
Mental Health and Well-Being of Solid Organ Transplant Donors. The Forgotten Sacrifices

 , and
, and 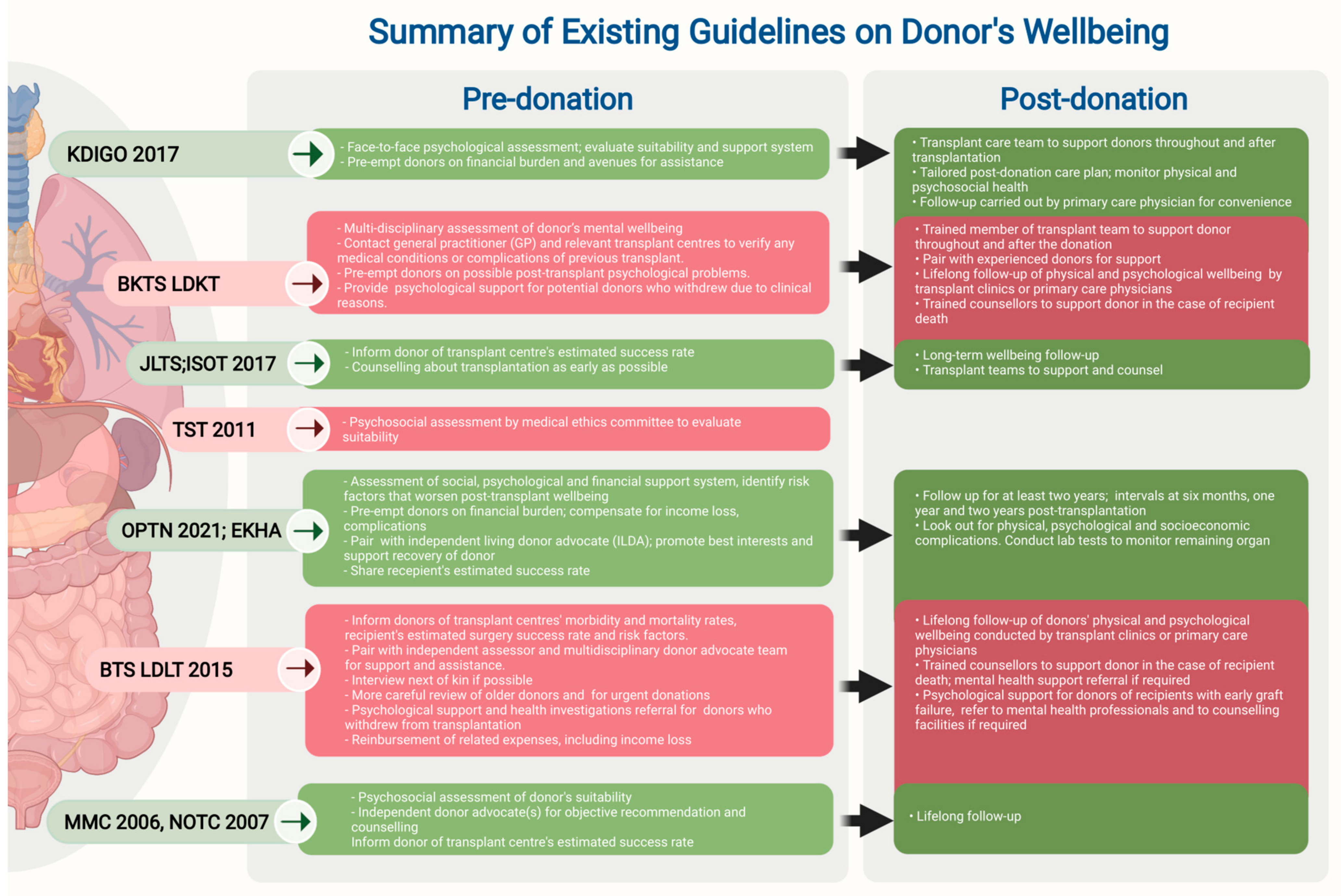{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
3. Current Status of Living Donor Transplant
4. The Impact of Organ Donation on Donors
5. Current Guidance on Donor Wellbeing
6. Risk Factors for Adverse Mental Outcomes in Donors
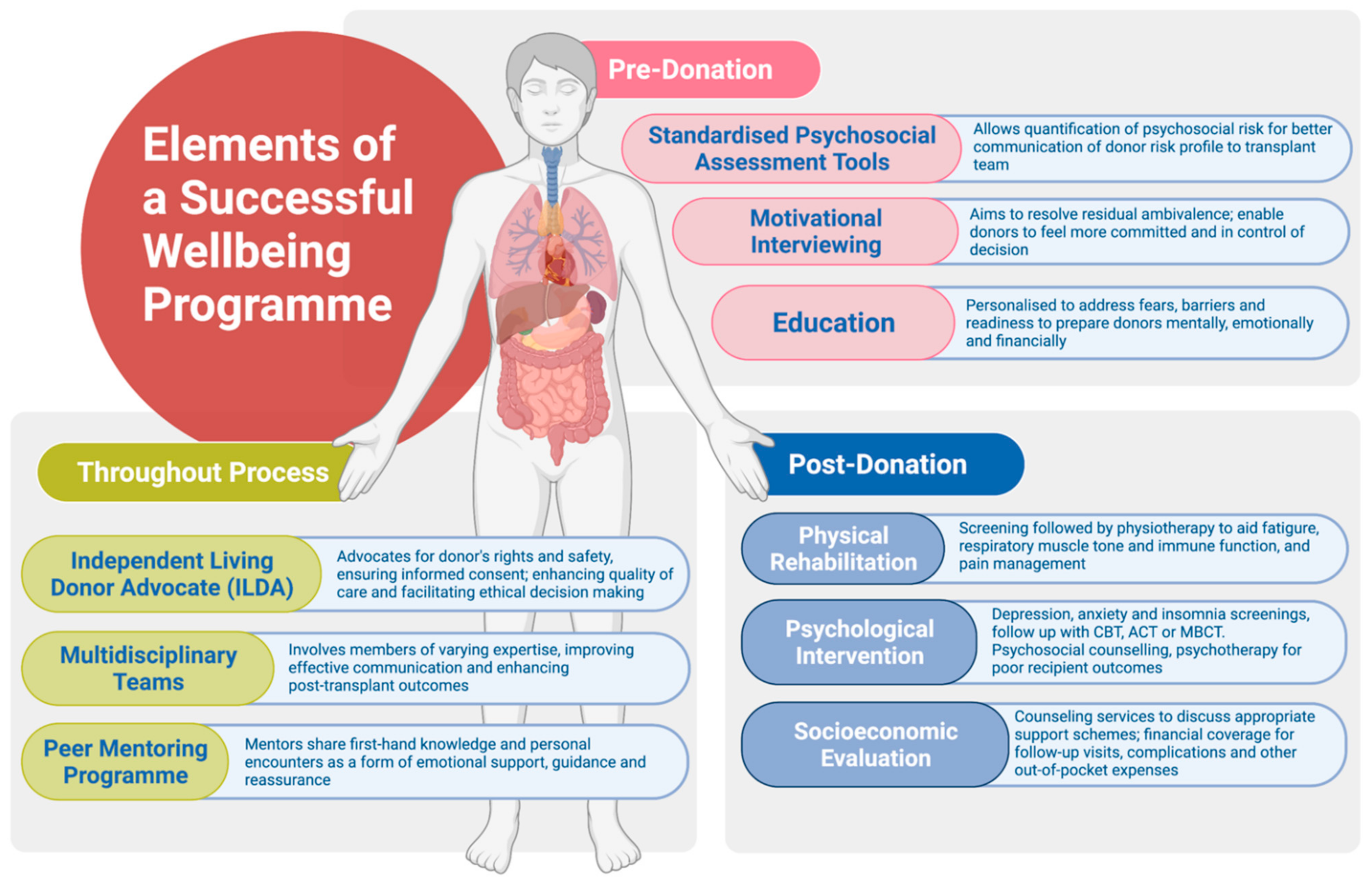
7. Elements of a Successful Wellbeing Programme
7.1. Pre-Donation
7.2. Post-Donation
7.3. Throughout Donation Process
8. Gaps for Future Research
9. Future Directions
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Merrill, J.P.; Harrison, J.H.; Murray, J.; Guild, W.R. Successful Homotransplantation of the Kidney in an Identical Twin. Trans. Am. Clin. Clim. Assoc. 1955, 67, 166–173. [Google Scholar]
- Raia, S.; Nery, J.R.; Mies, S. Liver transplantation from live donors. Lancet 1989, 2, 497. [Google Scholar] [CrossRef]
- Mahillo, B.; Carmona, M.; Alvarez, M.; Marco, J.; Nuñez, J.R.; López-Fraga, M.; Matesanz, R.; Domínguez-Gil, B. Worldwide distribution of solid organ transplantation and access of population to those practices. Transplantation 2018, 102, S71–S72. [Google Scholar] [CrossRef]
- Abouna, G. Organ Shortage Crisis: Problems and Possible Solutions. Transplant. Proc. 2008, 40, 34–38. [Google Scholar] [CrossRef]
- Shukla, A.; Vadeyar, H.; Rela, M.; Shah, S. Liver Transplantation: East versus West. J. Clin. Exp. Hepatol. 2013, 3, 243–253. [Google Scholar] [CrossRef] [Green Version]
- Akabayashi, A. Brain-Death and Organ Transplantation: The First Japanese Path. In Bioethics Across the Globe; Springer Science and Business Media LLC: Berlin, Germany, 2020; pp. 13–26. [Google Scholar]
- Tong, A.; Chapman, J.R.; Kee, T.; Li, P.K.T.; Tsai, D.F.C.; Wong, G.; Craig, J.C. Perspectives of Transplant Professionals on the Values, Ethics, and Challenges of Living Kidney Donor Evaluation in Asia. Transplantation 2015, 99, 1386–1395. [Google Scholar] [CrossRef]
- Lee, L.-Y.; Pham, T.A.; Melcher, M.L. Living Kidney Donation: Strategies to Increase the Donor Pool. Surg. Clin. N. Am. 2019, 99, 37–47. [Google Scholar] [CrossRef]
- Russo, M.W.; Lapointe-Rudow, D.; Kinkhabwala, M.; Emond, J.; Brown, R.S. Impact of Adult Living Donor Liver Transplantation on Waiting Time Survival in Candidates Listed for Liver Transplantation. Arab. Archaeol. Epigr. 2004, 4, 427–431. [Google Scholar] [CrossRef]
- Olthoff, K.M.; Smith, A.; Abecassis, M.; Baker, T.; Emond, J.C.; Berg, C.L.; Beil, C.A.; Burton, J.R.; Fisher, R.A.; Freise, C.E.; et al. Defining Long-term Outcomes with Living Donor Liver Transplantation in North America. Ann. Surg. 2015, 262, 465–475. [Google Scholar] [CrossRef] [Green Version]
- Niemi, M.; Mandelbrot, D.A. The Outcomes of Living Kidney Donation from Medically Complex Donors: Implications for the Donor and the Recipient. Curr. Transplant. Rep. 2014, 1, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Levitsky, J. Does the Liver Provide Immunosuppressive Advantage? Clin. Liver Dis. 2019, 13, 180–183. [Google Scholar] [CrossRef]
- Levitsky, J.; Feng, S. Tolerance in clinical liver transplantation. Hum. Immunol. 2018, 79, 283–287. [Google Scholar] [CrossRef]
- Braun, H.J.; Ascher, N.L.; Roll, G.R.; Roberts, J.P. Biliary complications following living donor hepatectomy. Transplant. Rev. 2016, 30, 247–252. [Google Scholar] [CrossRef]
- Lentine, K.L.; Lam, N.N.; Segev, D.L. Risks of living kidney donation: Current state of knowledge on outcomes important to donors. Clin. J. Am. Soc. Nephrol. 2019, 14, 597–608. [Google Scholar] [CrossRef] [Green Version]
- Boyarsky, B.J.; Massie, A.B.; Alejo, J.L.; Van Arendonk, K.J.; Wildonger, S.; Garonzik-Wang, J.M.; Montgomery, R.A.; Deshpande, N.A.; Muzaale, A.D.; Segev, D.L. Experiences Obtaining Insurance After Live Kidney Donation. Arab. Archaeol. Epigr. 2014, 14, 2168–2172. [Google Scholar] [CrossRef] [Green Version]
- The Lancet Gastroenterology & Hepatology. Removing barriers to living organ donation. Lancet Gastroenterol. Hepatol. 2021, 6, 335. [Google Scholar] [CrossRef]
- OPTN/SRTR 2019 Annual Data Report: Kidney. 2019. Available online: https://srtr.transplant.hrsa.gov/annual_reports/2019/Kidney.aspx (accessed on 6 May 2021).
- OPTN/SRTR 2019 Annual Data Report: Liver. 2019. Available online: https://srtr.transplant.hrsa.gov/annual_reports/2019/Liver.aspx (accessed on 6 May 2021).
- Abu-Gazala, S.; Olthoff, K.M. Current Status of Living Donor Liver Transplantation in the United States. Annu. Rev. Med. 2019, 70, 225–238. [Google Scholar] [CrossRef]
- 2020 Organ Procurement Transplantation Network. Available online: https://optn.transplant.hrsa.gov/data/view-data-reports/build-advanced/ (accessed on 6 May 2021).
- Ghobrial, R.M.; Freise, C.E.; Trotter, J.F.; Tong, L.; Ojo, A.O.; Fair, J.H.; Fisher, R.A.; Emond, J.C.; Koffron, A.J.; Pruett, T.L.; et al. Donor Morbidity after Living Donation for Liver Transplantation. Gastroenterol 2008, 135, 468–476. [Google Scholar] [CrossRef] [Green Version]
- Sommerer, C.; Morath, C.; Andrassy, J.; Zeier, M. The long-term consequences of living-related or unrelated kidney donation. Nephrol. Dial. Transplant. 2004, 19, iv45–iv47. [Google Scholar] [CrossRef]
- Butt, Z.; DiMartini, A.F.; Liu, Q.; Simpson, M.A.; Smith, A.R.; Zee, J.; Gillespie, B.W.; Holtzman, S.; Ladner, D.; Olthoff, K.; et al. Fatigue, Pain, and Other Physical Symptoms of Living Liver Donors in the Adult-to-Adult Living Donor Liver Transplantation Cohort Study. Liver Transplant. 2018, 24, 1221–1232. [Google Scholar] [CrossRef]
- Chien, C.H.; Wang, H.-H.; Chiang, Y.-J.; Chu, S.-H.; Liu, H.-E.; Liu, K.-L. Quality of Life After Laparoscopic Donor Nephrectomy. Transplant. Proc. 2010, 42, 696–698. [Google Scholar] [CrossRef]
- Ladner, D.P.; Dew, M.A.; Forney, S.; Gillespie, B.W.; Brown, R.S.; Merion, R.M.; Freise, C.E.; Hayashi, P.H.; Hong, J.C.; Ashworth, A.; et al. Long-term quality of life after liver donation in the adult to adult living donor liver transplantation cohort study (A2ALL). J. Hepatol. 2015, 62, 346–353. [Google Scholar] [CrossRef] [Green Version]
- Wee, I.J.; Syn, N.; Lee, L.S.; Tan, S.S.; Chiow, A.K. A systematic review and meta-analysis on the quality of life after hepatic resection. HPB 2020, 22, 177–186. [Google Scholar] [CrossRef]
- Butt, Z.; Dew, M.A.; Liu, Q.; Simpson, M.A.; Smith, A.R.; Zee, J.; Gillespie, B.W.; Abbey, S.E.; Ladner, D.P.; Weinrieb, R.; et al. Psychological Outcomes of Living Liver Donors from a Multicenter Prospective Study: Results From the Adult-to-Adult Living Donor Liver Transplantation Cohort Study2 (A2ALL-2). Arab. Archaeol. Epigr. 2016, 17, 1267–1277. [Google Scholar] [CrossRef] [Green Version]
- Walter, M.; Papachristou, C.; Pascher, A.; Danzer, G.; Neuhaus, P.; Klapp, B.F.; Frommer, J. Impaired psychosocial outcome of donors after living donor liver transplantation: A qualitative case study. Clin. Transplant. 2006, 20, 410–415. [Google Scholar] [CrossRef]
- Shi, Y.; Liu, C.; Zhang, H.; Huang, Y.; Sun, M.; Wang, W.; Shang, S. Changes in the quality of life of living liver donors: A meta-analysis. Int. J. Nurs. Stud. 2020, 109, 103586. [Google Scholar] [CrossRef]
- Watson, J.M.; Behnke, M.K.; Fabrizio, M.D.; McCune, T.R. Recipient graft failure or death impact on living kidney donor quality of life based on the living organ donor network database. J. Endourol. 2013, 27, 1525–1529. [Google Scholar] [CrossRef]
- Lentine, K.L.; Schnitzler, M.A.; Xiao, H.; Axelrod, D.; Davis, C.L.; McCabe, M.; Brennan, D.C.; Leander, S.; Garg, A.X.; Waterman, A. Depression diagnoses after living kidney donation: Linking U.S. Registry data and administrative claims. Transplantation 2012, 94, 77–83. [Google Scholar] [CrossRef]
- Massey, E.K.; Timmerman, L.; Ismail, S.Y.; Duerinckx, N.; Lopes, A.; Maple, H.; Mega, I.; Papachristou, C.; Dobbels, F.; ELPAT Psychosocial Care for Living Donors and Recipients Working Group. The ELPAT living organ donor Psychosocial Assessment Tool (EPAT): From ‘what’ to ‘how’ of psychosocial screening-A pilot study. Transpl. Int. 2018, 31, 56–70. [Google Scholar] [CrossRef] [Green Version]
- DiMartini, A.; Dew, M.A.; Liu, Q.; Simpson, M.A.; Ladner, D.P.; Smith, A.; Zee, J.; Abbey, S.; Gillespie, B.W.; Weinrieb, R.; et al. Social and Financial Outcomes of Living Liver Donation: A Prospective Investigation Within the Adult-to-Adult Living Donor Liver Transplantation Cohort Study 2 (A2ALL-2). Arab. Archaeol. Epigr. 2017, 17, 1081–1096. [Google Scholar] [CrossRef]
- Organ Procurement and Transplantation Network. Organ Procurement and Transplantation Network (OPTN) Policies; United Network for Organ Sharing: Richmond, VA, USA, 1984. [Google Scholar]
- British Transplantation Society. Living Donor Liver Transplantation; British Transplantation Society: Birmingham, UK, 2015. [Google Scholar]
- British Transplantation Society. Guidelines for Living Donor Kidney Transplantation, 4th ed.; British Transplantation Society: Birmingham, UK, 2018. [Google Scholar]
- Lentine, K.L.; Kasiske, B.L.; Levey, A.S.; Adams, P.L.; Alberú, J.; Bakr, M.A.; Gallon, L.; Garvey, C.A.; Guleria, S.; Li, P.K.-T.; et al. KDIGO Clinical Practice Guideline on the Evaluation and Care of Living Kidney Donors. Transplant 2017, 101, S7–S105. [Google Scholar] [CrossRef] [PubMed]
- Medical Development Division Malaysia. National Organ, Tissue and Cell Transplantation Policy; Malaysian Ministry of Health: Putrajaya, Malaysia, 2007.
- Regulation on Human Organ Transplant. Renti Qiguan Yizhi Tiaoli; The Central People’s Government of the People’s Republic of China: Beijing, China, 2011. [Google Scholar]
- Kute, V.B.; Agarwal, S.K.; Sahay, M.; Kumar, A.; Rathi, M.; Prasad, N.; Sharma, R.K.; Gupta, K.L.; Shroff, S.; Saxena, S.K.; et al. Kidney-paired donation to increase living donor kidney transplantation in India: Guidelines of Indian Society of Organ Transplantation–2017. Indian J. Nephrol. 2018, 28, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Japanese Liver Transplantation Society. Guidelines for Liver Donor Surgery. Available online: http://jlts.umin.ac.jp/history/donor.html (accessed on 7 May 2021).
- Malaysian Medical Council. Organ Transplantation, Guideline of the Malaysian Medical Council; Malaysian Ministry of Health: Putrajaya, Malaysia, 2006.
- Ergene, T.; Karadibak, D.; Polat, K.Y. Fatigue and Physiotherapy in Liver Transplant Recipients Fatigue and Physiotherapy. Clin. Exp. Health Sci. 2019, 9, 278–282. [Google Scholar] [CrossRef] [Green Version]
- Pang, A.; Lingham, S.; Zhao, W.; LeDuc, S.; Räkel, A.; Sapir-Pichhadze, R.; Mathur, S.; Janaudis-Ferreira, T. Physician Practice Patterns and Barriers to Counselling on Physical Activity in Solid Organ Transplant Recipients. Ann. Transplant. 2018, 23, 345–359. [Google Scholar] [CrossRef]
- National Institute of Diabetes and Digestive and Kidney Diseases. Adult Living Donor Liver Transplantation Studies (A2ALL); United States National Institutes of Health: Bethesda, MD, USA, 2003.
- Arbor Research Collaborative for Health. Adult-to-Adult Living Donor Transplant Cohort Study (A2ALL-2); United States National Institutes of Health: Bethesda, MD, USA, 2012.
- Rodrigue, J.R.; Schold, J.D.; Morrissey, P.; Whiting, P.; Vella, J.; Kayler, L.K.; Katz, D.; Jones, J.; Kaplan, B.; Fleishman, A.; et al. Mood, body image, fear of kidney failure, life satisfaction, and decisional stability following living kidney donation: Findings from the KDOC study. Am. J. Transplant. 2018, 18, 1397–1407. [Google Scholar] [CrossRef]
- Chen, J.; Bhattacharya, S.; Sirota, M.; Laiudompitak, S.; Schaefer, H.; Thomson, E.; Wiser, J.; Sarwal, M.M.; Butte, A.J. Assessment of Postdonation Outcomes in US Living Kidney Donors Using Publicly Available Data Sets. JAMA Netw. Open 2019, 2, e191851. [Google Scholar] [CrossRef]
- Faeder, S.; Moschenross, D.; Rosenberger, E.; Dew, M.A.; DiMartini, A. Psychiatric aspects of organ transplantation and donation. Curr. Opin. Psychiatry 2015, 28, 357–364. [Google Scholar] [CrossRef] [Green Version]
- Waterman, A.D.; Robbins, M.L.; Paiva, A.L.; Peipert, J.D.; Kynard-Amerson, C.S.; Goalby, C.J.; Davis, L.A.; Thein, J.L.; Schenk, E.A.; Baldwin, K.A.; et al. Your Path to Transplant: A randomized controlled trial of a tailored computer education intervention to increase living donor kidney transplant. BMC Nephrol. 2014, 15, 166. [Google Scholar] [CrossRef] [Green Version]
- Moore, D.R.; Serur, D.; Rudow, D.L.; Rodrigue, J.R.; Hays, R.; Cooper, M. Living Donor Kidney Transplantation: Improving Efficiencies in Live Kidney Donor Evaluation–Recommendations from a Consensus Conference. Clin. J. Am. Soc. Nephrol. 2015, 10, 1678–1686. [Google Scholar] [CrossRef] [Green Version]
- Dageforde, L.A.; Petersen, A.W.; Feurer, I.D.; Cavanaugh, K.L.; Harms, K.A.; Ehrenfeld, J.M.; Moore, D.E. Health Literacy of Living Kidney Donors and Kidney Transplant Recipients. Transplant 2014, 98, 88–93. [Google Scholar] [CrossRef] [Green Version]
- Dew, M.A.; DiMartini, A.F.; Dabbs, A.J.D.; Zuckoff, A.; Tan, H.P.; McNulty, M.L.; Switzer, G.E.; Fox, K.R.; Greenhouse, J.B.; Humar, A. Preventive Intervention for Living Donor Psychosocial Outcomes: Feasibility and Efficacy in a Randomized Controlled Trial. Arab. Archaeol. Epigr. 2013, 13, 2672–2684. [Google Scholar] [CrossRef]
- Zuckoff, A.; Dew, M.A. Research on MI in Equipoise: The Case of Living Organ Donation. Motiv. Interviewing Train. Res. Implement. Pract. 2012, 1, 39–41. [Google Scholar] [CrossRef] [Green Version]
- Holscher, C.M.; Leanza, J.; Thomas, A.G.; Waldram, M.M.; Haugen, C.E.; Jackson, K.R.; Bae, S.; Massie, A.B.; Segev, D.L. Anxiety, depression, and regret of donation in living kidney donors. BMC Nephrol. 2018, 19, 1–7. [Google Scholar] [CrossRef]
- Glaser, B.; Suter, E. Interprofessional collaboration and integration as experienced by social workers in health care. Soc. Work Health Care 2016, 55, 395–408. [Google Scholar] [CrossRef]
- Barr, M.L.; Belghiti, J.; Villamil, F.G.; Pomfret, E.A.; Sutherland, D.S.; Gruessner, R.W.; Langnas, A.N.; Delmonico, F.L. A Report of the Vancouver Forum on the Care of the Live Organ Donor: Lung, Liver, Pancreas, and Intestine Data and Medical Guidelines. Transplant 2006, 81, 1373–1385. [Google Scholar] [CrossRef] [Green Version]
- Takada, Y.; Suzukamo, Y.; Oike, F.; Egawa, H.; Morita, S.; Fukuhara, S.; Uemoto, S.; Tanaka, K. Long-term quality of life of donors after living donor liver transplantation. Liver Transpl. 2012, 18, 1343–1352. [Google Scholar] [CrossRef]
- Bossola, M.; Pepe, G.; Vulpio, C. Fatigue in kidney transplant recipients. Clin. Transplant. 2016, 30, 1387–1393. [Google Scholar] [CrossRef]
- Katz, N. The Impact of Pain Management on Quality of Life. J. Pain Symptom Manag. 2002, 24, S38–S47. [Google Scholar] [CrossRef]
- Tang, N.K.Y.; Crane, C. Suicidality in chronic pain: A review of the prevalence, risk factors and psychological links. Psychol. Med. 2006, 36, 575–586. [Google Scholar] [CrossRef]
- Onofre, T.; Junior, J.F.F.; Amorim, C.F.; Minamoto, S.T.; Paisani, D.D.M.; Chiavegato, L.D. Impact of an early physiotherapy program after kidney transplant during hospital stay: A randomized controlled trial. Braz. J. Nephrol. 2017, 39, 424–432. [Google Scholar] [CrossRef]
- Dewe, G.; Steyaert, A.; De Kock, M.; Lois, F.; Reding, R.; Forget, P. Pain management in living related adult donor hepatectomy: Feasibility of an evidence-based protocol in 100 consecutive donors. BMC Res. Notes 2018, 11, 834. [Google Scholar] [CrossRef] [PubMed]
- Rodrigue, J.R.; Fleishman, A.; Schold, J.D.; Morrissey, P.; Whiting, J.; Vella, J.; Kayler, L.K.; Katz, D.A.; Jones, J.; Kaplan, B.; et al. Patterns and predictors of fatigue following living donor nephrectomy: Findings from the KDOC Study. Am. J. Transplant. 2020, 20, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Jowsey, S.G.; Jacobs, C.; Gross, C.R.; Hong, B.A.; Messersmith, E.E.; Gillespie, B.W.; Beebe, T.J.; Kew, C.; Matas, A.J.; Yusen, R.D.; et al. Emotional Well-Being of Living Kidney Donors: Findings from the RELIVE Study. Arab. Archaeol. Epigr. 2014, 14, 2535–2544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkinson, C.; Coulter, A.; Wright, L. Short form 36 (SF36) health survey questionnaire: Normative data for adults of working age. BMJ 1993, 306, 1437–1440. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Johnson, S.U.; Ulvenes, P.G.; Øktedalen, T.; Hoffart, A. Psychometric Properties of the General Anxiety Disorder 7-Item (GAD-7) Scale in a Heterogeneous Psychiatric Sample. Front. Psychol. 2019, 10, 1713. [Google Scholar] [CrossRef] [Green Version]
- Backhaus, J.; Junghanns, K.; Broocks, A.; Riemann, D.; Hohagen, F. Test–retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. J. Psychosom. Res. 2002, 53, 737–740. [Google Scholar] [CrossRef]
- Beck, A.T. Cognitive therapy: Nature and relation to behavior therapy. Behav. Ther. 1970, 1, 184–200. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Asnaani, A.; Vonk, I.J.J.; Sawyer, A.T.; Fang, A. The Efficacy of Cognitive Behavioral Therapy: A Review of Meta-analyses. Cogn. Ther. Res. 2012, 36, 427–440. [Google Scholar] [CrossRef] [Green Version]
- Foroushani, P.S.; Schneider, J.; Assareh, N. Meta-review of the effectiveness of computerised CBT in treating depression. BMC Psychiatry 2011, 11, 131. [Google Scholar] [CrossRef] [Green Version]
- Hayes, S.C.; Luoma, J.B.; Bond, F.W.; Masuda, A.; Lillis, J. Acceptance and Commitment Therapy: Model, processes and outcomes. Behav. Res. Ther. 2006, 44, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Twohig, M.P.; Levin, M.E. Acceptance and Commitment Therapy as a Treatment for Anxiety and Depression: A Review. Psychiatr. Clin. N. Am. 2017, 40, 751–770. [Google Scholar] [CrossRef]
- Bai, Z.; Luo, S.; Zhang, L.; Wu, S.; Chi, I. Acceptance and Commitment Therapy (ACT) to reduce depression: A systematic review and meta-analysis. J. Affect. Disord. 2020, 260, 728–737. [Google Scholar] [CrossRef]
- Krijn, M.; Emmelkamp, P.; Biemond, R.; Ligny, C.D.W.D.; Schuemie, M.J.; van der Mast, C.A. Treatment of acrophobia in virtual reality: The role of immersion and presence. Behav. Res. Ther. 2004, 42, 229–239. [Google Scholar] [CrossRef]
- Spielman, A.J.; Caruso, L.S.; Glovinsky, P.B. A Behavioral Perspective on Insomnia Treatment. Psychiatr. Clin. N. Am. 1987, 10, 541–553. [Google Scholar] [CrossRef]
- Powers, M.B.; Emmelkamp, P. Virtual reality exposure therapy for anxiety disorders: A meta-analysis. J. Anxiety Disord. 2008, 22, 561–569. [Google Scholar] [CrossRef]
- Morin, C.M.; Hauri, P.J.; Espie, C.A.; Spielman, A.J.; Buysse, D.J.; Bootzin, R.R. Nonpharmacologic Treatment of Chronic Insomnia. Sleep 1999, 22, 1134–1156. [Google Scholar] [CrossRef]
- Leichsenring, F.; Leibing, E. Psychodynamic psychotherapy: A systematic review of techniques, indications and empirical evidence. Psychol. Psychother. Theory Res. Pract. 2007, 80, 217–228. [Google Scholar] [CrossRef]
- Goetzmann, L.; Wagner-Huber, R.; Klaghofer, R.; Muellhaupt, B.; Clavien, P.; Buddeberg, C.; Scheuer, E. Waiting for a Liver Transplant: Psychosocial Well-Being, Spirituality, and Need for Counselling. Transplant. Proc. 2006, 38, 2931–2936. [Google Scholar] [CrossRef]
- Gallagher, M.; Tracey, A.; Millar, R. Ex-clients’ evaluation of bereavement counselling in a voluntary sector agency. Psychol. Psychother. Theory Res. Pract. 2005, 78, 59–76. [Google Scholar] [CrossRef]
- University of Michigan Health Michigan Medicine. Kidney Transplant Peer Mentor Program; University of Medicine and Health Sciences: Ann Arbor, MI, USA, 2020. [Google Scholar]
- American Transplant Foundation. Mentorship Testimonials; American Transplant Foundation: Denver, CO, USA, 2019. [Google Scholar]
- Fraser, R.T.; McMahon, B.T.; Wiggins, A.; Clift, A.; Hunter-Banks, S. Considerations in developing a specialized epilepsy employment program: A sponsor’s playbook. Epilepsy Behav. 2020, 102, 106698. [Google Scholar] [CrossRef] [PubMed]
- Tietjen, A.; Hays, R.; McNatt, G.; Howey, R.; Lebron-Banks, U.; Thomas, C.; Lentine, K.L. Billing for Living Kidney Donor Care: Balancing Cost Recovery, Regulatory Compliance, and Minimized Donor Burden. Curr. Transplant. Rep. 2019, 6, 155–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobs, C.; Thomas, C. Financial considerations in living organ donation. Prog. Transplant. 2003, 13, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Fonouni, H.; Golriz, M.; Mehrabi, A.; Oweira, H.; Schmied, B.; Müller, S.; Jarahian, P.; Rad, M.T.; Esmaeilzadeh, M.; Tönshoff, B.; et al. The Role of an Interdisciplinary Transplant Team on Living Donation Kidney Transplantation Program. Transplant. Proc. 2010, 42, 137–140. [Google Scholar] [CrossRef]
- Lumsdaine, J.; Wigmore, S.; Wooton, D.; Stewart, C.; Akyol, M.; Forsythe, J. Establishing a transplant coordinator-led living kidney donor follow-up clinic. Prog. Transplant. 2003, 13, 138–141. [Google Scholar] [CrossRef]
- Rudow, D.L.; Brown, R.S., Jr. Role of the independent donor advocacy team in ethical decision making. Prog. Transplant. 2005, 15, 298–302. [Google Scholar] [CrossRef]
- Killian, A.C.; Reed, R.D.; Carter, A.; McLeod, M.C.; Shelton, B.A.; Kumar, V.; Qu, H.; MacLennan, P.A.; Orandi, B.J.; Cannon, R.M.; et al. Self-advocacy is associated with lower likelihood of living donor kidney transplantation. Am. J. Surg. 2021, 222, 36–41. [Google Scholar] [CrossRef]
- Cahn-Fuller, K.L.; Parent, B. Transplant eligibility for patients with affective and psychotic disorders: A review of practices and a call for justice. BMC Med. Ethics 2017, 18, 72. [Google Scholar] [CrossRef] [Green Version]
- Rowley, A.A.; Hong, B.A.; Martin, S.; Jones, L.; Vijayan, A.; Shenoy, S.; Jendrisak, M. Psychiatric disorders: Are they an absolute contraindication to living donation? Prog. Transplant. 2009, 19, 128–131. [Google Scholar] [CrossRef]
- Pham, Y.H.; Miloh, T. Liver Transplantation in Children. Clin. Liver Dis. 2018, 22, 807–821. [Google Scholar] [CrossRef]
- Saeed, B. Pediatric renal transplantation. Int. J. Organ. Transplant. Med. 2012, 3, 62–73. [Google Scholar]
- Kärrfelt, H.M.E.; Berg, U.B.; Lindblad, F.I.E. Renal transplantation in children: Psychological and donation-related aspects from the parental perspective. Pediatr. Transplant. 2000, 4, 305–312. [Google Scholar] [CrossRef]
- Organ Procurement and Transplantation Network (OPTN) Living Non-Directed Organ Donation; United Network for Organ Sharing: Richmond, VA, USA, 2015.
- Moorlock, G.; Ives, J.; Draper, H. Altruism in organ donation: An unnecessary requirement? Table 1. J. Med. Ethics 2013, 40, 134–138. [Google Scholar] [CrossRef] [Green Version]
- Schulz, K.-H.; Kroencke, S.; Beckmann, M.; Nadalin, S.; Paul, A.; Fischer, L.; Nashan, B.; Senf, W.; Erim, Y. Mental and physical quality of life in actual living liver donors versus potential living liver donors: A prospective, controlled, multicenter study. Liver Transplant. 2009, 15, 1676–1687. [Google Scholar] [CrossRef]
- Burra, P.; De Bona, M. Quality of life following organ transplantation. Transpl. Int. 2007, 20, 397–409. [Google Scholar] [CrossRef]
- Papachristou, C.; Walter, M.; Schmid, G.; Frommer, J.; Klapp, B. Living donor liver transplantation and its effect on the donor-recipient relationship--a qualitative interview study with donors. Clin. Transplant. 2009, 23, 382–391. [Google Scholar] [CrossRef]
- Krause, S.; Pritlove, C.; Abbey, S.; Jung, J. The Meaning Behind the Scar: Anonymous Live Liver Donors’ Perceptions of Their Surgical Scars. Transplant 2021, 105, 1039–1043. [Google Scholar] [CrossRef]
- Lai, Y.-C.; Lee, W.-C.; Juang, Y.-Y.; Yen, L.-L.; Weng, L.-C.; Chou, H.F. Effect of social support and donation-related concerns on ambivalence of living liver donor candidates. Liver Transplant. 2014, 20, 1365–1371. [Google Scholar] [CrossRef]
- Erim, Y.; Kahraman, Y.; Vitinius, F.; Beckmann, M.; Kroncke, S.; Witzke, O. Resilience and quality of life in 161 living kidney donors before nephrectomy and in the aftermath of donation: A naturalistic single center study. BMC Nephrol. 2015, 16, 164. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, E.R.; Yousaf, O.; Vittersø, A.D.; Jones, L. Dispositional Mindfulness and Psychological Health: A Systematic Review. Mindfulness 2018, 9, 23–43. [Google Scholar] [CrossRef] [Green Version]
- Conversano, C.; Rotondo, A.; Lensi, E.; Della Vista, O.; Arpone, F.; Reda, M.A. Optimism and Its Impact on Mental and Physical Well-Being. Clin. Pract. Epidemiol. Ment. Health 2010, 6, 25–29. [Google Scholar] [CrossRef]
- Koenig, H.G. Research on Religion, Spirituality, and Mental Health: A Review. Can. J. Psychiatry 2009, 54, 283–291. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Chapman, J.R.; Israni, A.; Gordon, E.J.; Craig, J.C. Qualitative research in organ transplantation: Recent contributions to clinical care and policy. Am. J. Transplant. 2013, 13, 1390–1399. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, X.-H.; Toh, J.Z.K.; Ng, C.H.; Tay, P.W.L.; Wong, N.W.; Kow, A.W.C.; Vathsala, A.; Tan, E.X.-X.; Muthiah, M.D.; Lim, W.H. Mental Health and Well-Being of Solid Organ Transplant Donors. The Forgotten Sacrifices. Transplantology 2021, 2, 274-287. https://0-doi-org.brum.beds.ac.uk/10.3390/transplantology2030026
Pan X-H, Toh JZK, Ng CH, Tay PWL, Wong NW, Kow AWC, Vathsala A, Tan EX-X, Muthiah MD, Lim WH. Mental Health and Well-Being of Solid Organ Transplant Donors. The Forgotten Sacrifices. Transplantology. 2021; 2(3):274-287. https://0-doi-org.brum.beds.ac.uk/10.3390/transplantology2030026
Chicago/Turabian StylePan, Xin-Hui, Jonathan Zhi Kai Toh, Cheng Han Ng, Phoebe Wen Lin Tay, Neng Wei Wong, Alfred Wei Chieh Kow, Anantharaman Vathsala, Eunice Xiang-Xuan Tan, Mark Dhinesh Muthiah, and Wen Hui Lim. 2021. "Mental Health and Well-Being of Solid Organ Transplant Donors. The Forgotten Sacrifices" Transplantology 2, no. 3: 274-287. https://0-doi-org.brum.beds.ac.uk/10.3390/transplantology2030026