1. Introduction
The lymph is a fluid that originates in the interstitial space composed of cells, proteins, chylomicrons, and occasionally bacteria. This fluid enters the lymphatic system, making its way to the lymph nodes which act as filters for the lymph, then entering the cisterna chyli, and later reaching the thoracic duct, following its path until it reaches the major circulation, draining at the level of the left subclavian and left internal jugular vein. A high percentage of the lymph originates in the abdominal organs (particularly the liver and intestine) [
1]. When the structures of this system, more specifically its main ducts, are injured or obstructed, lymph spreads to the adjacent spaces causing a variety of conditions. If the above occurs in the context of a peritoneal effusion, it is referred to as chyloperitoneum or chylous ascites [
2]. The diagnosis of chyloperitoneum is based on the clinical presentation of ascites through the analysis of the fluid, including a milky appearance and triglyceride levels >200 mg/dL of the fluid [
3]. Chyloperitoneum fluid is rich in biologically unavailable nutrients and immunoglobulins after accumulation in the peritoneum, which can lead to dehydration, malnutrition, electrolyte-hydric alteration, and immunosuppression [
4].
The underlying etiologies of chyloperitoneum have been classified as congenital, traumatic, infectious, neoplastic, postoperative, cirrhotic, or cardiogenic [
3]; almost two-thirds of the reported cases in developed countries are of cirrhotic origin or associated with abdominal malignancy, while, in developing countries, infectious diseases such as tuberculosis account for the majority of cases [
5].
Chyloperitoneum is considered an uncommon yet severe complication during abdominal surgery [
6]. It occurs most often during postoperative retroperitoneal lymph node dissection, distal splenic shunt, abdominal aortic aneurysm repair, or liver transplant [
5,
7], while its presentation as a complication of colorectal cancer surgery is exceptional [
8].
The incidence of chyloperitoneum has increased due to prolonged survival after surgical interventions in patients with cancer, as well as patients who have undergone aggressive cardiothoracic and abdominal interventions [
6,
8]. The prognosis and treatment of this disease varies depending on the underlying cause; considering that there is no series of studies where the sociodemographic and clinical data of those affected were thoroughly analyzed, its medium- or long-term impact are uncertain. Bearing the limited knowledge on this subject, especially in developing countries, it is proposed to present the case of a 56-year-old man who presented with chyloperitoneum as the initial manifestation of gastrointestinal lymphoma. Since epidemiologically speaking its presentation is secondary to a neoplasm in the described location, this is a key finding in the quest to understand and document the effects of chyloperitoneum. Informed consent was requested by the medical team for the publication of this case report and was signed by the patient, including images.
2. Case
A 56-year-old Black man, working as an accountant, from an urban area, with a clinical history of approximately three months of evolution. His symptoms consisted of the sensation of an abdominal mass, predominantly in the left hemiabdomen, associated with progressive abdominal distension, changes in bowel habits, lower limb edema, dyspepsia, occasional postprandial emesis, and unintended 20 kg weight loss. The patient presented no comorbidities or surgical history; in addition, arterial hypertension was the only concern in his family history. He was not taking any medication at the time of the evaluation. A total abdomen ultrasonography was performed. The report displayed a non-specific mesenteric mass at the root of the mesentery, abundant ascitic fluid, and a small liver with dilated portal vein. At the time of the assessment by the general surgery service, the patient was in an acceptable general condition with vital signs of: BP, 130/90 mmHg; HR, 92 beats/min; height, 160 cm; weight, 52 kg; and BMI, 20 kg/m2. At the physical examination, globose abdomen was found, with a sensation of an irregular mass predominantly in the left hemiabdomen, positive ascitic wave, general pain, no signs of peritoneal irritation, and Grade III edema of the lower limbs. Within the initial paraclinical studies there was no evidence of alteration in the cell lines, the renal and hepatic function were preserved, and there were no electrolytic alterations.
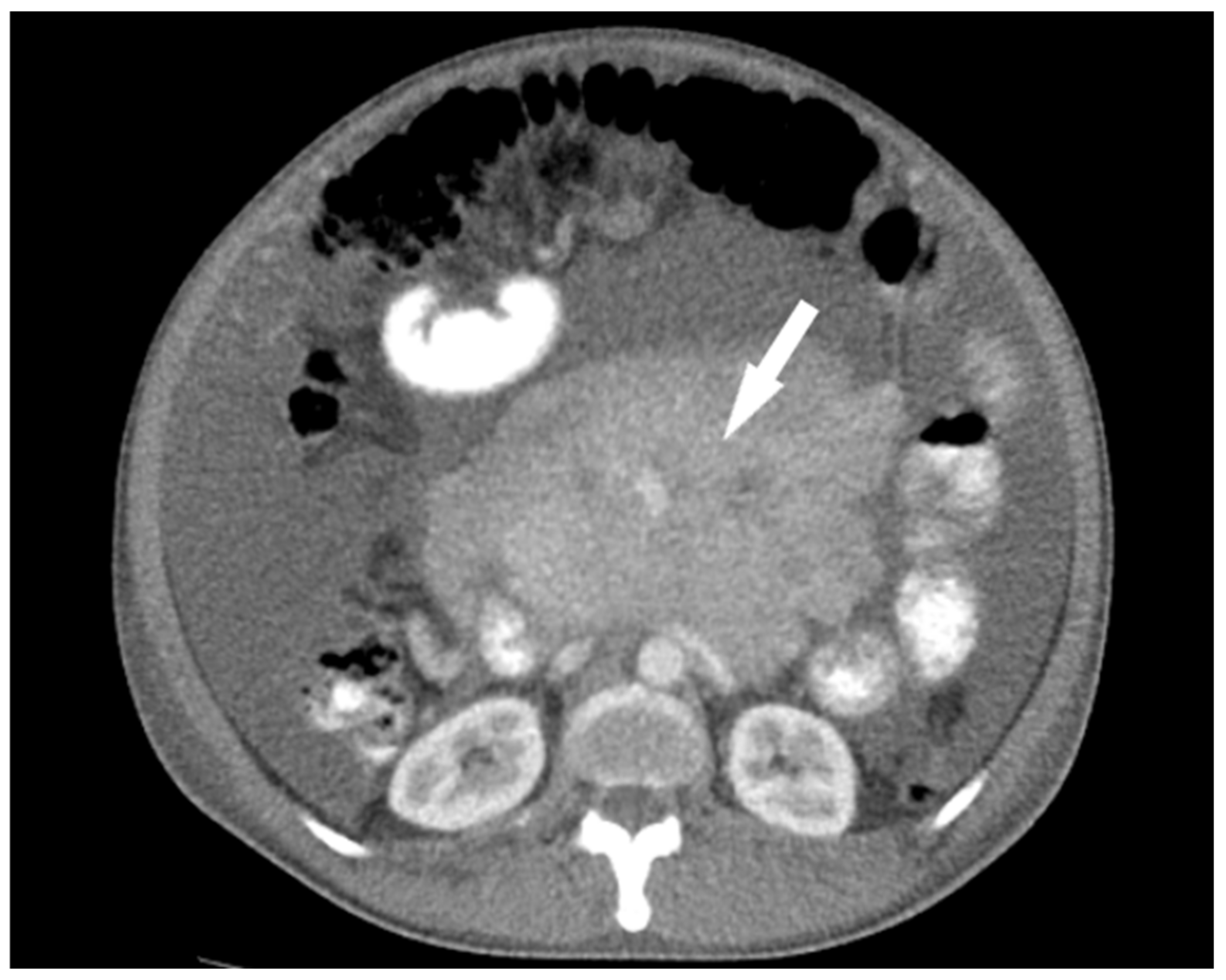
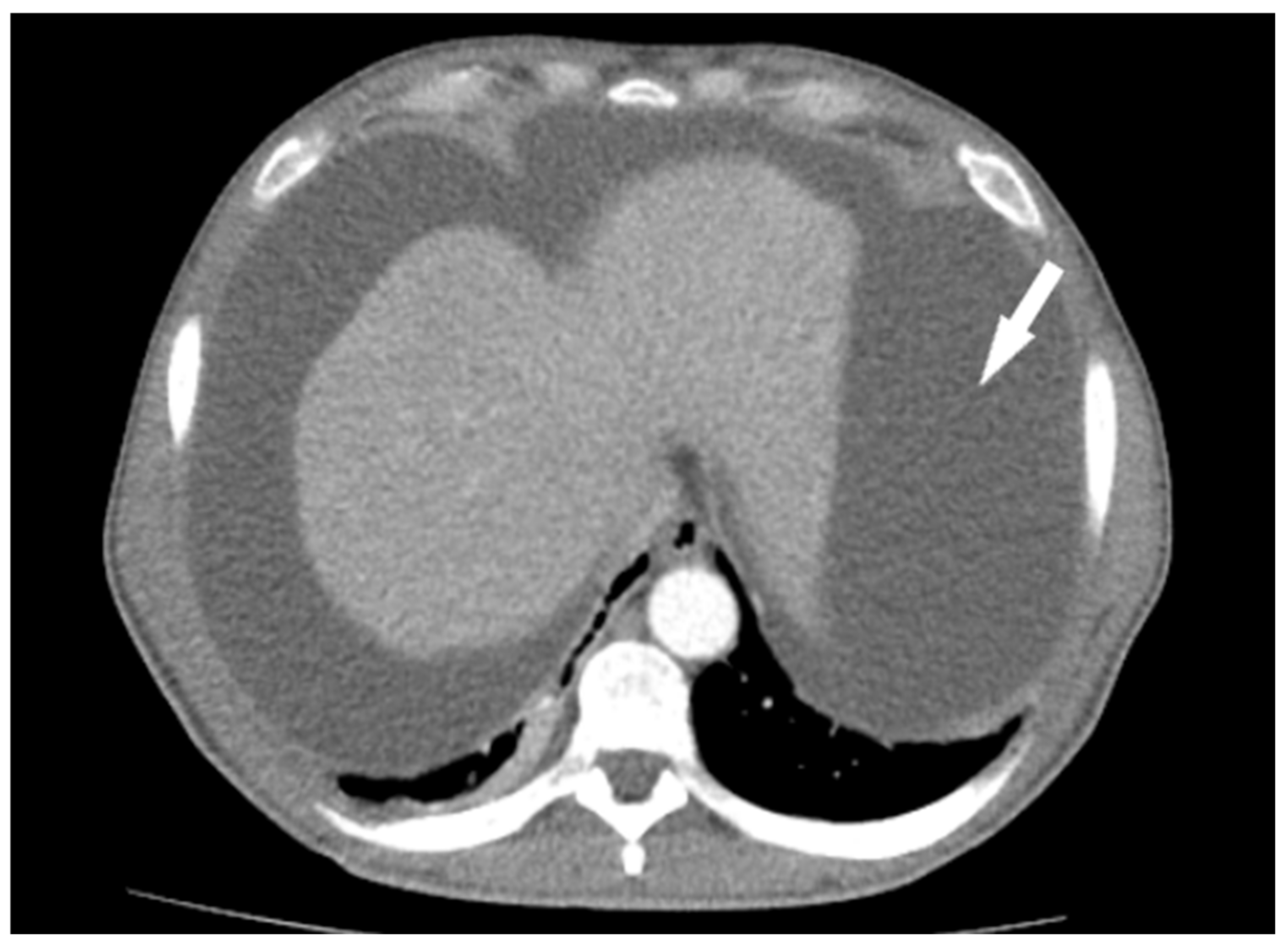
Tumor marker studies were requested (CA 19.9, CEA, and AFP), all of which were negative. Endoscopic studies (esophagogastroduodenoscopy and colonoscopy) were performed with findings of gastropathy, but without evidence of lesions suggestive of neoplasia. A contrast abdominal tomography scan was performed where a retroperitoneal-looking mass was found measuring 154 mm × 119 mm and extending to the mesogastrium, as well signs of ascites (
Figure 1 and
Figure 2). A simple chest tomography revealed right pleural thickening associated with bilateral posterior-basal atelectasis without evidence of adjacent lesions. In addition, a diagnostic laparoscopy was scheduled to collect samples for the histopathological study. The findings during the procedure were: chyloperitoneum of 10,000 ccs (
Figure 3) and a large mass measuring 20 cm × 20 cm involving the meso of the proximal jejunum, with fish meat appearance, and distension of the intestinal loops without evidence of obstruction. The chyloperitoneum was drained and lesion biopsies were taken.
The patient evolved satisfactorily, tolerating diet on his first postoperative day, with adequate control of abdominal pain, improvement in intestinal transit, and marked decrease in ascites, without complications inherent to the surgical procedure. The patient was discharged on the fourth day after surgery. A follow up fifteen days after discharge demonstrated adequate recovery from the surgical intervention; no abdominal pain was reported. In addition, surgical wounds were healing properly, and no signs of ascites were found at the physical examination.
The peritoneal fluid cytological examination showed to contain large groups of lymphoid-like cells on a fibrinoid background, suggesting lymphoid neoplastic infiltration. Furthermore, anatomical pathology results show lymph node infiltration in diffuse form, small lymphocytes with hyperchromatic nuclei, and areas of sclerosis in the node’s medulla. Consecutively, lymphoma was established as a definitive diagnosis.
3. Discussion
Pathophysiologically, chylous ascites can occur through three processes: acquired lymphatic disruption (dilation of retroperitoneal lymph vessels occurs, causing lymph extravasation to the abdomen through a fistula, which may be traumatic or iatrogenic), a congenital cause (such as congenital lymphangiectasia), or secondary to fibrosis of the lymphatic system (seen in malignancies, where there is lymph obstruction from the intestines to the cisterna chyli) [
3,
9]. One of the few systematic reviews of cases existing in the literature on chylous ascites mentions that the most frequent causes of nontraumatic chylous ascites in adults are malignancy (25%), followed by cirrhosis (16%) and mycobacterial infections (15%) [
10].
The most common symptoms described are abdominal distention and mild pain lasting weeks to months, with dyspnea, peritonitis, and weight gain in a few cases, due to increase in intra-abdominal pressure [
10]. However, among all age groups, the lymphatic abnormalities are the most frequent cause (32%), with lymphangiectasia being the most prevalent etiology and observed to a greater extent in the pediatric population (84%) compared to the adult population (8%) [
10]. The second most frequent cause in all groups are the malignant entities, responsible for approximately 17% of cases of nontraumatic chylous ascites, with lymphoma, neuroendocrine tumors, sarcomas, and leukemia being the most frequently encountered causes [
10]. The type of ascites secondary to malignant neoplasms is almost exclusively within the adult population, presenting only in 2% of cases in the infant population [
6,
11]. Taking into consideration that adenocarcinoma is the most frequently presented histologic subtype of cancer in the jejunum (58.7%), followed by carcinoid tumor (16.5%), lymphoma (9.7%), and sarcoma (6.3%) [
11,
12,
13], and that not all cases of lymphoma debut with chylous ascites, it can be said that the percentage of patients that present this complication is very low. Considering its non-specific presentation, it is necessary to begin with a clinical history and detailed physical examination to discard the great possible number of possible differential diagnoses (
Table 1).
Abdominal paracentesis is the most important tool for the evaluation of chylous ascites since it allows identifying the distinctive characteristics of this fluid (milky, thick, and cloudy appearance). It is recommended to obtain a minimum sample of 100 mL [
14]. Likewise, cell count, Gram staining, microbiological culture, evaluation of glucose levels, total proteins, albumin, amylase, lactate dehydrogenase, triglycerides, and cytology should be performed. In the case of suspected mycobacterial infection, resistant acid-alcohol staining and polymerase chain reaction are key [
14]. For the definitive diagnosis of chylous ascites, electrophoresis must be performed for the detection of chylomicrons through lipoproteins; however, accessing this type of specialized studies is complex [
15].
Cytology and peritoneal biopsy are important diagnostic methods if peritoneal carcinomatosis is suspected. It has shown a specificity of around 97% for cancer in the case of a positive cytology [
16]. Similarly, biopsy through laparoscopy has been found to be overly sensitive and specific for the diagnosis of peritoneal cancer and tuberculosis. It should be noted that laparoscopy in these cases serves as both a diagnostic and therapeutic technique and highly useful in clinical pictures where the etiology is difficult to identify [
17,
18].
Tomography has the function of identifying if there is an abdominal mass or affected lymph nodes that explain the picture presented. It also allows evaluating the amount of fluid in the peritoneal cavity, but it does not have the ability to distinguish between common ascitic fluid and chylous ascites because its imaging densities are similar [
17].
There is no consensus on the management of patients with chylous ascites secondary to gastrointestinal neoplasia. The approach depends on the cause and the findings found, so the therapeutic process can range from a simple drainage process to chemotherapy and definitive surgery. A low-sodium diet should be established in order to reduce fluid retention and reduce edema. The use of diuretics is not necessary, since there are no reliable studies that support their use; they have only been effective in 45% of cases [
18,
19,
20]. In addition, it has been found that somatostatin can control the production of chyloperitoneum by decreasing intestinal fat absorption, reducing the concentration of triglycerides in the thoracic duct, and regulating lymph flow in the major lymphatic vessels [
21]. However, there is insufficient evidence to recommend this therapy.
4. Conclusions
Chyloperitoneum is an infrequent finding, being most often found in lymphatic alterations and malignancies of gastrointestinal location. Lymphoma, neuroendocrine tumors, sarcomas, and leukemia are the neoplasms most associated with this complication, occurring almost exclusively in the adult population. Depending on the local or regional epidemiology and patient history, a large number of possible differential diagnoses, ranging from traumatic causes to congenital diseases, can be discarded. The evaluation of the clinical picture should be complemented by physical examination, imaging studies, analysis of the ascitic fluid, and intraoperative biopsy. The treatment then depends on the cause and symptoms, being able to establish a non-invasive approach based on diet, pharmacological therapy, and peritoneal-venous shunts.
Author Contributions
Conceptualization, I.D.L.-M., P.Z.-R., V.H.M.-B. and A.M.R.-G.; methodology, I.D.L.-M., D.T.-L. and M.B.-R.; formal analysis, I.D.L.-M., P.Z.-R., V.H.M.-B. and A.M.R.-G.; investigation, I.D.L.-M., D.T.-L., P.Z.-R., V.H.M.-B., M.B.-R. and A.M.R.-G.; writing—original draft preparation, I.D.L.-M., D.T.-L., P.Z.-R., V.H.M.-B., M.B.-R. and A.M.R.-G.; writing—review and editing, I.D.L.-M., D.T.-L., P.Z.-R., V.H.M.-B., M.B.-R. and A.M.R.-G.; and supervision, I.D.L.-M., P.Z.-R., V.H.M.-B. and A.M.R.-G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by ethics committee of Hospital Universitario San Jorge (14 August 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kim, J.-H.; Han, E.-H.; Jin, Z.-W.; Lee, H.-K.; Fujimiya, M.; Murakami, G.; Cho, B.H. Fetal Topographical Anatomy of the Upper Abdominal Lymphatics: Its Specific Features in Comparison with Other Abdominopelvic Regions. Anat. Rec. Adv. Integr. Anat. Evol. Biol. 2011, 295, 91–104. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Gutierrez, J.C.; Tovar, J.A. Chylothoraz and chylous ascites. Management and pitfalls. Semin. Pediatr. Surg. 2014, 23, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Lizaola, B.; Bonder, A.; Trivedi, H.D.; Tapper, E.B.; Cardenas, A. Review article: The diagnostic approach and current management of chylous ascites. Aliment. Pharmacol. Ther. 2017, 46, 816–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dababneh, Y.; Mousa, O.Y. Chylous Ascites. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Patil, A.; Nandikoor, S.; De Marco, J.; Bhat, R.; Shivakumar, S.; Mallrajapatna, G. Disorders of the lymphatic system of the abdomen. Clin. Radiol. 2016, 71, 941–952. [Google Scholar] [CrossRef] [PubMed]
- Aalami, O.O.; Allen, D.B.; Organ, C.H. Chylous ascites: A collective review. Surgery 2000, 128, 761–778. [Google Scholar] [CrossRef] [PubMed]
- Campisi, C.; Bellini, C.; Eretta, C.; Zilli, A.; Da Rin, E.; Davini, D.; Bonioli, E.; Boccardo, F. Diagnosis and management of primary chylous ascites. J. Vasc. Surg. 2006, 43, 1244–1248. [Google Scholar] [CrossRef] [PubMed]
- Cardenas, A.; Chopra, S. Chylous ascites. Am. J. Gastroenterol. 2002, 97, 1896–1900. [Google Scholar] [CrossRef] [PubMed]
- Al-Busafi, S.A.; Ghali, P.; Deschênes, M.; Wong, P. Chylous Ascites: Evaluation and Management. ISRN Hepatol. 2014, 2014, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinemann, D.C.; Dindo, D.; Clavien, P.-A.; Nocito, A. Atraumatic Chylous Ascites: Systematic Review on Symptoms and Causes. J. Am. Coll. Surg. 2011, 212, 899–905.e4. [Google Scholar] [CrossRef] [PubMed]
- Almakdisi, T.; Massoud, S.; Makdisi, G. Lymphomas and Chylous Ascites: Review of the Literature. Oncologist 2005, 10, 632–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schottenfeld, D.; Beebe-Dimmer, J.L.; Vigneau, F.D. The Epidemiology and Pathogenesis of Neoplasia in the Small Intestine. Ann. Epidemiol. 2009, 19, 58–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhardwaj, R.; Vaziri, H.; Gautam, A.; Ballesteros, E.; Karimeddini, D.; Wu, G.Y. Chylous Ascites: A Review of Pathogenesis, Diagnosis and Treatment. J. Clin. Transl. Hepatol. 2018, 6, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Thaler, M.A.; Bietenbeck, A.; Schulz, C.; Luppa, P.B. Establishment of triglyceride cut-off values to detect chylous ascites and pleural effusions. Clin. Biochem. 2017, 50, 134–138. [Google Scholar] [CrossRef]
- Runyon, B.A.; Hoefs, J.C.; Morgan, T.R. Ascitic fluid analysis in malignancy-related ascites. Hepatology 1988, 8, 1104–1109. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.-M.; Lin, S.-M.; Peng, S.-M.; Wu, C.-S.; Liaw, Y.-F. The role of laparoscopy in the evaluation of ascites of unknown origin. Gastrointest. Endosc. 1994, 40, 285–289. [Google Scholar] [CrossRef]
- Lee, C.W.; Bociek, G.; Faught, W. A Survey of Practice in Management of Malignant Ascites. J. Pain Symptom Manag. 1998, 16, 96–101. [Google Scholar] [CrossRef]
- Saif, M.W.; Siddiqui, I.A.; Sohail, M.A. Management of ascites due to gastrointestinal malignancy. Ann. Saudi Med. 2009, 29, 369–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, M.; Rossi, M. Managing ascities via Tenckhoff catheter. Medsurg. Nurs. 1995, 4, 468–471. [Google Scholar] [PubMed]
- Becker, G.; Galandi, D.; Blum, H.E. Malignant ascites: Systematic review and guideline for treatment. Eur. J. Cancer 2006, 42, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Karaca, S.; Gemayel, G.; Kalangos, A. Somatostatin treatment of a persistent chyloperitoneum following abdominal aortic surgery. J. Vasc. Surg. 2012, 56, 1409–1412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 



{kind=link}
{kind=link}
{kind=link}