Pain Reduction in Adults with Limb Spasticity Following Treatment with IncobotulinumtoxinA: A Pooled Analysis

 , and
, and
Abstract
:1. Introduction
2. Results
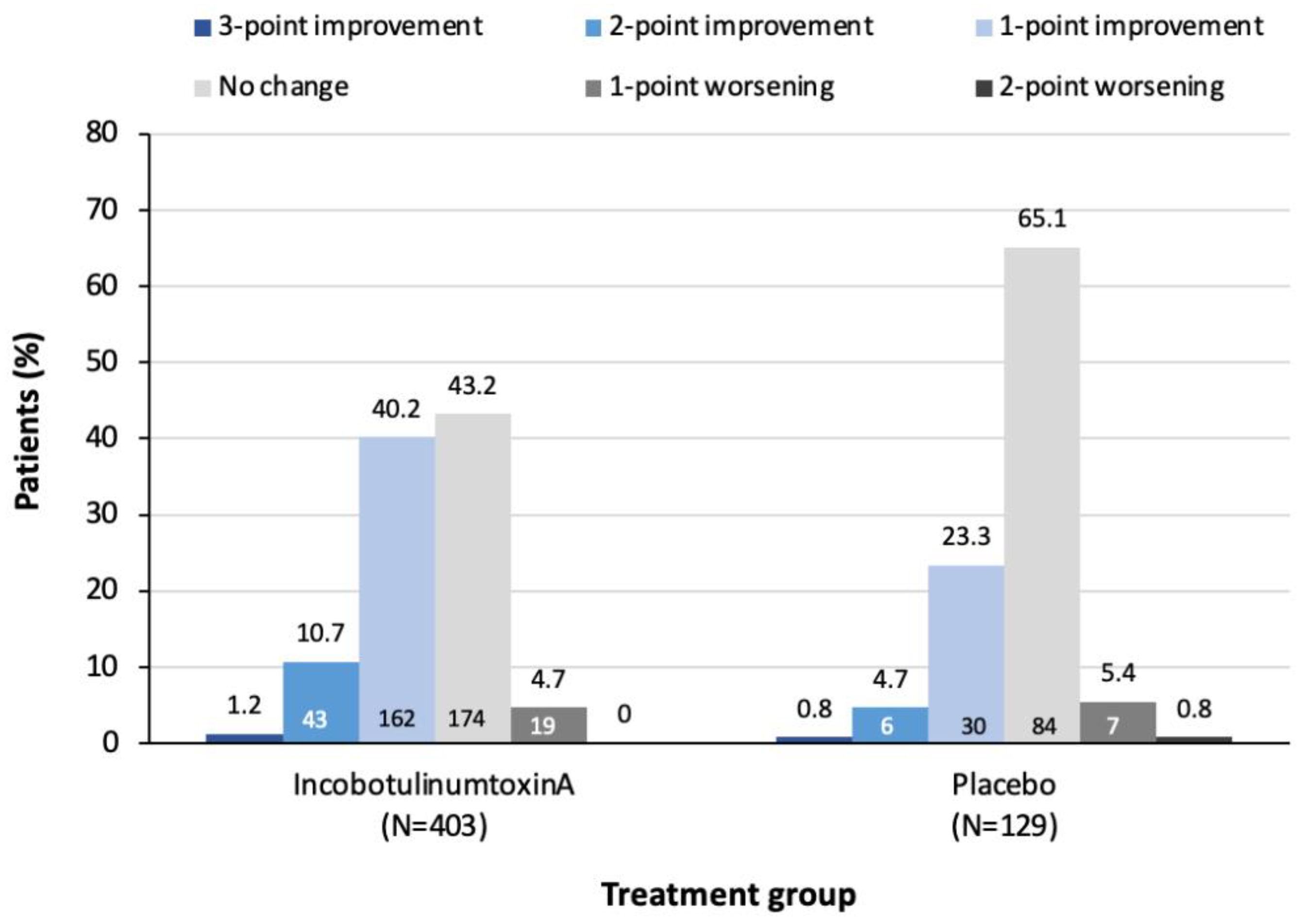
2.1. Frequency of Change in DAS Pain Score at Week 4
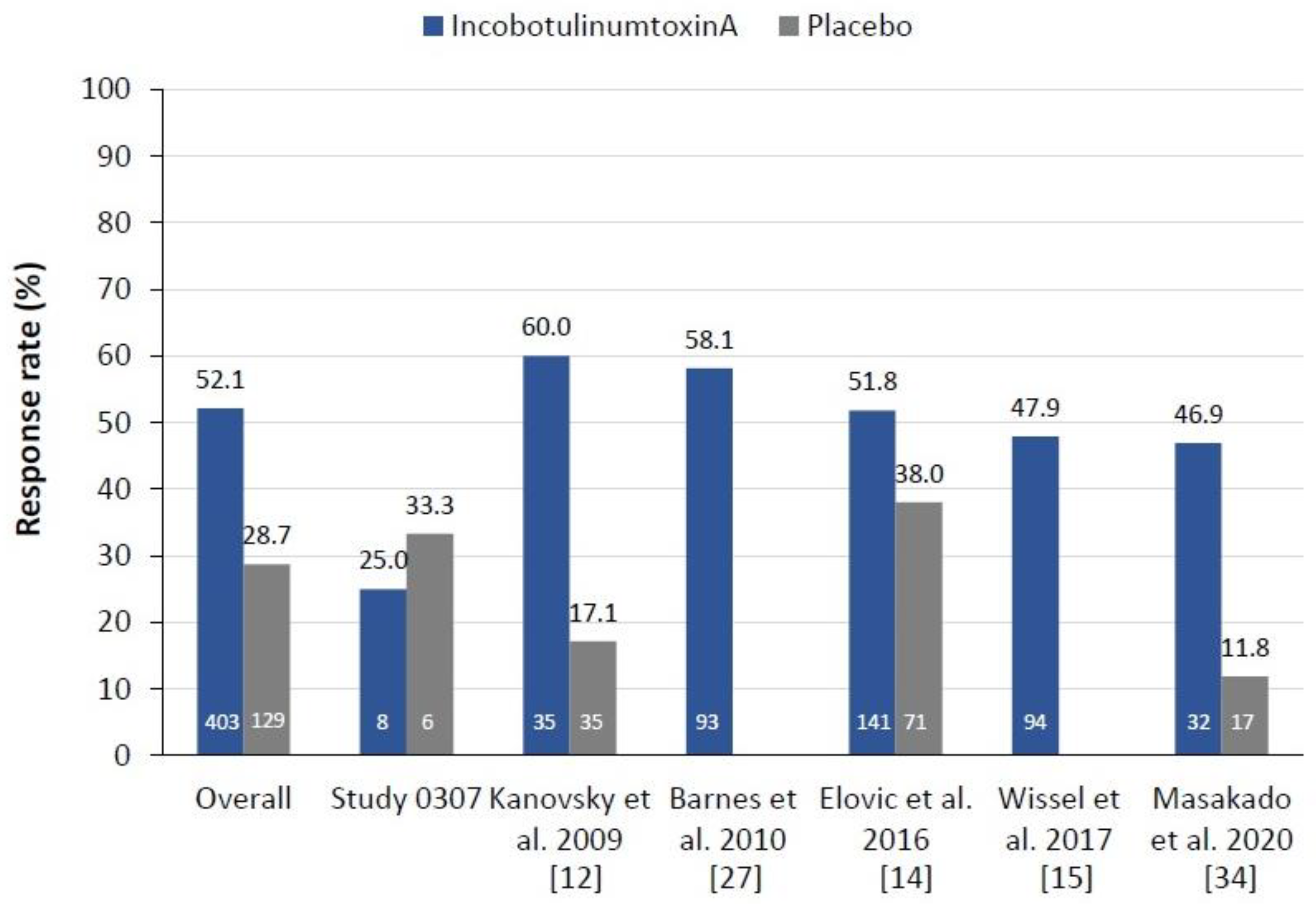
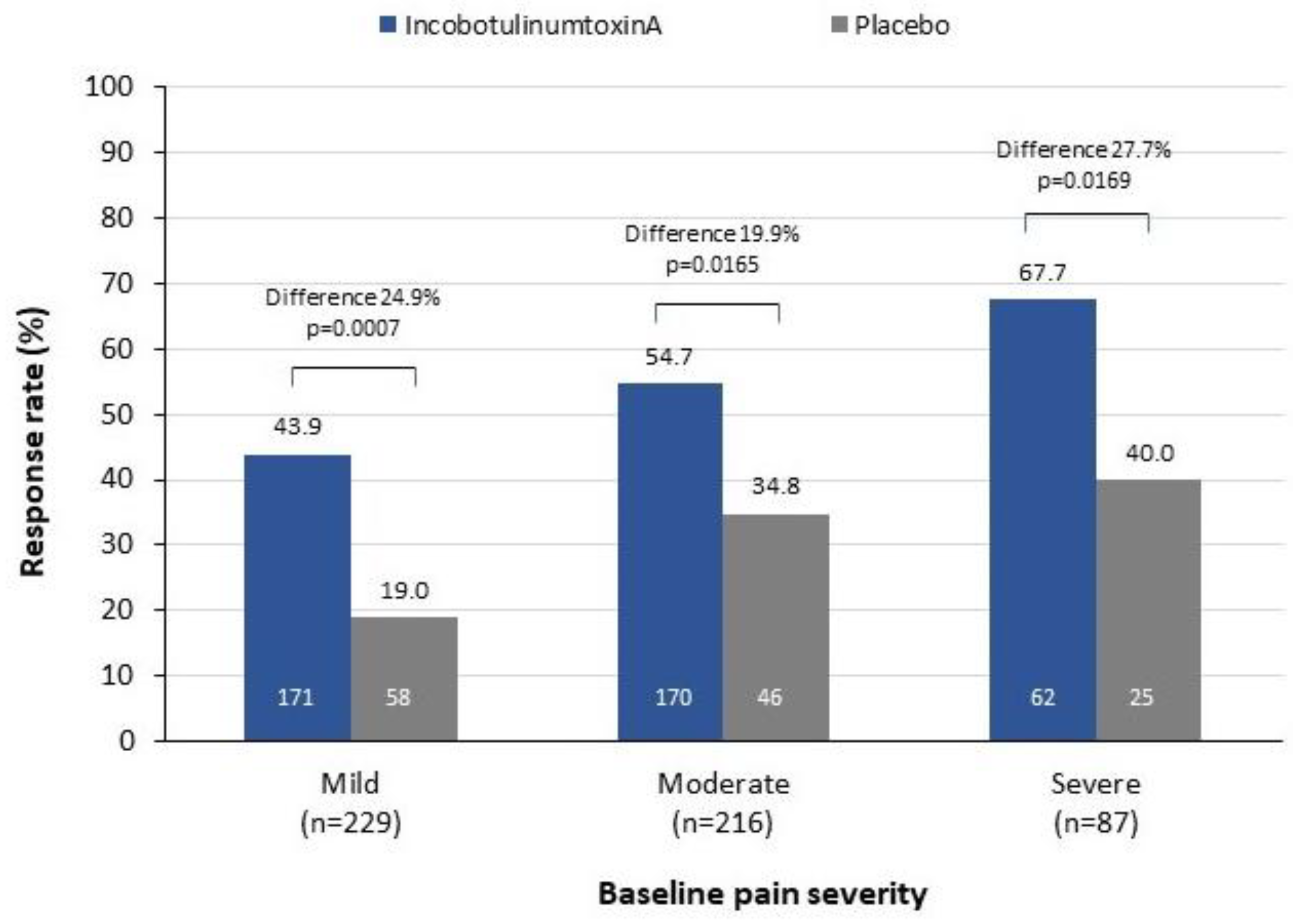
2.2. Pain Response Rates at Week 4
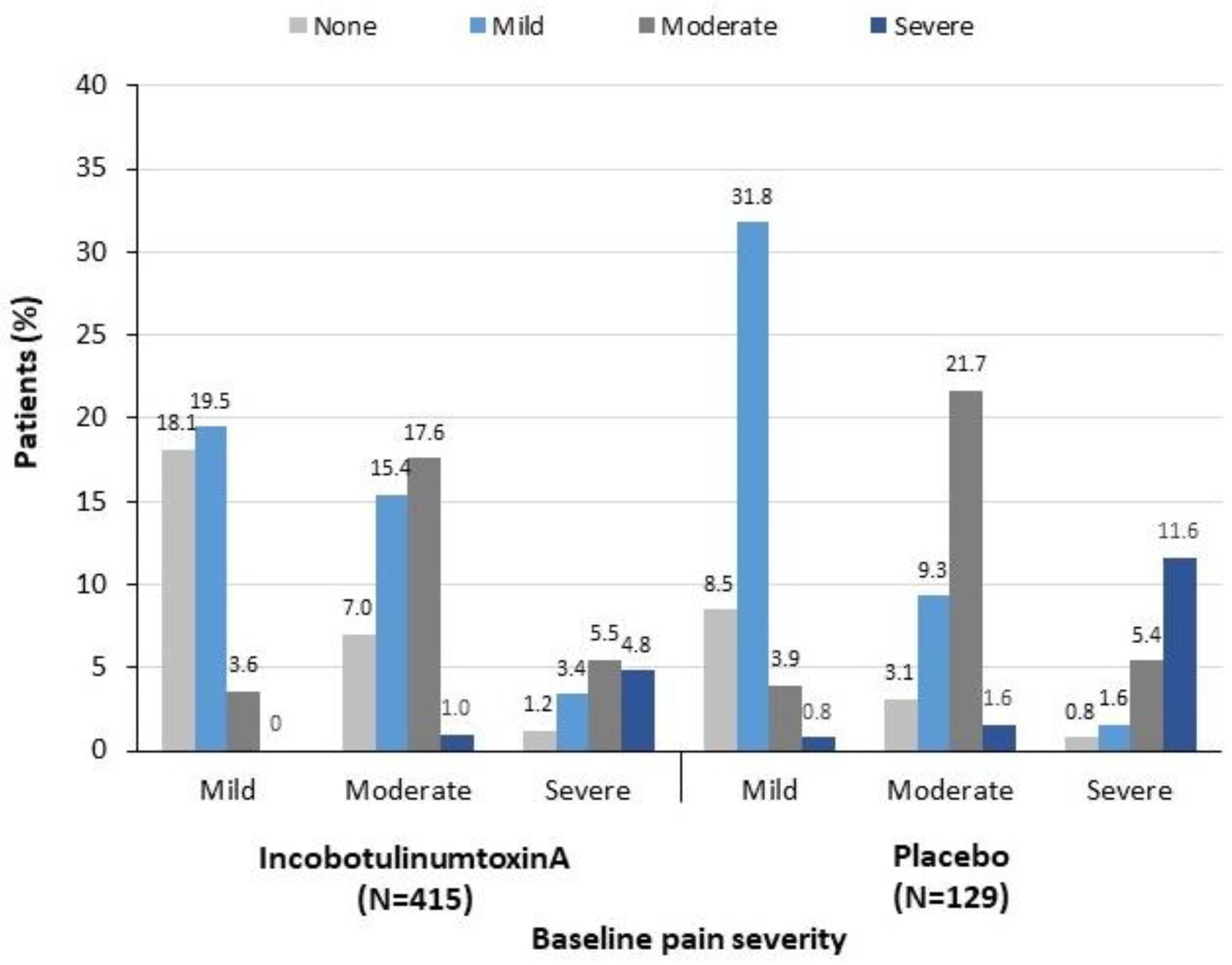
2.3. Change in Pain Severity from Baseline to Week 4
2.4. Complete Pain Relief at Week 4
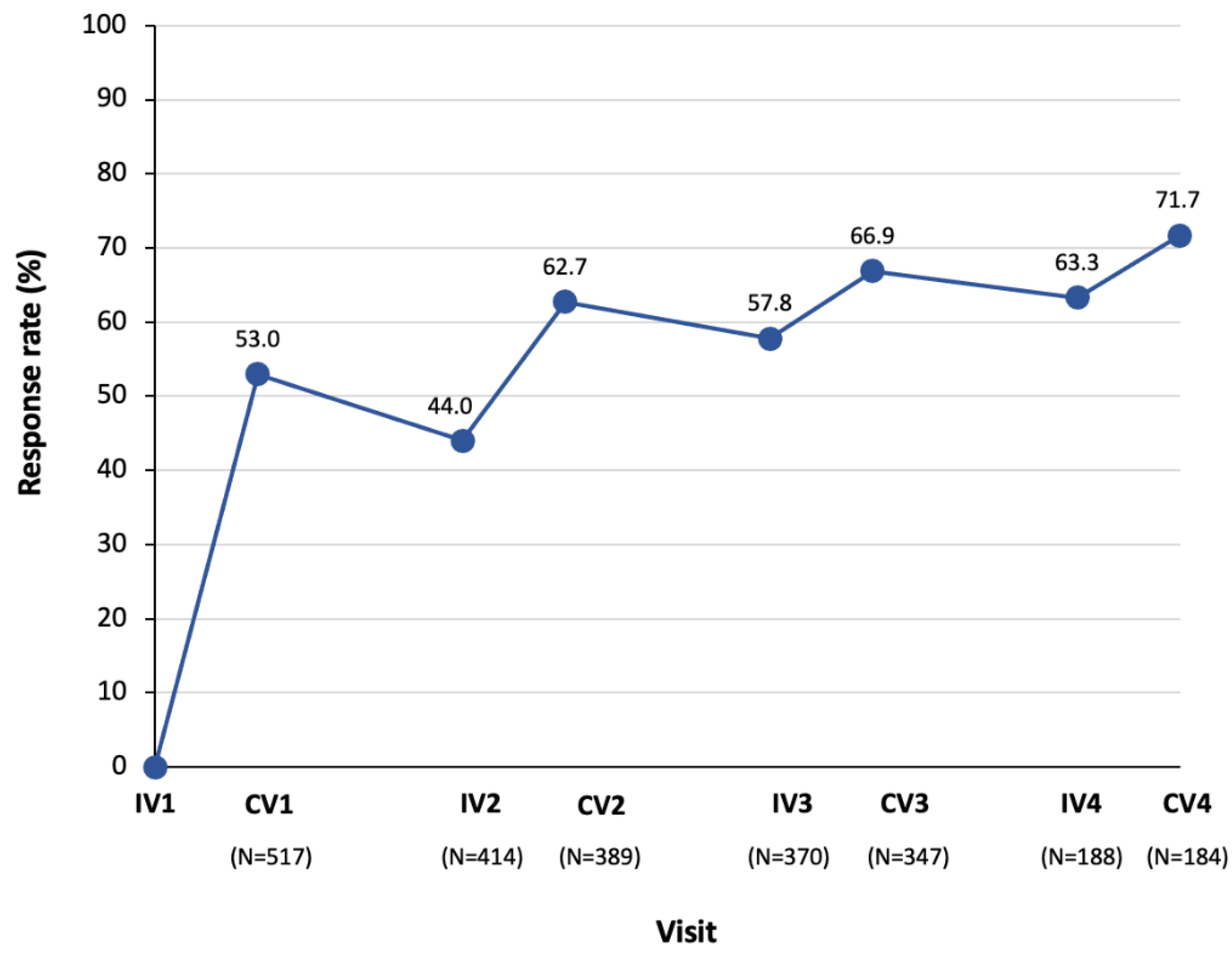
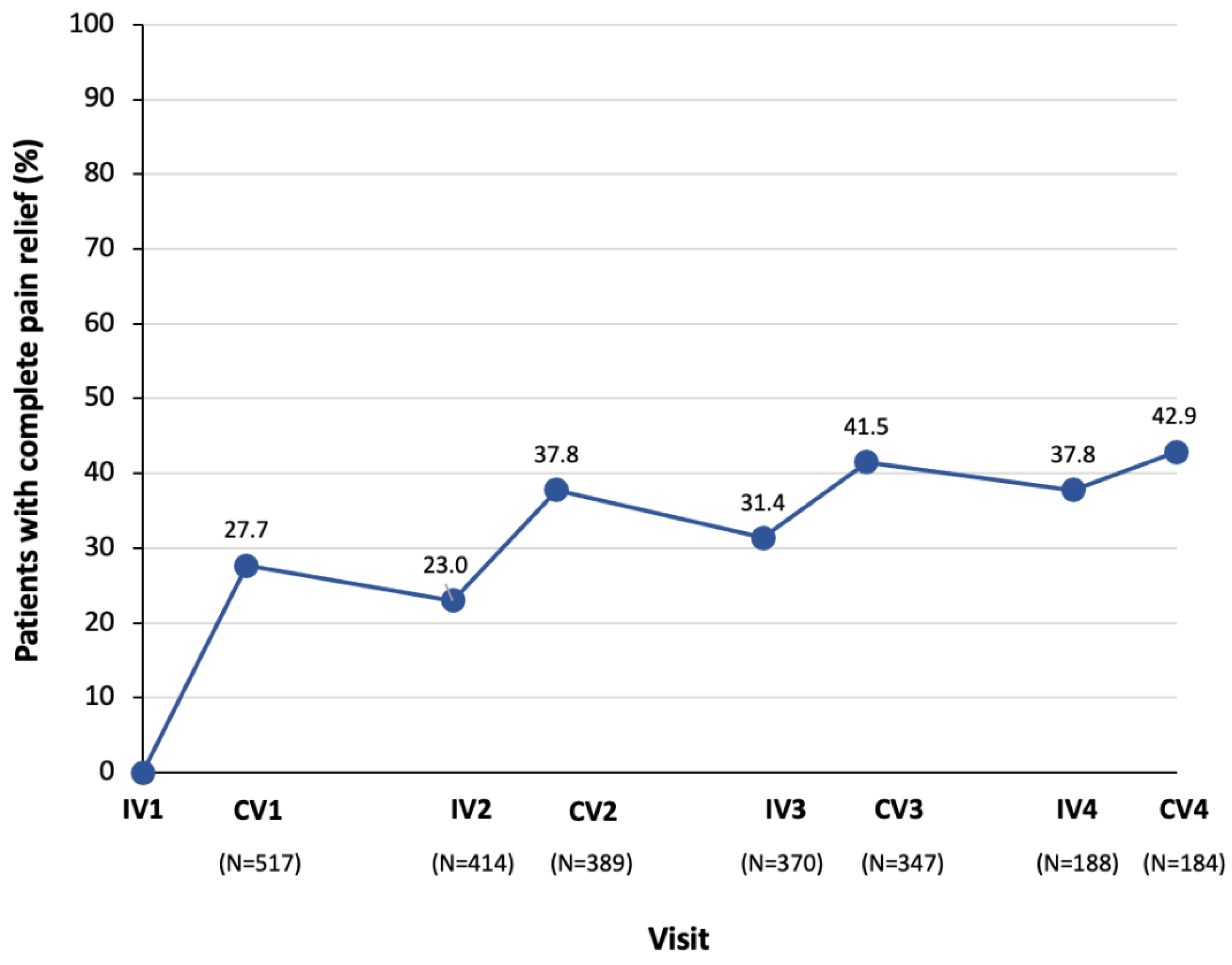
2.5. Pain Response Rates and Proportion with Complete Pain Relief Following Multiple Injection Cycles
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Studies Included in the Analyses
5.2. Analyses
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Doan, Q.V.; Brashear, A.; Gillard, P.J.; Varon, S.F.; Vandenburgh, A.M.; Turkel, C.C.; Elovic, E.P. Relationship between disability and health-related quality of life and caregiver burden in patients with upper limb poststroke spasticity. PM R 2012, 4, 4–10. [Google Scholar] [CrossRef]
- Martin, A.; Abogunrin, S.; Kurth, H.; Dinet, J. Epidemiological, humanistic, and economic burden of illness of lower limb spasticity in adults: A systematic review. Neuropsychiatr. Dis. Treat. 2014, 10, 111–122. [Google Scholar] [CrossRef] [Green Version]
- Gillard, P.J.; Sucharew, H.; Kleindorfer, D.; Belagaje, S.; Varon, S.; Alwell, K.; Moomaw, C.J.; Woo, D.; Khatri, P.; Flaherty, M.L.; et al. The negative impact of spasticity on the health-related quality of life of stroke survivors: A longitudinal cohort study. Health Qual. Life Outcomes 2015, 13, 159. [Google Scholar] [CrossRef] [Green Version]
- Wissel, J.; Ward, A.B.; Erztgaard, P.; Bensmail, D.; Hecht, M.J.; Lejeune, T.M.; Schnider, P.; Altavista, M.C.; Cavazza, S.; Deltombe, T.; et al. European consensus table on the use of botulinum toxin type A in adult spasticity. J. Rehabil. Med. 2009, 41, 13–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esquenazi, A.; Novak, I.; Sheean, G.; Singer, B.J.; Ward, A.B. International consensus statement for the use of botulinum toxin treatment in adults and children with neurological impairments-introduction. Eur. J. Neurol. 2010, 17 (Suppl. 2), 1–8. [Google Scholar] [CrossRef]
- Chang, E.; Ghosh, N.; Yanni, D.; Lee, S.; Alexandru, D.; Mozaffar, T. A review of spasticity treatments: Pharmacological and interventional approaches. Crit. Rev. Phys. Rehabil. Med. 2013, 25, 11–22. [Google Scholar] [CrossRef] [Green Version]
- Simpson, D.M.; Hallett, M.; Ashman, E.J.; Comella, C.L.; Green, M.W.; Gronseth, G.S.; Armstrong, M.J.; Gloss, D.; Potrebic, S.; Jancovic, J.; et al. Practice guideline update summary: Botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2016, 86, 1818–1826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Royal College of Physicians; British Society of Rehabilitation Medicine; Chartered Society of Physiotherapy; Association of Chartered Physiotherapists in Neurology; Royal College of Occupational Therapists. Spasticity in Adults: Management Using Botulinum Toxin. National Guidelines. 2018. Available online: https://www.rcplondon.ac.uk/guidelines-policy/spasticity-adults-management-using-botulinum-toxin (accessed on 15 March 2021).
- Fitterer, J.W.; Picelli, A.; Winston, P. A novel approach to new-onset hemiplegic shoulder pain with decreased range of motion using targeted diagnostic nerve blocks: The ViVe algorithm. Front. Neurol. 2021, 12, 731. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, P.; Jansen, A.; Lee, J.I.; Moll, M.; Ringelstein, M.; Rosenthal, D.; Bigalke, H.; Aktas, O.; Hartung, H.P.; Hefter, H. High prevalence of neutralizing antibodies after long-term botulinum neurotoxin therapy. Neurology 2019, 92, e48–e54. [Google Scholar] [CrossRef]
- Walter, U.; Mühlenhoff, C.; Benecke, R.; Dressler, D.; Mix, E.; Alt, J.; Wittstock, M.; Dudesek, A.; Storch, A.; Kamm, C. Frequency and risk factors of antibody-induced secondary failure of botulinum neurotoxin therapy. Neurology 2020, 94, e2109–e2120. [Google Scholar] [CrossRef]
- Kañovský, P.; Slawek, J.; Denes, Z.; Platz, T.; Sassin, I.; Comes, G.; Grafe, S. Efficacy and safety of botulinum neurotoxin NT 201 in poststroke upper limb spasticity. Clin. Neuropharm. 2009, 32, 259–265. [Google Scholar] [CrossRef]
- Kañovský, P.; Slawek, J.; Denes, Z.; Platz, T.; Comes, G.; Grafe, S.; Pulte, I. Efficacy and safety of treatment with incobotulinum toxin A (botulinum neurotoxin type A free from complexing proteins.; NT 201) in post-stroke upper limb spasticity. J. Rehabil. Med. 2011, 43, 486–492. [Google Scholar] [CrossRef] [Green Version]
- Elovic, E.P.; Munin, M.C.; Kañovský, P.; Hanschmann, A.; Hiersemenzel, R.; Marciniak, C. Randomized, placebo-controlled trial of incobotulinumtoxinA for upper-limb post-stroke spasticity. Muscle Nerve 2016, 53, 415–421. [Google Scholar] [CrossRef]
- Wissel, J.; Bensmail, D.; Ferreira, J.J.; Molteni, F.; Satkunam, L.; Moraleda, S.; Rekand, T.; McGuire, J.; Scheschonka, A.; Flatau-Baqué, A.; et al. Safety and efficacy of incobotulinumtoxinA doses up to 800 U in limb spasticity. The TOWER study. Neurology 2017, 88, 1321–1328. [Google Scholar] [CrossRef] [Green Version]
- Bensmail, D.; Wissel, J.; Laffont, I.; Simon, O.; Scheschonka, A.; Flatau-Baqué, B.; Dressler, D.; Simpson, D.M. Efficacy of incobotulinumtoxinA for the treatment of adult lower-limb post-stroke spasticity, including pes equinovarus. Ann. Phys. Rehabil. Med. 2020, 64, 101376. [Google Scholar] [CrossRef]
- Fheodoroff, K.; Rekand, T.; Medeiros, L.; Kossmehl, P.; Wissel, J.; Bensmail, D.; Scheschonka, A.; Flatau-Baqué, B.; Simon, O.; Dressler, D.; et al. Quality of life in subjects with upper- and lower-limb spasticity treated with incobotulinumtoxinA. Health Qual. Life Outcomes 2020, 18, 51. [Google Scholar] [CrossRef] [Green Version]
- Marciniak, C.; Munin, M.C.; Brashear, A.; Rubin, B.S.; Patel, A.T.; Slawek, J.; Hanschmann, A.; Hiersemenzel, R.; Elovic, E.P. IncobotulinumtoxinA treatment in upper-limb post-stroke spasticity in the open-label extension period of PURE: Efficacy in passive function, caregiver burden and quality of life. PM R 2020, 12, 491–499. [Google Scholar] [CrossRef]
- Shaikh, A.; Phadke, C.P.; Ismail, F.; Boulias, C. Relationship between botulinum toxin, spasticity, and pain: A survey of patient perception. Can. J. Neurol. Sci. 2016, 43, 311–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wissel, J.; Ganapathy, V.; Ward, A.B.; Borg, J.; Ertzgaard, P.; Herrmann, C.; Haggstrom, A.; Sakel, M.; Ma, J.; Dimitrova, A.; et al. OnabotulinumtoxinA improves pain in patients with post-stroke spasticity: Findings from a randomized, double-blind, placebo-controlled trial. J. Pain Symptom. Manage. 2016, 52, 17–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lejeune, T.; Khatkova, S.; Turner-Stokes, L.; Picaut, P.; Maisonobe, P.; Balcaitiene, J.; Boyer, F.C. AbotulinumtoxinA injections in shoulder muscles to improve adult upper limb spasticity: Results from a phase 4 real-world study and a phase 3 open-label trial. J. Rehabil. Med. 2020, 52, jrm00068. [Google Scholar] [CrossRef] [PubMed]
- Wissel, J.; Müller, J.; Dressnandt, J.; Heinen, F.; Naumann, M.; Topka, H.; Poewe, W. Management of spasticity associated pain with botulinum toxin A. J. Pain Symptom. Manag. 2000, 20, 44–49. [Google Scholar] [CrossRef]
- Esquenazi, A.; Mayer, N.; Lee, S.; Brashear, A.; Elovic, E.; Francisco, G.E.; Yablon, S.; PROS Study Group. Patient registry of outcomes in spasticity care. Am. J. Phys. Med. Rehabil. 2012, 91, 729–746. [Google Scholar] [CrossRef]
- Marciniak, C.M.; Harvey, R.L.; Gagnon, C.M.; Duraski, S.A.; Denby, F.A.; McCarty, S.; Bravi, L.A.; Polo, K.M.; Fierstein, K.M. Does botulinum toxin type A decrease pain and lessen disability in hemiplegic survivors of stroke with shoulder pain and spasticity? A randomized, double-blind, placebo-controlled trial. Am. J. Phys. Med. Rehabil. 2012, 91, 1007–1019. [Google Scholar] [CrossRef]
- De Icco, R.; Perrotta, A.; Berra, E.; Allena, M.; Alfonsi, E.; Tamburin, S.; Serrao, M.; Sandrini, G.; Tassorelli, C. Onabotulinum-toxinA reduces temporal pain processing at spinal level in patients with lower limb spasticity. Toxins 2019, 11, 359. [Google Scholar] [CrossRef] [Green Version]
- Slawek, J.; Bogucki, A.; Reclawowicz, D. Botulinum toxin type A for upper limb spasticity following stroke: An open-label study with individualised, flexible injection regimens. Neurol. Sci. 2005, 26, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Barnes, M.; Schnitzler, A.; Medeiros, L.; Aguilar, M.; Lehnert-Batar, A.; Minnasch, P. Efficacy and safety of NT 201 for upper limb spasticity of various etiologies—A randomized parallel-group study. Acta Neurol. Scand. 2010, 122, 295–302. [Google Scholar] [CrossRef]
- Dunne, J.W.; Gracies, J.M.; Hayes, M.; Zeman, B.; Singer, B.J.; Multicentre Study Group. A prospective, multicentre, randomized, double-blind, placebo-controlled trial of onabotulinumtoxinA to treat plantarflexor/invertor overactivity after stroke. Clin. Rehabil. 2012, 26, 787–797. [Google Scholar] [CrossRef] [PubMed]
- Rousseaux, M.; Daveluy, W.; Kozlowski, O.; Allart, E. Onabotulinumtoxin-A injection for disabling lower limb flexion in hemiplegic patients. NeuroRehabilitation 2014, 35, 25–30. [Google Scholar] [CrossRef]
- Gracies, J.M.; Brashear, A.; Jech, R.; McAllister, P.; Banach, M.; Valkovic, P.; Walker, H.; Marciniak, C.; Deltombe, T.; Skoromets, A.; et al. Safety and efficacy of abobotulinumtoxinA for hemiparesis in adults with upper limb spasticity after stroke or traumatic brain injury: A double-blind randomised controlled trial. Lancet Neurol. 2015, 14, 992–1001. [Google Scholar] [CrossRef]
- Fujimura, K.; Kagaya, H.; Onaka, H.; Okochi, Y.; Yamada, M.; Teranishi, T.; Kanada, Y.; Saitoh, E. Improvement in Disability Assessment Scale after botulinum toxin A treatment for upper limb spasticity. Jpn. J. Compr. Rehabil. Sci. 2017, 8, 4–9. [Google Scholar] [CrossRef]
- Rosales, R.L.; Balcaitiene, J.; Berard, H.; Maisonobe, P.; Goh, K.J.; Kumthornthip, W.; Mazlam, M.; Latif, L.A.; Delos Santos, M.M.D.; Chotiyarnwong, C.; et al. Early abobotulinumtoxinA (Dysport®) in post-stroke adult upper limb spasticity: ONTIME pilot study. Toxins 2018, 10, 253. [Google Scholar] [CrossRef] [Green Version]
- Wein, T.; Esquenazi, A.; Jost, W.H.; Ward, A.B.; Pan, G.; Dimitrova, R. OnabotulinumtoxinA for the treatment of poststroke distal lower limb spasticity: A randomized trial. PM R 2018, 10, 693–703. [Google Scholar] [CrossRef]
- Masakado, Y.; Abo, M.; Kondo, K.; Saeki, S.; Saitoh, E.; Dekundy, A.; Hanschmann, A.; Kaji, R.; J-PURE Study Group. Efficacy and safety of incobotulinumtoxinA in post-stroke upper-limb spasticity in Japanese subjects: Results from a randomized, double-blind, placebo-controlled study (J-PURE). J. Neurol. 2020, 267, 2029–2041. [Google Scholar] [CrossRef] [Green Version]
- Wissel, J.; Bensmail, D.; Scheschonka, A.; Flatau-Baqué, B.; Simon, O.; Althaus, M.; Simpson, D.M. Post hoc analysis of the improvement in shoulder spasticity and safety observed following treatment with incobotulinumtoxinA. J. Rehabil. Med. 2020, 52, jrm00028. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.A.; Pereira, G. The efficacy of botulinum toxin A for spasticity and pain in adults: A systematic review and meta-analysis using the Grades of Recommendation, Assessment, Development and Evaluation approach. Clin. Rehabil. 2013, 27, 1084–1096. [Google Scholar] [CrossRef] [PubMed]
- Jia, S.; Liu, Y.; Shen, L.; Liang, X.; Xu, X.; Wei, Y. Botulinum toxin type A for upper limb spasticity in poststroke patients: A meta-analysis of randomized controlled trials. J. Stroke Cerebrovasc. Dis. 2020, 29, 104682. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, L.; DeBeer, H.; et al. GRADE guidelines:1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Turner-Stokes, L.; Jacinto, J.; Fheodoroff, K.; Brashear, A.; Maisonobe, P.; Lysandropoulos, A.; Ashford, S.; Upper Limb International Spasticity-III (ULIS-III) Study Group. Assessing the effectiveness of upper-limb spasticity management using a structured approach to goal-setting and outcome measurement: First cycle results from the ULIS-III Study. J. Rehabil. Med. 2021, 53, jrm00133. [Google Scholar] [CrossRef]
- Turner-Stokes, L.; Jacinto, J.; Fheodoroff, K.; Brashear, A.; Maisonobe, P.; Lysandropoulos, A.; Ashford, S.; Upper Limb International Spasticity (ULIS-III) Study Group. Longitudinal goal attainment with integrated upper limb spasticity management including repeat injections of botulinum toxin A: Findings from the prospective, observational Upper Limb International Spasticity (ULIS-III) cohort study. J. Rehabil. Med. 2021, 53, jrm00157. [Google Scholar] [CrossRef] [PubMed]
- Marque, P.; Denis, A.; Gasq, D.; Chaleat-Valayer, E.; Yelnik, A.; Colin, C.; Botuloscope Group; Pérennou, D. Botuloscope: 1-year follow-up of upper limb post-stroke spasticity treated with botulinum toxin. Ann. Phys. Rehabil. Med. 2019, 62, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Geister, T.L.; Bushnell, D.M.; Yang, J.; Zhnag, Y.; Martin, M.L.; Heilbronn, A.; Liu, Z. Initial psychometric validation of the questionnaire on pain caused by spasticity (QPS). Health Qual. Life Outcomes 2017, 15, 229. [Google Scholar] [CrossRef] [Green Version]
- Brashear, A.; Zafonte, R.; Corcoran, M.; Galvez-Jiminez, N.; Gracies, J.M.; Gordon, M.F.; McAfee, A.; Ruffing, K.; Thompson, B.; Williams, M.; et al. Inter- and intrarater reliability of the Ashworth Scale and the Disability Assessment Scale in patients with upper-limb post-stroke spasticity. Arch. Phys. Med. Rehabil. 2002, 83, 1349–1354. [Google Scholar] [CrossRef] [PubMed]
- Harrison, R.A.; Field, T.S. Post stroke pain: Identification, assessment, and therapy. Cerebrovasc. Dis. 2015, 39, 190–201. [Google Scholar] [CrossRef]
- Magrinelli, F.; Zanette, G.; Tamburin, S. Neuropathic pain: Diagnosis and treatment. Pract. Neurol. 2013, 13, 292–307. [Google Scholar] [CrossRef] [PubMed]
- Intiso, D.; Basciani, M.; Santamato, A.; Intiso, M.; Di Rienzo, F. Botulinum toxin type A for the treatment of neuropathic pain in neuro-rehabilitation. Toxins 2015, 7, 2454–2480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matak, I.; Bölcskei, K.; Bach-Rojecky, L.; Helyes, Z. Mechanisms of botulinum toxin type A action on pain. Toxins 2019, 11, 459. [Google Scholar] [CrossRef] [Green Version]
- Pirazzini, M.; Rossetto, O.; Eleopra, R.; Montecucco, C. Botulinum neurotoxins: Biology, pharmacology, and toxicology. Pharmacol. Rev. 2017, 69, 200–235. [Google Scholar] [CrossRef] [PubMed]
- Shin, M.C.; Wakita, M.; Xie, D.J.; Yamaga, T.; Iwata, S.; Torii, Y.; Harakawa, T.; Ginnaga, A.; Kozaki, S.; Akaike, N. Inhibition of membrane Na+ channels by A type botulinum toxin at femtomolar concentrations in central and peripheral neurons. J. Pharmacol. Sci. 2012, 118, 33–42. [Google Scholar] [CrossRef] [Green Version]
- Colloca, L.; Ludman, T.; Bouhassira, D.; Baron, R.; Dickenson, A.H.; Yarnitsky, D.; Freeman, R.; Tuini, A.; Attal, N.; Finnerup, N.B.; et al. Neuropathic pain. Nat. Rev. Dis. Primers 2017, 16, 17002. [Google Scholar] [CrossRef] [Green Version]
- Atzeni, F.; Masala, I.F.; Sarzi-Puttini, P. A review of chronic musculoskeletal pain: Central and peripheral effects of diclofenac. Pain Ther. 2018, 7, 163–177. [Google Scholar] [CrossRef] [Green Version]
- Volkow, N.; Benveniste, H.; McLellan, A.T. Use and misuse of opioids in chronic pain. Annu. Rev. Med. 2018, 69, 451–465. [Google Scholar] [CrossRef] [Green Version]
- Crombez, G.; Eccleston, C.; van Damme, S.; Vlaeyen, J.W.S.; Karoly, P. Fear-avoidance model of chronic pain: The next generation. Clin. J. Pain 2012, 28, 475–483. [Google Scholar] [CrossRef] [Green Version]
- Sturgeon, J.A.; Zautra, A.J.; Arewasikporn, A. A multilevel structural equation modeling analysis of vulnerabilities and resilience resources influencing affective adaptation to chronic pain. Pain 2014, 155, 292–298. [Google Scholar] [CrossRef] [Green Version]
- Borsook, D.; Youssef, A.M.; Simons, L.; Elman, I.; Eccleston, C. When pain gets stuck: The evolution of pain chronification and treatment resistance. Pain 2018, 159, 2421–2436. [Google Scholar] [CrossRef] [PubMed]
- Turner-Stokes, L.; Fhedoroff, K.; Jacinto, J.; Maisonobe, P.; Ashford, S. ULIS (Upper Limb International Spasticity), a 10-year odyssey. An international, multicentric, longitudinal cohort of person-centered spasticity management in real-life practice. J. Int. Soc. Phys. Rehabil. Med. 2019, 2, 138–150. [Google Scholar] [CrossRef]
- Ashworth, B. Preliminary trial of carisoprodol in multiple sclerosis. Practitioner 1964, 192, 540–542. [Google Scholar] [PubMed]
- Bohannon, R.W.; Smith, M.B. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys. Ther. 1987, 67, 206–207. [Google Scholar] [CrossRef] [PubMed]
- Marciniak, C.; Munin, M.C.; Brashear, A.; Rubin, B.S.; Patel, A.T.; Slawek, J.; Hanschmann, A.; Hiersemenzel, R.; Elovic, E.P. IncobotulinumtoxinA efficacy and safety in adults with upper-limb spasticity following stroke: Results from the open-label extension period of a phase 3 study. Adv. Ther. 2019, 36, 187–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brashear, A.; Gordon, M.F.; Elovic, E.; Kassicieh, D.; Marciniak, C.; Do, M.; Lee, C.-H.; Jenkins, S.; Turkel, C.; Botox Post-Stroke Spasticity Study Group. Intramuscular injection of botulinum toxin for the treatment of wrist and finger spasticity after a stroke. N. Engl. J. Med. 2002, 347, 395–400. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | IncobotulinumtoxinA (N = 415) | Placebo (N = 129) | Total (N = 544) |
|---|---|---|---|
| Age (years) | 56.5 ± 12.9 | 56.2 ± 10.6 | 56.4 ± 12.4 |
| Age group | |||
| 18–50 years | 124 (29.9) | 38 (29.5) | 162 (29.8) |
| 51–65 years | 180 (43.4) | 64 (49.6) | 244 (44.9) |
| ≥66 years | 111 (26.8) | 27 (20.9) | 138 (25.4) |
| Male | 249 (60.0) | 80 (62.0) | 329 (60.5) |
| Ethnicity | |||
| White | 324 (78.1) | 99 (76.7) | 423 (77.8) |
| Asian | 57 (13.7) | 29 (22.5) | 86 (15.8) |
| Black or African American | 9 (2.2) | 1 (0.8) | 10 (1.8) |
| Other | 4 (1.0) | 0 | 4 (0.7) |
| Missing | 21 (5.1) | 0 | 21 (3.9) |
| Height (cm) | 167.8 ± 9.4 a | 168.8 ± 8.3 | 168.0 ± 9.1 |
| Weight (kg) | 75.7 ± 15.0 b | 74.5 ± 15.4 | 75.4 ± 15.1 |
| Duration of spasticity (time since diagnosis, years) | 5.4 ± 6.7 c | 3.3 ± 4.8 | 4.9 ± 6.3 |
| Aetiology of spasticity | |||
| Stroke | 389 (93.7) | 128 (99.2) | 517 (95.0) |
| Brain injury | 10 (2.4) | 0 | 10 (1.8) |
| Infantile cerebral palsy | 5 (1.2) | 0 | 5 (0.9) |
| Multiple sclerosis | 0 | 1 (0.8) | 1 (0.2) |
| Other | 11 (2.7) | 0 | 11 (2.0) |
| Baseline DAS pain score | |||
| 1 = Mild | 177 (42.7) | 58 (45.0) | 235 (43.2) |
| 2 = Moderate | 175 (42.2) | 46 (35.7) | 221 (40.6) |
| 3 = Severe | 63 (15.2) | 25 (19.4) | 88 (16.2) |
| BoNT-A naïve | 202 (48.7) | 94 (72.9) | 296 (54.4) |
| Patients taking concomitant pain-relieving medication | 81 (19.5) | 16 (12.4) | 97 (17.8) |
| Study Name, NCT Number and Reference(s) | Phase | Study Design and Objective | Patients and Indication | Treatments | Clinical Patterns Treated | Primary Outcome |
|---|---|---|---|---|---|---|
| MRZ_60201_0307 | 2 | Prospective, randomised, double-blind, placebo-controlled, parallel-group, multicentre pilot study (12 weeks) to investigate the efficacy and safety of incobotulinumtoxinA in the treatment of pain in upper limb spasticity | N = 14 adults with pain caused by upper limb spasticity due to multiple aetiologies a | (1) IncobotulinumtoxinA, up to 400 U (2) Placebo | Flexed elbow Clenched fist Flexed wrist Thumb in palm Pronated forearm Adducted/ internally rotated shoulder Intrinsic plus hand | Mean evening pain intensity measured using the 11-point box scale b |
| MRZ_60201_0410 NCT00432666 Kanovsky et al. 2009 [12] Kanovsky et al. 2011 [13] | 3 | Prospective, randomised, double-blind, placebo-controlled, parallel-group, multicentre trial (20 weeks) with an open-label extension period (69 weeks) to investigate the efficacy and safety of incobotulinumtoxinA in the treatment of post-stroke upper limb spasticity | N = 148 adults with post-stroke upper limb spasticity | (1) IncobotulinumtoxinA, 170–400 U (2) Placebo | Flexed elbow Clenched fist Flexed wrist Thumb in palm Pronated forearm | Muscle tone response rate (≥1-point improvement in Ashworth Scale score) at Week 4 |
| MRZ_60201_0607 NCT00465738 Barnes et al. 2010 [27] | 3 | Prospective, randomised, observer-blind, parallel-group, multicentre trial (20 weeks) to assess the efficacy and safety of two different dilutions of incobotulinumtoxinA in patients with upper limb spasticity | N = 192 adults with stable upper limb spasticity of diverse aetiology | (1) IncobotulinumtoxinA, 400 U in 8 mL (2) IncobotulinumtoxinA, 400 U in 20 mL | Flexed elbow Clenched fist Flexed wrist Thumb in palm Pronated forearm Intrinsic plus hand | DAS response rate (≥1-point improvement) at Week 4 c |
| PURE MRZ_60201_SP3001 NCT01392300 Elovic et al. 2016 [14] Marciniak et al. 2019 [59] and 2020 [18] | 3 | Prospective, randomised, double-blind, placebo-controlled, parallel-group, multicentre study (12 weeks) with an open-label extension period (36 weeks) to investigate the efficacy and safety of incobotulinumtoxinA in the treatment of post-stroke upper limb spasticity | N = 317 adults with post-stroke upper limb spasticity | (1) IncobotulinumtoxinA, 400 U (2) Placebo | Flexed elbow Clenched fist Flexed wrist Thumb in palm Pronated forearm d | Change in muscle tone from baseline to Week 4, measured using the Ashworth Scale |
| TOWER MRZ_60201_3053 NCT01603459 Wissel et al. 2017 [15] | 3 | Prospective, non-randomised, open-label, single-arm, multicentre dose-titration study (48 weeks) to investigate the safety and efficacy of incobotulinumtoxinA in subjects requiring doses of 800 U during the course of the study for the treatment of upper and lower limb spasticity | N = 155 adults with chronic upper and lower limb spasticity of the same body side due to cerebral causes | (1) IncobotulinumtoxinA, 400 U (2) IncobotulinumtoxinA, 600 U (3) IncobotulinumtoxinA, 600–800 U | Upper limb Flexed elbow Clenched fist Flexed wrist Thumb in palm Pronated forearm Extended elbow Internally rotated/extended/adducted shoulder Lower limb Flexed hip Internally rotated hip | Safety |
| J-PURE MRZ_60201_3099 CTI-153029 (Japanese Clinical Trials Registry) Masakado et al. 2020 [34] | 3 | Prospective, randomised, double-blind, placebo-controlled, parallel-group, multicentre study (52 weeks in total), with an open-label lead-in tolerability period (1 week), a main study period (12 weeks) and an open-label extension period (32–40 weeks), to investigate the efficacy and safety of two different doses of incobotulinumtoxinA in the treatment of post-stroke upper limb spasticity | N = 111 adults with post-stroke upper limb spasticity | (1) IncobotulinumtoxinA, 400 U (2) Placebo, 400 U (3) IncobotulinumtoxinA, 250 U (4) Placebo, 250 U | Flexed elbow and pronated forearm Clenched fist Flexed wrist Thumb in palm | Change in muscle tone from baseline to Week 4, measured using the modified Ashworth Scale |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wissel, J.; Camões-Barbosa, A.; Comes, G.; Althaus, M.; Scheschonka, A.; Simpson, D.M. Pain Reduction in Adults with Limb Spasticity Following Treatment with IncobotulinumtoxinA: A Pooled Analysis. Toxins 2021, 13, 887. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13120887
Wissel J, Camões-Barbosa A, Comes G, Althaus M, Scheschonka A, Simpson DM. Pain Reduction in Adults with Limb Spasticity Following Treatment with IncobotulinumtoxinA: A Pooled Analysis. Toxins. 2021; 13(12):887. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13120887
Chicago/Turabian StyleWissel, Jörg, Alexandre Camões-Barbosa, Georg Comes, Michael Althaus, Astrid Scheschonka, and David M. Simpson. 2021. "Pain Reduction in Adults with Limb Spasticity Following Treatment with IncobotulinumtoxinA: A Pooled Analysis" Toxins 13, no. 12: 887. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13120887