One Health—Its Importance in Helping to Better Control Antimicrobial Resistance


1
Infectious Diseases and Microbiology, Canberra Hospital, Garran, ACT 2605, Australia
2
Medical School, Australian National University, Acton ACT 2601, Australia
3
Department of Population Medicine, University of Guelph, Guelph N1G 2W1, Canada
*
Author to whom correspondence should be addressed.
Trop. Med. Infect. Dis. 2019, 4(1), 22; https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed4010022
Submission received: 27 December 2018
/
Revised: 18 January 2019
/
Accepted: 23 January 2019
/
Published: 29 January 2019
(This article belongs to the Special Issue One Health and Zoonoses)
Abstract
:Approaching any issue from a One Health perspective necessitates looking at the interactions of people, domestic animals, wildlife, plants, and our environment. For antimicrobial resistance this includes antimicrobial use (and abuse) in the human, animal and environmental sectors. More importantly, the spread of resistant bacteria and resistance determinants within and between these sectors and globally must be addressed. Better managing this problem includes taking steps to preserve the continued effectiveness of existing antimicrobials such as trying to eliminate their inappropriate use, particularly where they are used in high volumes. Examples are the mass medication of animals with critically important antimicrobials for humans, such as third generation cephalosporins and fluoroquinolones, and the long term, in-feed use of antimicrobials, such colistin, tetracyclines and macrolides, for growth promotion. In people it is essential to better prevent infections, reduce over-prescribing and over-use of antimicrobials and stop resistant bacteria from spreading by improving hygiene and infection control, drinking water and sanitation. Pollution from inadequate treatment of industrial, residential and farm waste is expanding the resistome in the environment. Numerous countries and several international agencies have now included a One Health Approach within their action plans to address antimicrobial resistance. Necessary actions include improvements in antimicrobial use, better regulation and policy, as well as improved surveillance, stewardship, infection control, sanitation, animal husbandry, and finding alternatives to antimicrobials.
1. Introduction
Antimicrobial resistance is a global public health problem [1,2]. Most bacteria that cause serious infections and could once be successfully treated with several different antibiotic classes, have now acquired resistance—often to many antibiotics. In some regions the increased resistance has been so extensive that resistance is present in some bacteria to nearly all of these drugs [2,3,4]. The threat is most acute for antibacterial antimicrobials (antibiotics—the focus of this paper) but also threatens antifungals, antiparastics and antivirals [5].
Antimicrobial overuse is occurring in multiple sectors (human, animal, agriculture) [3,6]. Microorganisms faced with antimicrobial selection pressure enhance their fitness by acquiring and expressing resistance genes, then sharing them with other bacteria and by other mechanisms, for example gene overexpression and silencing, phase variation. When bacteria are resistant they also present in much larger numbers when exposed to antimicrobials, whether in an individual, in a location and in the environment. Additionally important in driving the deteriorating resistance problem are factors that promote the spread of resistant bacteria (or “contagion”) [7]. This spread involves not only bacteria themselves but the resistance genes they carry and that can be acquired by other bacteria [8]. Factors that facilitate “contagion” include poverty, poor housing, poor infection control, poor water supplies, poor sanitation, run off of waste from intensive agriculture, environmental contamination and geographical movement of infected humans and animals [9,10,11].
Wherever antimicrobials are used, there are often already large reservoirs of resistant bacteria and resistance genes. These include people and their local environments (both in hospitals and in the community), as well as animals, farms and aquaculture environments. Large reservoirs of resistance and residual antimicrobials occur in water, soil, wildlife and many other ecological niches, not only due to pollution by sewage, pharmaceutical industry waste and manure runoff from farms [10,12,13], but often resistant bacteria and resistance genes have already been there for millennia [14,15].
Most bacteria and their genes can move relatively easily within and between humans, animals and the environment. Microbial adaptations to antimicrobial use and other selection pressures within any one sector are reflected in other sectors [8,16]. Similarly, actions (or inactions) to contain antimicrobial resistance in one sector affect other sectors [17,18]. Antimicrobial resistance is an ecological problem that is characterized by complex interactions involving diverse microbial populations affecting the health of humans, animals and the environment. It makes sense to address the resistance problem by taking this complexity and ecological nature into account using a coordinated, multi-sectoral approach, such as One Health [5,19,20,21,22,23].
One Health is defined by WHO [24] and others [25] as a concept and approach to “designing and implementing programs, policies, legislation and research in which multiple sectors communicate and work together to achieve better public health outcomes. The areas of work in which a One Health approach is particularly relevant include food safety, the control of zoonoses and combatting antibiotic resistance” [24]. It needs to involve the “collaborative effort of multiple health science professions, together with their related disciplines and institutions—working locally, nationally, and globally—to attain optimal health for people, domestic animals, wildlife, plants, and our environment” [25]. The origins of One Health are centuries old and are based on the mutual inter-dependence of people and animals and a recognition that they share not only the same environment, but also many infectious diseases [23]. Our current concept of One Health however goes much further. It also embraces the health of the environment.
2. Use of Antimicrobials in Humans, Animals and Plants
The vast majority of antimicrobial classes are used both in humans and animals (including aquaculture; both farmed fish and shellfish). Only few antimicrobial classes are reserved exclusively for humans (e.g., carbapenems). There are also few classes limited to veterinary use (e.g., flavophospholipols, ionophores); mainly because of toxicity to humans [26,27,28,29,30].
Insects (e.g., bees) and some plants are frequently treated with antimicrobials. Tetracyclines, streptomycin and some other antimicrobials are used for treatment and prophylaxis of bacterial infections of fruit, such as apples and pears (e.g., “fire blight” caused by Erwinia amylovora) [31,32]. Antifungals, especially azoles, are used in huge quantities and applied to broad acre crops such as wheat [33].
There are marked differences in the ways antimicrobials are used in human compared to non-human sectors. In people, antimicrobials are mostly used for treatment of clinical infections in individual patients, with some limited prophylactic use in individuals (e.g., post-surgery) or occasionally in groups (e.g., prevention of meningococcal disease). Antimicrobial uses in companion animals (e.g., dogs, cats, pet birds, horses) are broadly similar to those in humans, with antimicrobials mostly administered on an individual basis to treat infection, and occasionally for prophylaxis, such as post-surgery [34,35].
In the food-producing animal sector, antimicrobials are also used therapeutically to treat individual clinically sick animals (e.g., dairy cows with mastitis) [26]. However, in intensive farming and aquaculture, for reasons of practicality and efficiency, antimicrobials are often administered through feed or water to entire groups (e.g., pens of pigs, flocks of broilers), either for prophylaxis (to healthy animals at risk of infection) or metaphylaxis (to healthy animals in the same group as diseased animals) [36]. Some have even succeeded in having this group level administration defined (and we believe inappropriately) in the animal health sector as “therapeutic” use. Growth promotion, prophylaxis and metaphylaxis account for by far the largest volumes of antimicrobials used in the food-producing animal sector [26,27,37].
Growth Promotion Use
Using antimicrobials for growth promotion is highly controversial because instead of treating sick animals they are administered to healthy animals, usually for prolonged periods of time, and often at sub-therapeutic doses in order to improve production. These conditions favor selection and spread of resistant bacteria within animals and to humans through food or other environmental pathways [38,39]. The period of exposure with growth promotion is usually greater than two weeks and often almost the entire life of an animal, for example in chicken for 36 days or more.
Based on studies, mostly conducted decades ago, the purported production benefits of antimicrobial growth promoters range widely (1–10%). Surveillance and animal production data however now suggests that benefits in animals reared in good conditions are probably quite small and may be non-existent. Many large poultry corporations are now marketing chicken raised without antimicrobials administered at hatchery or farm levels [40]. Expressed concerns are that antimicrobial growth promoters are used to compensate for poor hygiene and housing, and as replacement for proper animal health management [18,41,42]. For these reasons, the World Health Organization (WHO) advocates the termination of antimicrobial use for growth promotion [5,41]. This practice has now been banned in Europe and elsewhere and is being phased out in some other countries [43,44,45]. However there are still many countries where they continue to be used [46], including drugs categorized by WHO as critically important to humans, for example colistin, fluoroquinolones and macrolides [47].
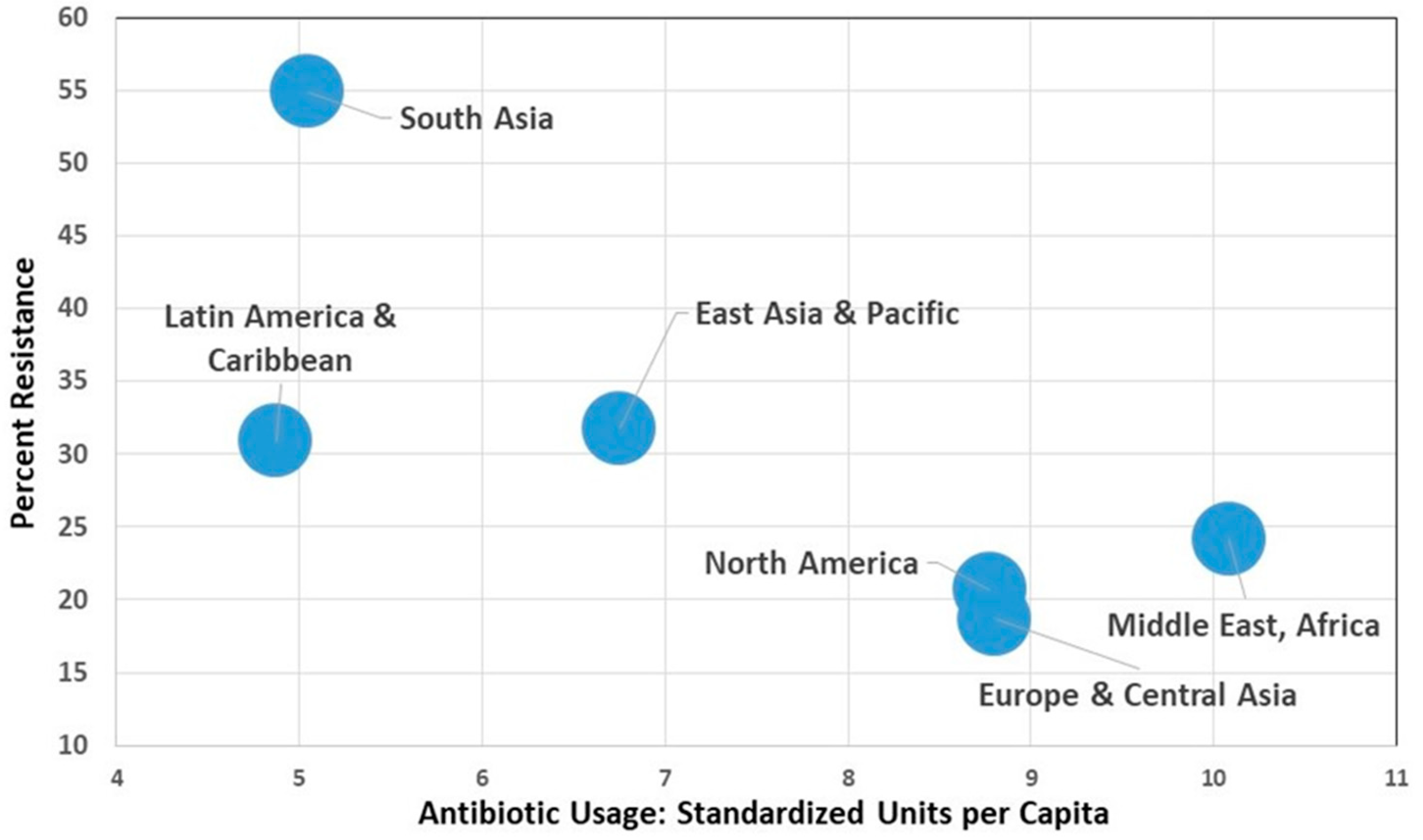
Comprehensive global quantitative data on use of antimicrobial agents in humans, animals and plants is generally lacking. Table 1 shows the varying levels of antibiotic usage in people around the world, associated resistance levels, plus some social and infrastructure parameters—the latter of which can facilitate the spread of resistant bacteria (e.g., poor sanitation). Figure 1 shows antibiotic use in different regions globally in people and the lack of correlation with increased resistance levels in bacteria and human antibiotic usage. These data strongly suggest that there are other very important factors influencing antimicrobial resistance over and above simply antibiotic usage.
Aggregating countries into regional groupings shows a pattern where there is an inverse aggregate relationship between antimicrobial resistance and usage. These data help confirm that there are other very important factors influencing antimicrobial resistance over and above simply antibiotic usage. (Figures assembled from data taken from reference 7)
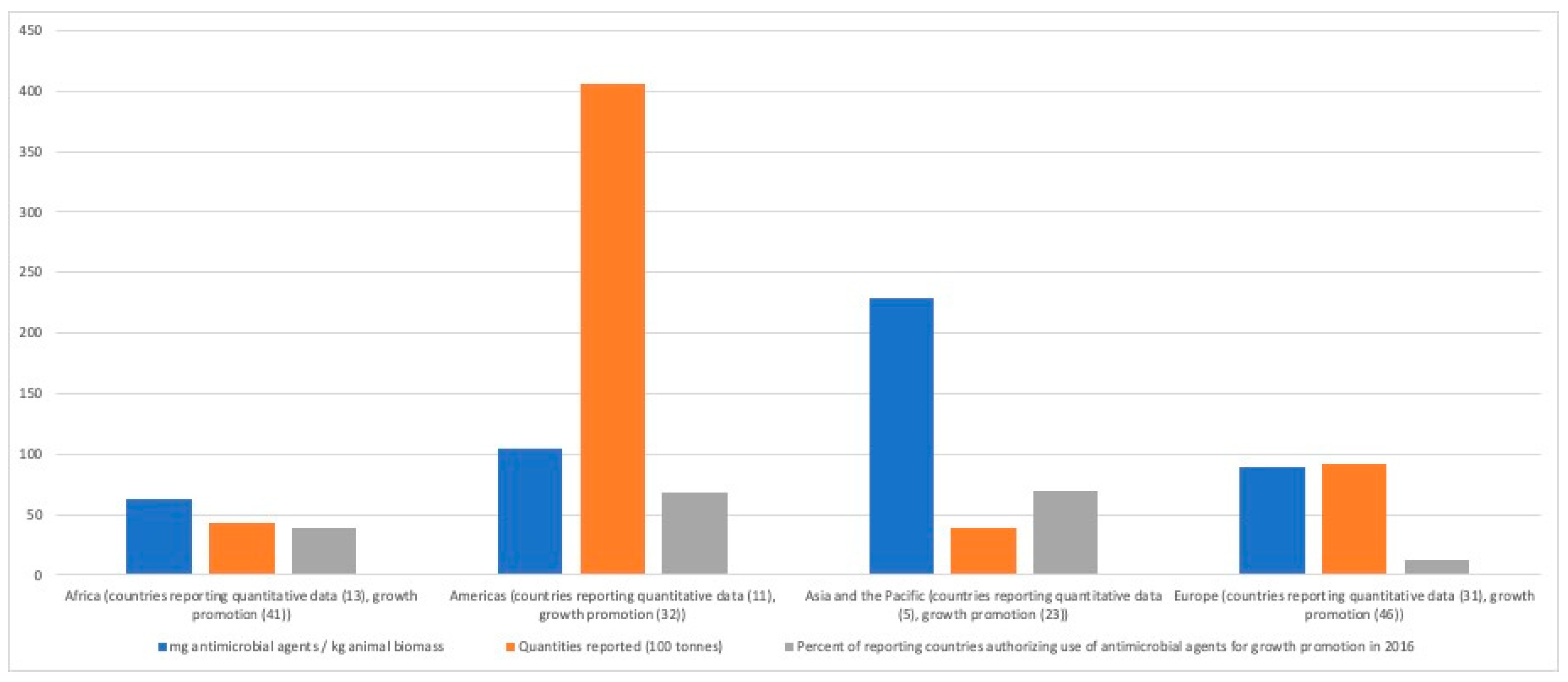
The World Organization for Animal Health has developed a global database on the use of antimicrobial agents in animals [46]. Figure 2 shows reported quantities of antimicrobials used in animals in 2014, summarized by OIE Region and expressed as total quantities (tons) and adjusted for animal biomass. Additionally, included is the per cent of countries authorizing the use of antimicrobials for growth promotion. Tetracyclines accounted for the largest proportion of overall antimicrobial use globally (37.1% of total), followed by polypeptides (15.7%), penicillins (9.8%), macrolides (8.9%) and aminoglycosides (7.8%) [46].
3. One Health Antimicrobial Resistance Case Studies
The following examples illustrate antimicrobial resistance problems that arise when the same classes of antimicrobials are used in humans and animals, and the challenges that arise from competing interests and imbalances of risk and benefit in various sectors.
3.1. Third Generation Cephalosporins
Third generation cephalosporins are broad spectrum beta-lactam antimicrobials that are widely used in humans and animals. In people, cefotaxime, ceftriaxone and several other members of the class are used for a wide variety of frequently serious infections, particularly in hospital settings, for example bloodstream infections due to Escherichia coli and other bacteria, but also in community settings, for example Neisseria gonorrhea [47]. Third generation cephalosporins are classified as “critically important” for human health [47].
Ceftiofur is the principal third generation cephalosporin for veterinary use; others include cefpodoxime, cefoperazone and cefovecin. Ceftiofur is injected and used in animals as therapy to treat pneumonia, arthritis, septicemia and other conditions [48,49]. However ceftiofur is also used in mass therapy (metaphylaxis or prophylaxis), either under an approved label claim (e.g., injection of feedlot cattle for control of bovine respiratory disease), or off-label (e.g., injection of hatching eggs or day-old chicks for prevention of E. coli infections). Factors that encourage overuse of ceftiofur are its broad spectrum activity, zero withdrawal time for milk from dairy animals (due to its high maximum residual level; MRL), and availability of a long-acting preparation [48,49].
In Europe, approximately 14 tons of third and fourth generation cephalosporins were used in 2014 for use in animals [28]. Similar volumes are used in the US [50]. In many countries, cephalosporins are commonly used in humans but with wide variations. Overall, 101 tons of third generation cephalosporins were used in people Europe in 2012 [29] and in the US, approximately 82 tons in 2011 [51].
Resistance to the third generation cephalosporins is mainly mediated by extended-spectrum beta-lactamases (ESBLs) and AmpC beta-lactamases [47]. ESBL genes are highly mobile and transmitted on plasmids, transposons and other genetic elements. AmpC beta-lactamases were originally reported to be chromosomal but have also been identified on plasmids and to have spread horizontally among Enterobacteriaceae [47]. Unfortunately, in many countries resistance to third generation cephalosporins is now common among E. coli and K. pneumonia [52,53]. Resistance genes are frequently co-located with genes encoding resistance to other classes of antimicrobials, including tetracyclines, aminoglycosides and sulfonamides. As a consequence, the use of other antimicrobials in animals, for example tetracyclines administered in feed, can select for ESBL strains of bacteria [54].
Ceftiofur can be administered to eggs or day-old chicks in hatcheries, using automated equipment that injects small quantities of the drug into the many thousands of hatching eggs or chicks intended for treated flocks as prophylaxis against E. coli infections [55,56]. This practice selected for cephalosporin resistance in Salmonella Heidelberg, an important cause of human illness and associated with consumption of poultry products [57]. Surveillance detected a high degree of time-related correlations in trends of resistance to ceftiofur (and ceftriaxone, a drug of choice for treatment of severe cases of salmonellosis in children and pregnant women) among Salmonella Heidelberg from clinical infections in humans, from poultry samples collected at retail, and in E. coli from retail poultry samples [55]. Voluntary termination of ceftiofur use in hatcheries in Quebec was followed by a precipitous drop in the prevalence of resistance to ceftiofur. Subsequent re-introduction of its use, was followed by a return to higher prevalence of resistance [56]. In recognition of the resultant human health risks, in 2014, the Canadian poultry industry placed a voluntary ban on the use of ceftiofur and other critically important antimicrobials for disease prophylaxis [58].
In Japan, voluntary withdrawal of the off-label use of ceftiofur in hatcheries in 2012 was also followed by a significant decrease in broad-spectrum cephalosporin resistance in E. coli from broilers [59]. Some other countries (e.g., Denmark and Australia) have also placed voluntary restrictions in its use [60]. The label claim for day-old injection of poultry flocks was withdrawn in Europe, while some countries banned off-label use of third generation cephalosporins (e.g., U.S.) [48,61], and in other countries there is a requirement that use is restricted to situations where no other effective approved drugs are available for treatment [62].
3.2. Colistin
Colistin is in the polymyxin class of antimicrobials, and has been used in both people and animals for over 50 years [63]. Polymyxins, when administered systemically, frequently cause nephrotoxicity and neurotoxicity in people [64]. Thus, until recently its use was mainly limited to topical use and the treatment of infections in cystic fibrosis patients by inhalation (with a colistimethate sodium).
Colistin however is now used much more frequently, as a drug of last resort by injection, for treatment of multi-resistant gram-negative infections including carbapenem-resistant Pseudomonas aeruginosa and E. coli [65,66,67]. Where approved for use in food animals (e.g., Brazil, Europe, China), most colistin is administered orally to groups of pigs, poultry and in some cases calves, for treatment and prophylaxis of diarrhea due to gram-negative infections or for growth promotion [63,67,68]. In countries where data are available, the quantities consumed for animal production vastly exceed those used in humans and is very variable between countries [69]. In 2013 total animal consumption in Europe was 495 tons; 99.7% in oral form (e.g., for oral solution, medicated feed premix and oral powder) [63]. In China, the world’s largest producer of pigs and poultry, an estimated 12,000 tons of colistin was used in food animals [68].
Until recently, limited data on colistin resistance were available, partly because of technical difficulties in phenotypic susceptibility testing [63,70]. In Europe in 2016, resistance was found in 1.9% of indicator E. coli from broilers, 3.9% from broiler meat, 6.1% from turkeys and 10.1% from turkey meat [71]. Colistin resistance was thought limited to chromosomal mutation and was essentially non-transferable [63], however in 2015 the transferable plasmid-mediated colistin resistance gene, mcr-1, was found in E. coli isolates obtained from animals, food and human bloodstream infections from China [68]. Spread of the gene by conjugation has been shown in Klebsiella pneumoniae, Enterobacter aerogenes, Enterobacter spp. and P. aeruginosa [68]. Retrospective analyses have demonstrated the mcr-1 gene in several bacterial species isolated from humans, animals and environmental samples in numerous countries [72,73,74,75,76], and the gene was found in about 5% of healthy travelers [77]. The earliest identification of the gene thus far was in E. coli from poultry collected in the 1980s in China [78]. The mcr-1 gene has also been detected in isolates obtained from wildlife and surface water samples, demonstrating environmental contamination [79]. Recently, other plasmid-mediated colistin resistance genes has been reported for example mcr-2 in E. coli from pigs in Belgium [80].
Colistin illustrates some important One Health dimensions of antimicrobial resistance that differ from those of third generation cephalosporins. The toxicity with systemic use and the availability of other safer and more effective antimicrobials, meant for many years colistin was mainly used topically in people. However with the emergence of multi-drug resistance in many Gram-negative bacteria, there has been increasing need for this drug to systemically treat severe, life-threatening infections in humans in many countries. The colistin case demonstrates (once again) that using large quantities antimicrobials for group treatments or growth promotion in animals can lead to significant antimicrobial resistance problems for human health, even if the drug class is initially believed to be of lesser importance, because the relative importance of antimicrobials to human health can change. This is the same problem that arose from using avoparcin as a growth promoter until it was banned; it selected for resistance to another glycopeptide, vancomycin, which is used for the treatment of life-threatening MRSA (methicillin resistant Staphylococcus aureus) and for treating serious enterococcal infections (the latter especially in penicillin allergic patients) [81,82].
4. Risks to Public Health and Animal Health
Antimicrobial resistance is harmful to health because it reduces the effectiveness of antimicrobial therapy and tends to increase the severity, incidence and costs of infection [3,83]. There is now considerable evidence that antimicrobial use in animals is an important contributor to antimicrobial resistance among some pathogens of humans, in particular, common enteric pathogens such as Salmonella spp., Campylobacter spp., Enterococcus spp. and E. coli [6,18,26,38,41].
Non-typhoidal Salmonella (NTS) are among the most common bacteria isolated from foodborne infections of humans. Globally, there are approximately 94 million cases, including 155,000 deaths each year [1]. Animals are the most important reservoirs of NTS for humans [38,84,85,86]. Fecal shedding by carrier animals is an important source of antimicrobial resistant Salmonella contamination of meat and poultry products [38], and may also be responsible for fruit and vegetable contamination through fecal contamination of the environment [87]. Salmonella resistance to any medically important antimicrobial is of concern, but particularly to those critically important to human health, such as cephalosporins and fluoroquinolones [38,41,56]. Therapy in some groups (e.g., children and pregnant women) can be very restricted and beta-lactams such as third generation cephalosporins often may be the only therapy available to treat serious infections.
From the One Health antimicrobial resistance perspective, the third generation cephalosporins are good examples of antimicrobials that are considered critically important for both human and animal health. The main concern regarding selection and spread of resistance from animals to humans is their use as mass medications in large numbers of animals, either for therapy or prophylaxis. There are parallels with fluoroquinolones, another class of critically important antimicrobials, to which resistance among Campylobacter jejuni emerged following mass medication of poultry flocks [88,89,90]. In Australia where fluoroquinolones were never approved in food animals, fluoroquinolone resistant strains in food animals remain very rare [91].
Fluoroquinolone use in food animals is also linked to quinolone resistance in Salmonella [41,92,93,94]. Surveillance data compiled by WHO indicate that rates of fluoroquinolone resistance in non-typhoidal Salmonella vary widely by geographical region. For example, rates are relatively low in Europe (2–3%), higher in the Eastern Mediterranean region (up to 40–50%) and wide ranging in the Americas (0–96%) (1). Many Salmonella are also resistant to antimicrobials that have long been used as growth promoters in many countries (e.g., Canada, USA) including tetracyclines, penicillins and sulfonamides [41,84]. Antimicrobial resistance in some of the more virulent Salmonella serovars (e.g., Heidelberg, Newport, Typhimurium) has been associated with more severe infections in humans [38,83,86,95]. Resistance to other critically important antimicrobials continues to emerge in Salmonella, for example, a carbapenem resistant strain of Salmonella was identified on a pig farm that routinely administered prophylactic cephalosporin (ceftiofur) to piglets [96].
Escherichia coli are important pathogens of both humans and animals. In humans, E. coli are a common cause of serious bacterial infections, including enteritis, urinary tract infection and bloodstream infections [97,98,99]. Currently in England the rate for blood stream infections is about 64 cases per 100,000 per year and rising. A large and increasing proportion involves antimicrobial resistance, including fluoroquinolone resistance [100]. These higher rates are also being seen in countries with good surveillance systems in place, for example Denmark [60].
Many E. coli appear to behave as commensals of the gut of animals and humans, but may be opportunistic pathogens as well as donors of resistance genetic elements for pathogenic E. coli or other species of bacteria [101,102]. Although antimicrobial resistance is a rapidly increasing problem in E. coli infections of both animals and humans, the problem is better documented for isolates from human infections, where resistance is extensive, particularly in developing countries [1,103]. Humans are regularly exposed to antimicrobial resistant E. coli through foods and inadequately treated drinking water [104,105].
Travelers from developed countries are at risk of acquiring multi-resistance E. coli from other people or contaminated food and/or water [97,105,106]. There are now serious problems with extended spectrum beta lactamase (ESBL) E. coli in both developing and developed countries and foods from animals, in particular poultry, have been implicated as sources for humans [99,107,108], although the magnitude of the contribution from food animals is uncertain [102,103,104].
Given the critical importance of third and fourth generation cephalosporins and fluoroquinolones to human medicine and the clear evidence that treatment of entire groups of animals selects for resistance in important pathogens that spread from animals to humans [56,90], these drugs should be used rarely, if at all in animals, and only when supporting laboratory data demonstrate that no suitable alternatives of lesser human health importance are available. Their use as mass medications should be restricted.
Serious staphylococcal infections in people are common, including with Methicillin-resistant Staphylococcus aureus (MRSA) in both community and hospital settings, causing skin, wound, bloodstream and other types of infection [1,109,110,111]. Staphylococcus aureus and other staphylococci are also recognized pathogens of animals, for example they are responsible for cases of mastitis in cattle, and skin infections in pigs and companion animals [112,113]. MRSA were until recently relatively rare in animals but strains pathogenic to humans have emerged in several animal species [113,114,115,116]. Transmission to humans is thought currently to be mainly through contact with carrier animals [116]. The predominant strain isolated from animals is sequence type (ST) 398, and while pathogenic to humans, it is not considered a major epidemic strain [112,113]. Antimicrobial use in livestock, as well as lapses in biosecurity within and between farms, and international trade in animals, food or other products, are factors contributing to the spread of this pathogen in animals [113,117].
5. One Health Considerations from the Environment
One Health includes consideration of the environment as well as human and animal health [23,111]. The ecological nature of antimicrobial resistance is a reflection and consequence of the interconnectedness and diversity of life on the planet [22]. Many pathogenic bacteria, the antimicrobials that we use to treat them, and genes that confer resistance, have environmental origins (e.g., soil) [8,14,20]. Some important resistance genes, such as beta lactamases, are millions of years old [14,15]. Soil and other environmental matrices are rich sources of highly diverse populations of bacteria and their genes [14,118]. Antimicrobial resistance to a wide variety of drugs has been demonstrated in environmental bacteria isolated from the pre-antibiotic era, as well as from various sites (e.g., caves) free of other sources of exposure to modern antimicrobials [8,15,111,119]. Despite having ancient origins, there is abundant evidence that human activity has an impact on the resistome, which is the totality of resistance genes in the wider environment [13,14,118,119]. Hundreds of thousands of tons of antimicrobials are produced annually and find their way into the environment [18,27]. Waste from treatment plants and pharmaceutical industry, particularly if inadequately treated, can release high concentrations of antimicrobials into surface water [18,19,120,121]. Residues of antimicrobials are constituents of human sewage, livestock manure, and aquaculture, along with fecal bacteria and resistance genes [118,122,123,124,125]. Sewage treatment and composting of manure reduce concentrations of some but not all antimicrobials and microorganisms, which are introduced to soil upon land application of human and animal bio-solids [126].
Various environmental pathways are important routes of human exposure to resistant bacteria and their genes from animal and plant reservoirs [18,96,127] and provide opportunities for better regulations to control antimicrobial resistance. In developed countries with good quality sewage and drinking water treatment, and where most people have little to no direct contact with food-producing animals, transmission of bacteria and resistance genes from agricultural sources is largely foodborne, either from direct contamination of meat and poultry during slaughter and processing, or indirectly from fruit and vegetables contaminated by manure or irrigation water [38,87,90].
In countries with poor sewage and water treatment, drinking water is likely to be very important in transmission of resistant bacteria and/or genes from animals [11,97,111,120]). Poor sanitation also facilitates indirect person–person waterborne transmission of enteric bacteria among residents as well as international travelers who then return home colonized with resistant bacteria acquired locally [103,128]. Through these and other means, including globalized trade in animals and food, and long-distance migratory patterns of wildlife, antimicrobial resistant bacteria are globally disseminated.
General measures to address antimicrobial resistance in the wider environment include improved controls on pollution from industrial, residential and agricultural sources. Improved research as well as environmental monitoring and risk assessment is required to better understand the role of the environment in selection and spread of antimicrobial resistance, and to identify more specific measures to address resistance in this sector [12,14,18,100,103,129].
6. One Health Strategies to Address Antimicrobial Resistance
WHO and other international agencies (e.g., Food and Agriculture Organization (FAO), World Organization for Animal Health (OIE)), along with many individual countries, have developed comprehensive action plans to address the antimicrobial resistance crisis [5,130,131,132,133,134,135,136]. The WHO Global Action Plan seeks to address five major objectives that comprise the subtitles of the following sections. The WHO Plan embraces a One Health approach to address antimicrobial resistance, and it calls on member countries to do the same when developing their own action plans (6). There are five main pillars to the WHO Global Plan:
- Improve Awareness and Understanding of Antimicrobial Resistance through Effective Communication, Education and Training
- Strengthen the Knowledge and Evidence Base through Surveillance and Research
- Reduce the Incidence of Infection through Effective Sanitation, Hygiene and Infection Prevention Measures
- Optimize the Use of Antimicrobial Medicines in Human and Animal Health
- Develop the Economic Case tor Sustainable Investment that Takes Account of the Needs of All Countries, and Increase Investment in New Medicines, Diagnostic Tools, Vaccines and Other Interventions
The One Health approach laid out in the WHO Global Action Plan is appropriate and consistent with statements made in action plans from other international and national organizations. There is however, a long way to go before a fully integrated One Health approach to antimicrobial resistance is implemented at country and global levels. Among the numerous barriers to overcome include the competing interests among multiple sectors (involving animals, humans, and environment) and organizations, agreement on priorities for action, and gaps in antimicrobial resistance surveillance, antimicrobial use policy, and infection control in many parts of the world.
7. Conclusions
History has shown that it is not feasible to neatly separate antimicrobial classes into those exclusively for use in human or non-human sectors, with the exception of new antimicrobial classes. These should probably be reserved for use in humans as long as there are few or no alternatives available. The majority of classes, however, will be available for use in both sectors and the challenge for One Health is to ensure that use of these drugs is optimal overall. This is likely to be achieved when antimicrobials used in both sectors are used for therapy, only rarely for prophylaxis and never for growth promotion, and when we better control the types and amounts of antimicrobials plus the numbers of resistant bacteria we allow to be placed into the environment. What is vitally important is that we do more to stop the spread of resistant bacteria—not only from person to person but between and within the human and agriculture sectors and the environment, giving particular emphasis to controls of contaminated water.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization (WHO). Antimicrobial Resistance: Global Report on Surveillance; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Centers for Disease Control (CDC). Antibiotic Resistance Threats in the United States; CDC: Atlanta, GA, USA, 2013.
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations the Review On Antimicrobial Resistance. 2016. Available online: https://amr-review.org/sites/default/files/160525_Final paper_with cover.pdf (accessed on 15 January 2019).
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.M.; Wertheim, H.F.L.; Sumpradit, N.; Vlieghe, E.; Hara, G.L.; Gould, I.M.; Goossens, H.; et al. Antibiotic Resistance—The Need for Global Solutions. Lancet Infect. Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Action Plan on Antimicrobial Resistance; WHO: Geneva, Switzerland, 2015; Available online: http://www.wpro.who.int/entity/drug_resistance/resources/global_action_plan_eng.pdf (accessed on 15 January 2019).
- Aarestrup, F.M.; Wegener, H.C.; Collignon, P. Resistance in Bacteria of The Food Chain: Epidemiology and Control Strategies. Expert Rev. Anti-Infect. Ther. 2008, 6, 733–750. [Google Scholar] [CrossRef]
- Collignon, P.; Beggs, J.J.; Walsh, T.R.; Gandra, S.; Laxminarayan, R. Anthropological and Socioeconomic Factors Contributing to Global Antimicrobial Resistance: A Univariate and Multivariable Analysis. Lancet Planet Heal. 2018, 2, e398–e405. [Google Scholar] [CrossRef]
- Holmes, A.H.; Moore, L.S.P.; Sundsfjord, A.; Steinbakk, M.; Regmi, S.; Karkey, A.; Guerin, P.J.; Piddock, L.J. Understanding the Mechanisms and Drivers of Antimicrobial Resistance. Lancet 2016, 387, 176–187. [Google Scholar] [CrossRef]
- Burow, E.; Käsbohrer, A. Risk Factors for Antimicrobial Resistance in Escherichia coli in Pigs Receiving Oral Antimicrobial Treatment: A Systematic Review. Microb. Drug Resist. 2017, 23, 194–205. [Google Scholar] [CrossRef] [PubMed]
- Marti, E.; Variatza, E.; Balcazar, J.L. The Role of Aquatic Ecosystems as Reservoirs of Antibiotic Resistance. Trends Microbiol. 2014, 22, 36–41. [Google Scholar] [CrossRef]
- Bürgmann, H.; Frigon, D.; Gaze, W.H.; Manaia, C.M.; Pruden, A.; Singer, A.C.; Smets, B.F.; Zhang, T. Water and Sanitation: An Essential Battlefront in the War on Antimicrobial Resistance. FEMS Microbiol. Ecol. 2018, 94, fiy101. [Google Scholar] [CrossRef]
- Huijbers, P.M.C.; Blaak, H.; de Jong, M.C.M.; Graat, E.A.M.; Vandenbroucke-Grauls, C.M.J.E.; de Roda Husman, A.M. Role of the Environment in the Transmission of Antimicrobial Resistance to Humans: A Review. Environ. Sci. Technol. 2015, 49, 11993–12004. [Google Scholar] [CrossRef]
- Anonymous. Initiatives for Addressing Antimicrobial Resistance in the Environment: Current Situation and Challenges. 2018. Available online: https://wellcome.ac.uk/sites/default/files/antimicrobial-resistance-environment-report.pdf (accessed on 15 January 2019).
- Gaze, W.H.; Krone, S.M.; Larsson, D.G.J.; Li, X.-Z.; Robinson, J.A.; Simonet, P.; Smalla, K.; Timinouni, M.; Topp, E.; Wellington, E.M.; et al. Influence of Humans on Evolution and Mobilization of Environmental Antibiotic Resistome. Emerg. Infect. Dis. 2013, 19, e120871. [Google Scholar] [CrossRef]
- Perry, J.A.; Wright, G.D. Forces Shaping the Antibiotic Resistome. BioEssays 2014, 36, 1179–1184. [Google Scholar] [CrossRef]
- Woolhouse, M.E.J.; Ward, M.J. Sources of Antimicrobial Resistance. Science 2013, 341, 1460–1461. [Google Scholar] [CrossRef]
- Heuer, O.E.; Kruse, H.; Grave, K.; Collignon, P.; Karunasagar, I.; Angulo, F.J. Human Health Consequences of Use of Antimicrobial Agents in Aquaculture. Clin. Infect. Dis. 2009, 49, 1248–1253. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, J. Antimicrobials in Agriculture and the Environment: Reducing Unnecessary Use and Waste. The Review on Antimicrobial Resistance. 2015. Available online: https://amr-review.org/sites/default/files/Antimicrobials in agriculture and the environment—Reducing unnecessary use and waste.pdf (accessed on 15 January 2019).
- So, A.D.; Shah, T.A.; Roach, S.; Ling Chee, Y.; Nachman, K.E. An Integrated Systems Approach is Needed to Ensure the Sustainability of Antibiotic Effectiveness for Both Humans and Animals. J. Law Med. Ethics 2015, 43, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Collignon, P. The Importance of a One Health Approach to Preventing the Development and Spread of Antibiotic Resistance. In One Health: The Human-Animal-Environment Interfaces in Emerging Infectious Diseases: Food Safety and Security, and International and National Plans for Implementation of One Health Activities; Mackenzie, J.S., Jeggo, M., Daszak, P., Richt, J.A., Eds.; Springer: Berlin/Heidelberg, Germany, 2013; pp. 19–36. [Google Scholar]
- Torren-Edo, J.; Grave, K.; Mackay, D. “One Health”: The Regulation and Consumption of Antimicrobials for Animal Use in the EU. IHAJ 2015, 2, 14–16. [Google Scholar]
- Robinson, T.P.; Bu, D.P.; Carrique-Mas, J.; Fèvre, E.M.; Gilbert, M.; Grace, D.; Hay, S.I.; Jiwakanon, J.; Kakkar, M.; Kariuki, S.; et al. Antibiotic Resistance is the Quintessential One Health Issue. Trans. R. Soc. Trop. Med. Hyg. 2016, 110, 377–380. [Google Scholar] [CrossRef] [PubMed]
- Zinsstag, J.; Meisser, A.; Schelling, E.; Bonfoh, B.; Tanner, M. From ‘Two Medicines’ to ‘One Health’ and Beyond. Onderstepoort J. Vet. Res. 2012, 79, a492. [Google Scholar] [CrossRef]
- World Health Organization. One Health. 2017. Available online: https://www.who.int/features/qa/one-health/en/ (accessed on 15 January 2019).
- One Health Commission. What is One Health? 2018. Available online: https://www.onehealthcommission.org/en/why_one_health/what_is_one_health/ (accessed on 15 January 2019).
- McEwen, S.A.; Fedorka-Cray, P.J. Antimicrobial Use and Resistance in Animals. Clin. Infect. Dis. 2002, 34, S93–S106. [Google Scholar] [CrossRef]
- Van Boeckel, T.P.; Brower, C.; Gilbert, M.; Grenfell, B.T.; Levin, S.A.; Robinson, T.P.; Teillant, A.; Laxminarayan, R. Global Trends in Antimicrobial Use in Food Animals. Proc. Natl. Acad. Sci. USA 2015, 112, 5649–5654. [Google Scholar] [CrossRef]
- European Medicines Agency (EMA). Sales of Veterinary Antimicrobial Agents in 29 European Countries in 2014; EMA: London, UK, 2016. [Google Scholar]
- ECDC (European Centre for Disease Prevention and Control); EFSA (European Food Safety Authority); EMA (European Medicines Agency). ECDC/EFSA/EMA First Joint Report on The Integrated Analysis of The Consumption of Antimicrobial Agents and Occurrence of Antimicrobial Resistance in Bacteria from Humans and Food-Producing Animals. EFSA J. 2015, 13, 4006. [Google Scholar] [CrossRef]
- Food and Agriculture Organization (FAO). Drivers, Dynamics and Epidemiology of Antimicrobial Resistance in Animal Oroduction. 2016. Available online: http://www.fao.org/3/a-i6209e.pdf (accessed on 15 January 2019).
- Vidaver, A.K. Uses of Antimicrobials in Plant Agriculture. Clin. Infect. Dis. 2002, 34, S107–S110. [Google Scholar] [CrossRef]
- Sundin, G.W.; Wang, N. Antibiotic Resistance in Plant-Pathogenic Bacteria. Annu. Rev. Phytopathol. 2018, 56, 161–180. [Google Scholar] [CrossRef] [PubMed]
- Collignon, P. Use of Critically Important Antimicrobials in Food Production. In Kucers’ The Use of Antibiotics: A Clinical Review of Antibacterial, Antifungal, Antiparasitic and Antivral Drugs, 7th ed.; Grayson, L., Ed.; American Society for Microbiology and CRC Press: Boca Raton, FL, USA, 2018; pp. 9–18. [Google Scholar]
- Sykes, J.E. Antimicrobial Drug Use in Dogs and Cats. In Antimicrobial Therapy in Veterinary Medicine, 5th ed.; Giguère, S., Prescott, J.F., Dowling, P.M., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2013; pp. 473–494. [Google Scholar]
- Giguère, S.; Abrams-Ogg, A.C.G.; Kruth, S.A. Prophylactic Use of Antimicrobial Agents, and Antimicrobial Chemotherapy for the Neutropenic Patient. In Antimicrobial Therapy in Veterinary Medicine, 5th ed.; Giguère, S., Prescott, J.F., Dowling, P.M., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2013; pp. 357–378. [Google Scholar]
- National Research Council. The Use of Drugs in Food Animals: Benefits and Risks; The National Academies Press: Washington, DC, USA, 1999. [Google Scholar]
- Murphy, D.; Ricci, A.; Auce, Z.; Beechinor, J.G.; Bergendahl, H.; Breathnach, R.; Bures, J.; Pedro, J.; da Silva, D.; Hederová, J.; et al. EMA and EFSA Joint Scientific Opinion on Measures to Reduce the Need to Use Antimicrobial Agents in Animal Husbandry in the European Union, and the Resulting Impacts on Food Safety (RONAFA). EFSA J. 2017, 15, 4666. [Google Scholar]
- Food and Agriculture Organization (FAO); World Organisation for Animal Health (OIE); World Health Organization (WHO) (FAO/OIE/WHO). Joint FAO/OIE/WHO Expert Workshop on Non-Human Antimicrobial Usage and Antimicrobial Resistance: Scientific Assessment; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Food and Agriculture Organization (FAO); World Health Organization (WHO). FAO/WHO Expert Meeting on Foodborne Antimicrobial Resistance: Role of Environment, Crops and Biocides. Summary Report; FAO: Rome, Italy, 2018. [Google Scholar]
- Zuraw, L. Perdue Announces Dramatic Reduction in Antibiotic Use in its Chickens. Food Safety News. 2014. Available online: http://www.foodsafetynews.com/2014/09/perdue-dramatically-reduces-antibiotic-use-in-chickens/#.WjLZulQ-dTZ (accessed on 15 January 2019).
- World Health Organization (WHO). Impacts of Antimicrobial Growth Promoter Termination in Denmark. The WHO International Review Panel’s Evaluation of the Termination of the Use of Antimicrobial Growth Promoters in Denmark; WHO: Foulum, Denmark, 2003. [Google Scholar]
- World Health Organization (WHO). The Medical Impact of the Use of Antimicrobials in Food Animals; WHO: Berlin, Germany, 1997. [Google Scholar]
- European Union (EU). Guidelines for the Prudent Use of Antimicrobials in Veterinary Medicine (2015/C 299/04). Off. J. Eur. Union 2015, C299, C299:7–C299:26. [Google Scholar]
- Food and Drug Administration (FDA). Guidance for Industry #213. New Animal Drugs and New Animal Drug Combination Products Administered in or on Medicated Feed or Drinking Water of Food-Producing Animals: Recommendations for Drug Sponsors for Voluntarily Aligning Product Use Conditions with GFI #209; FDA: Rockville, MD, USA, 2013.
- Mehrotra, M.; Li, X.-Z.; Ireland, M.J. Enhancing Antimicrobial Stewardship by Strengthening the Veterinary Drug Regulatory Framework. Can. Commun. Dis. Rep. 2017, 43, 220–223. [Google Scholar] [CrossRef]
- World Organisation for Animal Health (OIE). OIE Annual Report on Antimicrobial Agents Intended for Use in Animals. Second Report; OIE: Paris, France, 2018; Available online: http://www.oie.int/fileadmin/Home/eng/Our_scientific_expertise/docs/pdf/AMR/Annual_Report_AMR_2.pdf (accessed on 15 January 2019).
- WHO Advisory Group on Integrated Surveillance of Antimicrobial Resistance (AGISAR). Critically Important Antimicrobials for Human Medicine; 4th revision 2013; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- European Medicines Agency (EMA). Revised Reflection Paper on the Use of 3rd and 4th Generation Cephalosporins in Food Producing Animals in the European Union: Development of Resistance and Impact on Human and Animal Health; EMA: London, UK, 2009. [Google Scholar]
- Prescott, J.F. Beta-lactam Antibiotics. In Antimicrobial Therapy in Veterinary Medicine, 5th ed.; Giguère, S., Prescott, J.F., Dowling, P.M., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2013; pp. 153–173. [Google Scholar]
- Food and Drug Administration (FDA). 2017 Summary Report on Antimicrobials Sold or Distributed for Use in Food-Producing Animals; FDA: Washington, DC, USA, 2018.
- Food and Drug Administration (FDA). Drug Use Review. Food and Drug Administration, Department of Health and Human Services; FDA: Washington, DC, USA, 2012. Available online: http://www.fda.gov/downloads/Drugs/DrugSafety/InformationbyDrugClass/UCM319435.pdf (accessed on 15 January 2019).
- de Kraker, M.E.A.; Wolkewitz, M.; Davey, P.G.; Koller, W.; Berger, J.; Nagler, J.; Icket, C.; Kalenic, S.; Horvatic, J.; Seifert, H.; et al. Burden of Antimicrobial Resistance in European Hospitals: Excess Mortality and Length of Hospital Stay Associated with Bloodstream Infections due to Escherichia coli Resistant to Third-Generation Cephalosporins. J. Antimicrob. Chemother. 2011, 66, 398–407. [Google Scholar] [CrossRef]
- Park, S.H. Third-Generation Cephalosporin Resistance in Gram-Negative Bacteria in the Community: A Growing Public Health Concern. Korean J. Intern. Med. 2014, 29, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Kanwar, N.; Scott, H.M.; Norby, B.; Loneragan, G.H.; Vinasco, J.; McGowan, M.; Cottell, J.L.; Chengappa, M.M.; Bai, J.; Boerlin, P. Effects of Ceftiofur and Chlortetracycline Treatment Strategies on Antimicrobial Susceptibility and on tet(A), tet(B), and blaCMY-2 Resistance Genes among E. coli Isolated from the Feces of Feedlot Cattle. PLoS ONE 2013, 8, e80575. [Google Scholar] [CrossRef]
- Canadian Integrated Program for Antimicrobial Resistance (CIPARS). Salmonella Heidelberg—Ceftiofur-Related Resistance in Human and Retail Chicken Isolates. 2009. Available online: http://www.phac-aspc.gc.ca/cipars-picra/heidelberg/pdf/heidelberg_e.pdf (accessed on 15 January 2019).
- Dutil, L.; Irwin, R.; Finley, R.; Ng, L.K.; Avery, B.; Boerlin, P.; Bourgault, A.M.; Cole, L.; Daignault, D.; Desruisseau, A.; et al. Ceftiofur Resistance in Salmonella enterica Serovar Heidelberg From Chicken Meat and Humans, Canada. Emerg. Infect. Dis. 2010, 16, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.E.; Medus, C.; Meyer, S.D.; Boxrud, D.J.; Leano, F.; Hedberg, C.W.; Elfering, K.; Braymen, C.; Bender, J.B.; Danila, R.N. Outbreaks of Salmonellosis in Minnesota (1998 through 2006) Associated with Frozen, Microwaveable, Breaded, Stuffed Chicken Products. Vol. 71. J. Food Prot. 2008, 71, 2153–2160. [Google Scholar] [CrossRef] [PubMed]
- Chicken Farmers of Canada. Antibiotics. 2018. Available online: https://www.chickenfarmers.ca/antibiotics/ (accessed on 15 January 2019).
- Hiki, M.; Kawanishi, M.; Abo, H.; Kojima, A.; Koike, R.; Hamamoto, S.; Asai, T. Decreased Resistance to Broad-Spectrum Cephalosporin in Escherichia coli from Healthy Broilers at Farms in Japan After Voluntary Withdrawal of Ceftiofur. Foodborne Pathog. Dis. 2015, 12, 639–643. [Google Scholar] [CrossRef]
- DANMAP 2014. Use of Antimicrobial Agents and Occurrence of Antimicrobial Resistance in Bacteria from Food Animals, Food and Humans in Denmark. Statens Serum Institut, National Veterinary Institute, Technical University of Denmark, National Food Institute, Technical University of Denmark, 2015. Available online: https://www.danmap.org/downloads/reports.aspx (accessed on 15 January 2019).
- Department of Health and Human Services, Food and Drug Administration. 2012, 21 CFR Part 530 [Docket No. FDA–2008–N–0326] New Animal Drugs; Cephalosporin Drugs; Extra Label Animal Drug Use; Order of Prohibition. Fed. Regist. 2012, 77, 735–745. [Google Scholar]
- European Medicines Agency (EMA). Answers to the Request for Scientific Advice on the Impact on Public Health and Animal Health of the Use of Antibiotics in Animals. 2014. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/Other/2014/07/WC500170253.pdf (accessed on 15 January 2019).
- European Medicines Agency (EMA). Updated Advice on the Use of Colistin Products in Animals Within the European Union: Development of Resistance and Possible Impact on Human and Animal Health. In Committee for Medicinal Products for Veterinary use (CVMP), Committee for Medicinal Products; EMA: London, UK, 2016. [Google Scholar]
- Falagas, M.E.; Kasiakou, S.K. Toxicity of Polymyxins: A Systematic Review of the Evidence from Old and Recent Studies. Crit. Care 2006, 10, R27. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Kasiakou, S.K.; Saravolatz, L.D. Colistin: The Revival of Polymyxins for the Management of Multidrug-Resistant Gram-Negative Bacterial Infections. Clin. Infect. Dis. 2005, 40, 1333–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linden, P.K.; Kusne, S.; Coley, K.; Fontes, P.; Kramer, D.J.; Paterson, D. Use of Parenteral Colistin for the Treatment of Serious Infection Due to Antimicrobial-Resistant Pseudomonas aeruginosa. Clin. Infect. Dis. 2003, 37, e154–e160. [Google Scholar] [CrossRef]
- Fernandes, M.R.; Moura, Q.; Sartori, L.; Silva, K.C.; Cunha, M.P.V.; Esposito, F.; Lopes, R.; Otutumi, L.K.; Gonçalves, D.D.; Dropa, M.; et al. Silent Dissemination of Colistin-Resistant Escherichia coli in South America Could Contribute to the Global Spread of the mcr-1 Gene. Eurosurveillance 2016, 21. [Google Scholar] [CrossRef]
- Liu, Y.-Y.; Wang, Y.; Walsh, T.R.; Yi, L.-X.; Zhang, R.; Spencer, J.; Doi, Y.; Tian, G.; Dong, B.; Huang, X.; et al. Emergence of Plasmid-Mediated Colistin Rresistance Mechanism MCR-1 in Animals and Human Beings in China: A Microbiological and Molecular Biological Study. Lancet Infect. Dis. 2016, 16, 161–168. [Google Scholar] [CrossRef]
- European Centers for Disease Control and Prevention (ECDC). Summary of the Latest Data on Antibiotic Consumption in the European Union. Antibiotic Consumption in Europe; ECDC: Stockholm, Sweden, 2015.
- Landman, D.; Georgescu, C.; Martin, D.A.; Quale, J. Polymyxins Revisited. Clin. Microbiol. Rev. 2008, 21, 449–465. [Google Scholar] [CrossRef] [Green Version]
- European Food Safety Authority (EFSA), European Centre for Disease Prevention and Control (ECDC). The European Union Summary Report on Antimicrobial Resistance in Zoonotic and Indicator Bacteria from Humans, Animals and Food in 2016. EFSA J. 2018, 16, e05182. [Google Scholar]
- Catry, B.; Cavaleri, M.; Baptiste, K.; Grave, K.; Grein, K.; Holm, A.; Jukes, H.; Liebana, E.; Navas, A.L.; Mackay, D.; et al. Use of Colistin-Containing Products Within the European Union and European Economic Area (EU/EEA): Development of Resistance in Animals and Possible Impact on Human and Animal Health. Int. J. Antimicrob Agents 2015, 46, 297–306. [Google Scholar] [CrossRef]
- Prim, N.; Rivera, A.; Rodríguez-Navarro, J.; Español, M.; Turbau, M.; Coll, P.; Mirelis, B. Detection of mcr-1 Colistin Resistance Gene in Polyclonal Escherichia coli Isolates in Barcelona, Spain, 2012 to 2015. Eurosurveillance 2016, 21. [Google Scholar] [CrossRef]
- Irrgang, A.; Roschanski, N.; Tenhagen, B.-A.; Grobbel, M.; Skladnikiewicz-Ziemer, T.; Thomas, K.; Roesler, U.; Käsbohrer, A. Prevalence of mcr-1 in E. coli from Livestock and Food in Germany, 2010–2015. PLoS ONE 2016, 11, e0159863. [Google Scholar] [CrossRef]
- Hasman, H.; Hammerum, A.M.; Hansen, F.; Hendriksen, R.S.; Olesen, B.; Agersø, Y.; Zankari, E.; Leekitcharoenphon, P.; Stegger, M.; Kaas, R.S.; et al. Detection of mcr-1 Encoding Plasmid-Mediated Colistin-Resistant Escherichia coli Isolates from Human Bloodstream Infection and Imported Chicken Meat, Denmark 2015. Eurosurveillance 2015, 20. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; van Dorp, L.; Shaw, L.P.; Bradley, P.; Wang, Q.; Wang, X.; Jin, L.; Zhang, Q.; Liu, Y.; Rieux, A.; et al. The Global Distribution and Spread of the Mobilized Colistin Resistance Gene mcr-1. Nat. Commun. 2018, 9, 1179. [Google Scholar] [CrossRef]
- von Wintersdorff, C.J.H.; Wolffs, P.F.G.; van Niekerk, J.M.; Beuken, E.; van Alphen, L.B.; Stobberingh, E.E.; Oude Lashof, A.M.L.; Hoebe, C.J.P.A.; Savelkoul, P.H.M.; Penders, J. Detection of the Plasmid-Mediated Colistin-Resistance Gene mcr-1 in Faecal Metagenomes of Dutch Travellers. J. Antimicrob Chemother. 2016, 71, 3416–3419. [Google Scholar] [CrossRef]
- Shen, Z.; Wang, Y.; Shen, Y.; Shen, J.; Wu, C. Early Emergence of mcr-1 in Escherichia coli from Food-Producing Animals. Lancet Infect. Dis. 2016, 16, 293. [Google Scholar] [CrossRef]
- Zurfuh, K.; Poirel, L.; Nordmann, P.; Nüesch-Inderbinen, M.; Hächler, H.; Stephan, R. Occurrence of the Plasmid-Borne mcr-1 Colistin Resistance Gene in Extended-Spectrum-β-Lactamase-Producing Enterobacteriaceae in River Water and Imported Vegetable Samples in Switzerland. Antimicrob. Agents Chemother. 2016, 60, 2594–2595. [Google Scholar] [CrossRef] [PubMed]
- Xavier, B.B.; Lammens, C.; Ruhal, R.; Kumar-Singh, S.; Butaye, P.; Goossens, H.; Malhotra-Kumar, S. Identification of a Novel Plasmid-Mediated Colistin-Resistance Gene, mcr-2, in Escherichia coli, Belgium, June 2016. Eurosurveillance 2016, 21. [Google Scholar] [CrossRef]
- Levine, D.P. Vancomycin: A History. Clin. Infect. Dis. 2006, 42, S5–S12. [Google Scholar] [CrossRef]
- Bager, F.; Madsen, M.; Christensen, J.; Aarestrup, F.M. Avoparcin Used as a Growth Promoter is Associated with the Occurrence of Vancomycin-Resistant Enterococcus faecium on Danish Poultry and Pig Farms. Prev. Vet. Med. 1997, 31, 95–112. [Google Scholar] [CrossRef]
- Barza, M. Potential Mechanisms of Increased Disease in Humans from Antimicrobial Resistance in Food Animals. Clin. Infect. Dis. 2002, 34, S123–S125. [Google Scholar] [CrossRef]
- Anderson, E.S. Drug Resistance in Salmonella typhimurium and its Implications. Br. Med. J. 1968, 3, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Swann, M.M. The Use of Antibiotics in Animal Husbandry and Veterinary Medicine; HMSO: London, UK, 1969.
- Institute of Medicine. Human Health Risks with the Subtherapeutic Use of Penicillin or Tetracyclines in Animal Feed; The National Academies Press: Washington, DC, USA, 1989. [Google Scholar]
- Hanning, I.B.; Nutt, J.D.; Ricke, S.C. Salmonellosis Outbreaks in the United States Due to Fresh Produce: Sources and Potential Intervention Measures. Foodborne Pathog. Dis. 2009, 6, 635–648. [Google Scholar] [CrossRef] [PubMed]
- Endtz, H.; Ruijs, G.; van Klingeren, B.; Jansen, W.H.; Reijden, T.; Mouton, R.P. Quinolone Resistance in Campylobacter Isolated from Man and Poultry Following the Introduction of Fluoroquinolones in Veterinary Medicine. J. Antimicrob Chemother. 1991, 27, 199–208. [Google Scholar] [CrossRef] [PubMed]
- McDermott, P.F.; Bodeis, S.M.; English, L.L.; White, D.G.; WalkeR, R.D.; Zhao, S.; Simjee, S.; Wagne, D.D. Ciprofloxacin Resistance in Campylobacter jejuni Evolves Rapidly in Chickens Treated with Fluoroquinolones. J. Infect. Dis. 2002, 185, 837–840. [Google Scholar] [CrossRef]
- Nelson, J.M.; Chiller, T.M.; Powers, J.H.; Angulo, F.J. Fluoroquinolone-Resistant Campylobacter Species and the Withdrawal of Fluoroquinolones from Use in Poultry: A Public Health Success Story. Clin. Infect. Dis. 2007, 44, 977–980. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.C.; Turnidge, J.; Collignon, P.; Looke, D.; Barton, M.; Gottlieb, T. Control of Fluoroquinolone Resistance through Successful Regulation, Australia. Emerg. Infect. Dis. 2012, 18, 1453–1460. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Use of Quinolones in Food Animals and Potential Impact on Human Health; WHO: Geneva, Switzerland, 1998. [Google Scholar]
- Chiu, C.H.; Wu, T.L.; Su, L.H.; Chu, C.; Chia, J.H.; Kuo, A.J.; Chien, M.S.; Lin, T.Y. The Emergence in Taiwan of Fluoroquinolone Resistance in Salmonella enterica Serotype Choleraesuis. N. Engl. J. Med. 2002, 346, 413–419. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency (EMA). Reflection Paper on the Use of Fluoroquinolones in Food-Producing Animals in the European Union: Development of Resistance and Impact on Human and Animal Health; EMEA/CVMP/SAGAM/184651/2005; EMA: London, UK, 2006. [Google Scholar]
- Helms, M.; Simonsen, J.; Mølbak, K. Quinolone Resistance Is Associated with Increased Risk of Invasive Illness or Death during Infection with Salmonella Serotype Typhimurium. J. Infect. Dis. 2004, 190, 1652–1654. [Google Scholar] [CrossRef] [PubMed]
- Mollenkopf, D.F.; Stull, J.W.; Mathys, D.A.; Bowman, A.S.; Feicht, S.M.; Grooters, S.V.; Daniels, J.B.; Wittum, T.E. Carbapenemase-Producing Enterobacteriaceae Recovered from the Environment of a Swine Farrow-to-Finish Operation in the United States. Antimicrob. Agents Chemother. 2017, 61, e01298-16. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, K.; Collignon, P. Colonisation with Escherichia coli Resistant to “Critically Important” Antibiotics: A High Risk for International Travellers. Eur. J. Clin. Microbiol. Infect. Dis. 2010, 29, 1501–1506. [Google Scholar] [CrossRef]
- Laupland, K.B.; Church, D.L. Population-Based Epidemiology and Microbiology of Community-Onset Bloodstream Infections. Clin. Microbiol. Rev. 2014, 27, 647–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazarus, B.; Paterson, D.L.; Mollinger, J.L.; Rogers, B.A. Do Human Extraintestinal Escherichia coli Infections Resistant to Expanded-Spectrum Cephalosporins Originate From Food-Producing Animals? A Systematic Review. Clin. Infect. Dis. 2015, 60, 439–452. [Google Scholar] [CrossRef] [PubMed]
- Bou-Antoun, S.; Davies, J.; Guy, R.; Johnson, A.P.; Sheridan, E.A.; Hope, R.J. Descriptive Epidemiology of Escherichia coli Bacteraemia in England, April 2012 to March 2014. Eurosurveillance 2016, 21. [Google Scholar] [CrossRef] [PubMed]
- Hammerum, A.M.; Larsen, J.; Andersen, V.D.; Lester, C.H.; Skovgaard Skytte, T.S.; Hansen, F.; Olsen, S.S.; Mordhorst, H.; Skov, R.L.; Aarestrup, F.M.; et al. Characterization of Extended-Spectrum β-lactamase (ESBL)-Producing Escherichia coli Obtained from Danish Pigs, Pig farmers and Their Families from Farms with High or no Consumption of Third- or Fourth-Generation Cephalosporins. J. Antimicrob Chemother. 2014, 69, 2650–2657. [Google Scholar] [CrossRef] [PubMed]
- Collignon, P. Antibiotic Resistance: Are we all Doomed? Intern. Med. J. 2015, 45, 1109–1115. [Google Scholar] [CrossRef]
- Walsh, T.R.; Weeks, J.; Livermore, D.M.; Toleman, M.A. Dissemination of NDM-1 positive Bacteria in the New Delhi Environment and its Implications for Human Health: An Environmental Point Prevalence Study. Lancet Infect. Dis. 2011, 11, 355–362. [Google Scholar] [CrossRef]
- Graham, D.W.; Collignon, P.; Davies, J.; Larsson, D.G.J.; Snape, J. Underappreciated Role of Regionally Poor Water Quality on Globally Increasing Antibiotic Resistance. Environ. Sci. Technol. 2014, 48, 11746–11747. [Google Scholar] [CrossRef]
- Tängdén, T.; Cars, O.; Melhus, Å.; Löwdin, E. Foreign Travel Is a Major Risk Factor for Colonization with Escherichia coli Producing CTX-M-Type Extended-Spectrum β-Lactamases: A Prospective Study with Swedish Volunteers. Antimicrob. Agents Chemother. 2010, 54, 3564–3568. [Google Scholar] [CrossRef]
- Vieira, A.R.; Collignon, P.; Aarestrup, F.M.; McEwen, S.A.; Hendriksen, R.S.; Hald, T.; Wegener, H.C. Association Between Antimicrobial Resistance in Escherichia coli Isolates from Food Animals and Blood Stream Isolates From Humans in Europe: An Ecological Study. Foodborne Pathog. Dis. 2011, 8, 1295–1301. [Google Scholar] [CrossRef]
- De Been, M.; Lanza, V.F.; de Toro, M.; Scharringa, J.; Dohmen, W.; Du, Y.; Hu, J.; Lei, Y.; Li, N.; Tooming-Klunderud, A.; et al. Dissemination of Cephalosporin Resistance Genes between Escherichia coli Strains from Farm Animals and Humans by Specific Plasmid Lineages. PLOS Genet. 2014, 10, e1004776. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, L.; Kurbasic, A.; Skjøt-Rasmussen, L.; Ejrnæs, K.; Porsbo, L.J.; Pedersen, K.; Jensen, L.B.; Emborg, H.-D.; Agersø, Y.; Olsen, K.E.P.; et al. Escherichia coli Isolates from Broiler Chicken Meat, Broiler Chickens, Pork, and Pigs Share Phylogroups and Antimicrobial Resistance with Community-Dwelling Humans and Patients with Urinary Tract Infection. Foodborne Pathog. Dis. 2009, 7, 537–547. [Google Scholar] [CrossRef] [PubMed]
- ECDC (European Centre for Disease Prevention and Control); EFSA (European Food Safety Authority); EMA (European Medicines Agency). Joint Scientific Report of ECDC, EFSA and EMEA on Meticillin Resistant Staphylococcus aureus (MRSA) in Livestock, Companion Animals and Food. EFSA J. 2009, 7. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control (ECDC). Antimicrobial Resistance Surveillance in Europe 2014. Annual Report of the European Antimicrobial Resistance Surveillance Network (EARS-Net); ECDC: Stockholm, Sweden, 2015.
- Finley, R.L.; Collignon, P.; Larsson, D.G.J.; McEwen, S.A.; Li, X.-Z.; Gaze, W.H.; Reid-Smith, R.; Timinouni, M.; Graham, D.W.; Topp, E. The Scourge of Antibiotic Resistance: The Important Role of the Environment. Clin. Infect. Dis. 2013, 57, 704–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Price, L.B.; Stegger, M.; Hasman, H.; Aziz, M.; Larsen, J.; Andersen, P.S.; Pearson, T.; Waters, A.E.; Foster, J.T.; Schupp, J.; et al. Staphylococcus aureus CC398: Host Adaptation and Emergence of Methicillin Resistance in Livestock. mBio 2012, e00305-11. [Google Scholar] [CrossRef] [PubMed]
- Weese, J.S.; van Duijkeren, E. Methicillin-Resistant Staphylococcus aureus and Staphylococcus pseudintermedius in Veterinary Medicine. Vet. Microbiol. 2010, 140, 418–429. [Google Scholar] [CrossRef] [PubMed]
- Boost, M.V.; O’Donoghue, M.M.; Siu, K.H.G. Characterisation of Methicillin-Resistant Staphylococcus aureus Isolates from Dogs and Their Owners. Clin. Microbiol. Infect. 2007, 13, 731–733. [Google Scholar] [CrossRef]
- Lewis, H.C.; Mølbak, K.; Reese, C.; Aarestrup, F.M.; Selchau, M.; Sørum, M.; Skov, R.L. Pigs as Source of Methicillin-Resistant Staphylococcus aureus CC398 Infections in Humans, Denmark. Emerg. Infect. Dis. 2008, 14, 1383–1389. [Google Scholar] [CrossRef]
- Voss, A.; Loeffen, F.; Bakker, J.; Klaassen, C.; Wulf, M. Methicillin-Resistant Staphylococcus aureus in Pig Farming. Emerg. Infect. Dis. J. 2005, 11, 1965. [Google Scholar] [CrossRef]
- Dorado-Garcia, A.; Dohmen, W.; Bos, M.E.H.; Verstappen, K.M.; Houben, M.; Wagenaar, J.A.; Heederik, D.J. Dose-Response Relationship Between Antimicrobial Drugs and Livestock-Associated MRSA in Pig Farming. Emerg. Infect. Dis. 2015, 21, 950–959. [Google Scholar] [CrossRef]
- Ruuskanen, M.; Muurinen, J.; Meierjohan, A.; Parnanen, K.; Tamminen, M.; Lyra, C.; Kronberg, L.; Virta, M. Fertilizing with Animal Manure Disseminates Antibiotic Resistance Genes to the Farm Environment. J. Environ. Qual. 2016, 45, 488–493. [Google Scholar] [CrossRef]
- Wellington, E.M.H.; Boxall, A.B.; Cross, P.; Feil, E.J.; Gaze, W.H.; Hawkey, P.M.; Johnson-Rollings, A.S.; Jones, D.L.; Lee, N.M.; Otten, W.; et al. The Role of the Natural Environment in the Emergence of Antibiotic Resistance in Gram-Negative Bacteria. Lancet Infect. Dis. 2013, 13, 155–165. [Google Scholar] [CrossRef]
- Aubertheau, E.; Stalder, T.; Mondamert, L.; Ploy, M.-C.; Dagot, C.; Labanowski, J. Impact of Wastewater Treatment Plant Discharge on the Contamination of River Biofilms by Pharmaceuticals and Antibiotic Resistance. Sci. Total Environ. 2017, 579, 1387–1398. [Google Scholar] [CrossRef]
- Singer, A.C.; Shaw, H.; Rhodes, V.; Hart, A. Review of Antimicrobial Resistance in the Environment and Its Relevance to Environmental Regulators. Front. Microbiol. 2016, 7, 1728. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, L.; Manaia, C.; Merlin, C.; Schwartz, T.; Dagot, C.; Ploy, M.C.; Michael, I.; Fatta-Kassinos, D. Urban Wastewater Treatment Plants as Hotspots for Antibiotic Resistant Bacteria and Genes Spread into the Environment: A Review. Sci. Total Environ. 2013, 447, 345–360. [Google Scholar] [CrossRef]
- Zhang, Q.-Q.; Ying, G.-G.; Pan, C.-G.; Liu, Y.-S.; Zhao, J.-L. Comprehensive Evaluation of Antibiotics Emission and Fate in the River Basins of China: Source Analysis, Multimedia Modeling, and Linkage to Bacterial Resistance. Environ. Sci. Technol. 2015, 49, 6772–6782. [Google Scholar] [CrossRef] [PubMed]
- Cabello, F.C.; Godfrey, H.P.; Buschmann, A.H.; Dölz, H.J. Aquaculture as yet Another Environmental Gateway to the Development and Globalisation of Antimicrobial Resistance. Lancet Infect. Dis. 2016, 16, e127–e133. [Google Scholar] [CrossRef]
- Wang, H.; Yang, J.; Yu, X.; Zhao, G.; Zhao, Q.; Wang, N.; Jiang, Y.; Jiang, F.; He, G.; Chen, Y.; et al. Exposure of Adults to Antibiotics in a Shanghai Suburban Area and Health Risk Assessment: A Biomonitoring-Based Study. Environ. Sci. Technol. 2018, 52, 13942–13950. [Google Scholar] [CrossRef]
- Rahube, T.O.; Marti, R.; Scott, A.; Tien, Y.-C.; Murray, R.; Sabourin, L.; Duenk, P.; Lapen, D.R.; Topp, E. Persistence of antibiotic resistance and plasmid-associated genes in soil following application of sewage sludge and abundance on vegetables at harvest. Can. J. Microbiol. 2016, 62, 600–607. [Google Scholar] [CrossRef]
- European Medicines Agency (EMA). Reflection Paper on Antimicrobial Resistance in the Environment: Considerations for Current and Future Risk Assessment of Veterinary Medicinal Products Draft. 2018. Available online: https://www.ema.europa.eu/documents/scientific-guideline/draft-reflection-paper-antimicrobial-resistance-environment-considerations-current-future-risk_en.pdf (accessed on 15 January 2019).
- Collignon, P.; Kennedy, K.J. Long-Term Persistence of Multidrug-Resistant Enterobacteriaceae after Travel. Clin. Infect. Dis. 2015, 61, 1766–1767. [Google Scholar] [CrossRef] [PubMed]
- Ashbolt, N.J.; Amézquita, A.; Backhaus, T.; Borriello, P.; Brandt, K.K.; Collignon, P.; Coors, A.; Finley, R.; Gaze, W.H.; Heberer, T.; et al. Human Health Risk Assessment (HHRA) for Environmental Development and Transfer of Antibiotic Resistance. Environ. Health Perspect. 2013, 121, 993–1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Organisation for Animal Health (OIE). The OIE Strategy on Antimicrobial Resistance and the Prudent Use of Antimicrobials; OIE: Paris, France, 2016. [Google Scholar]
- Department of Health and Department for Environment Food & Rural Affairs. UK Five-Year Antimicrobial Resistance Strategy 2013 to 2018; Department of Health and Department for Environment Food & Rural Affairs: London, UK, 2013.
- Public Health Agency of Canada. Federal Action Plan on Antimicrobial Resistance and Use in Canada; Public Health Agency of Canada: Ottawa, ON, Cananda, 2015.
- Commonwealth of Australia. Responding to the Threat of Antimicrobial Resistance. Australia’s First National Antimicrobial Resistance Strategy 2015-2019; Commonwealth of Australia: Canberra, Australia, 2016.
- European Union (EU). Communication from the Commission to the European Parliament and the Council. Action Plan against the Rising Threats from Antimicrobial Resistance; EU: Brussels, Belgium, 2011. [Google Scholar]
- The White House. National Action Plan for Combating Antibiotic-Resistant Bacteria; The White House: Washington, DC, USA, 2015.
- Food and Agriculture Organization (FAO). The FAO Action Plan on Antimicrobial Resistance 2016-2020; FAO: Rome, Italy, 2016. [Google Scholar]
Figure 1.
Global aggregated regions: antimicrobial resistance E. coli to third generation cephalosporins and fluoroquinolones versus antibiotic usage.
Figure 1.
Global aggregated regions: antimicrobial resistance E. coli to third generation cephalosporins and fluoroquinolones versus antibiotic usage.

Figure 2.
Reported use of antimicrobial agents in animals in 2014 by World Organisation for Animal Health (OIE) Region (adapted from [46]).
Figure 2.
Reported use of antimicrobial agents in animals in 2014 by World Organisation for Animal Health (OIE) Region (adapted from [46]).


{kind=link}
{kind=link}
Table 1.
Levels of antibiotic usage in people, resistance levels and other parameters globally. (All data taken from reference 7).
Table 1.
Levels of antibiotic usage in people, resistance levels and other parameters globally. (All data taken from reference 7).
| Country | Antibiotic Usage (Standard units per 1000 pop - CCDEP) | E. coli % Resistance 3rd gen ceph (WHO) | E. coli % Resistance Fluoroquinolones (WHO) | Staphylococcus Aureus (MRSA Rates - WHO) | 2015 Corruption Index | GNP per capita 2015 (Purchasing Power Parity in 2011 Dollars) | % with Adequate Sanitation 2015 | Improved Water Source (% of Population with Access) |
|---|---|---|---|---|---|---|---|---|
| Algeria | 15.4 | 17 | 2 | 44.8 | 36 | $13,795 | 88 | 87.7 |
| Argentina | 6.2 | 5.1 | 7.8 | 54 | 32 | $19,102 | 96 | 98.9 |
| Australia | 11 | 7.7 | 10.6 | 30 | 79 | $43,631 | 100 | 100 |
| Austria | 7.2 | 9.1 | 22.3 | 7.4 | 76 | $44,048 | 100 | 100 |
| Bahrain | 55 | 62 | 10 | 51 | $43,754 | 99 | 100 | |
| Bangladesh | 4.3 | 57.4 | 89 | 46 | 25 | $3,137 | 61 | 86.2 |
| Belgium | 12.6 | 6 | 21.5 | 17.4 | 77 | $41,826 | 100 | 100 |
| Bhutan | 19.4 | 35.5 | 10 | 65 | $7,861 | 50 | 100 | |
| Bosnia and Herzegovina | 7.5 | 1.5 | 7.8 | 38 | $10,119 | 95 | 99.9 | |
| Brazil | 5.9 | 30 | 40 | 29.5 | 38 | $14,533 | 83 | 98.1 |
| Brunei Darussalam | 6.5 | 12 | 55 | $73,605 | 100 | 100 | ||
| Bulgaria | 9.4 | 22.9 | 30.2 | 22.4 | 41 | $17,000 | 86 | 99.6 |
| Burkina Faso | 36 | 52.8 | 38 | $1,593 | 20 | 82.1 | ||
| Burundi | 7.2 | 16 | 13 | 21 | $683 | 48 | 75.8 | |
| Cambodia | 45 | 71.8 | 21 | $3,278 | 42 | 73.4 | ||
| Canada | 7.2 | 8 | 26.9 | 21 | 83 | $42,983 | 100 | 99.8 |
| Central African Republic | 30 | 53 | 24 | $581 | 22 | 68.4 | ||
| Chile | 4.3 | 23.8 | 90 | 70 | $22,197 | 99 | 99 | |
| China | 3 | 51.9 | 55.1 | 38.3 | 70 | $13,572 | 77 | 94.8 |
| Colombia | 2.9 | 11.7 | 59 | 7.2 | 37 | $12,988 | 81 | 91.3 |
| Croatia | 10.6 | 6 | 14 | 13 | 51 | $20,664 | 97 | 99.6 |
| Cuba | 42.9 | 56 | 47 | $21,017 | 93 | 94.6 | ||
| Cyprus | 36.2 | 47.4 | 41.6 | 61 | $30,383 | 100 | 100 | |
| Czech Republic | 7.5 | 11.4 | 23.5 | 14.5 | 56 | $30,381 | 99 | 100 |
| Denmark | 6.7 | 8.5 | 14.1 | 1.2 | 91 | $45,484 | 100 | 100 |
| Dominican Republic | 2.4 | 33 | 49 | 30 | 33 | $13,372 | 84 | 86.5 |
| Ecuador | 6.7 | 15.1 | 43.8 | 29 | 32 | $10,777 | 85 | 86.9 |
| Egypt | 9.1 | 44.4 | 34.9 | 46 | 36 | $10,250 | 95 | 99.2 |
| Estonia | 4.4 | 9.9 | 1.7 | 70 | $27,345 | 97 | 99.6 | |
| Ethiopia | 62 | 71 | 31.6 | 33 | $1,530 | 28 | 55.4 | |
| Finland | 7.2 | 5.1 | 10.8 | 2.8 | 90 | $38,994 | 98 | 100 |
| France | 12.9 | 8.2 | 17.9 | 20.1 | 70 | $37,775 | 99 | 100 |
| Germany | 7.1 | 8 | 23.7 | 16.2 | 81 | $43,788 | 99 | 100 |
| Greece | 14.6 | 14.9 | 26.6 | 39.2 | 46 | $24,095 | 99 | 100 |
| Guatemala | 39.8 | 41.8 | 52 | 28 | $7,253 | 64 | 92.7 | |
| Honduras | 36.7 | 43.1 | 30 | 31 | $4,785 | 83 | 90.6 | |
| Hong Kong | 7.5 | 75 | $53,463 | 96 | 100 | |||
| Hungary | 7.3 | 15.1 | 31.2 | 26.2 | 51 | $24,831 | 98 | 100 |
| Iceland | 6.2 | 14 | 79 | $42,704 | 99 | 100 | ||
| India | 5 | 51.4 | 52.3 | 42.7 | 38 | $5,733 | 40 | 94.1 |
| Indonesia | 3.6 | 36 | $10,385 | 61 | 86.8 | |||
| Iran | 41 | 54 | 53 | 27 | $16,507 | 90 | 96.2 | |
| Ireland | 11.4 | 9 | 22.9 | 23.7 | 75 | $61,378 | 91 | 97.9 |
| Israel | 2.6 | 17.9 | 46.7 | 61 | $31,971 | 100 | 100 | |
| Italy | 11.5 | 19.8 | 40.5 | 38.2 | 44 | $34,220 | 100 | 100 |
| Japan | 5.3 | 16.6 | 34.3 | 53 | 75 | $37,872 | 100 | 100 |
| Jordan | 6.3 | 22.5 | 14.5 | 53 | $10,240 | 99 | 96.9 | |
| Kazakhstan | 7.5 | 28 | $23,522 | 98 | 93.5 | |||
| Kenya | 87.2 | 91.4 | 20 | 25 | $2,901 | 30 | 63.1 | |
| Kuwait | 6.3 | 20.1 | 32 | 49 | $70,107 | 100 | 99 | |
| Latvia | 5.2 | 15.9 | 16.8 | 9.9 | 55 | $23,080 | 88 | 99.3 |
| Lebanon | 9.3 | 27.7 | 47 | 20 | 28 | $13,089 | 81 | 99 |
| Lesotho | 2 | 14 | 44 | $2,770 | 30 | 81.6 | ||
| Lithuania | 7.6 | 7 | 12.9 | 5.8 | 61 | $26,971 | 92 | 96.6 |
| Luxembourg | 11 | 8.2 | 24.1 | 20.5 | 81 | $93,900 | 98 | 100 |
| Malaysia | 4.3 | 17.4 | 23 | 17.3 | 50 | $25,312 | 96 | 98.2 |
| Malta | 12.8 | 32 | 49.2 | 56 | $32,720 | 100 | 100 | |
| Mexico | 2.4 | 42.1 | 46.3 | 29.9 | 35 | $16,490 | 85 | 96.1 |
| Mongolia | 64.1 | 64.7 | 39 | $11,478 | 60 | 64.2 | ||
| Morocco | 6 | 4 | 23.3 | 19 | 36 | $7,365 | 77 | 85.3 |
| Myanmar | 68 | 55 | 26 | 22 | $4,931 | 80 | 80.5 | |
| Nepal | 37.9 | 64.3 | 44.9 | 27 | $2,312 | 46 | 90.7 | |
| Netherlands | 4.1 | 5.7 | 14.3 | 1.4 | 87 | $46,354 | 98 | 100 |
| New Zealand | 10.9 | 3 | 6.5 | 10.4 | 88 | $35,159 | 100 | 100 |
| Nicaragua | 48.1 | 42.9 | 27 | $4,884 | 68 | 86.9 | ||
| Nigeria | 6.7 | 36.5 | 47.1 | 26 | $5,639 | 29 | 67.6 | |
| Norway | 5.9 | 3.6 | 9 | 0.3 | 87 | $63,650 | 98 | 100 |
| Pakistan | 7.1 | 36.2 | 35.3 | 37.6 | 30 | $4,706 | 64 | 91.3 |
| Panama | 9.2 | 23.3 | 21.1 | 39 | $20,885 | 75 | 94.4 | |
| Papua New Guinea | 24.1 | 13.3 | 43.9 | 25 | $2,723 | 19 | 40 | |
| Paraguay | 1.4 | 22.1 | 27 | 27 | $8,639 | 89 | 96.6 | |
| Peru | 3.4 | 44.1 | 62.8 | 65.9 | 36 | $11,768 | 76 | 86.3 |
| Philippines | 2.2 | 26.7 | 40.9 | 54.9 | 35 | $6,938 | 74 | 91.5 |
| Poland | 9.3 | 11.7 | 27.3 | 24.3 | 62 | $25,323 | 97 | 98.3 |
| Portugal | 9.3 | 11.3 | 27.2 | 54.6 | 63 | $26,549 | 100 | 100 |
| Puerto Rico | 9.1 | 99 | ||||||
| Republic of Moldova | 28 | 15.3 | 50.3 | 33 | $4,742 | 76 | 88.4 | |
| Russian Federation | 6.2 | 18 | 25.7 | 29.3 | 29 | $24,124 | 72 | 96.9 |
| Rwanda | 21.4 | 54 | $1,655 | 62 | 75.5 | |||
| Serbia | 10.6 | 21.3 | 16 | 44.5 | 40 | $13,278 | 96 | 99.3 |
| Singapore | 5.7 | 20 | 37.8 | 85 | $80,192 | 100 | 100 | |
| Slovakia | 9.2 | 31 | 41.9 | 25.9 | 51 | $28,254 | 99 | 100 |
| Slovenia | 6.3 | 8.8 | 20.7 | 7.1 | 60 | $29,097 | 99 | 99.6 |
| South Africa | 8.7 | 8.2 | 16.1 | 52 | 44 | $12,393 | 66 | 92.8 |
| South Korea | 10.9 | 24.4 | 40.9 | 65.3 | 56 | $34,387 | 100 | 97.6 |
| Spain | 14.3 | 12 | 34.5 | 22.5 | 55 | $32,219 | 100 | 100 |
| Sri Lanka | 3.9 | 58.9 | 58.8 | 37 | $11,048 | 95 | 95.6 | |
| Sudan | 49.5 | 56.8 | 12 | $4,121 | 24 | 58.5 | ||
| Saudi Arabia | 11.1 | 15.9 | 40.9 | 41.9 | 52 | $50,284 | 100 | 97 |
| Sweden | 4.8 | 3 | 7.9 | 0.8 | 89 | $45,488 | 99 | 100 |
| Switzerland | 5.2 | 8.2 | 20.2 | 10.2 | 86 | $56,517 | 100 | 100 |
| Syrian Arab Republic | 49.8 | 18 | $- | 96 | 90.1 | |||
| Taiwan | 8.7 | 62 | ||||||
| Thailand | 7 | 37.9 | 52.5 | 22.4 | 38 | $15,347 | 93 | 97.8 |
| Tunisia | 18 | 20.6 | 9.4 | 55.8 | 38 | $10,770 | 92 | 97.7 |
| Turkey | 18.5 | 43.3 | 46.3 | 31.5 | 42 | $19,460 | 95 | 100 |
| United Arab Emirates | 10.5 | 23 | 32.5 | 33.4 | 70 | $65,717 | 98 | 99.7 |
| United Kingdom | 9 | 9.6 | 17.5 | 13.6 | 81 | $38,509 | 99 | 100 |
| United States of America | 10.3 | 14.6 | 33.3 | 51.3 | 76 | $52,704 | 100 | 99.2 |
| Uruguay | 6.6 | 0 | 15 | 40 | 74 | $19,952 | 96 | 99.6 |
| Venezuela | 8.1 | 12.5 | 37.2 | 31 | 17 | $16,769 | 94 | 93.1 |
| Vietnam | 9.4 | 0.2 | 31 | $5,667 | 78 | 96.4 | ||
| Zambia | 37.4 | 50.5 | 32 | 38 | $3,602 | 44 | 64.6 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Collignon, P.J.; McEwen, S.A. One Health—Its Importance in Helping to Better Control Antimicrobial Resistance. Trop. Med. Infect. Dis. 2019, 4, 22. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed4010022
AMA Style
Collignon PJ, McEwen SA. One Health—Its Importance in Helping to Better Control Antimicrobial Resistance. Tropical Medicine and Infectious Disease. 2019; 4(1):22. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed4010022
Chicago/Turabian StyleCollignon, Peter J., and Scott A. McEwen. 2019. "One Health—Its Importance in Helping to Better Control Antimicrobial Resistance" Tropical Medicine and Infectious Disease 4, no. 1: 22. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed4010022