Wound Infections of Snakebites from the Venomous Protobothrops mucrosquamatus and Viridovipera stejnegeri in Taiwan: Bacteriology, Antibiotic Susceptibility, and Predicting the Need for Antibiotics—A BITE Study

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Patients’ Characteristics
2.2. Bacteriology and the Possible Influence of Prophylactic Antibiotics
2.3. Antibiotic Susceptibility
2.4. Use of Prophylactic Antibiotics
2.5. Antibiotic Therapy for Infected Snakebite Wounds
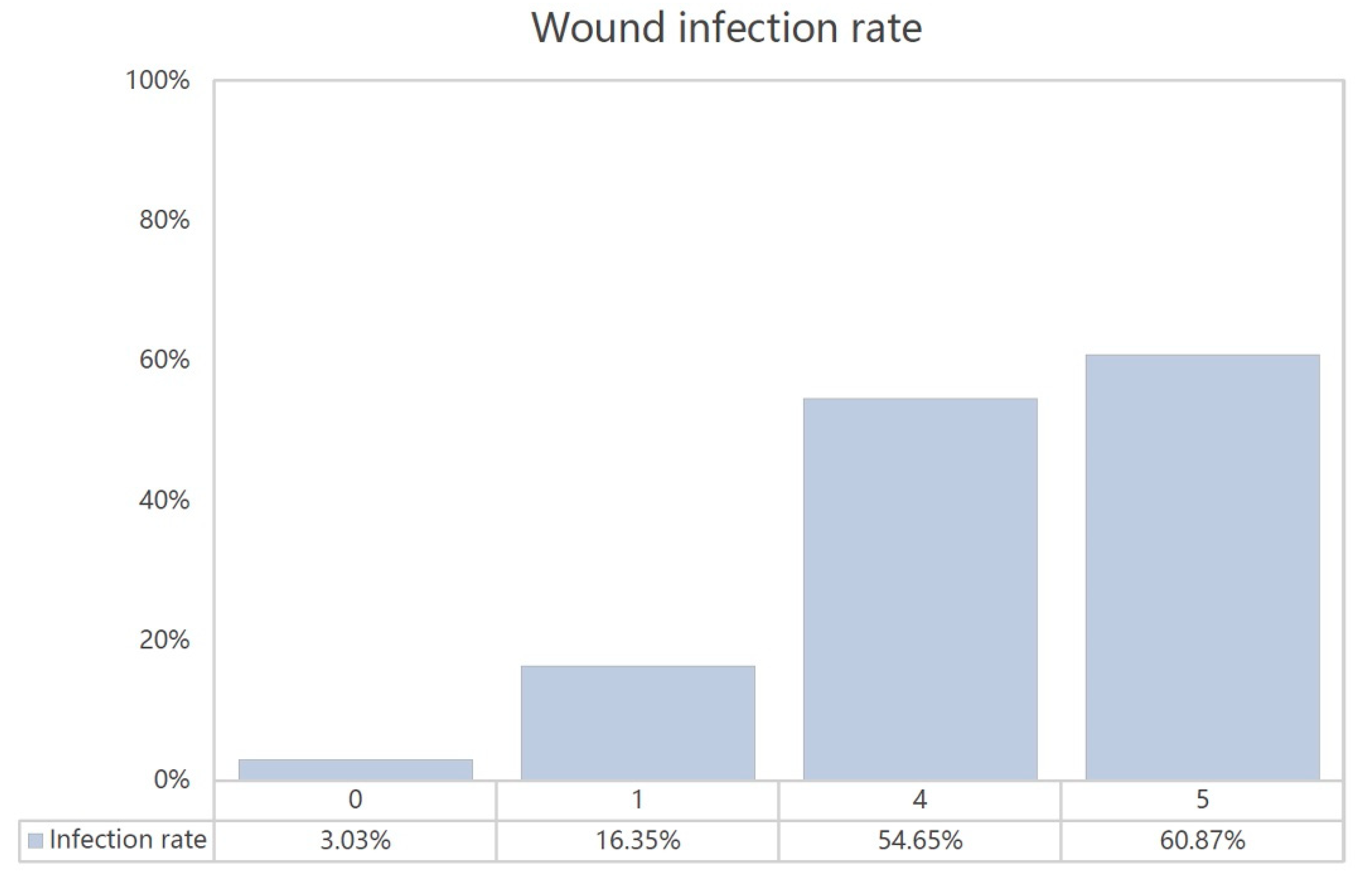
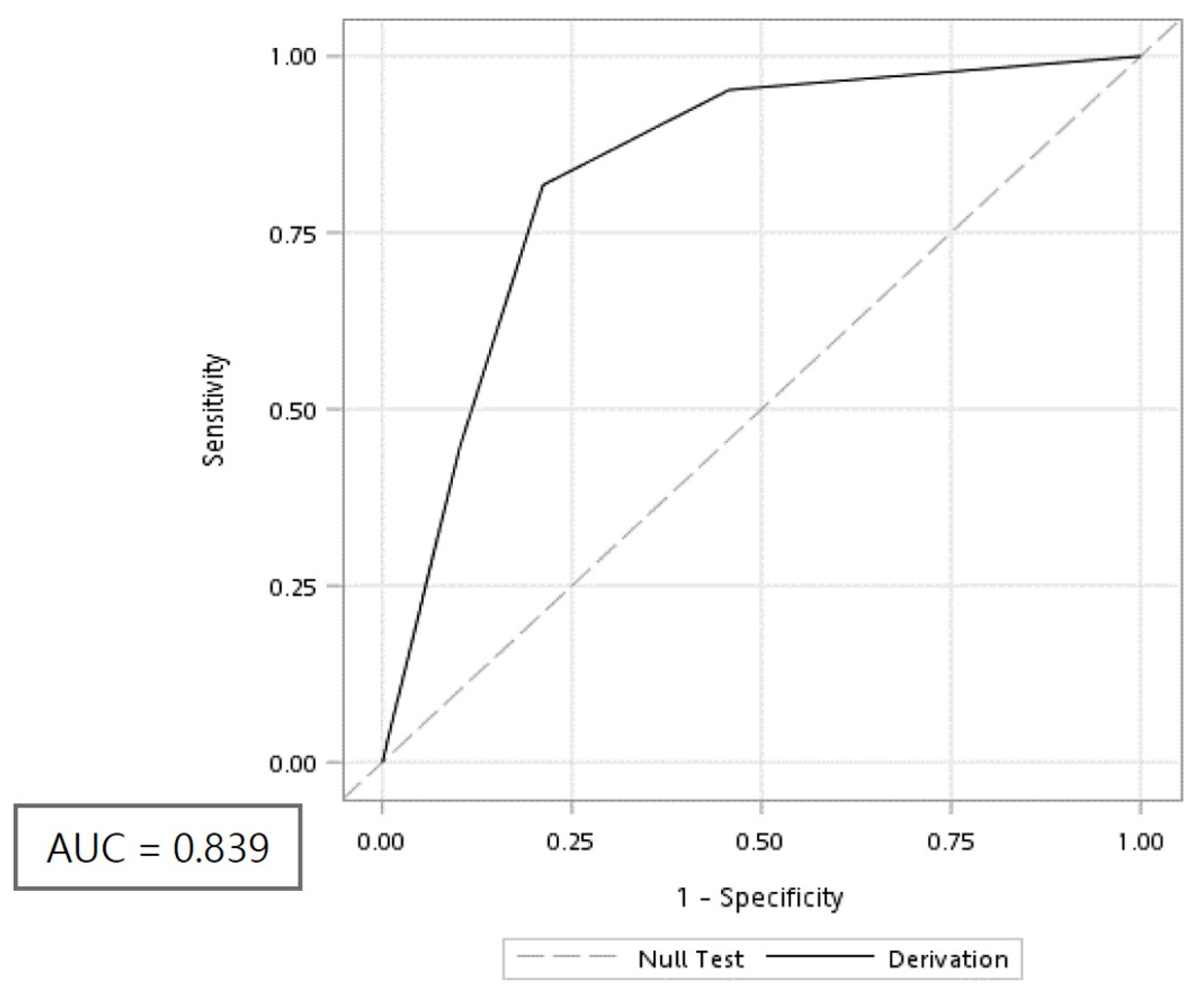
2.6. Development of the BITE Score
3. Discussion
3.1. Association of Polymicrobial Infection, Snake Oral Cavity Bacteriology, and Venom Effect on Tissue
3.2. Antibiotic Therapy in Infected Snakebite Wounds
3.3. Factors Associated with a Secondary Bacterial Infection from Taiwan Habu and Green Bamboo Viper Snakebites
3.4. Utility of the BITE Score
3.5. Limitations
4. Conclusions
5. Materials and Methods
5.1. Ethics Statement
5.2. Data Resources and Setting
5.3. Enrolment of Patients
5.4. Management Protocol for Patients Presenting with Snakebites
5.5. Definition of Wound Infection
5.6. Statistical Analysis and Development of the BITE Score
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chen, C.K.; Lin, C.C.; Shih, F.Y.; Chaou, C.H.; Lin, J.C.C.; Lai, T.I.; Tseng, C.Y.; Fang, C.C. Population-based study of venomous snakebite in Taiwan. J. Acute Med. 2015, 5, 38–42. [Google Scholar] [CrossRef]
- Tu, T.M. Statistical studies on victims of poisonous snakebites in Formosa. J. Formos. Med. Assoc. 1941, 40, 1477–1824. [Google Scholar]
- Sawai, Y.; Tseng, C.S. Snakebites on Taiwan. Snake 1969, 1, 9–18. [Google Scholar]
- Blaylock, R.S. Antibiotic use and infection in snakebite victims. S. Afr. Med. J. 1999, 89, 874–876. [Google Scholar]
- Lin, C.C.; Chaou, C.H.; Tseng, C.Y. An investigation of snakebite antivenom usage in Taiwan. J. Formos. Med. Assoc. 2016, 115, 672–677. [Google Scholar] [CrossRef] [Green Version]
- Huang, R.J.; Liau, M.Y.; Chen, S.W.; Chen, C.K. Preparation of highly potent hemorrhagic antivenin. Chin. Med. J. 1986, 37, 410–415. [Google Scholar]
- Liau, M.Y.; Huang, R.J. Toxoids and Antivenoms of Venomous Snakes in Taiwan. J. Toxicol. Toxin Rev. 1997, 16, 163–175. [Google Scholar]
- Chen, Y.W.; Chen, M.H.; Chen, Y.C.; Hung, D.Z.; Chen, C.K.; Yen, D.H.; Huang, C.I.; Lee, C.H.; Wang, L.M.; Yang, C.C. Differences in clinical profiles of patients with Protobothrops mucrosquamatus and Viridovipera stejnegeri envenoming in Taiwan. Am. J. Trop. Med. Hyg. 2009, 80, 28–32. [Google Scholar] [CrossRef]
- Huang, L.W.; Wang, J.D.; Huang, J.A.; Hu, S.Y.; Wang, L.M.; Tsan, Y.T. Wound infections secondary to snakebite in central Taiwan. J. Venom. Anim. Toxinsincl Trop. 2012, 18, 272–276. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, Y.H.; Hsueh, J.H.; Liu, W.C.; Yang, K.C.; Hsu, K.C.; Lin, C.T.; Ho, Y.Y.; Chen, L.W. Contributing factors for complications and outcomes in patients with snakebite: Experience in a medical center in southern Taiwan. Ann. Plast. Surg. 2017, 78, S32–S36. [Google Scholar] [CrossRef]
- Chen, C.M.; Wu, K.G.; Chen, C.J.; Wang, C.M. Bacterial infection in association with snakebite: A 10-year experience in a northern Taiwan medical center. J. Microbiol. Immunol. Infect. 2011, 44, 456–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.T.; Lin, C.Y.; Chen, Y.H.; Hsueh, P.R. Update on infections caused by Stenotrophomonas maltophilia with particular attention to resistance mechanisms and therapeutic options. Front. Microbiol. 2015, 6, 893–912. [Google Scholar] [CrossRef] [PubMed]
- Rupp, M.E.; Soper, D.E.; Archer, G.L. Colonization of the female genital tract with Staphylococcus saprophyticus. J. Clin. Microbiol. 1992, 30, 2975–2979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- May, A.K. Skin and soft tissue infections: The new surgical infection society guidelines. Surg. Infect. 2011, 12, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Jorge, M.T.; Ribeiro, L.A. Infections in the bite site after envenoming by snakes of the Bothrops genus. J. Venom. Anim. Toxins 1997, 3, 264–272. [Google Scholar] [CrossRef]
- Jorge, M.T.; Nishioka, S.d.A.; Oliveirá, R.B.d.; Ribeiro, L.A.; Silveira, P.V. Aeromonas hydrophila soft-tissue infection as a complication of snake bite: Report of three cases. Ann. Trop. Med. Parasitol. 1998, 92, 213–217. [Google Scholar] [CrossRef]
- Jorge, M.T.; Ribeiro, L.A.; Silva, M.L.D.; Kusano, E.J.; Mendonça, J.S.D. Microbiological studies of abscesses complicating Bothrops snakebite in humans: A prospective study. Toxicon 1994, 32, 743–748. [Google Scholar] [CrossRef]
- Shek, K.C.; Tsui, K.L.; Lam, K.K.; Crow, P.; Ng, K.H.; Ades, G.; Yip, K.T.; Grioni, A.; Tan, K.S.; Lung, D.C.; et al. Oral bacterial flora of the Chinese cobra (Naja atra) and bamboo pit viper (Trimeresurus albolabris) in Hong Kong SAR, China. Hong Kong Med. J. 2009, 15, 183–190. [Google Scholar]
- Shaikh, I.K.; Dixit, P.P.; Pawade, B.S.; Potnis-Lele, M.; Kurhe, B.P. Assessment of cultivable oral bacterial flora from important venomous snakes of india and their antibiotic susceptibilities. Curr. Microbiol. 2017, 74, 1278–1286. [Google Scholar] [CrossRef]
- Liu, C.C.; Lin, C.C.; Hsiao, Y.C.; Wang, P.J.; Yu, J.S. Proteomic characterization of six Taiwanese snake venoms: Identification of species-specific proteins and development of a SISCAPA-MRM assay for cobra venom factors. J. Proteom. 2018, 187, 59–68. [Google Scholar] [CrossRef]
- Gutiérrez, J.M.; Lomonte, B. Phospholipases A2: Unveiling the secrets of a functionally versatile group of snake venom toxins. Toxicon 2013, 62, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Sachett, J.A.G.; Silva, I.M.d.; Alves, E.C.; Oliveira, S.S.; Sampaio, V.S.; Vale, F.F.d.; Romero, G.A.S.; Santos, M.C.D.; Marques, H.O.; Colombini, M.; et al. Poor efficacy of preemptive amoxicillin clavulanate for preventing secondary infection from Bothrops snakebites in the Brazilian Amazon: A randomized controlled clinical trial. PLoS Negl. Trop. Dis. 2017, 11, e0005745. [Google Scholar] [CrossRef] [PubMed]
- Zahorec, R. Ratio of neutrophil to lymphocyte counts--rapid and simple parameter of systemic inflammation and stress in critically ill. Bratisl. Lek. Listy 2001, 102, 5–14. [Google Scholar] [PubMed]
- Hajibandeh, S.; Hajibandeh, S.; Hobbs, N.; Mansour, M. Neutrophil-to-lymphocyte ratio predicts acute appendicitis and distinguishes between complicated and uncomplicated appendicitis: A systematic review and meta-analysis. Am. J. Surg. 2020, 219, 154–163. [Google Scholar] [CrossRef] [Green Version]
- Honda, T.; Uehara, T.; Matsumoto, G.; Arai, S.; Sugano, M. Neutrophil left shift and white blood cell count as markers of bacterial infection. Clin. Chim. Acta 2016, 457, 46–53. [Google Scholar] [CrossRef]
- Bucaretchi, F.; Herrera, S.R.; Hyslop, S.; Baracat, E.C.; Vieira, R.J. Snakebites by Bothrops spp. in children in Campinas, São Paulo, Brazil. Rev. Inst. Med. Trop. Sao Paulo 2001, 43, 329–333. [Google Scholar] [CrossRef]
- Resiere, D.; Mehdaoui, H.; Névière, R.; Olive, C.; Severyns, M.; Beaudoin, A.; Florentin, J.; Brouste, Y.; Banydeen, R.; Cabié, A.; et al. Infectious complications following snakebite by bothrops lanceolatus in martinique: A case series. Am. J. Trop. Med. Hyg. 2020, 102, 232–240. [Google Scholar] [CrossRef]
- Mao, Y.C.; Hung, D.Z. Management of Snake Envenomation in Taiwan. In Clinical Toxinology in Asia Pacific and Africa, 1st ed.; Gopalakrishnakone, P., Faiz, A., Fernando, R., Gnanathasan, C., Habib, A., Yang, C.C., Eds.; Springer: Dordrecht, The Netherlands, 2015; Volume 2, pp. 23–52. [Google Scholar]
- Goldstein, E.J.; Citron, D.M.; Gonzalez, H.; Russell, F.E.; Finegold, S.M. Bacteriology of rattlesnake venom and implications for therapy. J. Infect. Dis. 1997, 140, 818–821. [Google Scholar] [CrossRef]
- Theakston, R.D.; Phillips, R.E.; Looareesuwan, S.; Echeverria, P.; Makin, T.; Warrell, D.A. Bacteriological studies of the venom and mouth cavities of wild Malayan pit vipers (Calloselasma rhodostoma) in southern Thailand. Trans. R. Soc. Trop. Med. Hyg. 1990, 84, 875–879. [Google Scholar] [CrossRef]
- Terry, P.; Mackway-Jones, K. Towards evidence based emergency medicine: Best BETs from the Manchester Royal Infirmary. The use of antibiotics in venomous snake bite. Emerg. Med. J. 2002, 19, 48–49. [Google Scholar] [CrossRef]
- Jorge, M.T.; Malaque, C.; Ribeiro, L.A.; Fan, H.W.; Cardoso, J.L.; Nishioka, S.A.; Sano-Martins, I.S.; França, F.O.; Kamiguti, A.S.; Theakston, R.D.; et al. Failure of chloramphenicol prophylaxis to reduce the frequency of abscess formation as a complication of envenoming by Bothrops snakes in Brazil: A double-blind randomized controlled trial. Trans. R. Soc. Trop. Med. Hyg. 2004, 98, 529–534. [Google Scholar] [CrossRef]
- Kularatne, S.A.; Kumarasiri, P.V.; Pushpakumara, S.K.; Dissanayaka, W.P.; Ariyasena, H.; Gawarammana, I.B.; Senanayake, N. Routine antibiotic therapy in the management of the local inflammatory swelling in venomous snakebites: Results of a placebo-controlled study. Ceylon Med. J. 2005, 50, 151–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, Y.C.; Liu, P.Y.; Hung, D.Z.; Lai, W.C.; Huang, S.T.; Hung, Y.M.; Yang, C.C. Bacteriology of Naja atra Snakebite Wound and Its Implications for Antibiotic Therapy. Am. J. Trop. Med. Hyg. 2016, 94, 1129–1135. [Google Scholar] [CrossRef] [PubMed]
- Kasturiratne, A.; Wickremasinghe, A.R.; Silva, N.D.; Gunawardena, N.K.; Pathmeswaran, A.; Premaratna, R.; Savioli, L.; Lalloo, D.G.; Silva, H.J.D. The global burden of snakebite: A literature analysis and modelling based on regional estimates of envenoming and deaths. PLoS Med. 2008, 5, e218. [Google Scholar] [CrossRef]
- Tsai, M.; Lin, M.H.; Lee, C.P.; Yang, Y.; Chen, W.C.; Chang, G.H.; Tsai, Y.T.; Chen, P.C.; Tsai, Y.H. Chang Gung research database: A multi-institutional database consisting of original medical records. Biomed. J. 2017, 40, 263–269. [Google Scholar] [CrossRef]
- Chang Gung Memorial Hospital. Available online: http://www.chang-gung.com/en/m/about.aspx?id=11&bid=1 (accessed on 29 August 2020).
- Lipsky, B.A.; Berendt, A.R.; Cornia, P.B.; Pile, J.C.; Peters, E.J.; Armstrong, D.G.; Deery, H.G.; Embil, J.M.; Joseph, W.S.; Karchmer, A.W.; et al. Infectious diseases society of america. 2012 infectious diseases society of america clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin. Infect. Dis. 2012, 54, e132–e173. [Google Scholar] [CrossRef] [Green Version]
- WHO/Regional Office for South-East Asia. Guidelines for the Management of Snakebites, 2nd ed.; Warrell, D., Ed.; SEARO Publications: New Delhi, India, 2016; ISBN 9789290225300. Available online: https://www.who.int/snakebites/resources/9789290225300/en/ (accessed on 29 August 2020).



{kind=link}
{kind=link}
| Variable | Patients | p-Value | |
|---|---|---|---|
| No Wound Infection (n = 563) | Wound Infection (n = 163) | ||
| Demographic Characteristics | |||
| Age | 51.88 (17.42) | 52.76 (18.04) | 0.57 |
| Male, n (%) | 400 (71.05) | 106 (65.03) | 0.17 |
| Laboratory Variables # | |||
| WBC (1000/μL) * | 8.15 (3.59) | 9.47 (3.97) | 0.0008 |
| Band | 0.07 (0.72) | 0.11 (0.74) | 0.58 |
| Segment * | 62.26 (14.03) | 67.54 (14.33) | 0.0003 |
| Lymphocyte * | 29.59 (12.43) | 24.63 (12.53) | 0.0001 |
| Neutrophil/lymphocyte ratio * | 3.26 (3.63) | 4.56 (5.19) | 0.01 |
| Hb (g/dL) | 14.35 (1.66) | 14.08 (1.74) | 0.11 |
| RDW | 18.38 (11.18) | 18.98 (11.70) | 0.60 |
| PLT (1000/μL) | 211.60 (61.00) | 214.50 (62.75) | 0.63 |
| Prothrombin time | 11.69 (7.11) | 11.37 (3.15) | 0.49 |
| APTT | 28.16 (7.14) | 27.38 (3.59) | 0.11 |
| Cr (mg/dL) | 0.93 (0.57) | 0.94 (0.97) | 0.90 |
| BUN (mg/dL) | 14.98 (8.20) | 14.72 (6.99) | 0.80 |
| ALT/GPT (U/L) | 27.44 (29.31) | 23.42 (12.87) | 0.06 |
| AST/GOT | 33.17 (36.37) | 40.49 (59.34) | 0.39 |
| Creatine kinase | 388.00 (520.50) | 1201.40 (3895.60) | 0.24 |
| Myoglobin | 168.90 (417.30) | 245.20 (770.40) | 0.49 |
| K (mEq/L) | 3.74 (0.38) | 3.78 (0.43) | 0.45 |
| Na (mEq/L) * | 140.00 (2.11) | 139.10 (2.51) | 0.0022 |
| Glucose (mg/dL) | 130.60 (47.57) | 144.00 (53.49) | 0.11 |
| Treatment Modalities | |||
| Antivenin dose (vial) &* | 2 (1–3) | 2 (1–4) | <0.0001 |
| Prophylactic antibiotics * | 215 (38.6) | 106 (62.72) | <0.0001 |
| Hospitalization | |||
| Hospital admission, n (%) * | 98 (17.41) | 132 (80.98) | <0.0001 |
| Length of hospitalization (day) * | 4.87 (3.50) | 9.50 (8.04) | <0.0001 |
| No. | Microorganism | Suggested Antibiotic Sensitivity | |||
|---|---|---|---|---|---|
| Aerobic Gram-Positive | Aerobic Gram-Negative | Anaerobic | |||
| 1 | Enterococcus faecalis | Morganella morganii | Bacteroides fragilis | Ampicillin | Clindamycin |
| 2 | Enterococcus faecalis | Morganella morganii | Ampicillin | ||
| Aeromonas hydrophila | Ceftriaxone | ||||
| 3 | Enterococcus faecalis | Morganella morganii | Ampicillin | ||
| 4 | Corynebacterium jeikeium | Enterobacter cloacae CR strain | Fluoroquinolone | ||
| 5 | Coagulase negative Staphylococcus | Vancomycin | |||
| 6 | Viridans streptococcus | Oxacillin | |||
| Staphylococcus aureus | Vancomycin | ||||
| Staphylococcus saprophyticus | Stenotrophomonas maltophilia | Enterobacter cloacae | Fluoroquinolone | ||
| Peptostreptococcus micros | |||||
| 7 | Staphylococcus aureus | Oxacillin | |||
| Corynebacterium jeikeium | Fluoroquinolone | ||||
| Corynebacterium spp. | |||||
| Variable | β | Odds Ratio | 95% Confidence Interval | Points ※ |
|---|---|---|---|---|
| Intercept | −1.06 | |||
| WBC (1000/μL) × neutrophil-lymphocyte ratio ≥ 19.84 | 0.37 | 2.112 | (1.289, 3.462) | 1 |
| Admission | 1.38 | 15.65 | (9.27, 26.42) | 4 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-C.; Chen, Y.-C.; Goh, Z.N.L.; Seak, C.-K.; Seak, J.C.-Y.; Shi-Ying, G.; Seak, C.-J.; SPOT Investigators. Wound Infections of Snakebites from the Venomous Protobothrops mucrosquamatus and Viridovipera stejnegeri in Taiwan: Bacteriology, Antibiotic Susceptibility, and Predicting the Need for Antibiotics—A BITE Study. Toxins 2020, 12, 575. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12090575
Lin C-C, Chen Y-C, Goh ZNL, Seak C-K, Seak JC-Y, Shi-Ying G, Seak C-J, SPOT Investigators. Wound Infections of Snakebites from the Venomous Protobothrops mucrosquamatus and Viridovipera stejnegeri in Taiwan: Bacteriology, Antibiotic Susceptibility, and Predicting the Need for Antibiotics—A BITE Study. Toxins. 2020; 12(9):575. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12090575
Chicago/Turabian StyleLin, Chih-Chuan, Yen-Chia Chen, Zhong Ning Leonard Goh, Chen-Ken Seak, Joanna Chen-Yeen Seak, Gao Shi-Ying, Chen-June Seak, and SPOT Investigators. 2020. "Wound Infections of Snakebites from the Venomous Protobothrops mucrosquamatus and Viridovipera stejnegeri in Taiwan: Bacteriology, Antibiotic Susceptibility, and Predicting the Need for Antibiotics—A BITE Study" Toxins 12, no. 9: 575. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12090575