
A Cluster of Dengue Cases in Travelers: A Clinical Series from Thailand

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Dengue Detection, Serotyping, and Envelope Nucleotide Sequencing
2.3. Phylogenetic Analysis
2.4. Data Analysis
3. Results
3.1. Descriptive Analysis of Warning Signs by Age Group
3.2. Hematological Profile during Illness
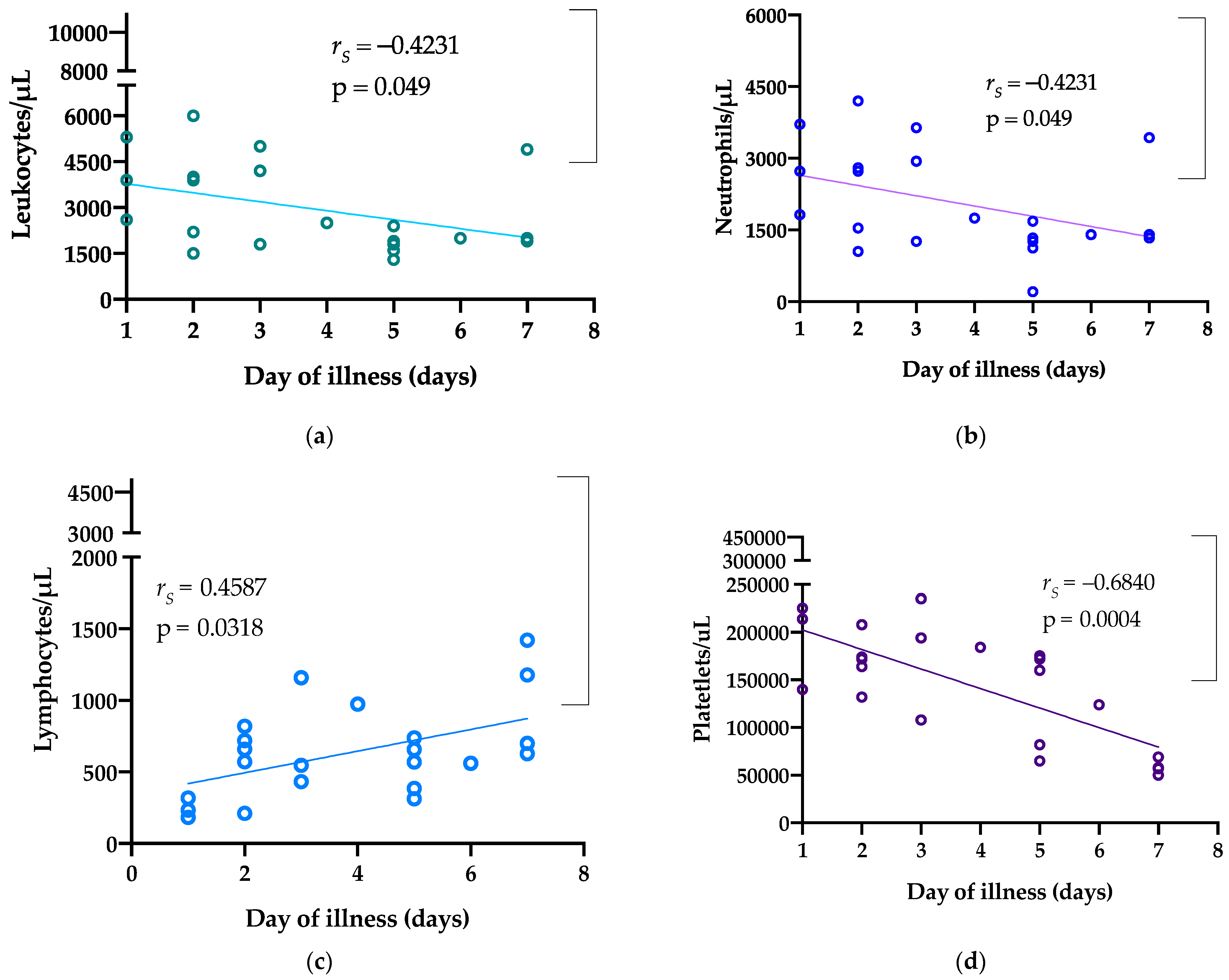
3.3. Analysis of Correlations between Clinical Parameters
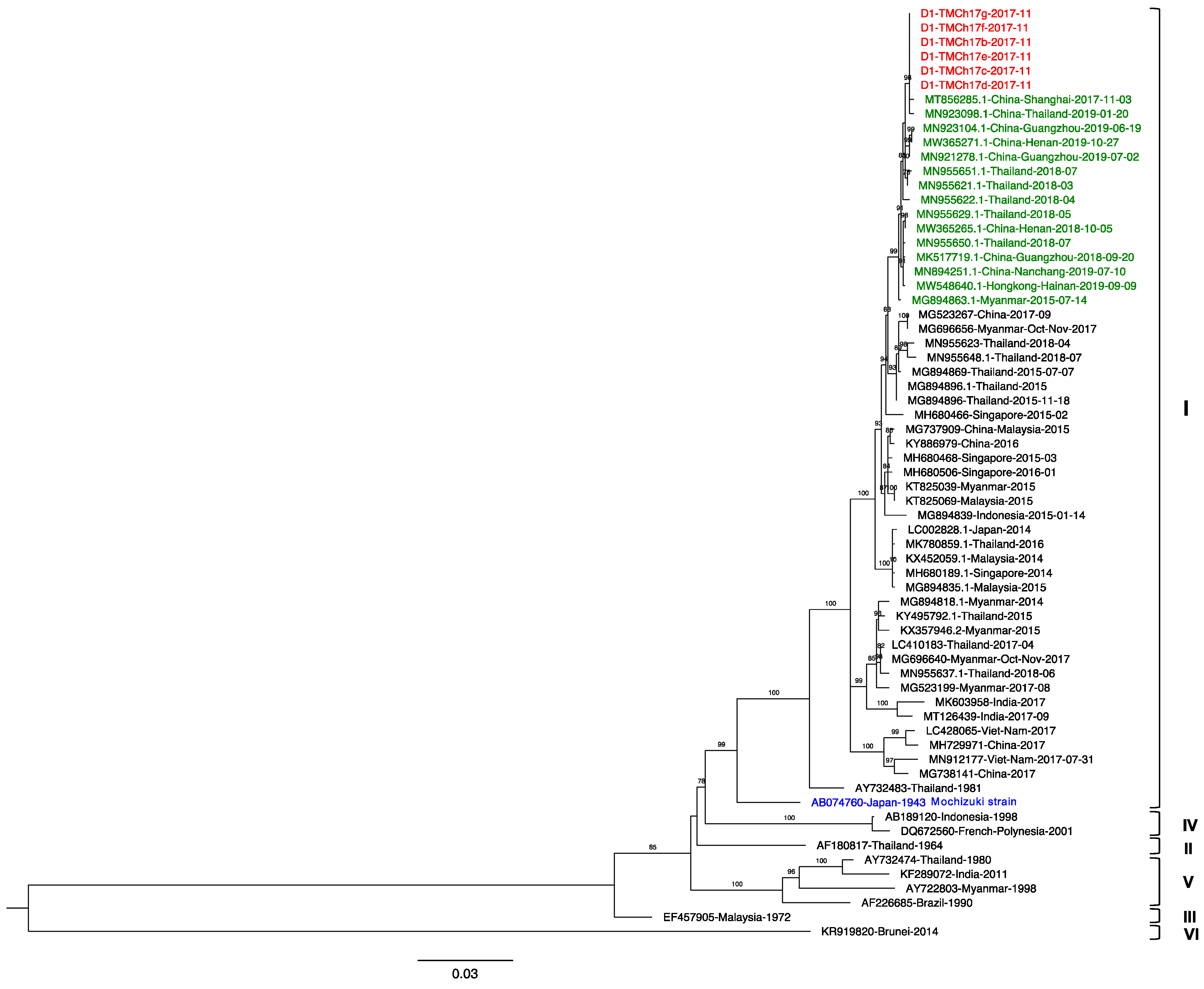
3.4. Phylogenetic Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Luvira, V.; Silachamroon, U.; Piyaphanee, W.; Lawpoolsri, S.; Chierakul, W.; Leaungwutiwong, P.; Thawornkuno, C.; Wattanagoon, Y. Etiologies of acute undifferentiated febrile illness in Bangkok, Thailand. Am. J. Trop. Med. Hyg. 2019, 100, 622–629. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The global distribution and burden of dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef]
- McGuire, P. The Devil’s disease: Dengue fever. The Magazine of the Johns Hopkins Bloomberg School of Public Health, 9 July 2010. [Google Scholar]
- Packard, R.M. The Fielding H. Garrison Lecture: “Break-Bone” Fever in Philadelphia, 1780: Reflections on the History of Disease. Bull. Hist. Med. 2016, 90, 193–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fortes-Lima, C.; Verdu, P. Anthropological genetics perspectives on the transatlantic slave trade. Hum. Mol. Genet. 2021, 30, R79–R87. [Google Scholar] [CrossRef] [PubMed]
- Hotta, S. Experimental studies on dengue. I. Isolation, identification and modification of the virus. J. Infect. Dis. 1952, 90, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sabin, A.B. Research on dengue during World War II. Am. J. Trop. Med. Hyg. 1952, 1, 30–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuno, G.; Chang, G.J.; Tsuchiya, K.R.; Karabatsos, N.; Cropp, C.B. Phylogeny of the genus Flavivirus. J. Virol. 1998, 72, 73–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilder-Smith, A.; Ooi, E.E.; Horstick, O.; Wills, B. Dengue. Lancet 2019, 393, 350–363. [Google Scholar] [CrossRef]
- Rico-Hesse, R.; Harrison, L.M.; Nisalak, A.; Vaughn, D.W.; Kalayanarooj, S.; Green, S.; Rothman, A.L.; Ennis, F.A. Molecular evolution of dengue type 2 virus in Thailand. Am. J. Trop. Med. Hyg. 1998, 58, 96–101. [Google Scholar] [CrossRef]
- Fried, J.R.; Gibbons, R.V.; Kalayanarooj, S.; Thomas, S.J.; Srikiatkhachorn, A.; Yoon, I.K.; Jarman, R.G.; Green, S.; Rothman, A.L.; Cummings, D.A. Serotype-specific differences in the risk of dengue hemorrhagic fever: An analysis of data collected in Bangkok, Thailand from 1994 to 2006. PLoS Negl. Trop. Dis. 2010, 4, e617. [Google Scholar] [CrossRef] [Green Version]
- Vaughn, D.W.; Green, S.; Kalayanarooj, S.; Innis, B.L.; Nimmannitya, S.; Suntayakorn, S.; Endy, T.P.; Raengsakulrach, B.; Rothman, A.L.; Ennis, F.A.; et al. Dengue viremia titer, antibody response pattern, and virus serotype correlate with disease severity. J. Infect. Dis. 2000, 181, 2–9. [Google Scholar] [CrossRef]
- Endy, T.P.; Chunsuttiwat, S.; Nisalak, A.; Libraty, D.H.; Green, S.; Rothman, A.L.; Vaughn, D.W.; Ennis, F.A. Epidemiology of inapparent and symptomatic acute dengue virus infection: A prospective study of primary school children in Kamphaeng Phet, Thailand. Am. J. Epidemiol. 2002, 156, 40–51. [Google Scholar] [CrossRef]
- Burke, D.S.; Nisalak, A.; Johnson, D.E.; Scott, R.M. A prospective study of dengue infections in Bangkok. Am. J. Trop. Med. Hyg. 1988, 38, 172–180. [Google Scholar] [CrossRef]
- Duong, V.; Lambrechts, L.; Paul, R.E.; Ly, S.; Lay, R.S.; Long, K.C.; Huy, R.; Tarantola, A.; Scott, T.W.; Sakuntabhai, A.; et al. Asymptomatic humans transmit dengue virus to mosquitoes. Proc. Natl. Acad. Sci. USA 2015, 112, 14688–14693. [Google Scholar] [CrossRef] [Green Version]
- Vongpunsawad, S.; Intharasongkroh, D.; Thongmee, T.; Poovorawan, Y. Seroprevalence of antibodies to dengue and chikungunya viruses in Thailand. PLoS ONE 2017, 12, e0180560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, M.; Johansson, M.A. The incubation periods of Dengue viruses. PLoS ONE 2012, 7, e50972. [Google Scholar] [CrossRef]
- Yoon, I.K.; Srikiatkhachorn, A.; Hermann, L.; Buddhari, D.; Scott, T.W.; Jarman, R.G.; Aldstadt, J.; Nisalak, A.; Thammapalo, S.; Bhoomiboonchoo, P.; et al. Characteristics of mild dengue virus infection in Thai children. Am. J. Trop. Med. Hyg. 2013, 89, 1081–1087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, S.; Vaughn, D.W.; Kalayanarooj, S.; Nimmannitya, S.; Suntayakorn, S.; Nisalak, A.; Lew, R.; Innis, B.L.; Kurane, I.; Rothman, A.L.; et al. Early immune activation in acute dengue illness is related to development of plasma leakage and disease severity. J. Infect. Dis. 1999, 179, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Kurane, I.; Rothman, A.L.; Livingston, P.G.; Green, S.; Gagnon, S.J.; Janus, J.; Innis, B.L.; Nimmannitya, S.; Nisalak, A.; Ennis, F.A. Immunopathologic mechanisms of dengue hemorrhagic fever and dengue shock syndrome. Posit. Strand RNA Viruses 1994, 9, 59–64. [Google Scholar] [CrossRef]
- Harrington, L.C.; Fleisher, A.; Ruiz-Moreno, D.; Vermeylen, F.; Wa, C.V.; Poulson, R.L.; Edman, J.D.; Clark, J.M.; Jones, J.W.; Kitthawee, S.; et al. Heterogeneous feeding patterns of the dengue vector, Aedes aegypti, on individual human hosts in rural Thailand. PLoS Negl. Trop. Dis. 2014, 8, e3048. [Google Scholar] [CrossRef] [Green Version]
- Dengue National Disease Surveillance; Bureau of Epidemiology MoPH: Nonthaburi, Thailand, 2017.
- Wilder-Smith, A.; Schwartz, E. Dengue in travelers. N. Engl. J. Med. 2005, 353, 924–932. [Google Scholar] [CrossRef]
- Wilder-Smith, A. Dengue infections in travellers. Paediatr. Int. Child Health 2012, 32, 28–32. [Google Scholar] [CrossRef] [Green Version]
- Massad, E.; Rocklov, J.; Wilder-Smith, A. Dengue infections in non-immune travellers to Thailand. Epidemiol. Infect. 2013, 141, 412–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilder-Smith, A.; Tambyah, P.A. Severe dengue virus infection in travelers. J. Infect. Dis. 2007, 195, 1081–1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morens, D.M.; Sather, G.E.; Gubler, D.J.; Rammohan, M.; Woodall, J.P. Dengue shock syndrome in an American traveler with primary dengue 3 infection. Am. J. Trop. Med. Hyg. 1987, 36, 424–426. [Google Scholar] [CrossRef]
- Halstead, S.; Wilder-Smith, A. Severe dengue in travellers: Pathogenesis, risk and clinical management. J. Travel Med. 2019, 26. [Google Scholar] [CrossRef]
- Pancharoen, C.; Mekmullica, J.; Thisyakorn, U. Primary dengue infection: What are the clinical distinctions from secondary infection? Southeast Asian J. Trop. Med. Public Health 2001, 32, 476–480. [Google Scholar]
- Barnes, W.J.; Rosen, L. Fatal hemorrhagic disease and shock associated with primary dengue infection on a Pacific island. Am. J. Trop. Med. Hyg. 1974, 23, 495–506. [Google Scholar] [CrossRef]
- Janssen, H.L.; Bienfait, H.P.; Jansen, C.L.; van Duinen, S.G.; Vriesendorp, R.; Schimsheimer, R.J.; Groen, J.; Osterhaus, A.D. Fatal cerebral oedema associated with primary dengue infection. J. Infect. 1998, 36, 344–346. [Google Scholar] [CrossRef]
- Cardenas-Perea, M.E.; Flores-Mendoza, L.K.; Perez-Contreras, I.; Diaz-Orea, M.A.; Gomez-Conde, E.; Cortes-Hernandez, P.; Reyes-Leyva, J.; Santos-Lopez, G.; Sosa-Jurado, F. Primary dengue infection in patients requiring hospitalization during an outbreak in a low incidence mexican region. Vector Borne Zoonotic Dis. 2020, 20, 380–386. [Google Scholar] [CrossRef] [Green Version]
- Uttayamakul, S.; Reawrang, S.; Nitiyanontakij, R.; Phadungsombat, J.; Nakayama, E.; Suttha, P.; Moolasart, V.; Shioda, T. Molecular characteristics of dengue viruses in patients hospitalized at the bamrasnaradura infectious diseases institute, Thailand. Jpn. J. Infect. Dis. 2020, 73, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Larsson, A. AliView: A fast and lightweight alignment viewer and editor for large datasets. Bioinformatics 2014, 30, 3276–3278. [Google Scholar] [CrossRef]
- Nguyen, L.T.; Schmidt, H.A.; von Haeseler, A.; Minh, B.Q. IQ-TREE: A fast and effective stochastic algorithm for estimating maximum-likelihood phylogenies. Mol. Biol. Evol. 2015, 32, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Hoang, D.T.; Chernomor, O.; von Haeseler, A.; Minh, B.Q.; Vinh, L.S. UFBoot2: Improving the ultrafast bootstrap approximation. Mol. Biol. Evol. 2018, 35, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Htun, T.P.; Xiong, Z.; Pang, J. Clinical signs and symptoms associated with WHO severe dengue classification: A systematic review and meta-analysis. Emerg. Microbes Infect. 2021, 10, 1116–1128. [Google Scholar] [CrossRef] [PubMed]
- Lambrechts, L.; Fansiri, T.; Pongsiri, A.; Thaisomboonsuk, B.; Klungthong, C.; Richardson, J.H.; Ponlawat, A.; Jarman, R.G.; Scott, T.W. Dengue-1 virus clade replacement in Thailand associated with enhanced mosquito transmission. J. Virol. 2012, 86, 1853–1861. [Google Scholar] [CrossRef] [Green Version]
- Koo, C.; Tien, W.P.; Xu, H.; Ong, J.; Rajarethinam, J.; Lai, Y.L.; Ng, L.C.; Hapuarachchi, H.C. Highly selective transmission success of dengue virus type 1 lineages in a dynamic virus population: An evolutionary and fitness perspective. iScience 2018, 6, 38–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabaa, M.A.; Simmons, C.P.; Fox, A.; Le, M.Q.; Nguyen, T.T.; Le, H.Y.; Gibbons, R.V.; Nguyen, X.T.; Holmes, E.C.; Aaskov, J.G. Dengue virus in sub-tropical northern and central Viet Nam: Population immunity and climate shape patterns of viral invasion and maintenance. PLoS Negl. Trop. Dis. 2013, 7, e2581. [Google Scholar] [CrossRef] [Green Version]
- Utama, I.M.S.; Lukman, N.; Sukmawati, D.D.; Alisjahbana, B.; Alam, A.; Murniati, D.; Utama, I.; Puspitasari, D.; Kosasih, H.; Laksono, I.; et al. Dengue viral infection in Indonesia: Epidemiology, diagnostic challenges, and mutations from an observational cohort study. PLoS Negl. Trop. Dis. 2019, 13, e0007785. [Google Scholar] [CrossRef] [Green Version]
- Xiao, J.P.; He, J.F.; Deng, A.P.; Lin, H.L.; Song, T.; Peng, Z.Q.; Wu, X.C.; Liu, T.; Li, Z.H.; Rutherford, S.; et al. Characterizing a large outbreak of dengue fever in Guangdong Province, China. Infect. Dis. Poverty 2016, 5, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Hu, T.S.; Zhang, H.L.; Feng, Y.; Fan, J.H.; Tang, T.; Liu, Y.H.; Zhang, L.; Yin, X.X.; Chen, G.; Li, H.C.; et al. Epidemiological and molecular characteristics of emergent dengue virus in Yunnan Province near the China-Myanmar-Laos border, 2013–2015. BMC Infect. Dis. 2017, 17, 1–12. [Google Scholar] [CrossRef]
- Tian, H.; Sun, Z.; Faria, N.R.; Yang, J.; Cazelles, B.; Huang, S.; Xu, B.; Yang, Q.; Pybus, O.G.; Xu, B. Increasing airline travel may facilitate co-circulation of multiple dengue virus serotypes in Asia. PLoS Negl. Trop. Dis. 2017, 11, e0005694. [Google Scholar] [CrossRef] [Green Version]
- Cobelens, F.G.; Groen, J.; Osterhaus, A.D.; Leentvaar-Kuipers, A.; Wertheim-van Dillen, P.M.; Kager, P.A. Incidence and risk factors of probable dengue virus infection among Dutch travellers to Asia. Trop. Med. Int. Health 2002, 7, 331–338. [Google Scholar] [CrossRef]
- Potasman, I.; Srugo, I.; Schwartz, E. Dengue seroconversion among Israeli travelers to tropical countries. Emerg. Infect. Dis. 1999, 5, 824–827. [Google Scholar] [CrossRef] [PubMed]
- Loh, B.; Song, R.J. Modeling dengue cluster size as a function of aedes aegypti population and climate in Singapore. Dengue Bull. 2001, 25, 74–78. [Google Scholar]
- Yan, H.; Ding, Z.; Yan, J.; Yao, W.; Pan, J.; Yang, Z.; Lou, X.; Mao, H.; Lin, J.; Sun, J.; et al. Epidemiological characterization of the 2017 dengue outbreak in Zhejiang, China and molecular characterization of the viruses. Front. Cell. Infect. Microbiol. 2018, 8, 216. [Google Scholar] [CrossRef]
- Malavige, G.N.; Ranatunga, P.K.; Velathanthiri, V.G.; Fernando, S.; Karunatilaka, D.H.; Aaskov, J.; Seneviratne, S.L. Patterns of disease in Sri Lankan dengue patients. Arch. Dis. Child. 2006, 91, 396–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malavige, G.N.; Velathanthiri, V.G.; Wijewickrama, E.S.; Fernando, S.; Jayaratne, S.D.; Aaskov, J.; Seneviratne, S.L. Patterns of disease among adults hospitalized with dengue infections. QJM 2006, 99, 299–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balmaseda, A.; Hammond, S.N.; Perez, L.; Tellez, Y.; Saborio, S.I.; Mercado, J.C.; Cuadra, R.; Rocha, J.; Perez, M.A.; Silva, S.; et al. Serotype-specific differences in clinical manifestations of dengue. Am. J. Trop. Med. Hyg. 2006, 74, 449–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seet, R.C.; Ooi, E.E.; Wong, H.B.; Paton, N.I. An outbreak of primary dengue infection among migrant Chinese workers in Singapore characterized by prominent gastrointestinal symptoms and a high proportion of symptomatic cases. J. Clin. Virol. 2005, 33, 336–340. [Google Scholar] [CrossRef]
- Zulkarnain, E.; Hotta, S.; Takegami, T. Molecular comparison of dengue type 1 Mochizuki strain virus and other selected viruses concerning nucleotide and amino acid sequences of genomic RNA: A consideration of viral epidemiology and variation. Microbiol. Immunol. 1994, 38, 581–585. [Google Scholar] [CrossRef] [Green Version]
- Hong, W.X.; Zhao, H.; Deng, Y.Q.; Jiang, T.; Yu, X.D.; Song, K.Y.; Wang, J.; Tan, X.H.; Yu, M.; Zhu, S.Y.; et al. Severe dengue due to secondary DENV-1 infection in Mainland China. J. Clin. Virol. 2013, 57, 184–186. [Google Scholar] [CrossRef]
- Ramesh, S.; Basavaraju, M.; Sandeep, R.; Shetty, S.; Srinivasa, M.; Surakshith, T.; Ravichethan, K. Study of Bradycardia in Dengue Fever. J. Evol. Med. Dent. Sci. 2014, 3, 2378–2389. [Google Scholar] [CrossRef]
- Lateef, A.; Fisher, D.A.; Tambyah, P.A. Dengue and relative bradycardia. Emerg. Infect. Dis. 2007, 13, 650–651. [Google Scholar] [CrossRef]
- Wittesjo, B.; Bjornham, A.; Eitrem, R. Relative bradycardia in infectious diseases. J. Infect. 1999, 39, 246–247. [Google Scholar] [CrossRef]
- Ostergaard, L.; Huniche, B.; Andersen, P.L. Relative bradycardia in infectious diseases. J. Infect. 1996, 33, 185–191. [Google Scholar] [CrossRef]
- Ye, F.; Hatahet, M.; Youniss, M.A.; Toklu, H.Z.; Mazza, J.J.; Yale, S. The clinical significance of relative bradycardia. WMJ 2018, 117, 73–78. [Google Scholar] [PubMed]
- Sharda, M.; Gupt, A.; Nagar, D.; Soni, A.K. Dengue fever: An additional cause for bradycardia. J. Assoc. Physicians India 2014, 62, 362–363. [Google Scholar] [PubMed]
- Chia, P.Y.; Thein, T.L.; Ong, S.W.X.; Lye, D.C.; Leo, Y.S. Severe dengue and liver involvement: An overview and review of the literature. Expert Rev. Anti Infect. Ther. 2020, 18, 181–189. [Google Scholar] [CrossRef]
- Itha, S.; Kashyap, R.; Krishnani, N.; Saraswat, V.A.; Choudhuri, G.; Aggarwal, R. Profile of liver involvement in dengue virus infection. Natl. Med. J. India 2005, 18, 127–130. [Google Scholar]
- Mitrakul, C. Bleeding problem in dengue haemorrhagic fever: Platelets and coagulation changes. Southeast Asian J. Trop. Med. Public Health 1987, 18, 407–412. [Google Scholar] [PubMed]
- Hassan, J.; Borhany, M.; Abid, M.; Zaidi, U.; Fatima, N.; Shamsi, T. Coagulation abnormalities in dengue and dengue haemorrhagic fever patients. Transfus. Med. 2020, 30, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Imad, H.A.; Phumratanaprapin, W.; Phonrat, B.; Chotivanich, K.; Charunwatthana, P.; Muangnoicharoen, S.; Khusmith, S.; Tantawichien, T.; Phadungsombat, J.; Nakayama, E.; et al. Cytokine expression in dengue fever and dengue hemorrhagic fever patients with bleeding and severe hepatitis. Am. J. Trop. Med. Hyg. 2020, 102, 943–950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, A.K.C.; Leung, A.A.M.; Wong, A.H.C.; Hon, K.L. Travelers’ diarrhea: A clinical review. Recent Pat. Inflamm. Allergy Drug Discov. 2019, 13, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Reisinger, E.C.; Fritzsche, C.; Krause, R.; Krejs, G.J. Diarrhea caused by primarily non-gastrointestinal infections. Nat. Clin. Pract. Gastroenterol. Hepatol. 2005, 2, 216–222. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Adolescents | p-Value | Adults | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| Group A (n = 3) | Group B (n = 5) | Adjusted p-Value | Group A (n = 1) | Group B (n = 3) | Adjusted p-Value | |||
| Exposure duration, days | 10 (9) | 16 (12) | 0.046 | 1.000 | 8 (8) | 20 (4) | 0.655 | 1.000 |
| Body mass index, kg/m2 | 21.0 (17.6) | 22.7 (22.0–26.2) | 0.025 | 1.000 | 23.1 (23.1) | 25.5 (22.9) | 0.655 | 1.000 |
| Temperature, °C | 39.3 (39.0) | 39.0 (38.3–39.5) | 0.539 | 1.000 | 37.3 (37.3) | 39.2 (38.4) | 0.180 | 1.000 |
| Heart rate, beats per minute | 82.0 (82.0) | 82.0 (60.0–98.5) | 0.878 | 1.000 | 68 (68) | 80 (70) | 0.180 | 1.000 |
| Mean arterial pressure, mmHg | 73.3 (68.0) | 79.3 (73.0–85.0) | 0.101 | 1.000 | 70.3 (70.3) | 97 (90.6) | 0.180 | 1.000 |
| Day of presentation, days | 2 (2) | 2 (1.5–2.5) | 0.491 | 1.000 | 5 (5) | 1 (1) | 0.157 | 1.000 |
| Hospitalization, n (%) | 3 (100) | 3 (60) | 0.464 | 1.000 | 1 (100) | 2 (66.7) | 0.505 | 1.000 |
| Fever, n (%) | 3 (100) | 5 (100) | NA | NA | 1 (100) | 3 (100) | NA | NA |
| Dizziness, n (%) | 0 | 2 (40) | 0.464 | 1.000 | 0 | 0 | NA | NA |
| Relative bradycardia, n (%) | 3 (100) | 4 (80) | 1.000 | 1.000 | 0 | 3 (100) | 0.250 | 1.000 |
| Hepatomegaly, n (%) | 1 (33.3) | 0 | 0.375 | 1.000 | 1 (100) | 0 | 0.250 | 1.000 |
| Headache, n (%) | 2 (66.7) | 3 (60) | 1.000 | 1.000 | 0 | 2 (66.7) | 1.000 | 1.000 |
| Myalgia, n (%) | 1 (33.3) | 1 (20) | 1.000 | 1.000 | 0 | 2 (66.7) | 1.000 | 1.000 |
| Arthralgia, n (%) | 0 | 0 | NA | NA | 0 | 0 | NA | NA |
| Rash, n (%) | 0 | 2 (40) | 0.464 | 1.000 | 1 (100) | 1 (33.3) | 1.000 | 1.000 |
| Bleeding, n (%) | 1 (33.3) | 0 | 0.375 | 1.000 | 1 (100) | 0 | 0.250 | 1.000 |
| Loss of appetite, n (%) | 2 (66.7) | 1 (20) | 0.464 | 1.000 | 1 (100) | 0 | 0.250 | 1.000 |
| Nausea, n (%) | 2 (66.7) | 1 (20) | 0.464 | 1.000 | 1 (100) | 1 (33.3) | 1.000 | 1.000 |
| Vomiting, n (%) | 1 (33.3) | 1 (20) | 1.000 | 1.000 | 0 | 0 | NA | NA |
| Abdominal pain, n (%) | 1 (33.3) | 0 | 0.375 | 1.000 | 0 | 0 | NA | NA |
| Diarrhea, n (%) | 1 (33.3) | 1 (20) | 1.000 | 1.000 | 0 | 0 | NA | NA |
| Fatigue, n (%) | 0 | 1 (20) | 1.000 | 1.000 | 0 | 0 | NA | NA |
| Parameters | Febrile Phase | Defervescence | p-Value | Adjusted p-Value |
|---|---|---|---|---|
| Hemoglobin, g/dL (14.00–18.00) | 14.70 (13.20–14.90) | 15.15 (13.85–15.70) | 0.121 | 1.000 |
| Hematocrit, % (40.00–54.00) | 43.30 (39.60–44.00) | 44.45 (42.93–45.35) | 0.130 | 1.000 |
| Leukocytes/µL (4000–11,000) | 3,900 (1900–3900) | 1900 (1750–2100) | 0.010 | 0.090 |
| Neutrophils/µL (2500–6000) | 2730 (1540–3640) | 1330 (1225–1470) | 0.010 | 0.090 |
| Lymphocytes/µL (1000–4800) | 546 (234–720) | 642 (516–797) | 0.260 | 1.000 |
| Monocytes/µL (300–900) | 156 (75–265) | 130 (60–209) | 0.231 | 1.000 |
| Eosinophils/µL (50–500) | 0 (0–26) | 26 (0–66) | 0.138 | 1.000 |
| Basophils/µL (0–300) | 216 (136–420) | 292 (210–402) | 0.481 | 1.000 |
| Platelets/µL (150,000–450,000) | 174,000 (140,000–214,000) | 103,000 (63,250–172,750) | 0.015 | 0.135 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imad, H.A.; Phadungsombat, J.; Nakayama, E.E.; Chatapat, L.; Pisutsan, P.; Matsee, W.; Piyaphanee, W.; Nguitragool, W.; Shioda, T. A Cluster of Dengue Cases in Travelers: A Clinical Series from Thailand. Trop. Med. Infect. Dis. 2021, 6, 152. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6030152
Imad HA, Phadungsombat J, Nakayama EE, Chatapat L, Pisutsan P, Matsee W, Piyaphanee W, Nguitragool W, Shioda T. A Cluster of Dengue Cases in Travelers: A Clinical Series from Thailand. Tropical Medicine and Infectious Disease. 2021; 6(3):152. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6030152
Chicago/Turabian StyleImad, Hisham A., Juthamas Phadungsombat, Emi E. Nakayama, Lapakorn Chatapat, Phimphan Pisutsan, Wasin Matsee, Watcharapong Piyaphanee, Wang Nguitragool, and Tatsuo Shioda. 2021. "A Cluster of Dengue Cases in Travelers: A Clinical Series from Thailand" Tropical Medicine and Infectious Disease 6, no. 3: 152. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6030152