Vitamin E-Bonded Membranes Do Not Influence Markers of Oxidative Stress in Hemodialysis Patients with Homozygous Glutathione Transferase M1 Gene Deletion

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
2.2. Primary Endpoint
2.2.1. Markers of Anti-Oxidant Activity
2.2.2. Markers of Oxidative Damage
2.2.3. Markers of Inflammation
2.3. Secondary Endpoints
2.4. Safety Data
3. Discussion
3.1. Primary Endpoints
3.2. Markers of Antioxidant Activity
3.3. Markers of Oxidative Damage
3.4. Markers of Inflammation
3.5. Secondary Endpoints
4. Conclusions
5. Materials and Methods
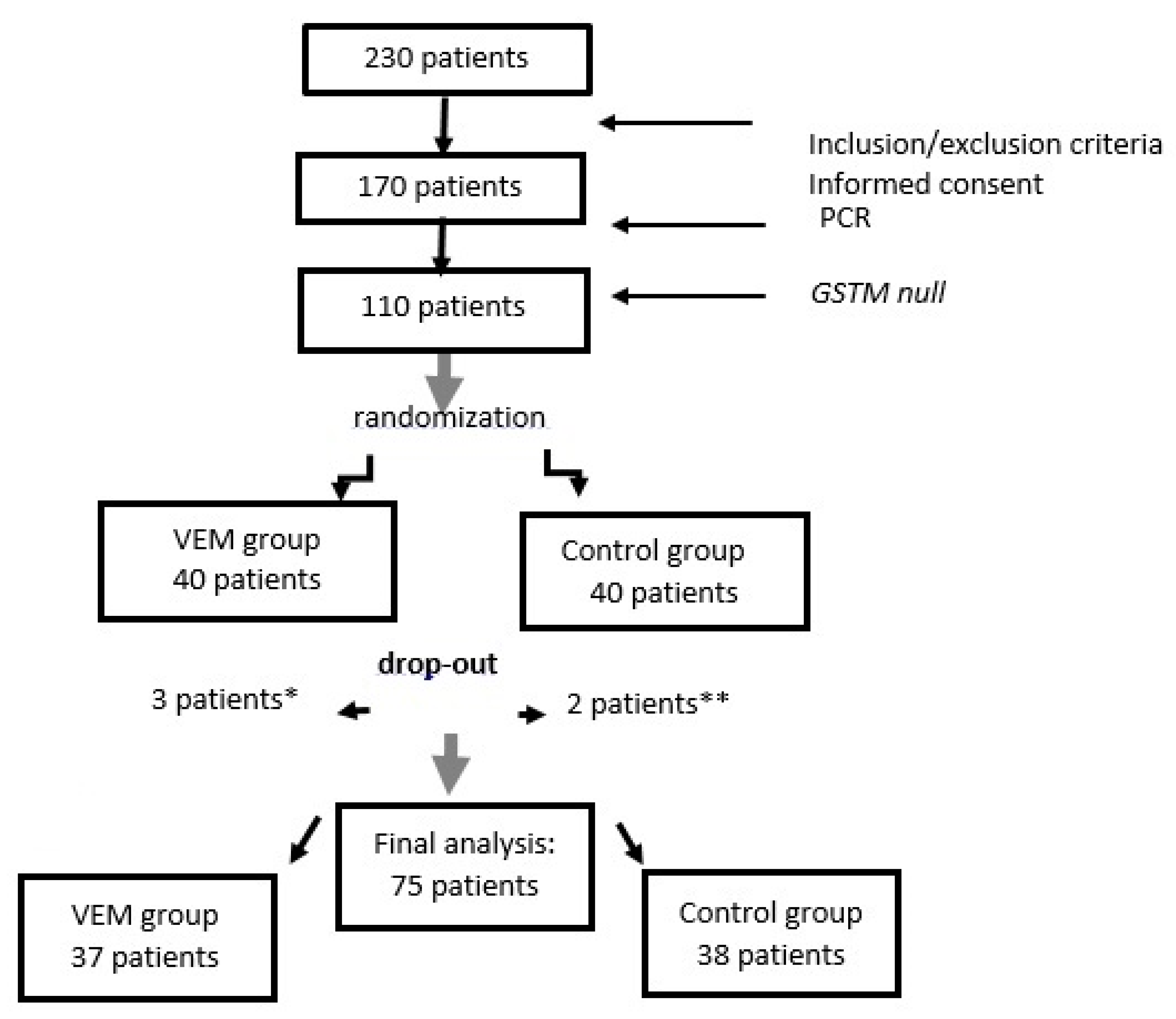
5.1. Patients and Trial Protocol
5.2. Demographic, Biochemical and Dialysis Data
5.3. Glutathione Transferase (GST) Genotyping
5.4. Determination of GSTM1 Gene Polymorphism
5.5. Plasma Separation
5.6. Protein Thiol Groups
5.7. Measurement of Malondialdehyde Level
5.8. Measurement of IL-6 Level
5.9. Determining the Activity of Antioxidant Enzymes
5.10. Statistics
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Usberti, M.; Gerardi, G.M.; Gazzotti, R.M.; Benedini, S.; Archetti, S.; Sugherini, L.; Valentini, M.; Tira, P.; Bufano, G.; Albertini, A.; et al. Oxidative stress and cardiovascular disease in dialyzed patients. Nephron 2002, 91, 25–33. [Google Scholar] [CrossRef]
- Sies, H.; Berndt, C.; Jones, D.P. Oxidative Stress. Annu. Rev. Biochem. 2017, 86, 715–748. [Google Scholar] [CrossRef]
- Salem, M.; Ivanovich, P.; Mujais, S. Biocompatibility of dialysis membranes. Contrib. Nephrol. 1993, 103, 55–64. [Google Scholar] [PubMed] [Green Version]
- Mimic-Oka, J.; Simic, T.; Ekmescic, V.; Dragicevic, P. Erythrocyte glutathione peroxidase and superoxide dismutase activities in different stages of chronic renal failure. Clin. Nephrol. 1995, 44, 44–48. [Google Scholar] [PubMed]
- Mimic-Oka, J.; Simic, T.; Djukanovic, L.; Reljić, Z.; Davicević, Z. Alteration in plasma antioxidant capacity in various degrees of chronic renal failure. Clin. Nephrol. 1999, 51, 233–241. [Google Scholar]
- Lin, Y.S.; Hung, S.C.; Wei, Y.H.; Tarng, D.C. GST M1 polymorphism associates with DNA oxidative damage and mortality among hemodialysis patients. J. Am. Soc. Nephrol. 2009, 20, 405–415. [Google Scholar] [CrossRef] [Green Version]
- Libetta, C.; Sepe, V.; Esposito, P.; Galli, F.; Dal Canton, A. Oxidative stress and inflammation: Implications in uremia and hemodialysis. Clin. Biochem. 2011, 44, 1189–1198. [Google Scholar] [CrossRef]
- Yilmaz, M.I.; Saglam, M.; Caglar, K.; Cakir, E.; Sonmez, A.; Ozgurtas, T.; Aydin, A.; Eyileten, T.; Ozcan, O.; Acikel, C.; et al. The Determinants of Endothelial Dysfunction in CKD: Oxidative Stress and Asymmetric Dimethylarginine. Am. J. Kidney Dis. 2006, 47, 42–50. [Google Scholar] [CrossRef]
- Mimic-Oka, J.; Simic, T.; Djukanovic Lj Stefanovski, J.; Ramic, Z. Glutathione and its associated enzymes in peripheral blood cells in different stages of renal insufficiency. Amino Acids 1992, 2, 215–224. [Google Scholar]
- Scott, B.; Deman, A.; Peeters, P.; Van den Branden, C.; Stolear, J.C.; Van Camp, G.; Verbeelen, D. Cardiac troponin T and malondialdehyde modified plasma lipids in haemodialysis patients. Nephrol. Dial. Transplant. 2003, 18, 737–742. [Google Scholar] [CrossRef] [Green Version]
- Board, P.; Coggan, M.; Johnston, P.; Ross, V.; Suzuki, T.; Webb, G. Genetic heterogeneity of the human glutathione transferases: A complex of gene families. Pharmacol. Ther. 1990, 48, 357–369. [Google Scholar] [CrossRef]
- Suvakov, S.; Jerotic, D.; Damjanovic, T.; Milic, N.; Pekmezovic, T.; Djukic, T.; Jelic-Ivanovic, Z.; Savic Radojevic, A.; Pljesa-Ercegovac, M.; Matic, M.; et al. Markers of Oxidative Stress and Endothelial Dysfunction Predict Haemodialysis Patients Survival. Am. J. Nephrol. 2019, 50, 115–125. [Google Scholar] [CrossRef]
- Bargnoux, A.S.; Cristol, J.P.; Jaussent, I.; Chalabi, L.; Bories, P.; Dion, J.J.; Henri, P.; Delage, M.; Dupuy, A.M.; Badiou, S.; et al. Vitamin E-coated polysulfone membrane improved red blood cell antioxidant status in hemodialysis patients. J. Nephrol. 2013, 26, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Kohlová, M.; Amorim, C.G.; Araújo, A.; Santos-Silva, A.; Solich, P.; Montenegro, M.C.B. The biocompatibility and bioactivity of hemodialysis membranes: Their impact in end-stage renal disease. J. Artif. Organs 2019, 22, 14–28. [Google Scholar] [CrossRef] [PubMed]
- Piroddi, M.; Pilolli, F.; Aritomi, M.; Galli, F. Vitamin E as a functional and biocompatibility modifier of synthetic hemodialyzer membranes: An overview of the literature on vitamin E-modified hemodialyzer membranes. Am. J. Nephrol. 2012, 1, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Galli, F. Vitamin E-derived copolymers continue the challenge to hemodialysis biomaterials. World J. Nephrol. 2012, 1, 100–105. [Google Scholar] [CrossRef] [PubMed]
- D’Arrigo, G.; Baggetta, R.; Tripepi, G.; Galli, F.; Bolignano, D. Effects of Vitamin E-Coated versus Conventional Membranes in Chronic Hemodialysis Patients: A Systematic Review and Meta-Analysis. Blood Purif. 2017, 43, 101–122. [Google Scholar] [CrossRef]
- Mydlík, M.; Derzsiová, K.; Rácz, O.; Sipulová, A.; Lovásová, E.; Molcányiová, A.; Petrovicová, J. Vitamin E-coated dialyzer and antioxidant defense parameters: Three-month study. Semin. Nephrol. 2004, 24, 525–531. [Google Scholar] [CrossRef]
- Yang, S.K.; Xiao, L.; Xu, B.; Xu, X.X.; Liu, F.Y.; Sun, L. Effects of vitamin E-coated dialyzer on oxidative stress and inflammation status in hemodialysis patients: A systematic review and meta-analysis. Ren. Fail. 2014, 36, 722–731. [Google Scholar] [CrossRef] [Green Version]
- Mandolfo, S.; Corradi, B.; Bucci, R.; Farina, M.; Pilolli, F.; Galli, F. Evaluation of the impact of a new synthetic vitamin E-bonded membrane on anemia and rHuEPO requirement in ESRD patients with central venous catheters: A pilot study. Int. Urol. Nephrol. 2012, 44, 1493–1500. [Google Scholar] [CrossRef]
- Andrulli, S.; Di Filippo, S.; Manzoni, C.; Stefanelli, L.; Floridi, A.; Galli, F.; Locatelli, F. Effect of synthetic vitamin E-bonded membrane on responsiveness to erythropoiesis-stimulating agents in hemodialysis patients: A pilot study. Nephron Clin. Pract. 2010, 115, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Aoun, B.; Janssen-Lozinska, Y.; Ulinski, T. Effect of vitamin E coated dialyzers on anticoagulation requirement in hemodialyzed children. Saudi J. Kidney Dis. Transpl. 2010, 21, 466–470. [Google Scholar] [PubMed]
- Lines, S.W.; Carter, A.M.; Dunn, E.J.; Lindley, E.J.; Tattersall, J.E.; Wright, M.J. A randomized controlled trial evaluating the erythropoiesis stimulating agent sparing potential of a vitamin E-bonded polysulfone dialysis membrane. Nephrol. Dial. Transplant. 2014, 29, 649–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Locatelli, F.; Andrulli, S.; Vigano, S.M.; Concetti, M.; Urbini, S.; Giacchino, F.; Broccoli, R.; Aucella, F.; Cossu, M.; Conti, P.; et al. Evaluation of the impact of a new synthetic vitamin E-bonded membrane on the hypo-responsiveness to the erythropoietin therapy in hemodialysis patients: A multicenter study. Blood Purif. 2017, 43, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Nishikawa, O.; Yukawa, S.; Yoshimoto, M.; Nishide, I. Effects of hemodialysis membrane on serum lipid profile of maintenance hemodialysis patients. Nihon Jinzo Gakkai Shi 1999, 41, 1–7. [Google Scholar] [PubMed]
- Tsuruoka, S.; Kawaguchi, A.; Nishiki, K.; Hayasaka, T.; Fukushima, C.; Sugimoto, K.; Saito, T.; Fujimura, A. Vitamin E-bonded hemodialyzer improves neutrophil function and oxidative stress in patients with end-stage renal failure. Am. J. Kidney Dis. 2002, 39, 127–133. [Google Scholar] [CrossRef]
- Daugirdas, J.T. Second generation logarithmic estimates of single-pool variable volume Kt/V: An analysis of error. J. Am. Soc. Nephrol. 1993, 4, 1205–1213. [Google Scholar]
- The Renal Association. UK Renal Registry: The Fourteenth Annual Report; The Renal Association: Bristol, UK, 2011. [Google Scholar]
- Abdel-Rahman, S.Z.; El-Zein, R.A.; Anwar, W.A.; Au, W.W. A multiplex PCR procedure for polymorphic analysis of GSTM1 and GSTT1 genes in population studies. Cancer Lett. 1996, 107, 229–233. [Google Scholar] [CrossRef]
- Jocelyn, P.C. Spectrophotometric Assay of Thiols. Methods Enzymol. 1987, 143, 44–67. [Google Scholar]
- Misra, H.P.; Fridovich, I. The role of superoxide anion in the autoxidation of epinephrine and a simple assay for superoxide dismutase. J. Biol. Chem. 1972, 247, 3170–3175. [Google Scholar]
- Flohé, L.; Günzler, W.A. Assays of glutathione peroxidase. Methods Enzymol. 1984, 105, 114–121. [Google Scholar] [PubMed]


{kind=link}
| Variable | Control Group n = 40 | VEM Group n= 40 | p |
|---|---|---|---|
| Males, % | 55 | 60 | 0.651 |
| Age, years | 65 ± 12 | 62 ± 11 | 0.225 |
| Mean Rank (Sum of Ranks) | 44.1 (1764) | 36.9 (1476) | 0.160 |
| Body weight kg (mean ± SD) | 69.8 ± 15.4 | 74.3 ± 14.8 | 0.182 |
| Mean Rank (Sum of Ranks) | 36.1 (1472) | 44.2 (1768) | 0.427 |
| AVF, No, % | 39/97.5 | 36/90.0 | 0.210 |
| Dialysis vintage, months | 71.5 ± 65.7 | 66.6 ± 58.7 | 0.726 |
| Diabetes (main disease or co-morbidity), No, % | 11/27.5 | 12/32.2 | 0.875 |
| IM (yes) No, % | 4/10 | 2/5 | 0.675 |
| Stroke (yes) No, % | 1/2.5 | 1/2.5 | 1.000 |
| HTA (yes) No, % | 39/97.5 | 39/97.5 | 1.000 |
| ESRD assumed due to (No, %): | 0.273 | ||
| Hypertension | 19/47.5 | 12/30.0 | |
| Diabetes mellitus | 7/17.5 | 6/15.0 | |
| Glomerulonephritis | 6/15.0 | 5/12.5 | |
| ADPKD | 4/10.0 | 10/25.0 | |
| Other | 4/10.0 | 7/17.5 | |
| HDF (yes) No, % | 6/15 | 10/25 | 0.264 |
| Dialyzer surface, m2 | 1.62 ± 0.27 | 1.67 ± 0.32 | 0.407 |
| S-urea, mmol/L | 23.1 ± 7.1 | 23.0 ± 6.0 | 0.981 |
| S-Creatinine, umol/L | 872 ± 211 | 853 ± 154 | 0.649 |
| S-Bicarbonate, mmol/L | 20.3 ± 2.4 | 13.0 ± 3.8 | 0.782 |
| Kt/V | 1.32 ± 0.31 | 1.35 ± 0.30 | 0.657 |
| Mean Rank (Sum of Ranks) | 39.2 (1569) | 41.78 (1671) | 0.624 |
| Kt/V in target, % | 68.4 | 73.0 | 0.801 |
| CRP, mg/L | 4.57 ± 5.07 | 5.49 ± 5.29 | 0.430 |
| CRP in reference range, % | 72.5 | 60.0 | 0.344 |
| Parameter | Control Group N = 40 | VEM Group N = 40 | p |
|---|---|---|---|
| ESA (yes) No, % | 31/77.5 | 32/80.0 | 0.785 |
| ESA dose, IU/week | 6677 ± 3995 | 5156 ± 3380 | 0.108 |
| Hb, g/dL | 10.5 ± 1.0 | 10.5 ± 1.0 | 0.874 |
| Hb in target range, % | 92.5 | 92.5 | 1.000 |
| ERI | 11.3 ± 10.1 | 7.4 ± 5.6 | 0.063 |
| Transferrin saturation, % | 28 ± 9 | 34 ± 10 | 0.014 |
| Ferritin, ng/mL | 212 ± 224 | 258 ± 146 | 0.281 |
| Albumin, g/L | 39.0 ± 2.9 | 40.1 ± 3.3 | 0.165 |
| Serum-Iron, umol/L | 10.8 ± 3.7 | 13.0 ± 3.8 | 0.010 |
| Total proteins, g/L | 68.3 ± 5.5 | 67.6 ± 5.0 | 0.552 |
| PTH, pg/mL | 278 ± 361 | 290 ± 524 | 0.905 |
| Total Cholesterol, mmol/L | 4.25 ± 0.98 | 4.54 ± 0.88 | 0.170 |
| HDL-Cholesterol, mmol/L | 1.08 ± 0.41 | 0.99 ± 0.24 | 0.260 |
| LDL-Cholesterol, mmol/L | 2.38 ± 0.75 | 2.67 ± 0.79 | 0.106 |
| Triglycerides, mmol/L | 1.83 ± 1.24 | 2.22 ± 1.22 | 0.161 |
| S-Ca, mmol/L | 2.29 ± 0.24 | 2.29 ± 0.23 | 0.925 |
| S-PO4, mmol/L | 1.61 ± 0.57 | 1.8 ± 0.51 | 0.109 |
| Parameter | Control Group | VEM Group | ||||
|---|---|---|---|---|---|---|
| Before | After | Before | After | p | p * | |
| Markers of anti-oxidant activity | ||||||
| GPX, nmol/mg | 0.000 | 0.474 | ||||
| PP data | 206.7 ± 67.2 | 273.7 ± 61.6 | 203.7 ± 59.1 | 285.7 ± 78.7 | ||
| ITT data | 204.6 ± 66.9 | 273.7 ± 61.6 | 201.7 ± 60.6 | 285.7 ± 78.7 | ||
| SOD, U × 103/L | 0.269 | 0.607 | ||||
| PP data | 55.4 ± 11.7 | 60.4 ± 22.4 | 53.8 ± 9.8 | 55.1 ± 21.2 | ||
| ITT data | 55.4 ± 11.5 | 60.4 ± 22.4 | 53.8 ± 9.5 | 55.7 ± 21.2 | ||
| Markers of oxidative damage | ||||||
| MDA, ng/mL | ||||||
| PP data | 510.9 ± 394.7 | 69.5 ± 440.7 | 403.4 ± 218.8 | 752.1 ± 439.0 | 0.000 | 0.446 |
| ITT data | 691.5 ± 478.3 | 69.5 ± 440.7 | 598.5 ± 425.7 | 729.9 ± 438.7 | ||
| Mean Rank (Sum of Ranks) | 32.6 (978) | 21.5(430) | 29.4(912) | 19.5(389) | ||
| Thiol groups, mcmol/L | 0.000 | 0.445 | ||||
| PP data | 6.79 ± 1.81 | 8.33 ± 2.26 | 7.31 ± 2.58 | 8.31 ± 2.48 | ||
| ITT data | 6.69 ± 1.86 | 8.33 ± 2.26 | 7.23 ± 2.61 | 8.31 ± 2.48 | ||
| Markers of inflammation | ||||||
| IL-6, ng/mL | ||||||
| PP data | 48.5 ± 40.7 | 67.6 ± 120.2 | 34.4 ± 32.4 | 34.4 ± 32.4 | 0.543 | 0.376 |
| ITT data | 37.5 ± 34.8 | 67.6 ± 120.2 | 34.5 ± 26.3 | 33.3 ± 31.4 | ||
| Mean Rank (Sum of Ranks) | 37.2(1412) | 26.1(548) | 37.9(1363) | 23.3(628) | ||
| CRP, mg/L | 0.458 | 0.894 | ||||
| PP data | 4.9 ± 5.4 | 5.5 ± 6.2 | 5.1 ± 4.8 | 5.9 ± 7.0 | ||
| ITT data | 4.6 ± 5.1 | 5.5 ± 6.2 | 5.5 ± 5.3 | 5.9 ± 7.0 | ||
| Parameter | Control Group | VEM Group | ||||
|---|---|---|---|---|---|---|
| Before | After | Before | After | p | p * | |
| ESA dose, IU/week | 0.427 | 0.491 | ||||
| PP data | 6862 ± 4033 | 6344 ± 3957 | 5630 ± 3443 | 5593 ± 3765 | ||
| ITT data | 6677 ± 3995 | 6000 ± 3856 | 5156 ± 3380 | 5379 ± 3717 | ||
| ESA (yes) No, % | 0.540 | 0.213 | ||||
| PP data | 31/81 | 33/86.8 | 31/83.8 | 29/78.4 | ||
| ITT data | 31/77.5 | 33/86.8 | 32/80.0 | 29/78.4 | ||
| Transferrin saturation, % | 0.766 | 0.020 | ||||
| PP data | 28.0 ± 8.8 | 33.0 ± 11.5 | 33.8 ± 10.1 | |||
| ITT data | 28.0 ± 9.0 | 32.8 ± 11.5 | 34.0 ±10.0 | 30.4 ± 10.9 | ||
| Ferritin, ng/mL | 0.262 | 0.061 | ||||
| PP data | 215 ± 230 | 271 ± 274 | 245 ± 141 | 230 ± 165 | ||
| ITT data | 212 ± 224 | 272 ± 274 | 258 ± 146 | 230 ± 165 | ||
| Iron dose, mg | 203 ± 256 | 222 ± 199 | 0.697 | |||
| S-Iron, umol/L | 0.817 | 0.087 | ||||
| PP data | 10.8 ± 3.8 | 11.7 ± 4.2 | 13.1 ± 3.7 | 11.9 ± 4.1 | ||
| ITT data | 10.8 ± 3.7 | 11.7 ± 4.2 | 13.0 ± 3.8 | 11.9 ± 4.1 | ||
| Hb, g/dL | 0.347 | 0.229 | ||||
| PP data | 10.48 ± 0.94 | 10.17 ± 0.93 | 10.49 ± 1.06 | 10.53 ± 1.37 | ||
| ITT data | 10.50 ± 1.00 | 10.17 ± 0.93 | 10.50 ± 1.00 | 10.53 ± 1.37 | ||
| Er, 1012/L | 0.598 | 0.053 | ||||
| PP data | 3.49 ± 0.35 | 3.36 ± 0.34 | 3.42 ± 0.36 | 3.49 ± 0.51 | ||
| ITT data | 3.49 ± 0.34 | 3.36 ± 0.34 | 3.42 ± 0.40 | 3.49 ± 0.51 | ||
| Hematocrit, % | 0.313 | 0.200 | ||||
| PP data | 32.9 ± 2.7 | 31.8 ± 2.8 | 32.8 ± 3.5 | 32.9 ± 4.2 | ||
| ITT data | 33.0 ± 2.8 | 31.8 ± 2.8 | 32.8 ± 3.4 | 32.9 ± 4.2 | ||
| ERI | 0.352 | 0.310 | ||||
| PP data | 11.77 ± 10.28 | 10.67 ± 9.75 | 8.08 ± 5.78 | 8.13 ± 6.29 | ||
| ITT data | 11.30 ± 10.10 | 10.00 ± 9.35 | 7.40 ± 5.60 | 7.87 ± 6.20 | ||
| Total protein, g/L | 0.048 | 0.853 | ||||
| PP data | 68.3 ± 5.5 | 69.5 ± 5.7 | 67.2 ± 5.0 | 68.2 ± 5.9 | ||
| ITT data | 68.3 ± 5.5 | 69.5 ± 5.7 | 67.6 ± 5.0 | 68.2 ± 5.9 | ||
| Albumin, g/L | 0.003 | 0.421 | ||||
| PP data | 39.08 ± 2.96 | 40.87 ± 4.94 | 39.97 ± 3.26 | 41.03 ± 4.29 | ||
| ITT data | 39.00 ± 2.90 | 40.87 ± 4.94 | 40.10 ± 3.30 | 41.03 ± 4.29 | ||
| Uric acid, umol/L | 0.069 | 0.333 | ||||
| PP data | 365 ± 67 | 339 ± 64 | 346 ± 67 | 338 ± 71 | ||
| ITT data | 364 ± 65 | 339 ± 64 | 345 ± 65 | 338 ± 71 | ||
| S-Creatinine, umol/L | 0.092 | 0.179 | ||||
| PP data | 872 ± 217 | 819 ± 247 | 860 ± 158 | 854 ± 159 | ||
| ITT data | 872 ± 211 | 819 ± 247 | 853 ± 154 | 854 ± 159 | ||
| S-Urea, mmol/L | 0.021 | 0.540 | ||||
| PP data | 23.2 ± 7.3 | 20.1 ± 5.8 | 22.7 ± 6.0 | 21.4 ± 6.2 | ||
| ITT data | 23.1 ± 7.1 | 20.1 ± 5.8 | 23.0 ± 6.0 | 21.4 ± 6.2 | ||
| Total Cholesterol, mmol/L | 0.361 | 0.986 | ||||
| PP data | 4.23 ± 1.00 | 4.20 ± 0.91 | 4.57 ± 0.87 | 4.50 ± 1.25 | ||
| ITT data | 4.25 ± 0.98 | 4.14 ± 0.91 | 4.54 ± 0.88 | 4.50 ± 1.25 | ||
| HDL-Cholesterol, mmol/L | 0.004 | 0.064 | ||||
| PP data | 1.09 ± 0.42 | 1.11 ± 0.50 | 0.99 ± 0.25 | 1.10 ± 0.28 | ||
| ITT data | 1.08 ± 0.41 | 1.11 ± 0.50 | 0.99 ± 0.24 | 1.10 ± 0.28 | ||
| LDL-Cholesterol, mmol/L | 0.553 | 0.641 | ||||
| PP data | 2.36 ± 0.76 | 2.26 ± 0.73 | 2.68 ± 0.80 | 2.67 ± 1.05 | ||
| ITT data | 2.38 ± 0.75 | 2.26 ± 0.73 | 2.67 ± 0.79 | 2.60 ± 1.06 | ||
| Triglycerides, mmol/L | 0.003 | 0.102 | ||||
| PP data | 1.80 ± 1.27 | 1.66 ± 1.14 | 2.28 ± 1.25 | 1.77 ± 0.74 | ||
| ITT data | 1.83 ± 1.24 | 1.66 ± 1.14 | 2.22 ± 1.22 | 1.77 ± 0.74 | ||
| S-Ca, mmol/L | 0.052 | 0.562 | ||||
| PP data | 2.27 ± 0.23 | 2.31 ± 0.19 | 2.30 ± 0.23 | 2.37 ± 0.27 | ||
| ITT data | 2.29 ± 0.24 | 2.31 ± 0.19 | 2.29 ± 0.23 | 2.37 ± 0.27 | ||
| S-PO4, mmol/L | 0.000 | 0.909 | ||||
| PP data | 1.61 ± 0.59 | 1.39 ± 0.51 | 1.82 ± 0.52 | 1.59 ± 0.50 | ||
| ITT data | 1.61 ± 0.57 | 1.39 ± 0.51 | 1.8 ± 0.51 | 1.59 ± 0.50 | ||
| Serum bicarbonate, mmol/L | 0.009 | 0.664 | ||||
| PP data | 20.32 ± 2.47 | 21.55 ± 1.48 | 20.60 ± 4.63 | 21.49 ± 3.00 | ||
| ITT data | 20.31 ± 2.40 | 21.55 ± 1.48 | 13.01 ± 3.82 | 21.49 ± 3.00 | ||
| Kt/V | 0.044 | 0.567 | ||||
| PP data | 1.32 ± 0.29 | 1.39 ± 0.33 | 1.35 ± 0.31 | 1.39 ± 0.25 | ||
| ITT data | 1.32 ± 0.31 | 1.39 ± 0.33 | 1.35 ± 0.30 | 1.39 ± 0.25 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Djuric, P.; Suvakov, S.; Simic, T.; Markovic, D.; Jerotic, D.; Jankovic, A.; Bulatovic, A.; Tosic Dragovic, J.; Damjanovic, T.; Marinkovic, J.; et al. Vitamin E-Bonded Membranes Do Not Influence Markers of Oxidative Stress in Hemodialysis Patients with Homozygous Glutathione Transferase M1 Gene Deletion. Toxins 2020, 12, 352. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12060352
Djuric P, Suvakov S, Simic T, Markovic D, Jerotic D, Jankovic A, Bulatovic A, Tosic Dragovic J, Damjanovic T, Marinkovic J, et al. Vitamin E-Bonded Membranes Do Not Influence Markers of Oxidative Stress in Hemodialysis Patients with Homozygous Glutathione Transferase M1 Gene Deletion. Toxins. 2020; 12(6):352. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12060352
Chicago/Turabian StyleDjuric, Petar, Sonja Suvakov, Tatjana Simic, Dragana Markovic, Djurdja Jerotic, Aleksandar Jankovic, Ana Bulatovic, Jelena Tosic Dragovic, Tatjana Damjanovic, Jelena Marinkovic, and et al. 2020. "Vitamin E-Bonded Membranes Do Not Influence Markers of Oxidative Stress in Hemodialysis Patients with Homozygous Glutathione Transferase M1 Gene Deletion" Toxins 12, no. 6: 352. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12060352