
Lightweight Neural Network for COVID-19 Detection from Chest X-ray Images Implemented on an Embedded System †




Abstract
:1. Introduction
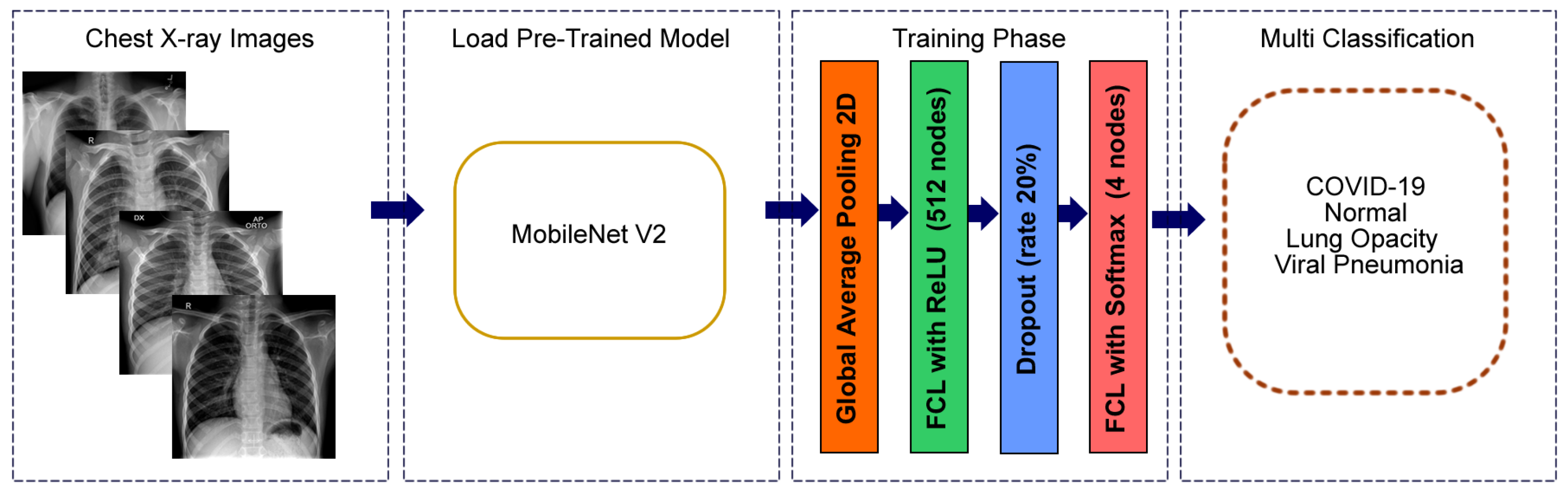
- We propose a modified neural network structure of the MobileNetV2 model, to maximize the learning ability for classification of chest X-rays. The modified version of our architecture requires significant less training time than other existing DL architectures due to the small number of network parameters.
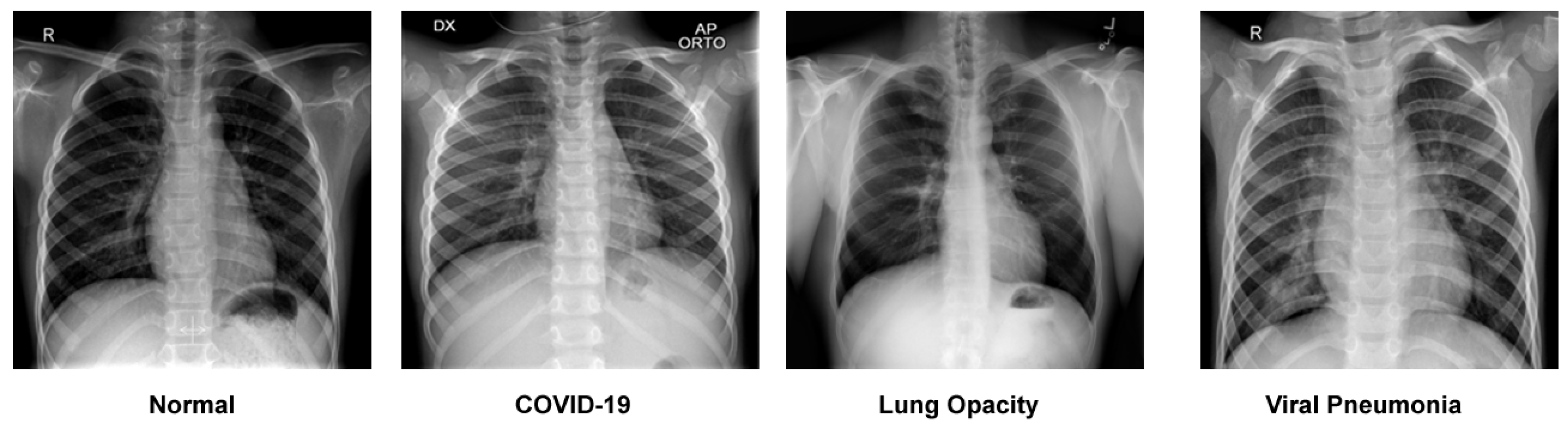
- Our design can classify four different categories of chest X-rays (COVID-19, normal, viral pneumonia and lung opacity). The accuracy of our approach is significantly higher than standard architecture and surpasses other state-of-the-art methods.
- This is the first study to investigate a large set of chest X-ray images (21.165 chest X-ray images) combined from many other studies that appear in the literature, which include few X-ray samples and mainly concern binary classifications.
- The modified structure of the architecture yields excellent classification results and, in combination with the small size of the network, leads to an attractive model for diagnosing chest X-rays in embedded systems.
2. Related Work
3. Materials and Methods
3.1. Dataset Description
3.2. Splitting the Dataset
3.3. Data Pre-Processing
3.4. Proposed Modified Model Architecture
3.5. Training Strategy
3.6. Training the Model on the Embedded GPU
3.7. Model Evaluation Metrics on the Test Dataset
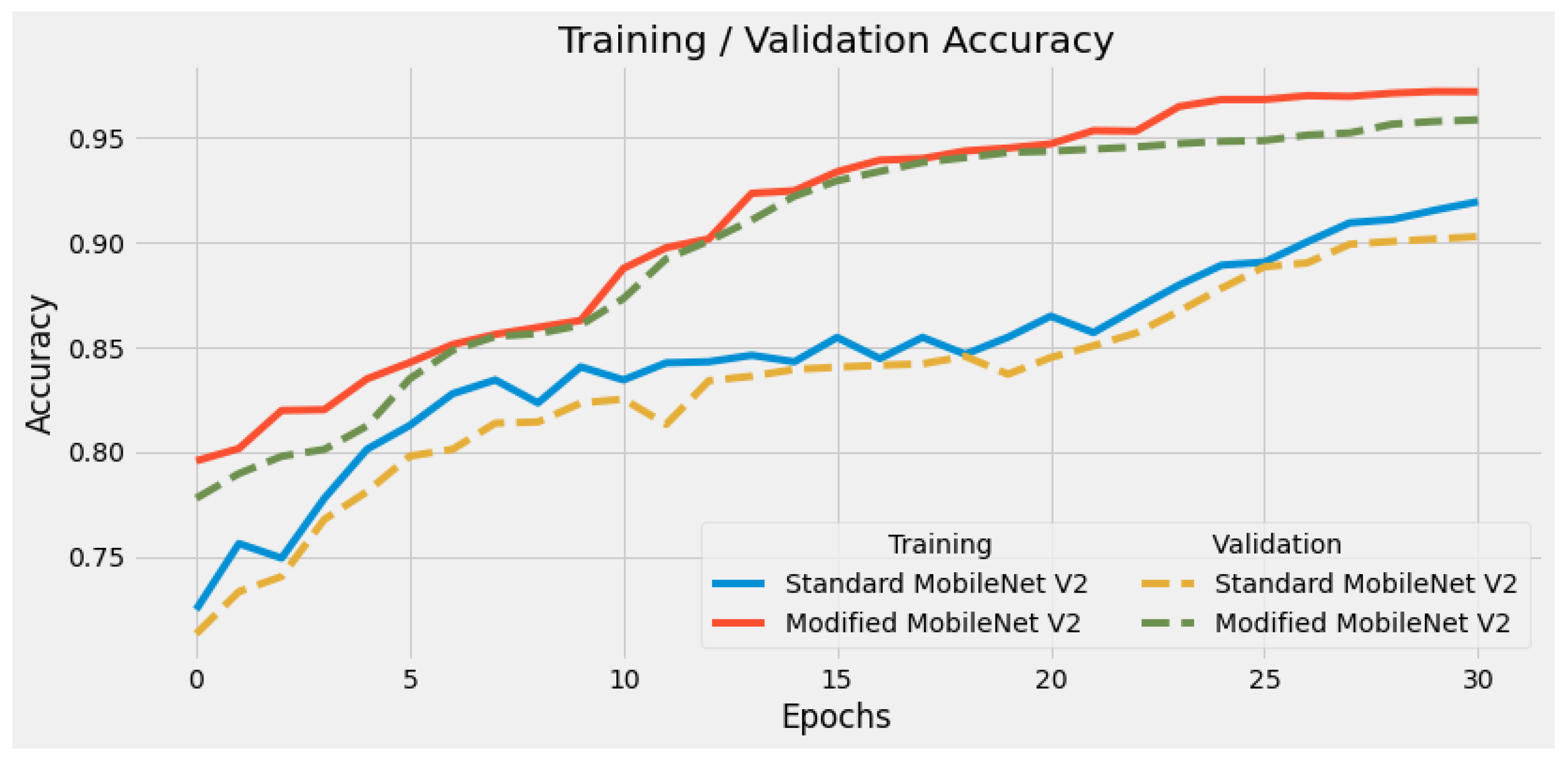
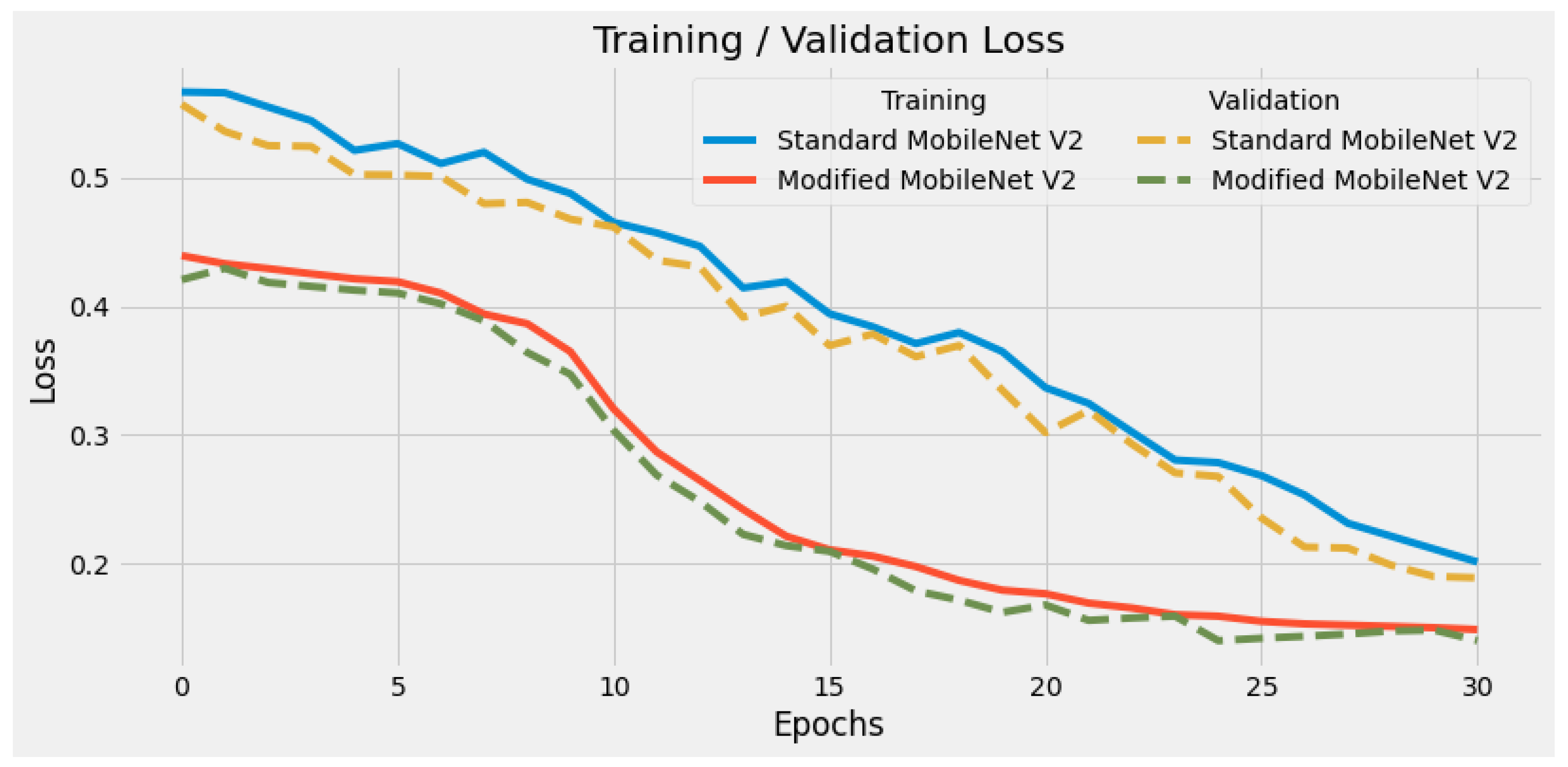
4. Experimental Results
Comparison with Other Approaches
5. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | Artificial Intelligence |
| ARDS | Acute Respiratory Distress Syndrome |
| ARM | Architecture Reference Manual |
| CNN | Convolutional Neural Network |
| CPU | Central Processing Unit |
| CUDA | Compute Unified Device Architecture |
| DL | Deep Learning |
| eMMC | Embedded MultiMedia Card |
| FN | False Negative |
| FP | False Positive |
| GPU | Graphics Processing Unit |
| RAM | Random access memory |
| ReLU | Rectified Linear Unit |
| PC | Personal Computer |
| PIL | Python Imaging Library |
| PNG | Portable Network Graphics |
| TN | True Negative |
| TP | True Positive |
| WHO | World Health Organization |
References
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/ (accessed on 5 January 2022).
- Worldometer. COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 15 January 2022).
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Puderbach, M.; Eichinger, M.; Haeselbarth, J.; Ley, S.; Kopp-Schneider, A.; Tuengerthal, S.; Schmaehl, A.; Fink, C.; Plathow, C.; Wiebel, M.; et al. Assessment of morphological MRI for pulmonary changes in cystic fibrosis (CF) patients: Comparison to thin-section CT and chest X-ray. Investig. Radiol. 2007, 42, 715–724. [Google Scholar] [CrossRef]
- Jaiswal, A.K.; Tiwari, P.; Kumar, S.; Gupta, D.; Khanna, A.; Rodrigues, J.J. Identifying pneumonia in chest X-rays: A deep learning approach. Measurement 2019, 145, 511–518. [Google Scholar] [CrossRef]
- Bai, H.X.; Hsieh, B.; Xiong, Z.; Halsey, K.; Choi, J.W.; Tran, T.M.L.; Pan, I.; Shi, L.B.; Wang, D.C.; Mei, J.; et al. Performance of radiologists in differentiating COVID-19 from non-COVID-19 viral pneumonia at chest CT. Radiology 2020, 296, E46–E54. [Google Scholar] [CrossRef]
- Chung, M.; Bernheim, A.; Mei, X.; Zhang, N.; Huang, M.; Zeng, X.; Cui, J.; Xu, W.; Yang, Y.; Fayad, Z.A.; et al. CT imaging features of 2019 novel coronavirus (2019-nCoV). Radiology 2020, 295, 202–207. [Google Scholar] [CrossRef] [Green Version]
- Toussie, D.; Voutsinas, N.; Finkelstein, M.; Cedillo, M.A.; Manna, S.; Maron, S.Z.; Jacobi, A.; Chung, M.; Bernheim, A.; Eber, C.; et al. Clinical and chest radiography features determine patient outcomes in young and middle-aged adults with COVID-19. Radiology 2020, 297, E197–E206. [Google Scholar] [CrossRef]
- Gattinoni, L.; Chiumello, D.; Caironi, P.; Busana, M.; Romitti, F.; Brazzi, L.; Camporota, L. COVID-19 pneumonia: Different respiratory treatments for different phenotypes? Intensive Care Med. 2020, 46, 1099–1102. [Google Scholar] [CrossRef]
- Zech, J.R.; Badgeley, M.A.; Liu, M.; Costa, A.B.; Titano, J.J.; Oermann, E.K. Variable generalization performance of a deep learning model to detect pneumonia in chest radiographs: A cross-sectional study. PLoS Med. 2018, 15, e1002683. [Google Scholar] [CrossRef] [Green Version]
- Hurt, B.; Kligerman, S.; Hsiao, A. Deep learning localization of pneumonia: 2019 coronavirus (COVID-19) outbreak. J. Thorac. Imaging 2020, 35, W87–W89. [Google Scholar] [CrossRef]
- Longoni, C.; Bonezzi, A.; Morewedge, C.K. Resistance to medical artificial intelligence. J. Consum. Res. 2019, 46, 629–650. [Google Scholar] [CrossRef]
- Sanida, T.; Varlamis, I. Application of Affinity Analysis Techniques on Diagnosis and Prescription Data. In Proceedings of the 2017 IEEE 30th International Symposium on Computer-Based Medical Systems (CBMS), Thessaloniki, Greece, 22–24 June 2017; pp. 403–408. [Google Scholar] [CrossRef]
- Sanchez-Reyes, L.M.; Rodriguez-Resendiz, J.; Salazar-Colores, S.; Avecilla-Ramírez, G.N.; Pérez-Soto, G.I. A High-accuracy mathematical morphology and multilayer perceptron-based approach for melanoma detection. Appl. Sci. 2020, 10, 1098. [Google Scholar] [CrossRef] [Green Version]
- Toledo-Perez, D.; Rodríguez-Reséndiz, J.; Gómez-Loenzo, R.A. A study of computing zero crossing methods and an improved proposal for EMG signals. IEEE Access 2020, 8, 8783–8790. [Google Scholar] [CrossRef]
- Ortiz-Echeverri, C.J.; Salazar-Colores, S.; Rodríguez-Reséndiz, J.; Gómez-Loenzo, R.A. A new approach for motor imagery classification based on sorted blind source separation, continuous wavelet transform, and convolutional neural network. Sensors 2019, 19, 4541. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Reyes, L.M.; Rodríguez-Reséndiz, J.; Avecilla-Ramírez, G.N.; García-Gomar, M.L.; Robles-Ocampo, J.B. Impact of eeg parameters detecting dementia diseases: A systematic review. IEEE Access 2021, 9, 78060–78074. [Google Scholar] [CrossRef]
- Kermany, D.S.; Goldbaum, M.; Cai, W.; Valentim, C.C.; Liang, H.; Baxter, S.L.; McKeown, A.; Yang, G.; Wu, X.; Yan, F.; et al. Identifying medical diagnoses and treatable diseases by image-based deep learning. Cell 2018, 172, 1122–1131. [Google Scholar] [CrossRef]
- Rajpurkar, P.; Irvin, J.; Zhu, K.; Yang, B.; Mehta, H.; Duan, T.; Ding, D.; Bagul, A.; Langlotz, C.; Shpanskaya, K.; et al. Chexnet: Radiologist-level pneumonia detection on chest x-rays with deep learning. arXiv 2017, arXiv:1711.05225. [Google Scholar]
- Shi, F.; Wang, J.; Shi, J.; Wu, Z.; Wang, Q.; Tang, Z.; He, K.; Shi, Y.; Shen, D. Review of artificial intelligence techniques in imaging data acquisition, segmentation and diagnosis for COVID-19. IEEE Rev. Biomed. Eng. 2020, 14, 4–15. [Google Scholar] [CrossRef] [Green Version]
- Bullock, J.; Luccioni, A.; Pham, K.H.; Lam, C.S.N.; Luengo-Oroz, M. Mapping the landscape of artificial intelligence applications against COVID-19. J. Artif. Intell. Res. 2020, 69, 807–845. [Google Scholar] [CrossRef]
- Tayarani-N, M.H. Applications of artificial intelligence in battling against COVID-19: A literature review. Chaos Solitons Fractals 2020, 142, 110338. [Google Scholar] [CrossRef]
- Yang, W.; Sirajuddin, A.; Zhang, X.; Liu, G.; Teng, Z.; Zhao, S.; Lu, M. The role of imaging in 2019 novel coronavirus pneumonia (COVID-19). Eur. Radiol. 2020, 30, 4874–4882. [Google Scholar] [CrossRef] [Green Version]
- Greenspan, H.; Van Ginneken, B.; Summers, R.M. Guest editorial deep learning in medical imaging: Overview and future promise of an exciting new technique. IEEE Trans. Med. Imaging 2016, 35, 1153–1159. [Google Scholar] [CrossRef]
- Sanida, T.; Tsiktsiris, D.; Sideris, A.; Dasygenis, M. A Heterogeneous Lightweight Network for Plant Disease Classification. In Proceedings of the 2021 10th International Conference on Modern Circuits and Systems Technologies (MOCAST), Thessaloniki, Greece, 5–7 July 2021; pp. 1–4. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Paluru, N.; Dayal, A.; Jenssen, H.B.; Sakinis, T.; Cenkeramaddi, L.R.; Prakash, J.; Yalavarthy, P.K. Anam-Net: Anamorphic depth embedding-based lightweight CNN for segmentation of anomalies in COVID-19 chest CT images. IEEE Trans. Neural Netw. Learn. Syst. 2021, 32, 932–946. [Google Scholar] [CrossRef]
- An, L.; Peng, K.; Yang, X.; Huang, P.; Luo, Y.; Feng, P.; Wei, B. E-TBNet: Light Deep Neural Network for Automatic Detection of Tuberculosis with X-ray DR Imaging. Sensors 2022, 22, 821. [Google Scholar] [CrossRef]
- Kamal, K.; Yin, Z.; Wu, M.; Wu, Z. Evaluation of deep learning-based approaches for COVID-19 classification based on chest X-ray images. Signal Image Video Process. 2021, 15, 959–966. [Google Scholar]
- Ghoshal, B.; Tucker, A. Estimating uncertainty and interpretability in deep learning for coronavirus (COVID-19) detection. arXiv 2020, arXiv:2003.10769. [Google Scholar]
- Khan, A.I.; Shah, J.L.; Bhat, M.M. CoroNet: A deep neural network for detection and diagnosis of COVID-19 from chest x-ray images. Comput. Methods Programs Biomed. 2020, 196, 105581. [Google Scholar] [CrossRef]
- Mahmud, T.; Rahman, M.A.; Fattah, S.A. CovXNet: A multi-dilation convolutional neural network for automatic COVID-19 and other pneumonia detection from chest X-ray images with transferable multi-receptive feature optimization. Comput. Biol. Med. 2020, 122, 103869. [Google Scholar] [CrossRef]
- Wang, L.; Lin, Z.Q.; Wong, A. COVID-net: A tailored deep convolutional neural network design for detection of COVID-19 cases from chest x-ray images. Sci. Rep. 2020, 10, 19549. [Google Scholar] [CrossRef]
- Ozturk, T.; Talo, M.; Yildirim, E.A.; Baloglu, U.B.; Yildirim, O.; Acharya, U.R. Automated detection of COVID-19 cases using deep neural networks with X-ray images. Comput. Biol. Med. 2020, 121, 103792. [Google Scholar] [CrossRef] [PubMed]
- Apostolopoulos, I.D.; Mpesiana, T.A. COVID-19: Automatic detection from x-ray images utilizing transfer learning with convolutional neural networks. Phys. Eng. Sci. Med. 2020, 43, 635–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misra, S.; Jeon, S.; Lee, S.; Managuli, R.; Jang, I.S.; Kim, C. Multi-channel transfer learning of chest x-ray images for screening of COVID-19. Electronics 2020, 9, 1388. [Google Scholar] [CrossRef]
- El Asnaoui, K.; Chawki, Y. Using X-ray images and deep learning for automated detection of coronavirus disease. J. Biomol. Struct. Dyn. 2020, 39, 3615–3626. [Google Scholar] [CrossRef] [PubMed]
- Narin, A.; Kaya, C.; Pamuk, Z. Automatic detection of coronavirus disease (COVID-19) using x-ray images and deep convolutional neural networks. Pattern Anal. Appl. 2021, 24, 1207–1220. [Google Scholar] [CrossRef]
- Kaggle. COVID-19 Radiography Dataset. Available online: https://www.kaggle.com/tawsifurrahman/covid19-radiography-database/activity (accessed on 25 May 2021).
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L.C. Mobilenetv2: Inverted residuals and linear bottlenecks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 4510–4520. [Google Scholar]
- Yadav, S.S.; Jadhav, S.M. Deep convolutional neural network based medical image classification for disease diagnosis. J. Big Data 2019, 6, 113. [Google Scholar] [CrossRef] [Green Version]
- Deng, J.; Dong, W.; Socher, R.; Li, L.J.; Li, K.; Fei-Fei, L. Imagenet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar]
- Lin, M.; Chen, Q.; Yan, S. Network in network. arXiv 2013, arXiv:1312.4400. [Google Scholar]
- Hinton, G.E. Rectified linear units improve restricted boltzmann machines vinod nair. Citeseer 2010, 7, 1–8. [Google Scholar]
- Hinton, G.E.; Srivastava, N.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R.R. Improving neural networks by preventing co-adaptation of feature detectors. arXiv 2012, arXiv:1207.0580. [Google Scholar]
- Hawkins, D.M. The problem of overfitting. J. Chem. Inf. Comput. Sci. 2004, 44, 1–12. [Google Scholar] [CrossRef]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A simple way to prevent neural networks from overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Nvidia Developer. Jetson AGX Xavier Developer Kit. Available online: https://developer.nvidia.com/embedded/jetson-agx-xavier-developer-kit (accessed on 30 May 2021).
- Mittal, S.; Vetter, J.S. A survey of CPU-GPU heterogeneous computing techniques. ACM Comput. Surv. (CSUR) 2015, 47, 1–35. [Google Scholar] [CrossRef]
- Ardiyanto, I.; Nugroho, H.A.; Buana, R.L.B. Deep learning-based diabetic retinopathy assessment on embedded system. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Korea, 11–15 July 2017; pp. 1760–1763. [Google Scholar]
- Page, A.; Shea, C.; Mohsenin, T. Wearable seizure detection using convolutional neural networks with transfer learning. In Proceedings of the 2016 IEEE International Symposium on Circuits and Systems (ISCAS), Montreal, QC, Canada, 22–25 May 2016; pp. 1086–1089. [Google Scholar]
- Attaran, N.; Puranik, A.; Brooks, J.; Mohsenin, T. Embedded low-power processor for personalized stress detection. IEEE Trans. Circuits Syst. II Express Briefs 2018, 65, 2032–2036. [Google Scholar] [CrossRef]
- Géron, A. Hands-on Machine Learning with Scikit-Learn, Keras, and TensorFlow: Concepts, Tools, and Techniques to Build Intelligent Systems; O’Reilly Media: Sebastopol, CA, USA, 2019. [Google Scholar]
- Hossin, M.; Sulaiman, M. A review on evaluation metrics for data classification evaluations. Int. J. Data Min. Knowl. Manag. Process. 2015, 5, 1. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Train | Validation | Test |
|---|---|---|---|
| COVID-19 | 2530 | 723 | 363 |
| Normal | 7134 | 2038 | 1020 |
| Lung Opacity | 4208 | 1202 | 602 |
| Viral Pneumonia | 941 | 269 | 135 |
| Total | 14,813 | 4232 | 2120 |
| Layer (Type) | Output Shape | Parameters |
|---|---|---|
| MobileNetV2 (Model) | 2,257,984 | |
| Global Average Pooling | 0 | 0 |
| Fully Connected Layer | 512 | 655,872 |
| Dropout | 0 | 0 |
| Fully Connected Layer (Classes) | 4 | 2052 |
| Total Parameters: 2,915,908 | ||
| Parameters | Value |
|---|---|
| Optimizer | Adam ( and ) |
| Learning Rate | 0.001–0.0001 |
| Batch Size | 32 |
| Dropout value | 0.20 |
| Loss Function | Categorical cross-entropy |
| Activation function at intermediate layers | ReLU |
| Activation function at output layer | SoftMax |
| Total Training Epochs | 30 |
| Modified MobileNetV2 | Standard MobileNetV2 | ||||||
|---|---|---|---|---|---|---|---|
| Class | Precision | Recall | F1-Score | Precision | Recall | F1-Score | Support |
| COVID | 0.9888 | 0.9697 | 0.9791 | 0.8880 | 0.9174 | 0.9024 | 363 |
| Lung Opacity | 0.9416 | 0.9369 | 0.9392 | 0.8680 | 0.8953 | 0.8814 | 602 |
| Normal | 0.9527 | 0.9667 | 0.9596 | 0.9312 | 0.9029 | 0.9169 | 1020 |
| Viral Pneumonia | 0.9923 | 0.9556 | 0.9736 | 0.9259 | 0.9259 | 0.9259 | 135 |
| Accuracy | 0.9580 | 0.9047 | 2120 | ||||
| Macro avg | 0.9688 | 0.9572 | 0.9629 | 0.9033 | 0.9104 | 0.9067 | 2120 |
| Weighted avg | 0.9582 | 0.9580 | 0.9581 | 0.9055 | 0.9047 | 0.9049 | 2120 |
| Study | Architecture | Dataset | Number of Classes | Number of Parameters (million) | Overall Accuracy (%) |
|---|---|---|---|---|---|
| [30] | MobileNetV2 | 186 COVID-19, 186 normal, 186 bacterial pneumonia and 186 viral pneumonia | 4 | 3.5 | 95.40 |
| [31] | Bayesian CNN | 68 COVID-19, 1.583 normal, 2.786 bacterial pneumonia and 1.504 viral pneumonia | 4 | - | 89.82 |
| [32] | CoroNet | 284 COVID-19, 310 normal, 330 bacterial pneumonia and 327 viral pneumonia | 4 | 33 | 89.60 |
| [33] | CovXNet | 305 COVID-19, 305 normal, 305 viral pneumonia and 305 bacterial pneumonia | 4 | - | 90.20 |
| [34] | COVID Net | 358 COVID-19, 8.066 normal and 5.538 pneumonia | 3 | 11.75 | 93.30 |
| [35] | DarkCovidNet | 127 COVID-19, 500 normal and 500 pneumonia | 3 | 3.1 | 87.02 |
| [36] | MobileNetV2 | 224 COVID-19, 504 normal, 714 bacterial and viral pneumonia | 3 | - | 94.72 |
| [37] | ResNet | 184 COVID-19, 1.579 normal and 4.245 pneumonia | 3 | 25 | 93.90 |
| [38] | MobileNetV2 | 231 COVID-19, 1.583 normal and 2.780 bacterial pneumonia | 3 | - | 85.47 |
| Proposed | Modified MobileNetV2 | 3.616 COVID-19, 10.192 normal, 6.012 lung opacity and 1.345 viral pneumonia | 4 | 2.9 | 95.80 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanida, T.; Sideris, A.; Tsiktsiris, D.; Dasygenis, M. Lightweight Neural Network for COVID-19 Detection from Chest X-ray Images Implemented on an Embedded System. Technologies 2022, 10, 37. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies10020037
Sanida T, Sideris A, Tsiktsiris D, Dasygenis M. Lightweight Neural Network for COVID-19 Detection from Chest X-ray Images Implemented on an Embedded System. Technologies. 2022; 10(2):37. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies10020037
Chicago/Turabian StyleSanida, Theodora, Argyrios Sideris, Dimitris Tsiktsiris, and Minas Dasygenis. 2022. "Lightweight Neural Network for COVID-19 Detection from Chest X-ray Images Implemented on an Embedded System" Technologies 10, no. 2: 37. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies10020037