2020, indicating an aged society. According to the National Statistical Office, this number will reach 24.2% by 2030, entering a super-aged society. In addition, with the increase in the aging population, the number of older single-person households has rapidly increased—it has more than doubled from 95,000 in 2005 to approximately 210,000 in 2017. Such households are mainly low-income households, with more than 90% of them earning less than 2 million won per month. As such, by observing the medical care access of older adults using public transportation in Seoul, we address important issues in establishing an equitable city in an aging society, including the complex social problems of an aging population, a decrease in income, an increase in medical demand, and an increase in dependence on public transportation.
Seoul provides big data (including real-time location, route, and transfer information for public transportation, including buses and subways) at no charge through an API. Therefore, it is possible to investigate medical accessibility based on accurate information using this API [34].
3.2. Research Scope and Method
The purpose of this study was to analyze the primary care accessibility and its equity in relation to people aged 65 years or over in Seoul, Korea. Until recently, only a few studies on medical accessibility in large cities have been conducted. This is due to the fact that research on urban access is less important than adequate and intuitive research on suburban areas [35]. However, owing to rapid demographic changes in recent times, accessibility and equity in large cities in developed countries is becoming an important research dimension. The decline in birth rates and longer life spans over the last half century have led to rapid aging in developed countries [36]. Therefore, recent studies have been conducted on dense metropolitan areas such as the Tokyo Metropolitan Area of Japan [37], Ile de France [38], and North Manhattan [39].
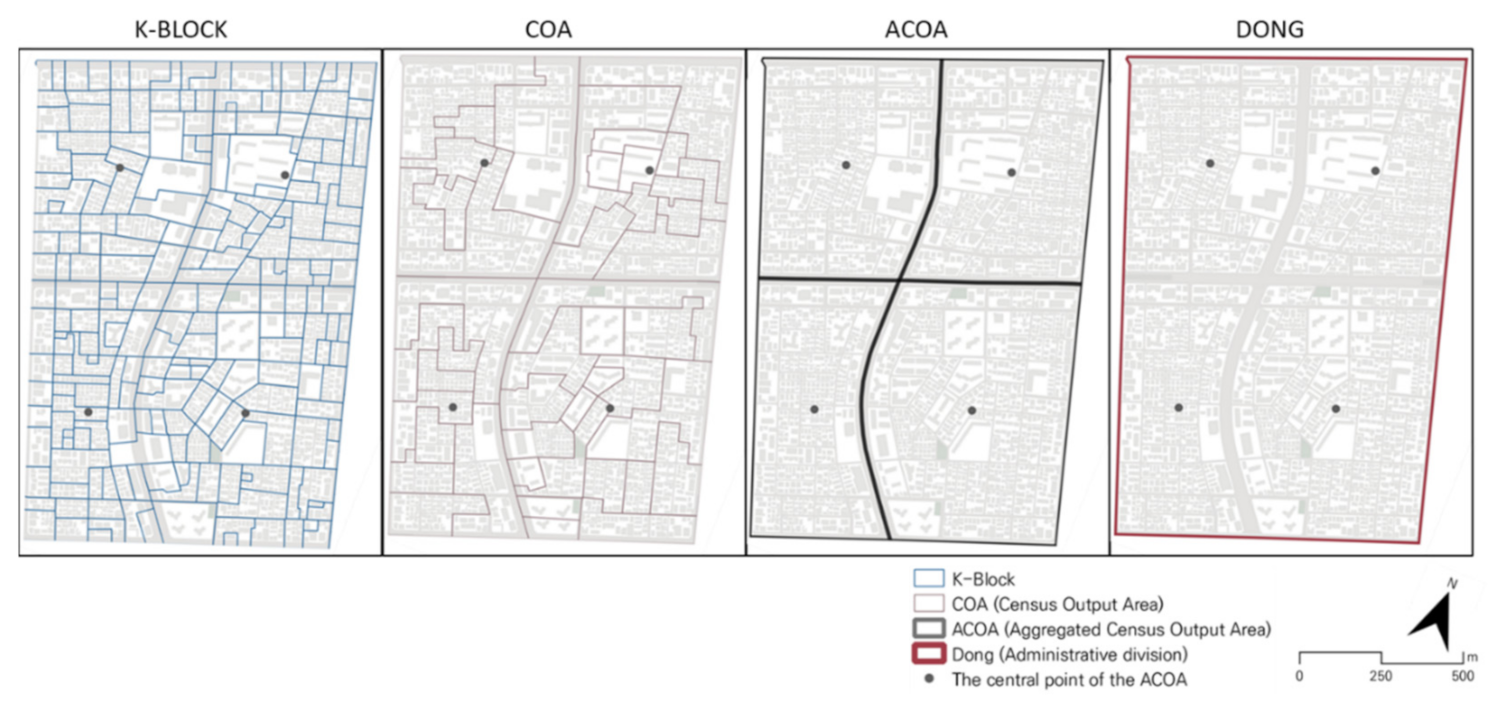
Primary care accessibility was analyzed by modifying the 2SFCA model. The starting point was the center of the aggregated census output area (ACOA; n = 1415), and the arrival point was the primary care facility. The COA is the minimum statistical counting area, based on population size (up to 500 people), socio-economic homogeneity (housing type, land price), and shape. As of 2017, there were a total of 19,253 districts in Seoul, with an average area of 31,436 m2. The threshold distance was defined as the distance reachable within 30 min of walking and public transportation use. Most previous studies use Euclidean distance, network distance, and travel time for accessibility analysis. However, considering that our study subjects were older adults, public transport travel time was considered a more appropriate measure.
To determine the public transport travel time, the OPEN API of the Korea Open Data Portal was used. Using these data, the threshold distance to a primary care facility accessible within 30 min depends on the level of public transport in the area; areas with high-density subway or bus routes have higher threshold distances to primary medical facilities than do low-density areas. These data reflect the differences in the city’s actual accessibility [40], allowing for a more appropriate measurement of accessibility without applying new models. The primary medical facilities were medical clinics and public health centers. Medical facilities for internal medicine or orthopedics used by older adults were selected and analyzed.
Spatial equity was analyzed using the concentration index and concentration curve of the annual average income of ACOA residents and primary care accessibility.
The procedure of the study is as follows. First, using modified 2SFCA, this study calculates the primary care accessibility for elderly in Seoul and analyzes the differences in accessibility by region. Second, it compares primary care access with that for all ages. Third, spatial equity is analyzed using the concentration curve and concentration index for the correlation between access to primary care facilities and income level.
3.3. Data
For the primary care accessibility analysis, public transport time data between ODs were collected using the “public transit route inquiry service” of the Korea Open Data Portal, OPEN API. The input data were the latitude and longitude coordinates of the departure and arrival points, and the output data were the route and time taken when travelling by bus or the subway. Data collection using the API was performed using the R 3.3 version, a programming language developed by the University of Auckland.
The API utilized in this research is a service that is also used by smartphone applications for pathfinding, such as SK T-map. We calculated primary medical accessibility from 751,304 data sets of less than 30 min of transit time between the central point of the ACOA and primary medical facilities. In the API, if the transit time was less than 5 min, the result was not loaded. In using the travel time for analysis, we measured the pedestrian network distance using GIS and multiplied it by the average walking speed of Korean older adults (0.66 m/s).
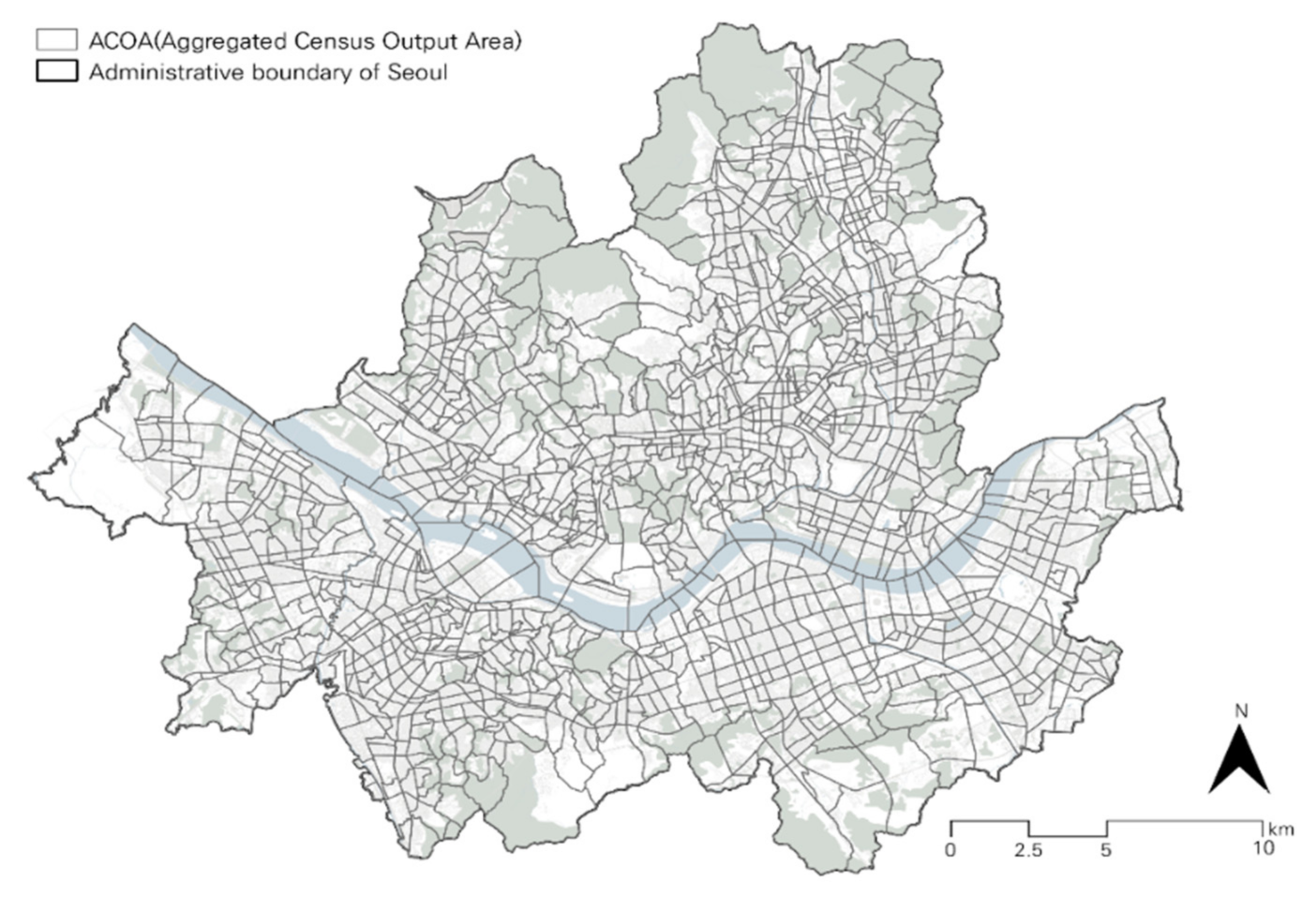
The starting point of the OD in this study was the central point of the ACOA in Seoul, Korea. The ACOA was established to account for the daily API quota and analysis accuracy. The ACOA is a unit comprising approximately ten COAs (see Figure 2). This area is larger than the COA and narrower than the dong (administrative division) (see Figure 3).
Demographic data from 2017 were used to obtain information on the total population and the population aged 65 or older by ACOA.
The arrival point used “clinic” data from industry-specific license data provided by the Korea Local Information Research and Development Institute. Data such as the clinic address, number of doctors, and medical departments were obtained, and the addresses were geocoded and used for analysis. We extracted 4624 internal medicine or orthopedic clinics in Seoul as of 31 December 2017. According to the 2015 Korean Medical Panel data, hypertension and arthritis are the most common causes of clinic visits by older people. Therefore, we chose internal medicine and orthopedics clinics as sources of primary care services.
To determine the level of medical service in each clinic, the 2017 (13th) hypertension adequacy evaluation data provided by the Health Insurance Review and Assessment Service (HIRAS) were used. The HIRAS evaluates healthcare facilities and publishes its results to improve the quality of hypertension care. The evaluation criteria consist of prescription persistence evaluation (continuous management of hypertension evaluation) and prescription evaluation (appropriateness of drug prescription). Five subjects were evaluated. Regarding clinics in Seoul, 1010 received “good” evaluations and were released; 947 (20.5%) of the 4624 clinics used in this study had received “good” evaluations. The clinic’s care level was considered a way of weighting these clinics.
For the equity analysis, we used K-Atlas income data to calculate the median income of local residents for each ACOA. K-Atlas income data are provided through the Korea Credit Bureau’s (KCB) collection or statistical estimation of income information for approximately 43 million individuals in small-area units (K-blocks). Approximately 20 K-blocks are bordered by one ACOA. The annual income estimates for each ACOA are based on the median of the K-blocks’ annual income estimates.
3.4. Measurement of Medical Accessibility
To measure medical accessibility, Gesler [41] proposed a comprehensive spatial classification method, and Guagliardo [35] proposed four methods for measuring accessibility based on recent analyses.
The provider-to-population ratio is intuitive and widely used for measuring spatial accessibility, as it does not require a geographical information system (GIS) program or expertise. Accessibility is derived from the number of doctors (volume of medical care, including number of beds) relative to the number of people in a particular area and is used for research related to ACSC. However, there is a limitation to accessibility determination associated with non-physically-adjacent suppliers located outside of a regional boundary.
The distance (or time) to the nearest medical service provider is a commonly used method for measuring spatial accessibility. A standard measure of spatial accessibility in rural areas is the distance from the center of residences to the nearest supplier using Euclidean distance, network distance, or time.
The average distance (or time) to a medical service supplier is a method of averaging and measuring the moving distance (time) from all suppliers within a space. This method also has the limitation of MAUP (Modifiable areal unit problem).
Gravity models have been developed to interpret retail activities or land use plans in cities. Gravity models represent potential interactions between all populations and services within reasonable distances while discounting other populations as the distance increases.
Two-Step Floating Catchment Area (2SFCA)
Recently, the 2SFCA an improvement over the gravity model, has been developed and used in most space accessibility studies. This method was first used by Luo and Wang [16] who improved the floating catchment area (FCA) model that Peng [42] used to study job access in cities [35,43]. The 2SFCA calculates accessibility via two steps. First, the supply capacity of the supply facilities (number of doctors or beds) relative to the population of the total demand area (threshold area) is calculated for each supply facility (clinic) (Step 1). Next, the value of Step 1 is summed by the demand area (threshold area) (Step 2).
divides the supply of medical facilities (=number of doctors in hospital , ) by population in the threshold distance . In the second step, is calculated by summing the values of the medical facilities within the threshold distance around the population center point .
The resulting spatial accessibility, , can be interpreted as the number of doctors per population in the demand area. The 2SFCA model is intuitive for interpreting the results. This model improves supply distribution even if one supplier (hospital) has jurisdiction over two demand sites [44]. In addition, the model is not limited to administrative boundaries, which prevents MAUP and considers regional differences in accessibility [17,45]. However, since the accessibility of facilities in a service area is assumed to be similar, accessibility can be overestimated by ignoring distance decay [17]. Recently, various modified models of the 2SFCA have been developed for increasingly sophisticated analyses [46]. However, these models offer no significant improvement over existing models [47]. In addition, no model has yet been proposed that considers the innovative quality of care within the FCA framework [48].
In this study, we modified the 2SFCA model for a more sophisticated analysis. Specifically, we first incorporated the distance decay effect using weights that decreased as the distance between the population center and the clinics increased. The threshold distance utilizes travel time, which is more stable than travel distance [49,50]. Second, we also considered the quality of care provided by the clinic.
This 2SFCA model has a limitation in that any clinic located within the threshold distance (catchment) has a weight of 1 and other clinics have a weight of 0, which does not reflect the difference in accessibility across distance. Subsequently, various modified models have been developed. Representative models include the step decay weights and continuous decay weights.
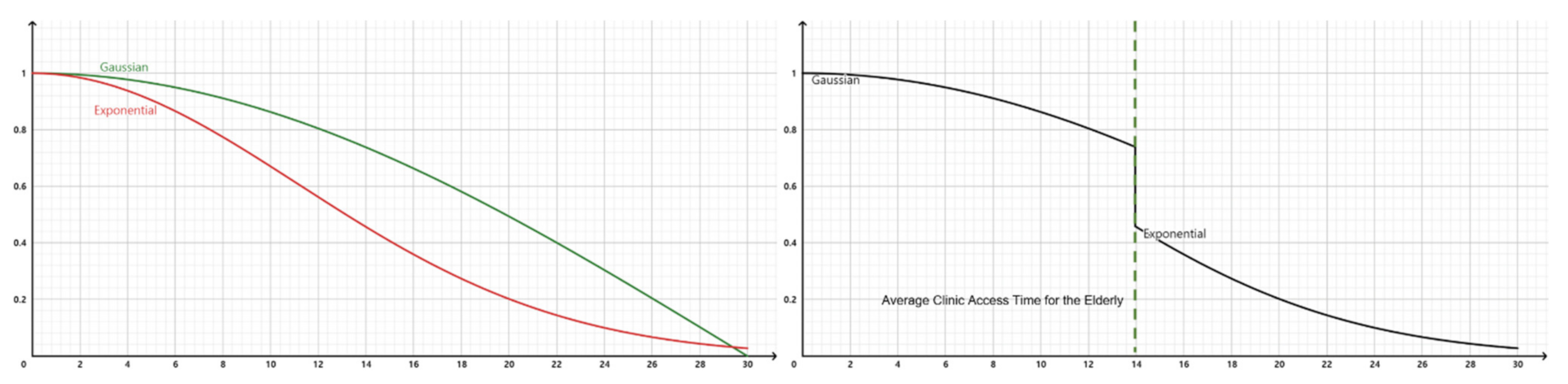
Previous studies have reported that continuous decay weights are more accurate for accessibility measurements compared to step decay weights. Luo and Qi [51] found that the E2SFCA model using step decay weights is more suitable than a model without decay weights. McGrail [52] found that continuous decay weights are more appropriate than step decay weights in a study of primary care accessibility in Victoria, Australia. Recent studies have used Gaussian functions [19,53] and exponential functions [54] to express continuous decay weights. Park, Woo, and Kim [17] used a mixture of Gaussian, exponential, and quadrature functions for their analysis.
This study adopted the Gaussian and exponential functions, as in Park, Woo and Kim [17]. According to Korea Health Panel (2015) data, the access time to clinics for those aged 60 or older has decreased dramatically to an average time of 13.96 min. Therefore, this study uses a Gaussian function, which has a relatively smooth curve, up to the average time and uses the exponential function above the average level to reflect continuous decay weights (see Figure 4).
In addition, hypertension adequacy evaluation data from the HIRAS were used to reflect the level of medical service. Approximately 21% of the clinics used in the analysis received a “good” grade, therefore a weight of 1 was applied to “good” clinics and a weight of 0.79 was applied to the other clinics.
Since this study aims to calculate clinic accessibility, the supply capacity (Sj) of each clinic was set to the number of doctors per clinic, not the number of beds.
In addition, the maximum threshold time () was set to 30 min based on a previous study, and the distance () from the population center point to the clinic was used for the transit time data in the OPEN API. Based on the aforementioned parameters, this study calculated medical accessibility by modifying the 2SFCA.
In the first stage of the 2SFCA, the medical service level weight () and distance decay weight () of each clinic were considered (see Equation (3)).
3.5. Equity
Spatial equity in this study was measured using a concentration index and concentration curve. The concentration index and curve were designed to measure the inequality in the distribution of one variable to another [55]. In particular, they were designed to measure the relationship between socioeconomic characteristics and health inequality [56]. Van Doorslaer, et al. [57] proposed the following basic conditions for calculating the scale of health inequality: (1) reflecting socioeconomic characteristics; (2) covering the entire population; and (3) reflecting changes as a result of differences in distribution among the classes. The concentration index is an indicator that meets these requirements and is widely used in health-related studies. The analysis utilizes DAD (Distributive Analysis/Analyze Distributive) 4.6, a specialized tool for equity analysis.
The concentration index is applied to health-related research by calculating the Lorentz curve and the Gini coefficient, which is the same as the Lorentz curve and the calculation process. In this study, after ranking the annual income variable of the ACOA, the cumulative proportion of this group was plotted against the cumulative proportion of primary care accessibility [58].
The concentration index is twice the area between the concentration curve and the 45° line and is between −1 and +1. If the concentration curve is below the 45° line, the concentration index will be positive (+), indicating that the distribution is concentrated in the high-income class. If the concentration curve is located above the 45° line, the concentration index has a negative (–) value. This indicates that the distribution is concentrated in the low-income group [59].
4. Results
4.1. Basic Analysis Result
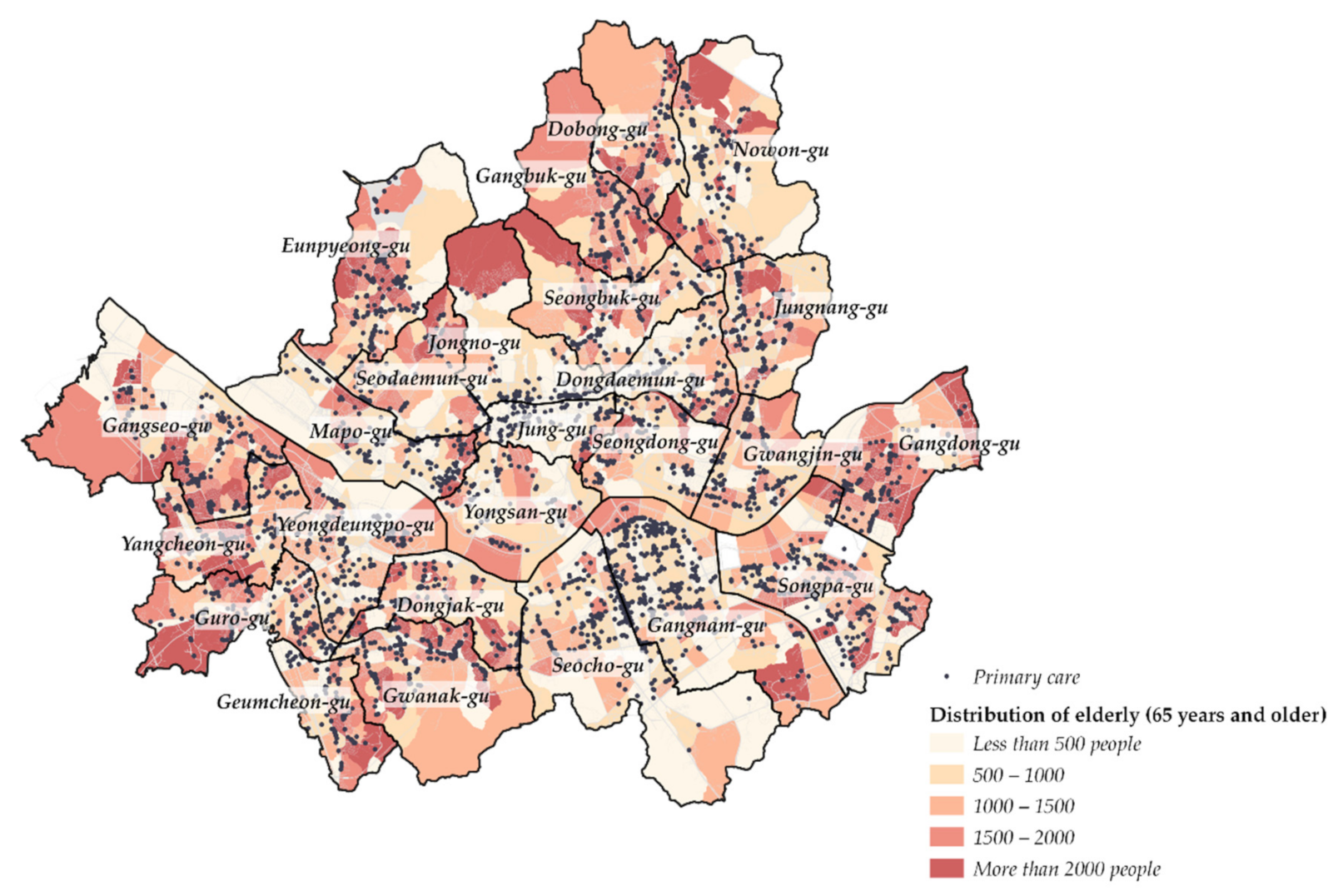
The average number of doctors per clinic in this study was 1.87. The number of clinics with only one doctor was 3118 (67.4%), and 840 (18.2%) had two doctors (see Table 1). Consequently, 85.6% of all clinics were small, with two doctors or fewer. The Seodaemun-gu Public Health Center was the largest with 46 doctors. On average, there were approximately 881 older adults per ACOA. The ACOA in Sinjeong 4-dong, Yangcheon-gu, had the largest population of older adults (3722). Those over 65 years of age primarily lived in Yangcheon-gu, Gangseo-gu, Eunpyeong-gu, Dobong-gu, Gangdong-gu, and Dongjak-gu (see Figure 5). The average annual income in all ACOAs was 33.43 million won ($27,500), with the highest annual income in an ACOA being 105.3 million won ($86,700). The average number of clinics that can be reached within 30 min of transit time is approximately 535 per ACOA; for the ACOA in Haengdang-1 dong, Seongdong-gu, this number was 957 clinics. To evaluate the performance of the public transportation system, we analyzed the distance to the clinic using public transportation in different time frames. When the travel time was under 15 min, the average distance was approximately 1.5 km. The maximum distance that could be covered within 15 min was approximately 3.8 km. This result was from an ACOA in Yangpyeong 2-dong, Yeongdeungpo-gu, to a clinic in Seogyo-dong, Mapo-gu. When the travel time was less than 30 min, the average distance was 4.2 km, with a maximum of 11.8 km.
4.2. Medical Accessibility Analysis
4.2.1. Primary Care Accessibility
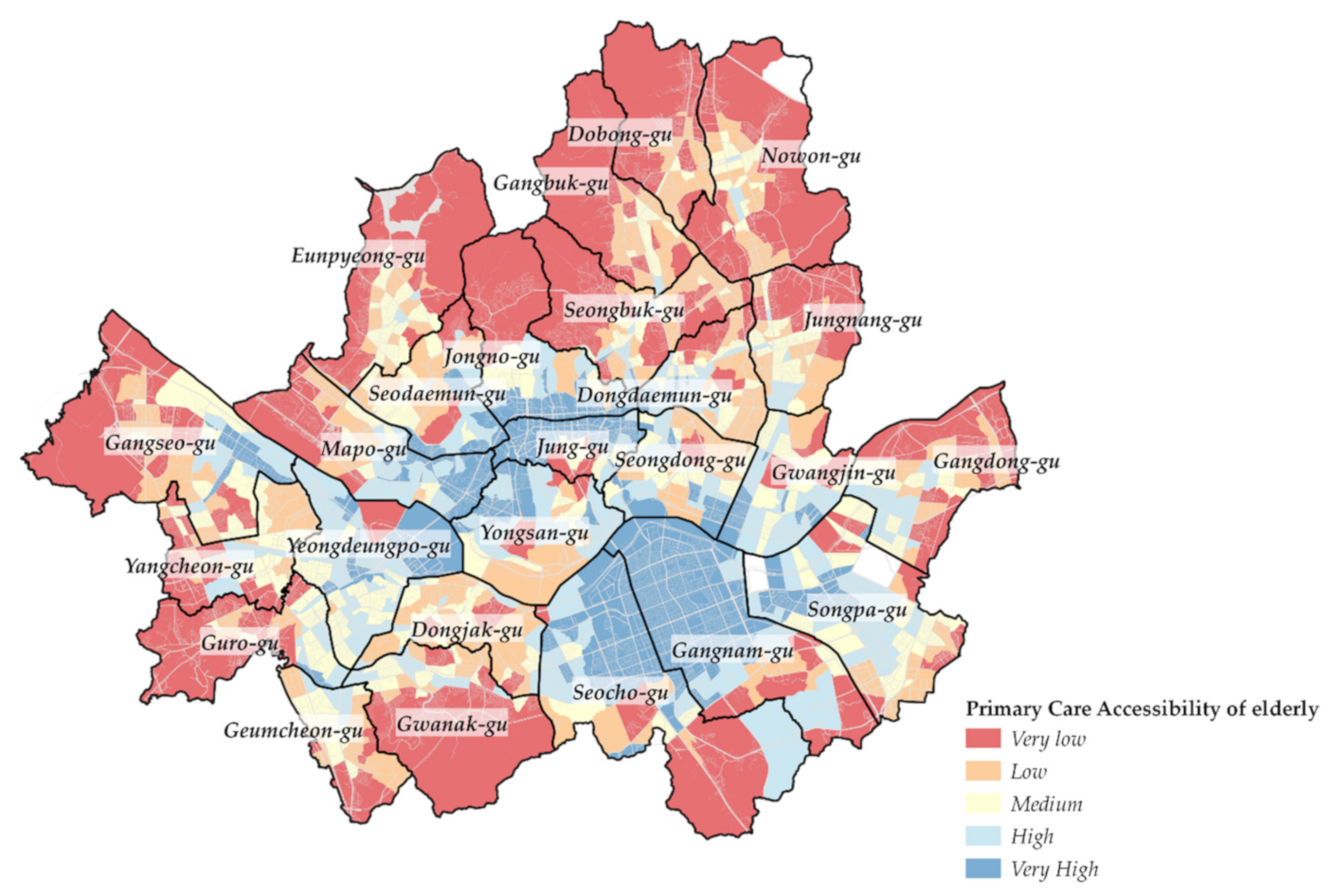
The results of the primary care accessibility analysis for older adults are shown in Figure 6. Since accessibility refers to the number of doctors per person, the high accessibility to medical care means that the number of doctors accessible to the elderly is relatively large. As a result of the analysis, the primary care accessibility of the elderly was highly analyzed in Jongno-gu, Jung-gu, Yeongdeungpo-gu, Gangnam-gu, and Seocho-gu, which are the three major centers of Seoul. The ACOA in Nonhyeon 2 dong, Gangnam-gu, had the highest primary care access, and 0.043 doctors were available per elderly. In addition to Nonhyeon 2 dong, the ACOAs in Seocho 2 dong, and Seocho 4 dong, Seocho-gu, also showed high medical accessibility. This area is judged to be the result of a mismatch between the residential area of the elderly and the location of the public transportation and medical system. As shown in Figure 5, the density of the elderly was low in these areas, while the density of subways, buses (see Figure 1), and primary care was relatively high.
On the other hand, in the Sanggye 3 · 4 dong and Sanggye 5 dong areas, Nowon-gu, primary care accessibility was less than 0.0003, 140 times less than that in Gangnam-gu. In general, it showed low primary care accessibility in fringe areas of Seoul. It is understood that these areas were not able to provide adequate medical and public transportation services due to restrictions on land use due to the green belt.
Also, there were areas with low primary care accessibility even though these areas are located inside the city. In Dongjak-gu and Dongdaemun-gu, many areas have low primary care accessibility. It is understood that these areas have relatively low subway station density or are located in curvilinear road networks and hills, so bus accessibility is relatively low. Next, the factors influencing this public transportation mobility on medical accessibility were additionally analyzed.
4.2.2. Medical Accessibility and Public Transport Mobility
Pearson’s correlation coefficient was used to analyze whether public transport mobility affected medical access. Public transport mobility was analyzed by distinguishing the neighborhood and regional public transport mobility. The neighborhood public transport mobility was defined as the maximum public transport speed for 15 min (Equation (6)), and the regional public transport mobility was defined as the maximum public transport speed for 30 min (Equation (7)).
The correlation analysis of the primary care accessibility of older adults showed a positive correlation with the public transport mobility; the higher the public transport mobility, the higher the medical accessibility (see Table 2). The neighborhood public transport mobility (0.205) was found to have a high correlation with primary care accessibility compared to the regional public transport mobility (0.098). Regarding clinics, public transport mobility in neighborhood units, reflecting distances traveled within 15 min, have a greater impact on older people’s primary care accessibility than do public transport mobility that serve longer distances.
4.2.3. Deviations between Regions
To examine regional deviations in primary care accessibility, the coefficient of variation (CV) for primary care accessibility for older adults and for all ages was examined. The primary care accessibility of older adults was 0.0079, with a standard deviation of 0.0059 and a CV of 0.7487. The primary care accessibility analysis of all age groups showed an average of 0.0010, standard deviation of 0.0007, and CV of 0.6758. The CV was higher for the older group (0.7487) than for all age groups (0.6758). Therefore, regional deviations were higher in primary care accessibility for older people.
4.3. Equity Analysis
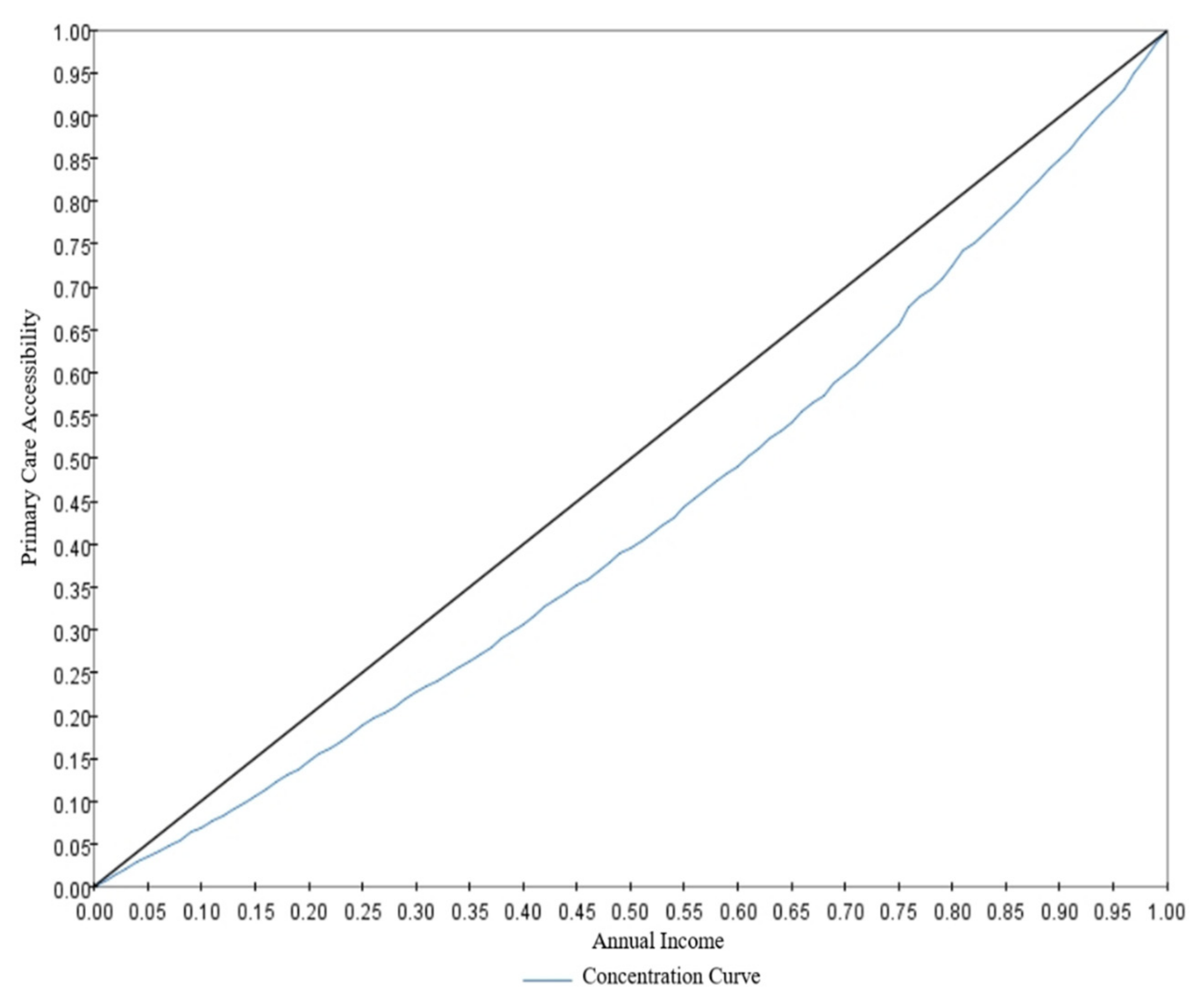
The concentration curve and index were used to determine whether there was social equity in the primary care accessibility of older people. The concentration index was positive, and the concentration curve in Figure 7 was located below the 45° line. Therefore, living in a high-income area is advantageous for primary care accessibility in this population group.
5. Discussion
Improving access to essential public services, such as healthcare and public transport, has a significant positive impact on the quality of life of older people and reduces social inequality [1,60,61,62]. Therefore, this study analyzed the primary care accessibility of older people using public transportation in Seoul and examined whether their accessibility is socially and economically equitable. In doing so, we attempted to derive policy implications for creating a more inclusive city despite significant social changes, such as an aging population.
The study confirmed that primary care accessibility is low in fringe areas of Seoul, especially for older people, and that income and primary care accessibility did not have an equitable relationship. This is consistent with previous results for Seoul focusing on a specific perspective (low public transport access in fringe areas of Seoul [63,64], poor public transport accessibility among older adults [65,66], and unequal doctor distribution [67,68]). In addition, unlike many accessibility studies that focus on equality in treatment and health [43], this study considered the socioeconomic equality of medical opportunities from the perspective of primary care accessibility using public transportation. This enables a more complex explanation of accessibility and can contribute to the existing literature on accessibility and equity by providing valuable data for related research. Studies in the United States [69,70] and China [71] analyzed that medical accessibility affects the rate of inpatients for ACSCs. Therefore, chronic disease management and prevention requires ready access to primary care facilities. The main result of this study is that spatial accessibility inequity equates to an inequity in chronic disease management and prevention. The potential costly sequelae of high blood pressure, for example, may be more common in the low income group as the result of the spatial accessibility inequity.
From a regional planning perspective, this study found that there are geographical differences in older people’s primary care accessibility. Their primary care accessibility was high in Gangnam-gu, Seocho-gu, Jung-gu, and Jongno-gu, where transportation and resources are relatively concentrated. Conversely, primary care accessibility was low in Dongjak-gu, Gwanak-gu, and Dongdaemun-gu, where the street network is curvilinear, there is a high density of older people, income is relatively low, and the number of clinics is insufficient.
These findings can be interpreted in two ways. The first concerns the location of medical facilities. Similar to the viewpoint suggesting the need for policies owing to the unequal spatial distribution of medical professionals [38], in Seoul, even after controlling for social and economic factors, the opening rate of clinics in areas with a high density of older adults is low [67]. The socioeconomic characteristics of the neighborhood influence the location of medical facilities. It is debatable whether primary care facilities should be considered public goods or services, and whether their location should be controlled by policy. However, considering the importance of primary care facilities in an aging society, the perspective of primary care accessibility using public transportation in this study, beyond the discussion of medical facility locations, can provide clues to solve the problem of unequal distribution of medical professionals.
The second is the perspective of street network patterns and the topographical characteristics of Seoul. In densely developed downtown Seoul, the curvilinear street network pattern formed by small blocks reduces the use of public transportation [72]. Simultaneously, Seoul is dotted with hilly areas in the city center. Residential areas located on hills have relatively poor accessibility to public transportation compared to residential areas with grid-type plans. In the case of Seoul, a free shuttle bus for older adults has been operating since 2000, but there is a limitation in that it is restricted to certain areas. It is necessary to operate a small free shuttle bus for older people in areas with low access to medical care, which is an important finding of this study. In particular, it is necessary to prioritize the public supply of medical resources, such as public health centers, on the shuttle bus route. In addition, the findings indicate that neighborhood-based public transportation modes, such as town buses and branch-line buses, are more important than regional-level public transportation modes, such as subways or trunk buses for primary care accessibility. Based on this, policies such as the expansion of town buses and branch buses or the redesign of routes should be considered.
We suggest policy implementation based on our analysis of primary care accessibility and its equity for older people in Seoul. However, our accessibility model based on public transportation use did not reflect the qualitative factors of public transportation, such as the number of transfers and waiting time for transfers. If the data and analysis methods are reinforced, we expect more in-depth implications to be derived.
6. Conclusions
For an equitable city in an aging society, urban planning in relation to medical care and public transportation is critical. By analyzing the primary care accessibility of elderly individuals using public transit, this study provides urban planning implications for a more equitable city.
First, integrated plans are required to create a “city for all”. Land use, health and welfare, and public transportation plans are independently designed with a focus on efficiency [73,74]. For example, the distribution of socially disadvantaged people—for example, older people—and public service facilities—such as medical facilities—is not considered in public transportation plans. To create an inclusive city, integrated plans are required. Habitat III’s New Urban Agenda presents integrated plans as a primary action plan for creating a “city for all”. This study, which analyzes older people’s access to medical care considering public transportation mobility, supports this implementation plan.
Second, this study’s results can facilitate the efficient distribution of resources for equity. Currently, public transportation projects consist mainly of large-scale projects, such as subway and light rail construction. The results of this study—that local public transportation services such as village buses significantly affect primary care accessibility—can help efficiently distribute resources, via small, relatively low-cost public transport infrastructure investments for inclusive cities. This can have implications for cities such as Seoul, Tokyo, Paris, and Hong Kong, which already have a high-level public transport infrastructure.
Third, this study analyzed the primary care accessibility of older adults using public transportation API big data and presented implications for urban planning. Recently, new technologies such as Internet of Things and artificial intelligence have been introduced into cities to create “smart cities”. However, it is true that while many smart cities emphasize technical aspects such as resolving traffic congestion, waste disposal, and energy saving, the use of urban planning has not progressed significantly. This study using the public transportation API is meaningful in that it presents urban planning solutions through big data analysis in smart cities such as Seoul.
Through such policy improvement, older people who are marginalized from medical services will receive medical services near their residence. This will reduce social costs and bring the city closer to a “city for all”.
Author Contributions
Y.Y. conceived the idea and designed this research. J.P. developed the idea for academic research and reviewed the manuscript as a corresponding author. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. NRF-2019R1A2C1088467).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Martínez, L. Health differences in an unequal city. Cities 2021, 108, 102976. [Google Scholar] [CrossRef]
- Zuo, T.; Wei, H.; Chen, N.; Zhang, C. First-and-last mile solution via bicycling to improving transit accessibility and advancing transportation equity. Cities 2020, 99, 102614. [Google Scholar] [CrossRef]
- Bocarejo, S.J.P.; Oviedo, H.D.R. Transport accessibility and social inequities: A tool for identification of mobility needs and evaluation of transport investments. J. Transp. Geogr. 2012, 24, 142–154. [Google Scholar] [CrossRef]
- New Urban Agenda. United Nations Conference on Housing and Sustainable Urban Development (Habitat III) in Quito, Ecuador; United Nations General Assembly (A/RES/71/256). 2017. Available online: https://uploads.habitat3.org/hb3/NUA-English.pdf (accessed on 1 August 2022).
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2019: Highlights (ST/ESA/SER.A/430). 2019. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf (accessed on 1 August 2022).
- Wong, R.; Szeto, W.; Yang, L.; Li, Y.; Wong, S. Public transport policy measures for improving elderly mobility. Transp. Policy 2018, 63, 73–79. [Google Scholar] [CrossRef] [Green Version]
- Shrestha, B.P.; Millonig, A.; Hounsell, N.; Mcdonald, M. Review of public transport needs of older people in European context. J. Popul. Ageing 2017, 10, 343–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casas, I. Social exclusion and the disabled: An accessibility approach. Prof. Geogr. 2007, 59, 463–477. [Google Scholar] [CrossRef]
- Farrington, J.; Farrington, C. Rural accessibility, social inclusion and social justice: Towards conceptualisation. J. Transp. Geogr. 2005, 13, 1–12. [Google Scholar] [CrossRef]
- Wang, H.; Kwan, M.-P.; Hu, M. Social exclusion and accessibility among low-and non-low-income groups: A case study of Nanjing, China. Cities 2020, 101, 102684. [Google Scholar] [CrossRef]
- Preston, J.; Rajé, F. Accessibility, mobility and transport-related social exclusion. J. Transp. Geogr. 2007, 15, 151–160. [Google Scholar] [CrossRef]
- Özkazanç, S.; Sönmez, F.N.Ö. Spatial analysis of social exclusion from a transportation perspective: A case study of Ankara metropolitan area. Cities 2017, 67, 74–84. [Google Scholar] [CrossRef]
- Penchansky, R.; Thomas, J.W. The concept of access: Definition and relationship to consumer satisfaction. Med. Care 1981, 19, 127–140. [Google Scholar] [CrossRef]
- Andersen, R.M. Revisiting the behavioral model and access to medical care: Does it matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef]
- Shin, H.-S.; Lee, S.-H. Factors affecting spatial distance to outpatient health services. Health Policy Manag. 2011, 21, 23–43. [Google Scholar] [CrossRef] [Green Version]
- Luo, W.; Wang, F. Measures of spatial accessibility to health care in a GIS environment: Synthesis and a case study in the Chicago region. Environ. Plan. B Plan. Des. 2003, 30, 865–884. [Google Scholar] [CrossRef] [Green Version]
- Park, J.H.; Woo, H.J.; Kim, Y.H. Measures of spatial accessibility to emergence medical services with a modified three-step floating catchment area model: A case study of the Chungnam province. J. Korean Assoc. Reg. Geogr. 2017, 23, 388–402. [Google Scholar]
- McGreevy, M.; Harris, P.; Delaney-Crowe, T.; Fisher, M.; Sainsbury, P.; Riley, E.; Baum, F. How well do Australian government urban planning policies respond to the social determinants of health and health equity? Land Use Policy 2020, 99, 105053. [Google Scholar] [CrossRef]
- Dai, D. Black residential segregation, disparities in spatial access to health care facilities, and late-stage breast cancer diagnosis in metropolitan Detroit. Health Place 2010, 16, 1038–1052. [Google Scholar] [CrossRef]
- Daly, M.R.; Mellor, J.M.; Millones, M. Do avoidable hospitalization rates among older adults differ by geographic access to primary care physicians? Health Serv. Res. 2018, 53, 3245–3264. [Google Scholar] [CrossRef]
- Fortney, J.; Rost, K.; Zhang, M.; Warren, J. The impact of geographic accessibility on the intensity and quality of depression treatment. Med. Care 1999, 37, 884–893. [Google Scholar] [CrossRef]
- Weissman, J.S.; Gatsonis, C.; Epstein, A.M. Rates of avoidable hospitalization by insurance status in Massachusetts and Maryland. JAMA 1992, 268, 2388–2394. [Google Scholar] [CrossRef]
- Ansari, Z. The concept and usefulness of ambulatory care sensitive conditions as indicators of quality and access to primary health care. Aust. J. Prim. Health 2007, 13, 91–110. [Google Scholar] [CrossRef]
- Kim, D.; Ahn, Y. Built environment factors contribute to asthma morbidity in older people: A case study of Seoul, Korea. J. Transp. Health 2018, 8, 91–99. [Google Scholar] [CrossRef]
- Merriam-Webster, I. Merriam-Webster’s Dictionary of Law; Merriam-Webster: Springfield, MA, USA, 1996. [Google Scholar]
- Frederickson, H.G. New Public Administration; University Alabama Press: Tuscaloosa, AL, USA, 1980. [Google Scholar]
- Lim, E. Searching for a theoretical ground of social equity: Focusing on R. Dworkin’s ‘equality of resources’. Korean J. Public Adm. 2007, 45, 1–22. [Google Scholar]
- Barry, B. Theories of Justice: A Treatise on Social Justice, Vol. 1; University of California Press: Oakland, CA, USA, 1989; Volume 16. [Google Scholar]
- Bae, M. A ‘Social Justice’ in Geography of Welfare. J. Korean Assoc. Reg. Geogr. 2003, 9, 546–558. [Google Scholar]
- Lim, E. Searching for the Justice-Theoretical Ground of Social Equity: Focus on Walzer’s Theory of Pluralistic Justice. Korean Public Adm. Rev. 2009, 43, 1–18. [Google Scholar]
- Lucy, W.H.; Gilbert, D.; Birkhead, G.S. Equity in local service distribution. Public Adm. Rev. 1977, 37, 687–697. [Google Scholar] [CrossRef]
- Vadrevu, L.; Kanjilal, B. Measuring spatial equity and access to maternal health services using enhanced two step floating catchment area method (E2SFCA)–a case study of the Indian Sundarbans. Int. J. Equity Health 2016, 15, 87. [Google Scholar] [CrossRef] [Green Version]
- Yoo, G.-s.; Kim, S.; Yeon, J.; Kim, J. Microscopic Evaluation of the Quality of Public Transportation Service by Region in Seoul; The Seoul Institute: Seoul, Korea, 2020.
- Yenisetty, P.T.; Bahadure, P. Assessing accessibility to ASFs from bus stops using distance measures: Case of two Indian cities. Land Use Policy 2021, 108, 105567. [Google Scholar] [CrossRef]
- Guagliardo, M.F. Spatial accessibility of primary care: Concepts, methods and challenges. Int. J. Health Geogr. 2004, 3, 3. [Google Scholar] [CrossRef] [Green Version]
- Lutz, W.; Sanderson, W.; Scherbov, S. The coming acceleration of global population ageing. Nature 2008, 451, 716–719. [Google Scholar] [CrossRef]
- Xia, T.; Song, X.; Zhang, H.; Song, X.; Kanasugi, H.; Shibasaki, R. Measuring spatio-temporal accessibility to emergency medical services through big GPS data. Health Place 2019, 56, 53–62. [Google Scholar] [CrossRef]
- Lucas-Gabrielli, V.; Mangeney, C. Comment améliorer les mesures d’accessibilité aux soins pour mieux cibler les zones sous-denses? Rev. D’épidémiologie Et De St. Publique 2019, 67, S25–S32. [Google Scholar] [CrossRef]
- Jin, Z.; Northridge, M.E.; Metcalf, S.S. Modeling the influence of social ties and transportation choice on access to oral healthcare for older adults. Appl. Geogr. 2018, 96, 66–76. [Google Scholar] [CrossRef]
- Ma, X.; Ren, F.; Du, Q.; Liu, P.; Li, L.; Xi, Y.; Jia, P. Incorporating multiple travel modes into a floating catchment area framework to analyse patterns of accessibility to hierarchical healthcare facilities. J. Transp. Health 2019, 15, 100675. [Google Scholar] [CrossRef]
- Gesler, W. The uses of spatial analysis in medical geography: A review. Soc. Sci. Med. 1986, 23, 963–973. [Google Scholar] [CrossRef]
- Peng, Z.-R. The jobs-housing balance and urban commuting. Urban Stud. 1997, 34, 1215–1235. [Google Scholar] [CrossRef]
- Neutens, T. Accessibility, equity and health care: Review and research directions for transport geographers. J. Transp. Geogr. 2015, 43, 14–27. [Google Scholar] [CrossRef]
- Cho, D.-H.; Shin, J.-Y.; Kim, K.-Y.; Lee, G.-H. An analysis of spatial accessibility to public healthcare services in rural areas. J. Korean Assoc. Reg. Geogr. 2010, 16, 137–153. [Google Scholar]
- Kim, J.-G.; Hong, I.-P.; Lee, J.-C.; Kim, C.-B.; Lee, W.-J.; Ko, E.-B. Spatial Distribution of Public Healthcare Personnel. J. Korea Plan. Assoc. 2014, 49, 161–174. [Google Scholar] [CrossRef]
- Freiria, S.; Tavares, A.O.; Julião, R.P. The benefits of a link-based assessment of health services accessibility: Unveiling gaps in Central Region of Portugal. Land Use Policy 2019, 87, 104034. [Google Scholar] [CrossRef]
- Plachkinova, M.; Vo, A.; Bhaskar, R.; Hilton, B. A conceptual framework for quality healthcare accessibility: A scalable approach for big data technologies. Inf. Syst. Front. 2018, 20, 289–302. [Google Scholar] [CrossRef]
- Delamater, P.L. Comment on “A Conceptual Framework for Quality Healthcare Accessibility: A Scalable Approach for Big Data Technologies”. Inf. Syst. Front. 2018, 20, 303–309. [Google Scholar] [CrossRef]
- Cheng, G.; Zeng, X.; Duan, L.; Lu, X.; Sun, H.; Jiang, T.; Li, Y. Spatial difference analysis for accessibility to high level hospitals based on travel time in Shenzhen, China. Habitat Int. 2016, 53, 485–494. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Du, F.; Huang, J.; Liu, Y. Access to hospitals: Potential vs. observed. Cities 2020, 100, 102671. [Google Scholar] [CrossRef]
- Luo, W.; Qi, Y. An enhanced two-step floating catchment area (E2SFCA) method for measuring spatial accessibility to primary care physicians. Health Place 2009, 15, 1100–1107. [Google Scholar] [CrossRef] [PubMed]
- McGrail, M.R. Spatial accessibility of primary health care utilising the two step floating catchment area method: An assessment of recent improvements. Int. J. Health Geogr. 2012, 11, 50. [Google Scholar] [CrossRef] [Green Version]
- Tao, Z.; Cheng, Y. Modelling the spatial accessibility of the elderly to healthcare services in Beijing, China. Environ. Plan. B Urban Anal. City Sci. 2019, 46, 1132–1147. [Google Scholar] [CrossRef]
- Jamtsho, S.; Corner, R.; Dewan, A. Spatio-temporal analysis of spatial accessibility to primary health care in Bhutan. ISPRS Int. J. Geo Inf. 2015, 4, 1584–1604. [Google Scholar] [CrossRef] [Green Version]
- Kakwani, N.C. Measurement of tax progressivity: An international comparison. Econ. J. 1977, 87, 71–80. [Google Scholar] [CrossRef]
- O’Donnell, O.; O’Neill, S.; Van Ourti, T.; Walsh, B. Conindex: Estimation of concentration indices. Stata J. 2016, 16, 112–138. [Google Scholar] [CrossRef] [Green Version]
- Van Doorslaer, E.; Wagstaff, A.; Bleichrodt, H.; Calonge, S.; Gerdtham, U.-G.; Gerfin, M.; Geurts, J.; Gross, L.; Häkkinen, U.; Leu, R.E. Income-related inequalities in health: Some international comparisons. J. Health Econ. 1997, 16, 93–112. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.-J.; Lee, H.-O.; Kim, H.-E. Analysis of the Inequalities in Healthcare Service Usage Considering Healthcare Service Needs. J. Korea Contents Assoc. 2017, 17, 435–445. [Google Scholar]
- Kim, D.-H.; Park, J.-A. Spatial Equity of Neighborhood Store Accessibility: Focused on the Census on Establishments (2006–2014) in Seoul, Korea. J. Korea Plan. Assoc. 2017, 52, 43–56. [Google Scholar] [CrossRef]
- Levinson, D.M.; Marshall, W.; Axhausen, K. Elements of Access: Transport Planning for Engineers, Transport Engineering for Planners; Network Design Lab: Sydney, Australia, 2017. [Google Scholar]
- Linchuan, Y.; Xu, C. Determinants of Elderly Mobility in Hong Kong: Implications for Elderly-Friendly Transport. China City Plan. Rev. 2020, 29, 74–83. [Google Scholar]
- Guida, C.; Carpentieri, G. Quality of life in the urban environment and primary health services for the elderly during the Covid-19 pandemic: An application to the city of Milan (Italy). Cities 2021, 110, 103038. [Google Scholar] [CrossRef]
- Yun, J.; Woo, M. Empirical Study on Spatial Justice through the Analysis of Transportation Accessibility of Seoul. J. Korea Plan. Assoc. 2015, 50, 69–85. [Google Scholar] [CrossRef]
- Ha, J.; Lee, S. An Analysis of Vulnerable Areas for Public Transit Services using API Route Guide Information—Focused on the Mobility to Major Employment Centers in Seoul, Korea. J. Korea Plan. Assoc. 2016, 51, 163–181. [Google Scholar] [CrossRef]
- Cho, D.-H. The Spatial Distribution of the Single-households Elderly and Public Transport Accessibility in Seoul. J. Korean Urban Geogr. Soc. 2014, 17, 119–136. [Google Scholar]
- Kim, K.; Kwon, K. The Impacts of Urban Built Environments on Travel Behavior of the Elderly: The Case of Seoul Metropolitan Area. J. Korean Urban Geogr. Soc. 2020, 23, 109–124. [Google Scholar] [CrossRef]
- Lee, S.K.; Cho, E.; Kim, M.J.; Kim, J.E.; Kim, S.E.; Hyun, S.J. The Characteristics of the Location of Medical Specialists’ Office in Korea. Korean J. Fam. Med. 2009, 30, 292–300. [Google Scholar] [CrossRef]
- Cho, H.-J. Equity in health care: Current situation in South Korea. J. Korean Med. Assoc. 2013, 56, 184–194. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Meyer, P.; Jin, L. Spatial access to health care and elderly ambulatory care sensitive hospitalizations. Public Health 2019, 169, 76–83. [Google Scholar] [CrossRef]
- Laditka, J.N. Physician supply, physician diversity, and outcomes of primary health care for older persons in the United States. Health Place 2004, 10, 231–244. [Google Scholar] [CrossRef]
- Chen, T.; Pan, J. The effect of spatial access to primary care on potentially avoidable hospitalizations of the elderly: Evidence from Chishui City, China. Soc. Indic. Res. 2020, 160, 645–665. [Google Scholar] [CrossRef]
- Sung, H.; Park, J.H.; Kim, D.J. Impact Analysis of Transit-Oriented Development and Revising Current Transportation and Urban Planning Laws for Its Application in Korea; The Korea Transport Institute: Sejong, Korea, 2007; ISBN 9788955032550.
- Su, S.; Pi, J.; Xie, H.; Cai, Z.; Weng, M. Community deprivation, walkability, and public health: Highlighting the social inequalities in land use planning for health promotion. Land Use Policy 2017, 67, 315–326. [Google Scholar] [CrossRef]
- Su, S.; Zhang, Q.; Pi, J.; Wan, C.; Weng, M. Public health in linkage to land use: Theoretical framework, empirical evidence, and critical implications for reconnecting health promotion to land use policy. Land Use Policy 2016, 57, 605–618. [Google Scholar] [CrossRef]
Figure 1.
Public transit network in Seoul.

Figure 2.
Study area.

Figure 3.
ACOA Scale (Example of Nonhyeon 2-dong).

Figure 4.
Distance decay in the FCA Model.

Figure 5.
Distribution of elderly people (More than 65 years) and primary care.

Figure 6.
Primary care accessibility of elderly individuals.

Figure 7.
Concentration curve of primary care accessibility of older people.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Summary statistics.
| Category | Number of Doctors | Aggregated Census Output Area (ACOA) | ||||
|---|---|---|---|---|---|---|
| Number of People over 65 | Annual Income(Million Won) | Number of Primary Care Facilities Accessible within 30 min | Transit Distance | |||
| 15 Min or Less | Less Than 30 Min | |||||
| N | 4624 | 1415 | 1381 | 1415 | 82,334 | 751,304 |
| Mean | 1.87 | 880.99 | 33.43 | 535.33 | 1551.14 | 4281.86 |
| Max | 46 | 3722 | 105.30 | 957 | 3860 | 11826 |
| Minimum | 1 | 5 | 24.04 | 1 | 167 | 167 |
| S.D. | 2.53 | 660.02 | 7.90 | 182.85 | 621.69 | 1715.68 |
| Data | License data | Census Output Area data | KCB Annual income estimate | Korea Open Data Portal Public transit route inquiry service | ||
| D.B date | 2017.12.31. | 2017 | 2017 | 2019.07. | ||
Table 2.
Correlation analysis results.
| Primary Care Accessibility of Older People | Regional Public Transport Mobility | Neighborhood Public Transport Mobility | |
|---|---|---|---|
| Primary care accessibility of older adults | 1 | ||
| Regional public transport mobility | 0.098 ** | 1 | |
| Neighborhood public transport mobility | 0.205 ** | 0.432 ** | 1 |
**: p < 0.01.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Yoon, Y.; Park, J. Equitable City in an Aging Society: Public Transportation-Based Primary Care Accessibility in Seoul, Korea. Sustainability 2022, 14, 9902. https://0-doi-org.brum.beds.ac.uk/10.3390/su14169902
AMA Style
Yoon Y, Park J. Equitable City in an Aging Society: Public Transportation-Based Primary Care Accessibility in Seoul, Korea. Sustainability. 2022; 14(16):9902. https://0-doi-org.brum.beds.ac.uk/10.3390/su14169902
Chicago/Turabian StyleYoon, Yoonchae, and Jina Park. 2022. "Equitable City in an Aging Society: Public Transportation-Based Primary Care Accessibility in Seoul, Korea" Sustainability 14, no. 16: 9902. https://0-doi-org.brum.beds.ac.uk/10.3390/su14169902
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.