
HealthGuard: An Intelligent Healthcare System Security Framework Based on Machine Learning


 , , and
, , and
Abstract
:1. Introduction
- In this work, we present HealthGuard, a data security solution that is built on machine learning and is intended for the detection of SHS vulnerabilities. HealthGuard was developed by the authors of this paper. HealthGuard is able to identify dangerous behaviours in a SHS by capturing the association between a patient’s different physiological processes and monitoring the vital signals of a variety of smart medical devices. This is important for the identification of harmful acts.
- When HealthGuard was being trained, a total of nine databases and twelve innocuous activities were used. These actions comprised seven behaviours that are characteristic of users and five behaviours that are associated with diseases.
- We put HealthGuard through its paces by subjecting it to three different hazards.
- Our in-depth analysis demonstrates that HealthGuard has a high level of accuracy as well as a score of F1 when it comes to identifying a variety of dangers to the intelligent healthcare system.
2. Related Work
2.1. Vulnerabilities in Security
2.2. Relatared Existing Remedies
2.3. Distinguish between Already-Existing Remedies
3. Background
3.1. Intelligent, Connected Health Care System
3.2. Involvement of Multiple Body Systems
3.3. A Study of Anomalous Behavior
4. Problem Scope
4.1. Scope of the Problem
4.2. Model Threat
- First, there is the possibility of harmful behaviour, in which an attacker is present and injects falsified data to carry out malevolent behaviours that alter the patient’s physical state. The danger here is that bogus information will be injected into a medical gadget [20].
- Second, harmful behaviour may be introduced into any medical equipment by the installation of a rogue programme that prevents the device from entering sleep mode. This danger is an example of an assault using a compromised equipment [21].
- Third, there is the possibility for malicious acts. Any medical device in the vicinity may be rendered temporarily inoperable if an attacker was able to tamper with it. A Denial of Service (DoS) assault [22] is being proposed.
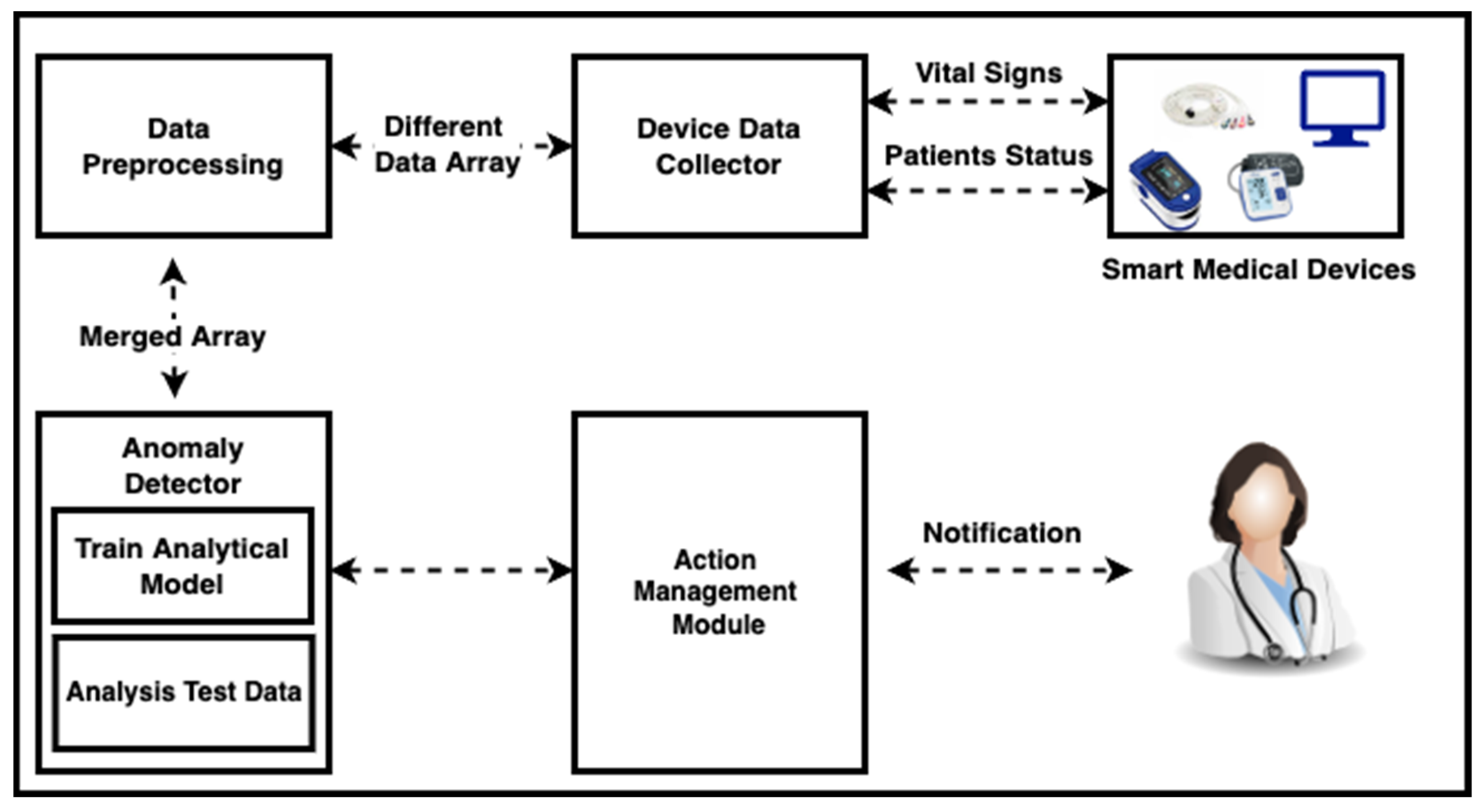
5. Overview of System
5.1. Module Is Being Used to Collect Data
5.2. Preprocessing of Data
5.3. Module for Anomaly Detector
5.4. Module for Managing Actions
6. Evaluation of Performance
- The first research question is: How effective is HealthGuard at an occurrence between a diseased user and a healthy user user? (Section 6.3)
- The second research question is: How effective is HealthGuard at spotting several harmful assaults on SHSs? (Section 6.4)
- The third research question is: How does the sheer abundance of gadgets in the typical SHS affect the effectiveness of HealthGuard? (Section 6.5)
- The fourth research question is: How does the frequency of assaults affect security within the SHS on the HealthGuard’s efficiency? (Section 6.6)
6.1. Methodology and Training Environment Approach
6.2. Metric Performance
6.3. Evaluation with Only Activities Affected by the Disease and Normal Ones
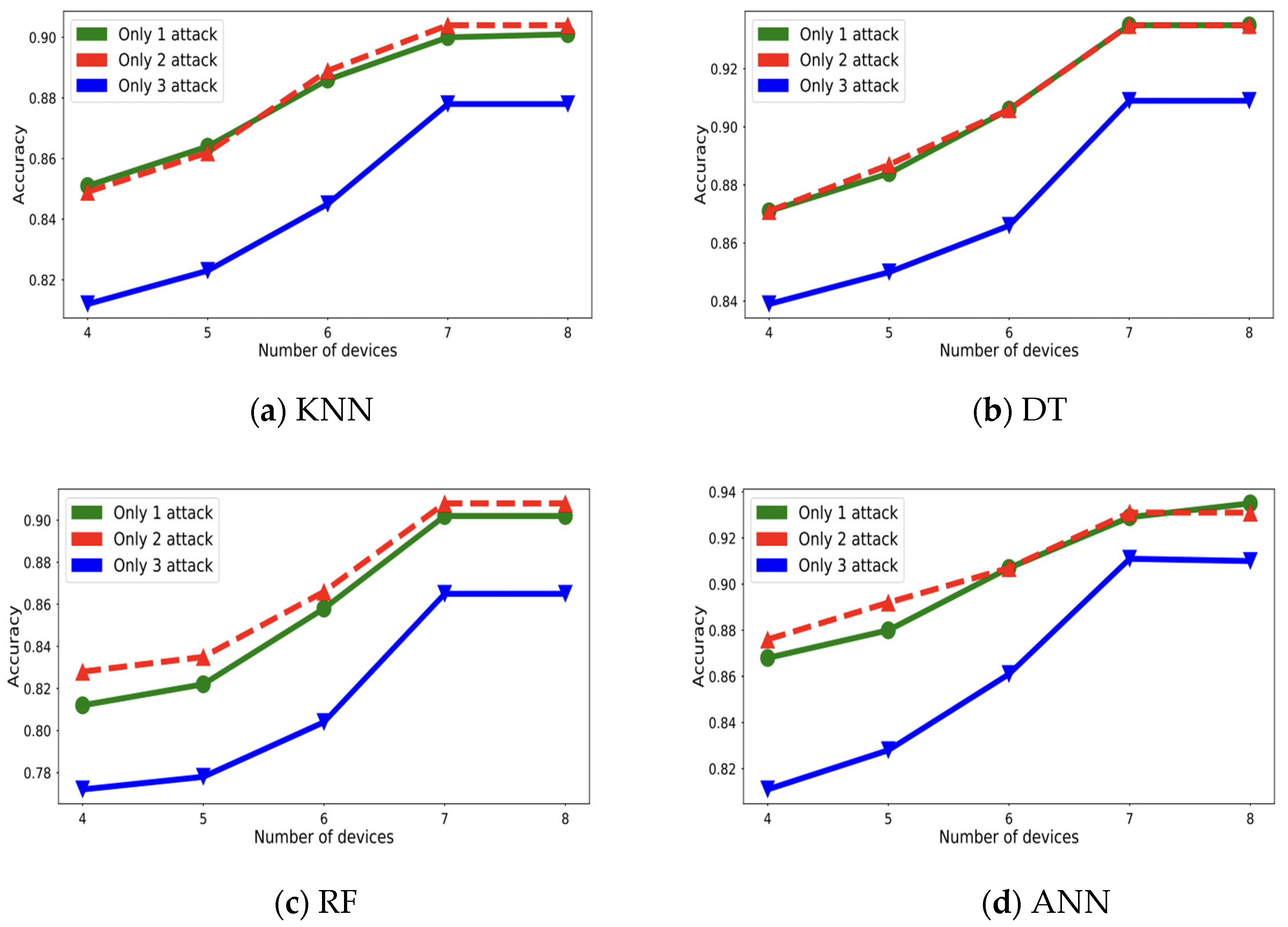
6.4. Testing under a Number of Attack Conditions
6.5. Testing with a Range of Device Counts
6.6. Testing under Simultaneous Threat Environments
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jilek, C.; Tzeis, S.; Reents, T.; Estner, H.L.; Fichtner, S.; Ammar, S.; Kolb, C. Safety of implantable pacemakers and cardioverter defibrillators in the magnetic field of a novel remote magnetic navigation system. J. Cardiovasc. Electrophysiol. 2010, 21, 1136–1141. [Google Scholar] [CrossRef] [PubMed]
- Coventry, L.; Branley, D. Cybersecurity in healthcare: A narrative review of trends, threats and ways forward. Maturitas 2018, 113, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Aurangzeb, S.; Aleem, M.; Iqbal, M.A.; Islam, M.A. Ransomware: A survey and trends. J. Inf. Assur. Secur. 2017, 6, 48–58. [Google Scholar]
- Bhogal, A.S.; Mani, A.R. Pattern analysis of oxygen saturation variability in healthy individuals: Entropy of pulse oximetry signals carries information about mean oxygen saturation. Front. Physiol. 2017, 8, 555. [Google Scholar] [CrossRef]
- Pirbhulal, S.; Pombo, N.; Felizardo, V.; Garcia, N.; Sodhro, A.H.; Mukhopadhyay, S.C. Towards Machine Learning Enabled Security Framework for IoT-Based Healthcare. In Proceedings of the 2019 13th International Conference on Sensing Technology (ICST), Sydney, Australia, 2–4 December 2019; pp. 1–6. [Google Scholar]
- Newaz, A.I.; Haque, N.I.; Sikder, A.K.; Rahman, M.A.; Uluagac, A.S. Adversarial Attacks to Machine Learning-Based Smart Healthcare Systems. In Proceedings of the GLOBECOM 2020–2020 IEEE Global Communications Conference, Taipei, Taiwan, 7–11 December 2020; pp. 1–6. [Google Scholar]
- Muhammad, K.; Khan, S.; Del Ser, J.; De Albuquerque, V.H.C. Deep Learning For Multigrade Brain Tumor Classification in Smart Healthcare Systems: A Prospective Survey. IEEE Trans. Neural Netw. Learn. Syst. 2020, 32, 507–522. [Google Scholar] [CrossRef] [PubMed]
- Ghazal, T.M.; Hasan, M.K.; Alshurideh, M.T.; Alzoubi, H.M.; Ahmad, M.; Akbar, S.S.; Akour, I.A. IoT for smart cities: Machine learning approaches in smart healthcare—A review. Future Internet 2021, 13, 218. [Google Scholar] [CrossRef]
- Ullah, Z.; Al-Turjman, F.; Mostarda, L.; Gagliardi, R. Applications of artificial intelligence and machine learning in smart cities. Comput. Commun. 2020, 154, 313–323. [Google Scholar] [CrossRef]
- Kaur, P.; Sharma, M.; Mittal, M. Big data and machine learning based secure healthcare framework. Procedia Comput. Sci. 2018, 132, 1049–1059. [Google Scholar] [CrossRef]
- Khalid, U.; Asim, M.; Baker, T.; Hung, P.C.K.; Tariq, M.A.; Rafferty, L. A Decentralized Lightweight Blockchain-Based Authen- tication Mechanism for IoT Systems. Clust. Comput. 2020, 23, 2067–2087. [Google Scholar] [CrossRef]
- Jamil, F.; Kahng, H.K.; Kim, S.; Kim, D.H. Towards secure fitness framework based on IoT-enabled blockchain network integrated with machine learning algorithms. Sensors 2021, 21, 1640. [Google Scholar] [CrossRef]
- Kaur, K.; Sharma, S.; Kahlon, K.S. Interoperability and Portability Approaches in Inter-Connected Clouds. ACM Comput. Surv. 2018, 50, 1–40. [Google Scholar] [CrossRef]
- Farhin, F.; Kaiser, M.S.; Mahmud, M. Secured Smart Healthcare System: Blockchain and Bayesian Inference Based Approach. In Proceedings of the International Conference on Trends in Computational and Cognitive Engineering; Springer: Singapore, 2021; pp. 455–465. [Google Scholar]
- Kaur, K.; Sharma, S.; Kahlon, K.S. A Middleware for Polyglot Persistence and Data Portability of Big Data PaaS Cloud Applications. Comput. Mater. Amp Contin. 2020, 65, 1625–1647. [Google Scholar] [CrossRef]
- Rajendran, S.; Mathivanan, S.K.; Jayagopal, P.; Janaki, K.P.; Bernard, B.A.M.M.; Pandy, S.; Somanathan, M.S. Emphasizing privacy and security of edge intelligence with machine learning for healthcare. Int. J. Intell. Comput. Cybern. 2021, 15, 92–109. [Google Scholar] [CrossRef]
- Yaacoub, J.P.A.; Noura, M.; Noura, H.N.; Salman, O.; Yaacoub, E.; Couturier, R.; Chehab, A. Securing internet of medical things systems: Limitations, issues and recommendations. Future Gener. Comput. Syst. 2020, 105, 581–606. [Google Scholar] [CrossRef]
- Vijay, J.A.; Kumar, C.D.P.; Gomathi, B. Secure and Privacy-Aware Intelligent Healthcare Systems: A Review. In Intelligent Healthcare; Springer Nature: Singapore, 2022; pp. 215–239. [Google Scholar] [CrossRef]
- Sujith, A.V.L.N.; Sajja, G.S.; Mahalakshmi, V.; Nuhmani, S.; Prasanalakshmi, B. Systematic review of smart health monitoring using deep learning and Artificial intelligence. Neurosci. Inf. 2022, 2, 100028. [Google Scholar] [CrossRef]
- Kanwal, S.; Tao, F.; Almogren, A.; Ur Rehman, A.; Taj, R.; Radwan, A. A Robust data hiding reversible technique for improving the security in e-health care system. Comput. Model. Eng. Sci. 2022, 132, 1309–1324. [Google Scholar] [CrossRef]
- Ahmad, I.; Ullah, I.; Khan, W.U.; Ur Rehman, A.; Mohmmed, S. Adress, Muhammad Qaiser Saleem, Omar Cheikhrouhou, Habib Hamam, and Muhammad Shafiq Efficient Algorithms for E-healthcare to Solve Multiobject Fuse Detection Problem. J. Healthc. Eng. 2021, 2021, 9500304. [Google Scholar] [CrossRef]
- Gupta, D.S.; Islam, S.H.; Obaidat, M.S.; Karati, A.; Sadoun, B. LAAC: Lightweight Lattice-Based Authentication and Access Control Protocol for E-Health Systems in IoT Environments. IEEE Syst. J. 2020, 15, 3620–3627. [Google Scholar] [CrossRef]
- Witten, I.H.; Frank, E. Data mining: Practical machine learning tools and techniques with Java implementations. ACM Sigmod Rec. 2002, 31, 76–77. [Google Scholar] [CrossRef]
- Prinzie, A.; Van den Poel, D. Random forests for multiclass classification: Random multinomial logit. Expert Syst. Appl. 2008, 34, 1721–1732. [Google Scholar] [CrossRef]
- Güney, S.; Atasoy, A. Multiclass classification of n-butanol concentrations with k-nearest neighbor algorithm and support vector machine in an electronic nose. Sens. Actuators B Chem. 2012, 166, 721–725. [Google Scholar] [CrossRef]
- Sarnak, M.J.; Levey, A.S.; Schoolwerth, A.C.; Coresh, J.; Culleton, B.; Hamm, L.L.; Wilson, P.W. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 2003, 108, 2154–2169. [Google Scholar] [CrossRef] [PubMed]
- Ray, P.P.; Dash, D.; Salah, K.; Kumar, N. Blockchain for IoT-Based Healthcare: Background, Consensus, Platforms, and Use Cases. IEEE Syst. J. 2021, 15, 85–94. [Google Scholar] [CrossRef]
- Delorme, A.; Makeig, S.; Fabre-Thorpe, M.; Sejnowski, T. From single-trial EEG to brain area dynamics. Neurocomputing 2002, 44, 1057–1064. [Google Scholar] [CrossRef]
- Pimentel, M.A.; Johnson, A.E.; Charlton, P.H.; Birrenkott, D.; Watkinson, P.J.; Tarassenko, L.; Clifton, D.A. Toward a robust estimation of respiratory rate from pulse oximeters. IEEE Trans. Biomed. Eng. 2016, 64, 1914–1923. [Google Scholar] [CrossRef]
- Raza, A.; Ayub, H.; Khan, J.A.; Ahmad, I.; Salama, A.S.; Daradkeh, Y.I.; Javeed, D.; Ur Rehman, A.; Hamam, H. A Hybrid Deep Learning-Based Approach for Brain Tumor Classification. Electronics 2022, 11, 1146. [Google Scholar] [CrossRef]
- Shah, A.D.; Nicholas, O.; Timmis, A.D.; Feder, G.; Abrams, K.R.; Chen, R.; Hemingway, H. Threshold haemoglobin levels and the prognosis of stable coronary disease: Two new cohorts and a systematic review and meta-analysis. PLoS Med. 2011, 8, e1000439. [Google Scholar] [CrossRef]
- Fell, J.C.; Voas, R.B. The effectiveness of a 0.05 blood alcohol concentration (bac) limit for driving in the United States. Addiction 2014, 109, 869–874. [Google Scholar] [CrossRef]
- Sikder, A.K.; Aksu, H.; Uluagac, A.S. 6thSense: A Context-aware Sensor-Based Attack Detector for Smart Devices. In 26th USENIX Security Symposium (USENIX Security 17); USENIX Security: Berkeley, CA, USA, 2017; pp. 397–414. [Google Scholar]
- Sikder, A.K.; Aksu, H.; Uluagac, A.S. Context-aware intrusion detection method for smart devices with sensors. U.S. Patent No. 10,417,413, 11 April 2019. [Google Scholar]
- Linda, O.; Vollmer, T.; Manic, M. Neural Network Based Intrusion Detection System for Critical Infrastructures. In Proceedings of the 2009 International Joint Conference on Neural Networks, Atlanta, GA, USA, 14–19 June 2009; pp. 1827–1834. [Google Scholar]
- Tepel, M.; Van Der Giet, M.; Statz, M.; Jankowski, J.; Zidek, W. The antioxidant acetylcysteine reduces cardiovascular events in patients with end-stage renal failure: A randomized, controlled trial. Circulation 2003, 107, 992–995. [Google Scholar] [CrossRef]
- Lee, C.H.; Yoon, H.-J. Medical Big Data: Promise and Challenges. Kidney Res. Clin. Pract. 2017, 36, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Tufail, A.B.; Ma, Y.-K.; Kaabar, M.K.A.; Rehman, A.U.; Khan, R.; Cheikhrouhou, O. Classification of Initial Stages of Alzheimer’s Disease through Pet Neuroimaging Modality and Deep Learning: Quantifying the Impact of Image Filtering Approaches. Mathematics 2021, 9, 3101. [Google Scholar] [CrossRef]
- Heckmann, M.; Ceballos-Baumann, A.O.; Plewig, G. Botulinum toxin A for axillary hyperhidrosis (excessive sweating). N. Engl. J. Med. 2001, 344, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Mackay, J.; Mensah, G.A.; Greenlund, K. The Atlas of Heart Disease and Stroke; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Chen, Z.; Venkat, P.; Seyfried, D.; Chopp, M.; Yan, T.; Chen, J. Brain–heart interaction: Cardiac complications after stroke. Circ. Res. 2017, 121, 451–468. [Google Scholar] [CrossRef] [PubMed]
- Dhindsa, S.; Tripathy, D.; Mohanty, P.; Ghanim, H.; Syed, T.; Aljada, A.; Dandona, P. Differential effects of glucose and alcohol on reactive oxygen species generation and intranuclear nuclear factor-κB in mononuclear cells. Metabolism 2004, 53, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Crabbe, J.B.; Dishman, R.K. Brain electrocortical activity during and after exercise: A quantitative synthesis. Psychophysiology 2004, 41, 563–574. [Google Scholar] [CrossRef]
- Block, A.J.; Boysen, P.G.; Wynne, J.W.; Hunt, L.A. Sleep apnea, hypopnea and oxygen desaturation in normal subjects: A strong male predominance. N. Engl. J. Med. 1979, 300, 513–517. [Google Scholar] [CrossRef]
- Shepard, J.W., Jr.; Garrison, M.W.; Grither, D.A.; Dolan, G.F. Relationship of ventricular ectopy to oxyhemoglobin desaturation in patients with obstructive sleep apnea. Chest 1985, 88, 335–340. [Google Scholar] [CrossRef]
- Robinson, R.W.; Zwillich, C.W.; Bixler, E.O.; Cadieux, R.J.; Kales, A.; White, D.P. Effects of oral narcotics on sleep-disordered breathing in healthy adults. Chest 1987, 91, 197–203. [Google Scholar] [CrossRef]
- Bordia, A.; Verma, S.K.; Srivastava, K.C. Effect of garlic (Allium sativum) on blood lipids, blood sugar, fibrinogen and fibrinolytic activity in patients with coronary artery disease. Prostaglandins Leukotrienes Essential Fat. Acids 1998, 58, 257–263. [Google Scholar] [CrossRef]
- Bakker, J.; Coffernils, M.; Leon, M.; Gris, P.; Vincent, J.L. Blood lactate levels are superior to oxygen-derived variables in predicting outcome in human septic shock. Chest 1991, 99, 956–962. [Google Scholar] [CrossRef]
- Bharany, S.; Sharma, S.; Badotra, S.; Khalaf, O.I.; Alotaibi, Y.; Alghamdi, S.; Alassery, F. Energy-Efficient Clustering Scheme for Flying Ad-Hoc Networks Using an Optimized LEACH Protocol. Energies 2021, 14, 6016. [Google Scholar] [CrossRef]
- Ferrag, M.A.; Shu, L. The performance evaluation of blockchain-based security and privacy systems for the Internet of Things: A tutorial. IEEE Internet Things J. 2021, 8, 17236–17260. [Google Scholar] [CrossRef]
- Kaur, K.; Bharany, S.; Badotra, S.; Aggarwal, K.; Nayyar, A.; Sharma, S. Energy-efficient polyglot persistence database live migration among heterogeneous clouds. J. Supercomput. 2022, 1–30. [Google Scholar] [CrossRef]
- Uddin, M.A.; Stranieri, A.; Gondal, I.; Balasubramanian, V. Continuous patient monitoring with a patient centric agent: A block architecture. IEEE Access 2018, 6, 32700–32726. [Google Scholar] [CrossRef]
- Jagadeeswari, V.; Subramaniyaswamy, V.; Logesh, R.; Vijayakumar, V. A Study on Medical Internet of Things and Big Data in Personalized Healthcare System. Health Inf. Sci. Syst. 2018, 6, 14. [Google Scholar] [CrossRef]
- Ferrag, M.A.; Shu, L.; Friha, O.; Yang, X. Cyber Security Intrusion Detection for Agriculture 4.0: Machine Learning-Based Solutions, Datasets, and Future Directions. IEEE/CAA J. Autom. Sin. 2021, 9, 407–436. [Google Scholar] [CrossRef]
- Smys, S.; Basar, A.; Wang, H. Hybrid intrusion detection system for internet of things (IoT). J. ISMAC 2020, 2, 190–199. [Google Scholar] [CrossRef]
- Ahmad, S.; Imran; Iqbal, N.; Jamil, F.; Kim, D. Optimal Policy-Making for Municipal Waste Management Based on Predictive Model Optimization. IEEE Access 2020, 8, 218458–218469. [Google Scholar] [CrossRef]
- Zhang, P.; Schmidt, D.C.; White, J.; Lenz, G. Block chain technology offers potential in healthcare. Pharmac. Econ. Outcomes News 2018, 809, 1–41. [Google Scholar]
- Niknam, S.; Dhillon, H.S.; Reed, J.H. Federated learning for wireless communications: Motivation, opportunities and challenges. arXiv 2019, arXiv:1908.06847. [Google Scholar] [CrossRef]
- Bharany, S.; Kaur, K.; Badotra, S.; Rani, S.; Kavita; Wozniak, M.; Shafi, J.; Ijaz, M.F. Efficient Middleware for the Portability of PaaS Services Consuming Applications among Heterogeneous Clouds. Sensors 2022, 22, 5013. [Google Scholar] [CrossRef] [PubMed]
- Musonda, C.; Monica, M.K.; Nyirenda, M.; Phiri, J. Security, Privacy and Integrity in Internet of Things—A Review. In Proceedings of the ICTSZ International Conference in ICTs, Lusaka, Zambia, 18 July 2019; pp. 148–152. [Google Scholar]
- Shuaib, M.; Badotra, S.; Khalid, M.I.; Algarni, A.D.; Ullah, S.S.; Bourouis, S.; Iqbal, J.; Bharany, S.; Gundaboina, L. A Novel Optimization for GPU Mining Using Overclocking and Undervolting. Sustainability 2022, 14, 8708. [Google Scholar] [CrossRef]
- Radanovi’c, I.; Liki´c, R. Opportunities for use of block chain technology in medicine. Appl. Health Econ. Health Policy 2018, 16, 583–590. [Google Scholar] [CrossRef]
- Iqbal, N.; Ahmad, S.; Kim, D.H. Towards Mountain Fire Safety Using Fire Spread Predictive Analytics and Mountain Fire Containment in IoT Environment. Sustainability 2021, 13, 2461. [Google Scholar] [CrossRef]
- Li, Q.; Zhang, K.; Cheffena, M.; Shen, X. Channel-Based Sybil Detection in Industrial Wireless Sensor Networks: A Multi-Kernel Approach. In Proceedings of the IEEE Global Communications Conference (GLOBECOM), Singapore, 4–8 December 2017; pp. 1–6. [Google Scholar]
- Firdaus, A.; Anuar, N.B.; Razak, M.F.A.; Hashem, I.A.T.; Bachok, S.; Sangaiah, A.K. Root exploit detection and features optimization: Mobile device and block chain based medical data management. J. Med. Syst. 2018, 42, 112. [Google Scholar] [CrossRef] [PubMed]
- Rathore, S.; Park, J.H. Semi-supervised learning based distributed attack detection framework for IoT. Appl. Soft Comput. 2018, 72, 79–89. [Google Scholar] [CrossRef]
- Bharany, S.; Sharma, S.; Frnda, J.; Shuaib, M.; Khalid, M.I.; Hussain, S.; Iqbal, J.; Ullah, S.S. Wildfire Monitoring Based on Energy Efficient Clustering Approach for FANETS. Drones 2022, 6, 193. [Google Scholar] [CrossRef]
- Hussain, M.; Mehmood, A.; Khan, S.; Khan, M.A.; Iqbal, Z. Authentication techniques and methodologies used in wireless body area networks. J. Syst. Archit. 2019, 101, 101655. [Google Scholar] [CrossRef]
- Imran, I.; Zaman, U.; Waqar, M.; Zaman, A. Using Machine Learning Algorithms for Housing Price Prediction: The Case of Islamabad Housing Data. Soft Comput. Mach. Intell. 2021, 1, 11–23. [Google Scholar] [CrossRef]
- Brownlee, J. A Gentle Introduction to Generative Adversarial Networks (GANS). Available online: https://machinelearningmastery.com/what-are-generative-adversarial-networks-gans/ (accessed on 12 July 2022).
- Ferdowsi, A.; Saad, W. Generative adversarial networks for distributed intrusion detection in the internet of things. In Proceedings of the 2019 IEEE Global Communications Conference (GLOBECOM), Waikoloa, HI, USA, 9–13 December 2019. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| References | Type of Device Monitoring | Model | Database | Value of Feature Parameter |
|---|---|---|---|---|
| [28] | Blood Pressure and Heart Rate | QardioArm | Data.Gov, Fetal ECG Synthetic Database | (60–100) min per beats, Diastolic (80 mm Hg) and Systolic (120 mm Hg) |
| [29] | Blood Oxygen | iHealth Air Wireless Pulse Oximeter | An Examination of the Patterns of Variation in Oxygen Saturation | SpO2 level ≥ 94% |
| [30] | Blood Glucose | Insulin Pump MiniMed 670G System | diabetes machine learning database at UCI | 70–130 mg/dL |
| [31] | Both Human Movement and Sleep | Smart Watch Versa Fitbit | The Sleep Database of CAP | NREM and REM sleep cycle |
| [32] | Blood Hemoglobin | Germaine AimStrip Hb Hemoglobin Meter | The DHS Hemoglobin Data | 12.3–17.5 g/dL |
| [33] | Neural system Activity | The Emotiv Insight of It | ERP/EEG data | Delta (0.5–4 Hz), Alpha (8–12 Hz), Theta (4–8 Hz), Beta (16–24 Hz) & ERP/EEG data |
| [34] | Blood Alcohol | Eliminate Continuous Monitoring of Alcohol (Cam) | StatCrunch dataset | 0.08 g/dL |
| [35] | Respiratory and Sweating Rate | QardioCore | Dataset of BIDMC PPG and Respiration | 0.5µ/min/cm2, Breaths per minute (12–20) |
| References | HM | NA | AL | HG | SL | OX | BR | GL | BP | ECG | SW | Disease Type |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [36] | No | Yes | No | Yes | No | Yes | No | Yes | Yes | No | Yes | High Cholesterol |
| [37] | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | Yes | No | Abnormal oxygen level |
| [38] | No | Yes | No | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Low or High blood sugar |
| [39] | Yes | Yes | No | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Excessive sweating |
| [40] | No | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes | High blood Pressure |
| References | NA | AL | HG | HM | SW | OX | BR | GL | BP | ECG | SW | Disease Type |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [41] | Yes | No | No | No | Yes | No | Yes | No | Yes | Yes | Yes | Stress |
| [42] | Yes | No | No | No | No | No | Yes | No | No | Yes | No | Heart-Attack |
| [43] | No | No | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Sleeping |
| [44] | Yes | No | Yes | Yes | No | No | No | No | Yes | Yes | Yes | Stroke |
| [45] | Yes | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Exercise |
| [46] | No | Yes | No | No | No | No | Yes | Yes | Yes | No | Yes | Drunk |
| [47] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Walking |
| Malicious | Benign | |||||||
|---|---|---|---|---|---|---|---|---|
| ANN | DT | RF | KNN | ANN | DT | RF | KNN | |
| Recall | 0.91 | 0.91 | 0.86 | 0.88 | 0.93 | 0.93 | 0.90 | 0.90 |
| F1-score | 0.89 | 0.90 | 0.86 | 0.87 | 0.93 | 0.93 | 0.90 | 0.90 |
| Precision | 0.90 | 0.91 | 0.86 | 0.88 | 0.92 | 0.92 | 0.90 | 0.90 |
| Accuracy | 0.910 | 0.909 | 0.865 | 0.878 | 0.927 | 0.931 | 0.898 | 0.903 |
| Device Count | 8 | 7 | 6 | 5 | 4 | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Algo | F1-Score | Recall | Precision | Accuracy | F1-Score | Recall | Precision | Accuracy | F1-Score | Recall | Precision | Accuracy | F1-Score | Recall | Precision | Accuracy | F1-Score | Recall | Precision | Accuracy |
| DT | 0.90 | 0.91 | 0.91 | 0.909 | 0.90 | 0.91 | 0.91 | 0.909 | 0.85 | 0.87 | 0.86 | 0.866 | 0.82 | 0.85 | 0.85 | 0.850 | 0.81 | 0.84 | 0.83 | 0.839 |
| ANN | 0.89 | 0.91 | 0.90 | 0.910 | 0.89 | 0.91 | 0.89 | 0.9111 | 0.82 | 0.86 | 0.82 | 0.861 | 0.79 | 0.83 | 0.82 | 0.828 | 0.77 | 0.81 | 0.78 | 0.811 |
| KNN | 0.87 | 0.88 | 0.88 | 0.878 | 0.87 | 0.88 | 0.88 | 0.878 | 0.83 | 0.84 | 0.84 | 0.845 | 0.79 | 0.82 | 0.81 | 0.823 | 0.78 | 0.81 | 0.82 | 0.812 |
| RF | 0.86 | 0.86 | 0.86 | 0.865 | 0.86 | 0.86 | 0.86 | 0.865 | 0.79 | 0.80 | 0.79 | 0.804 | 0.76 | 0.78 | 0.75 | 0.778 | 0.76 | 0.77 | 0.75 | 0.772 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sundas, A.; Badotra, S.; Bharany, S.; Almogren, A.; Tag-ElDin, E.M.; Rehman, A.U. HealthGuard: An Intelligent Healthcare System Security Framework Based on Machine Learning. Sustainability 2022, 14, 11934. https://0-doi-org.brum.beds.ac.uk/10.3390/su141911934
Sundas A, Badotra S, Bharany S, Almogren A, Tag-ElDin EM, Rehman AU. HealthGuard: An Intelligent Healthcare System Security Framework Based on Machine Learning. Sustainability. 2022; 14(19):11934. https://0-doi-org.brum.beds.ac.uk/10.3390/su141911934
Chicago/Turabian StyleSundas, Amit, Sumit Badotra, Salil Bharany, Ahmad Almogren, Elsayed M. Tag-ElDin, and Ateeq Ur Rehman. 2022. "HealthGuard: An Intelligent Healthcare System Security Framework Based on Machine Learning" Sustainability 14, no. 19: 11934. https://0-doi-org.brum.beds.ac.uk/10.3390/su141911934