High Seroprevalence of Dengue Virus Infection in Sudan: Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
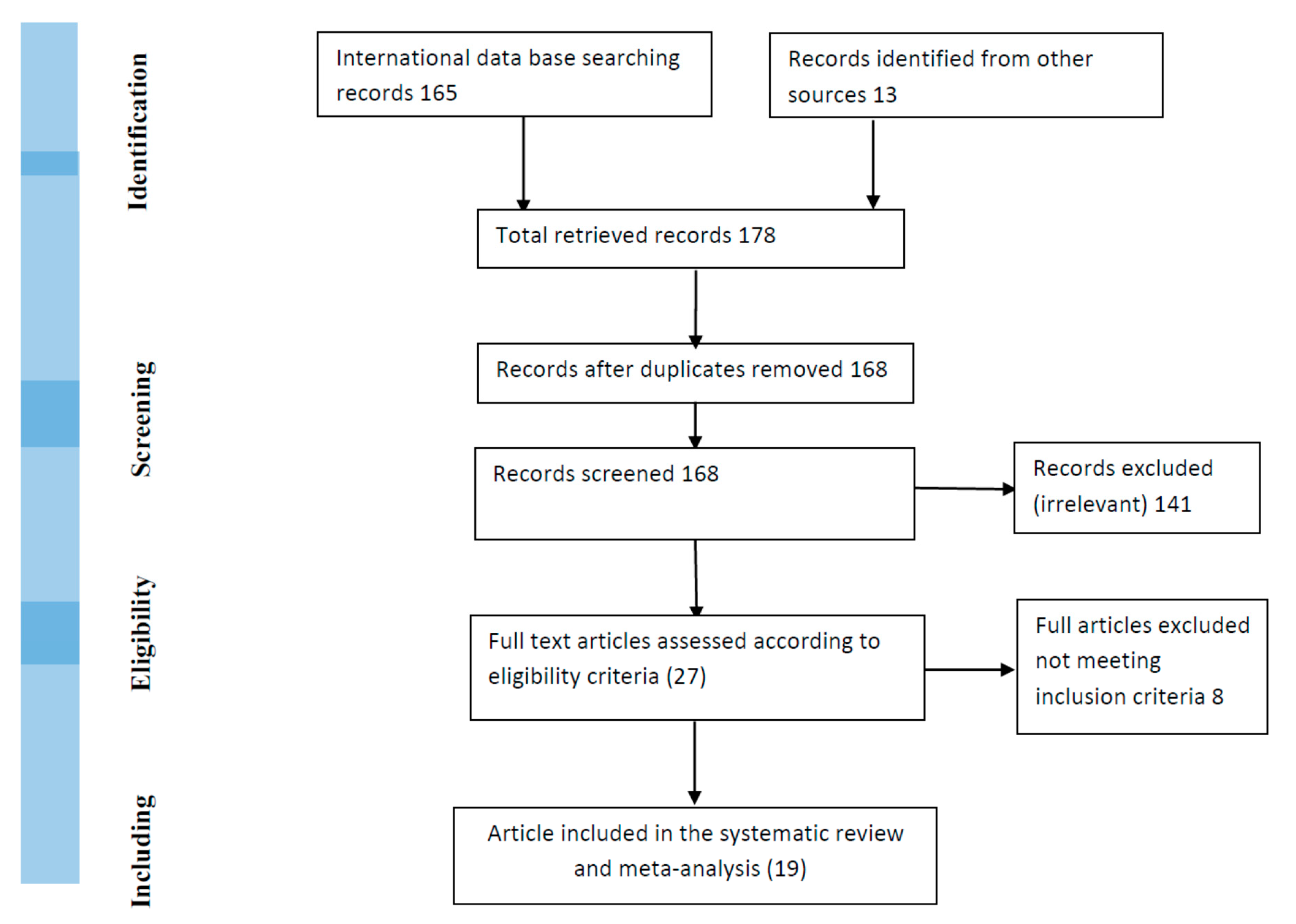
2.1. Searching Strategy
2.2. Inclusion Criteria
2.3. Data Extraction and Validity Assessment
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Weaver, S.C.; Reisen, W.K. Present and future arboviral threats. Antiviral Res. 2010, 85, 328–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Endy, T.P.; Anderson, K.B.; Nisalak, A.; Yoon, I.-K.; Green, S.; Rothman, A.L.; Thomas, S.J.; Jarman, R.G.; Libraty, D.H.; Gibbons, R.V. Determinants of Inapparent and Symptomatic Dengue Infection in a Prospective Study of Primary School Children in Kamphaeng Phet, Thailand. PLoS Negl. Trop. Dis. 2011, 5, e975. [Google Scholar] [CrossRef] [PubMed]
- Gubler, D.J. Dengue, Urbanization and Globalization: The Unholy Trinity of the 21st Century. Trop. Med. Health 2011, 39, S3–S11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngugi, H.N.; Mutuku, F.M.; Ndenga, B.A.; Musunzaji, P.S.; Mbakaya, J.O.; Aswani, P.; Irungu, L.W.; Mukoko, D.; Vulule, J.; Kitron, U.; et al. Characterization and productivity profiles of Aedes aegypti (L.) breeding habitats across rural and urban landscapes in western and coastal Kenya. Parasites Vectors 2017, 10, 331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The global distribution and burden of dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef] [PubMed]
- Vu, D.M.; Mutai, N.; Heath, C.J.; Vulule, J.M.; Mutuku, F.M.; Ndenga, B.A.; LaBeaud, A.D. Unrecognized Dengue Virus Infections in Children, Western Kenya, 2014–2015. Emerg. Infect. Dis. 2017, 23, 1915–1917. [Google Scholar] [CrossRef] [PubMed]
- Simmons, C.P.; Farrar, J.J.; van Vinh Chau, N.; Wills, B. Dengue. N. Engl. J. Med. 2012, 366, 1423–1432. [Google Scholar] [CrossRef]
- Saigh, S. Dengue in Port Sudan, Red Sea Province. J. Trop. Med. Hyg. 1906, 9, 348. [Google Scholar]
- Gindeel, N.J.H. Sero Investigation of Dengue Fever Epidemic in Port Sudan and Molecular Typing of the Virus. Master’s thesis, University of Khartoum, Khartoum, Sudan, 2015. Available online: http://khartoumspace.uofk.edu/handle/123456789/17010 (accessed on 24 February 2019).
- Malik, A.; Earhart, K.; Mohareb, E.; Saad, M.; Saeed, M.; Ageep, A.; Soliman, A. Dengue hemorrhagic fever outbreak in children in Port Sudan. J. Infect. Public Health 2011, 4, 1–6. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, M.C.; Haberberger, R.L.; Salib, A.W.; Soliman, B.A.; El-Tigani, A.; Khalid, I.O.; Watts, D.M. Evaluation of arthropod-borne viruses and other infectious disease pathogens as the causes of febrile illnesses in the Khartoum Province of Sudan. J. Med. Virol. 1996, 48, 141–146. [Google Scholar] [CrossRef]
- Watts, D.M.; el-Tigani, A.; Botros, B.A.; Salib, A.W.; Olson, J.G.; McCarthy, M.; Ksiazek, T.G. Arthropod-borne viral infections associated with a fever outbreak in the northern province of Sudan. J. Trop. Med. Hyg. 1994, 97, 228–230. [Google Scholar] [PubMed]
- Ahmed, A.; Elduma, A.; Magboul, B.; Higazi, T.; Ali, Y. The First Outbreak of Dengue Fever in Greater Darfur, Western Sudan. Trop. Med. Infect. Dis. 2019, 4, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, A.; Ali, Y.; Elmagboul, B.; Mohamed, O.; Elduma, A.; Bashab, H.; Mahamoud, A.; Khogali, H.; Elaagip, A.; Higazi, T. Dengue Fever in the Darfur Area, Western Sudan—Volume 25, Number 11—November 2019—Emerging Infectious Diseases Journal—CDC. Available online: https://wwwnc.cdc.gov/eid/article/25/11/18-1766_article (accessed on 29 September 2019).
- Soghaier, M.A.; Mahmood, S.F.; Pasha, O.; Azam, S.I.; Karsani, M.M.; Elmangory, M.M.; Elmagboul, B.A.; Okoued, S.I.; Shareef, S.M.; Khogali, H.S.; et al. Factors associated with dengue fever IgG sero-prevalence in South Kordofan State, Sudan, in 2012: Reporting prevalence ratios. J. Infect. Public Health 2014, 7, 54–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gayer, M.; Legros, D.; Formenty, P.; Connolly, M.A. Conflict and Emerging Infectious Diseases. Emerg. Infect. Dis. 2007, 13, 1625–1631. [Google Scholar] [CrossRef]
- Ahmed, A.; Dietrich, I.; LaBeaud, A.D.; Lindsay, S.W.; Musa, A.; Weaver, S.C. Risks and Challenges of Arboviral Diseases in Sudan: The Urgent Need for Actions. Viruses 2020, 12, 81. [Google Scholar] [CrossRef] [Green Version]
- Hamid, Z.; Hamid, T.; Alsedig, K.; Abdallah, T.; Elaagip, A.; Ahmed, A.; Khalid, F.; Abdel Hamid, M. Molecular Investigation of Dengue virus serotype 2 Circulation in Kassala State, Sudan. Jpn. J. Infect. Dis. 2019, 72, 58–61. [Google Scholar] [CrossRef] [Green Version]
- Wells, G. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non Randomised Studies in Meta-Analyses. 2012. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 20 May 2019).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Hyams, K.C.; Oldfield, E.C.; Scott, R.M.; Bourgeois, A.L.; Gardiner, H.; Pazzaglia, G.; Moussa, M.; Saleh, A.S.; Dawi, O.E.; Daniell, F.D. Evaluation of Febrile Patients in Port Sudan, Sudan: Isolation of Dengue Virus. Am. J. Trop. Med. Hyg. 1986, 35, 860–865. [Google Scholar] [CrossRef]
- Siddig, H.S. Sero—Epidemiology of Arboviruses South Khartoum State 2000. Medicinae Doctor’s Thesis, University of Khartoum, Khartoum, Sudan, 2004. Available online: http://khartoumspace.uofk.edu/handle/123456789/26065 (accessed on 24 February 2019).
- Adam, I.; Jumaa, A.M.; Elbashir, H.M.; Karsany, M.S. Maternal and perinatal outcomes of dengue in PortSudan, Eastern Sudan. Virol. J. 2010, 7, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seidahmed, O.M.; Hassan, S.A.; Soghaier, M.A.; Siam, H.A.; Ahmed, F.T.; Elkarsany, M.M.; Sulaiman, S.M. Spatial and temporal patterns of dengue transmission along a Red Sea coastline: A longitudinal entomological and serological survey in Port Sudan city. PLoS Negl. Trop. Dis. 2012, 6, e1821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdallah, T.M.; Ali, A.A.A.; Karsany, M.S.; Adam, I. Epidemiology of dengue infections in Kassala, Eastern Sudan. J. Med. Virol. 2012, 84, 500–503. [Google Scholar] [CrossRef] [PubMed]
- Himatt, S.; Osman, K.E.; Okoued, S.I.; Seidahmed, O.E.; Beatty, M.E.; Soghaier, M.A.; Elmusharaf, K. Sero-prevalence of dengue infections in the Kassala state in the eastern part of the Sudan in 2011. J. Infect. Public Health 2015, 8, 487–492. [Google Scholar] [CrossRef] [Green Version]
- Abdalla, T.M.; Karsany, M.S.; Ali, A.A. Correlation of measles and dengue infection in Kassala, Eastern Sudan. J. Med. Virol. 2015, 87, 76–78. [Google Scholar] [CrossRef]
- Baudin, M.; Jumaa, A.M.; Jomma, H.J.E.; Karsany, M.S.; Bucht, G.; Näslund, J.; Ahlm, C.; Evander, M.; Mohamed, N. Association of Rift Valley fever virus infection with miscarriage in Sudanese women: A cross-sectional study. Lancet Glob. Health 2016, 4, e864–e871. [Google Scholar] [CrossRef] [Green Version]
- Elduma, A.H.; Osman, W.M. Dengue and hepatitis E virus infection in pregnant women in Eastern Sudan, a challenge for diagnosis in an endemic area. Pan Afr. Med. J. 2014, 19. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC4430155/ (accessed on 26 February 2018). [CrossRef]
- Soghaier, M.A.; Mahmood, S.F.; Pasha, O.; Azam, S.I.; Karsani, M.M.; Elmangory, M.M.; Elmagboul, B.A.; Khogali, H.S.; Eltigai, E. Dengue fever in a border state between Sudan and Republic of South Sudan: Epidemiological perspectives. J. Public Health Epidemiol. 2013, 5, 319–324. [Google Scholar]
- Adam, A.; Schüttoff, T.; Reiche, S.; Jassoy, C. High seroprevalence of dengue virus indicates that dengue virus infections are frequent in central and eastern Sudan. Trop. Med. Int. Health 2018, 23, 960–967. [Google Scholar] [CrossRef]
- Eldigail, M.H.; Adam, G.K.; Babiker, R.A.; Khalid, F.; Adam, I.A.; Omer, O.H.; Ahmed, M.E.; Birair, S.L.; Haroun, E.M.; AbuAisha, H.; et al. Prevalence of dengue fever virus antibodies and associated risk factors among residents of El-Gadarif state, Sudan. BMC Public Health 2018, 18, 921. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, A. Urgent call for a global enforcement of the public sharing of health emergencies data: Lesson learned from serious arboviral disease epidemics in Sudan. Int. Health 2020. Available online: https://0-academic-oup-com.brum.beds.ac.uk/inthealth/advance-article/doi/10.1093/inthealth/ihz122/5788237 (accessed on 7 March 2020). [CrossRef]
- Vu, D.M.; Banda, T.; Teng, C.Y.; Heimbaugh, C.; Muchiri, E.M.; Mungai, P.L.; Mutuku, F.M.; Brichard, J.; Gildengorin, G.; Borland, E.M. Dengue and West Nile virus transmission in children and adults in coastal Kenya. Am. J. Trop. Med. Hyg. 2017, 96, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, L.J.; Cash, A.A.; Huang, Y.-J.S.; Sang, R.C.; Malhotra, I.; Moormann, A.M.; King, C.L.; Weaver, S.C.; King, C.H.; LaBeaud, A.D. Serologic evidence of arboviral infections among humans in Kenya. Am. J. Trop. Med. Hyg. 2011, 85, 158–161. [Google Scholar] [CrossRef] [Green Version]
- Amarasinghe, A.; Kuritsky, J.N.; Letson, G.W.; Margolis, H.S. Dengue Virus Infection in Africa. Emerg. Infect. Dis. 2011, 17, 1349–1354. [Google Scholar] [CrossRef] [PubMed]
- Alhaeli, A.; Bahkali, S.; Ali, A.; Househ, M.S.; El-Metwally, A.A. The epidemiology of Dengue fever in Saudi Arabia: A systematic review. J. Infect. Public Health 2016, 9, 117–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamal, H. The 1927 epidemic of Dengue in Egypt. Br. Med. J. 1928, 1, 1104. [Google Scholar] [CrossRef] [PubMed]
- Usman, A.; Ball, J.D.; Rojas, D.P.; Berhane, A.; Ghebrat, Y.; Mebrahtu, G.; Gebresellasie, A.; Zehaie, A.; Mufunda, J.; Liseth, O. Dengue fever outbreaks in Eritrea, 2005–2015. Glob. Health Res. Policy 2016, 1, 17. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No | Year of Survey | Region | State | Study Type | Diagnostic Test | Sample Size | No of Cases | Reported Prevalence | Detected Serotype | Mean Age | Sex | Reference |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1984 | East | Red Sea | Cross-sectional hospital-based | ELISA-IgM | 100 | 21 | 21% | DENV1 and 2 | - | M + F | [23] |
| 2 | 1988 | Central | Khartoum | Cross-sectional hospital-based | ELISA-IgG | 196 | 97 | 33% | DENV2 | 20 | M + F | [11] |
| 3 | 1989 | North | Northern | Cross-sectional hospital-based | ELISA-IgG | 185 | 44 | 24% | DENV2 | 34 | M + F | [12] |
| 4 | 2000 | Central | Khartoum | Cross-sectional community-based | ELISA-IgM | 1157 | 485 | 42% | - | - | M + F | [24] |
| 5 | 2005 | East | Red Sea | Cross-sectional hospital-based | ELISA-IgM | 312 | 36 | 12% | DENV3 | 5–15 | M + F | [10] |
| 6 | 2009 | East | Red Sea | Retrospective Cohort | ELISA-IgM | 10,820 | 78 | 1% | - | - | Pregnant women | [25] |
| 7 | 2009 | East | Red Sea | Cross-sectional community-based | ELISA-IgM | 791 | 41 | 5.2% | - | 30 | M + F | [26] |
| 8 | 2010 | East | Kassala | Cross-sectional hospital-based | ELISA-IgM | 113 | 81 | 72% | - | 25.5 | M + F | [27] |
| 9 | 2010 | East | Red Sea | Cross-sectional hospital-based | ELISA-IgM | 200 | 73 | 37% | DENV2–4 | 25 | M + F | [9] |
| 10 | 2011 | East | Kassala | Cross-sectional community-based | ELISA-IgM | 491 | 46 | 9% | - | 40 | M + F | [28] |
| 11 | 2012 | East | Kassala | Cross-sectional hospital-based | ELISA-IgM | 275 | 17 | 6% | - | 17.8 | M + F | [29] |
| 12 | 2012 | East | Red Sea | Cross-sectional hospital-based | ELISA-IgM | 130 | 9 | 7% | - | - | F | [30] |
| 13 | 2012 | East | Red Sea | Cross-sectional hospital-based | ELISA-IgM | 39 | 5 | 13% | - | 26 | Pregnant women | [31] |
| 14 | 2012 | West | South Kordofan | Cross-sectional community-based | ELISA-IgG | 615 | 170 | 28% | - | 37.5 | M + F | [32] |
| 15 | 2013 | East and West | Red Sea, Kassala, North Kordofan | Cross-sectional hospital-based | ELISA-IgM | 483 | 302 | 63% | DENV1–4 | 40.7 | M + F | [33] |
| 16 | 2015 | West | North Darfur | Cross-sectional hospital-based | ELISA-IgG | 50 | 35 | 70% | DENV1 and 3 | 37.8 | M + F | [14] |
| 17 | 2016 | West | Central, North, South, and West Darfur | Cross-sectional hospital-based | ELISA-IgM | 204 | 32 | 16% | DENV1 and 3 | - | M + F | [13] |
| 18 | 2017 | East | Gadaref | Cross-sectional community-based | ELISA-IgG | 701 | 334 | 48% | - | - | M + F | [34] |
| 19 | 2017 | East | Kassala | Cross-sectional hospital-based | RT-PCR | 106 | 4 | 4% | DENV2 | - | - | [18] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elduma, A.H.; LaBeaud, A.D.; A. Plante, J.; Plante, K.S.; Ahmed, A. High Seroprevalence of Dengue Virus Infection in Sudan: Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2020, 5, 120. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5030120
Elduma AH, LaBeaud AD, A. Plante J, Plante KS, Ahmed A. High Seroprevalence of Dengue Virus Infection in Sudan: Systematic Review and Meta-Analysis. Tropical Medicine and Infectious Disease. 2020; 5(3):120. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5030120
Chicago/Turabian StyleElduma, Adel Hussein, A. Desiree LaBeaud, Jessica A. Plante, Kenneth S. Plante, and Ayman Ahmed. 2020. "High Seroprevalence of Dengue Virus Infection in Sudan: Systematic Review and Meta-Analysis" Tropical Medicine and Infectious Disease 5, no. 3: 120. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5030120