Drivers of MERS-CoV Emergence in Qatar

 , ,
, ,  , , ,
, , ,
Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Methods
3. Results
3.1. Changes in the Economic Situation
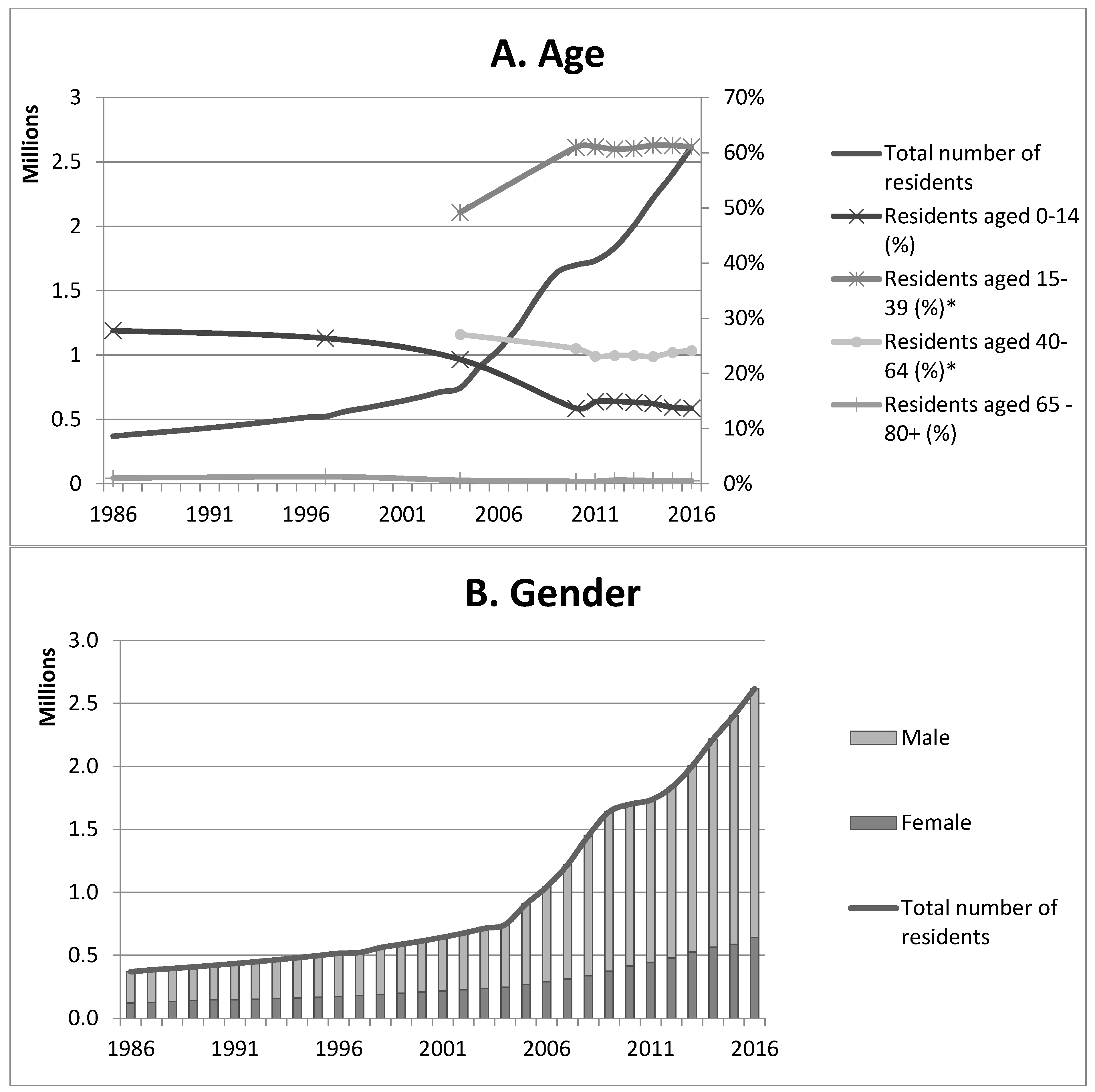
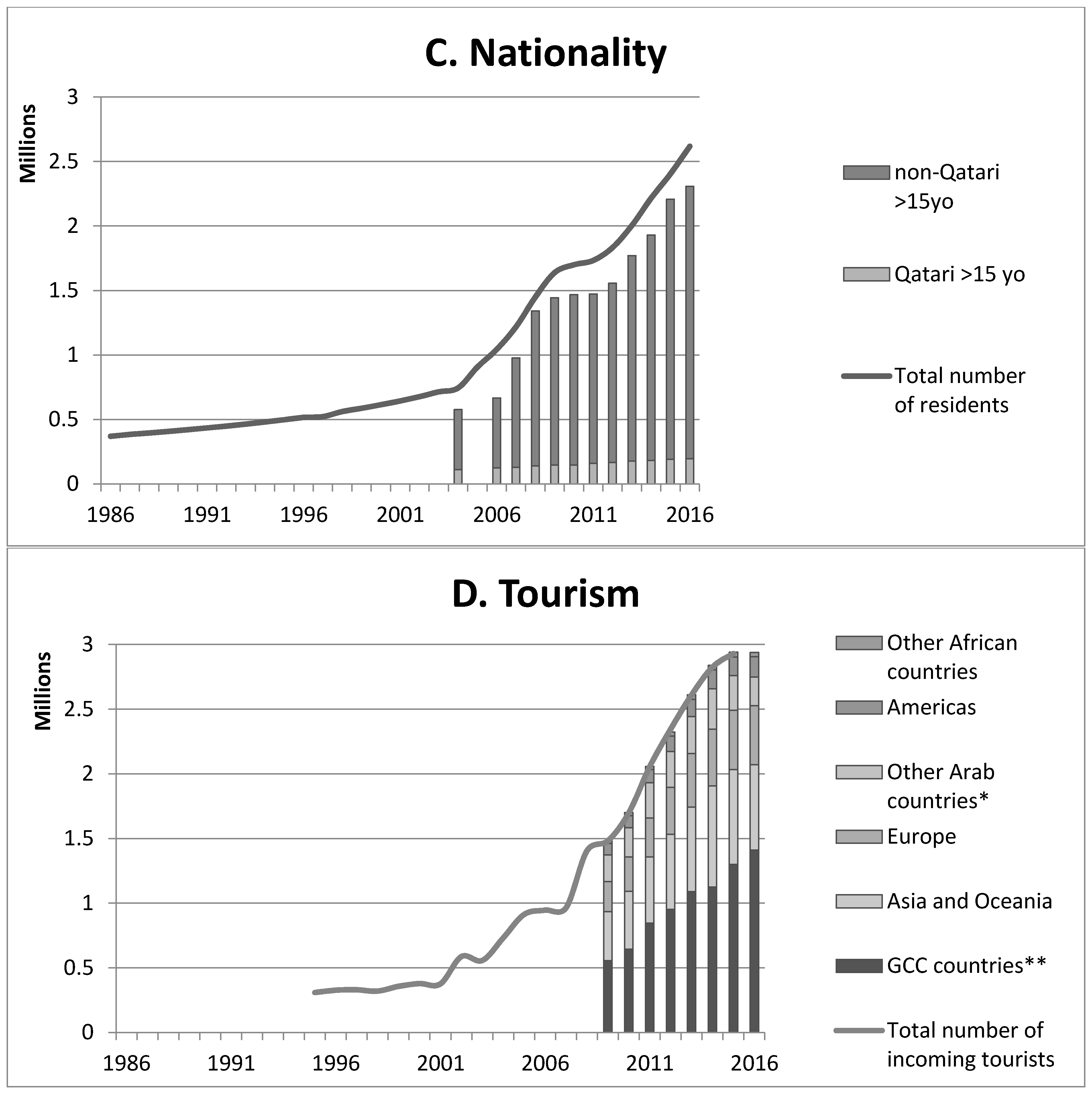
3.2. Changes in Human Demography and Health
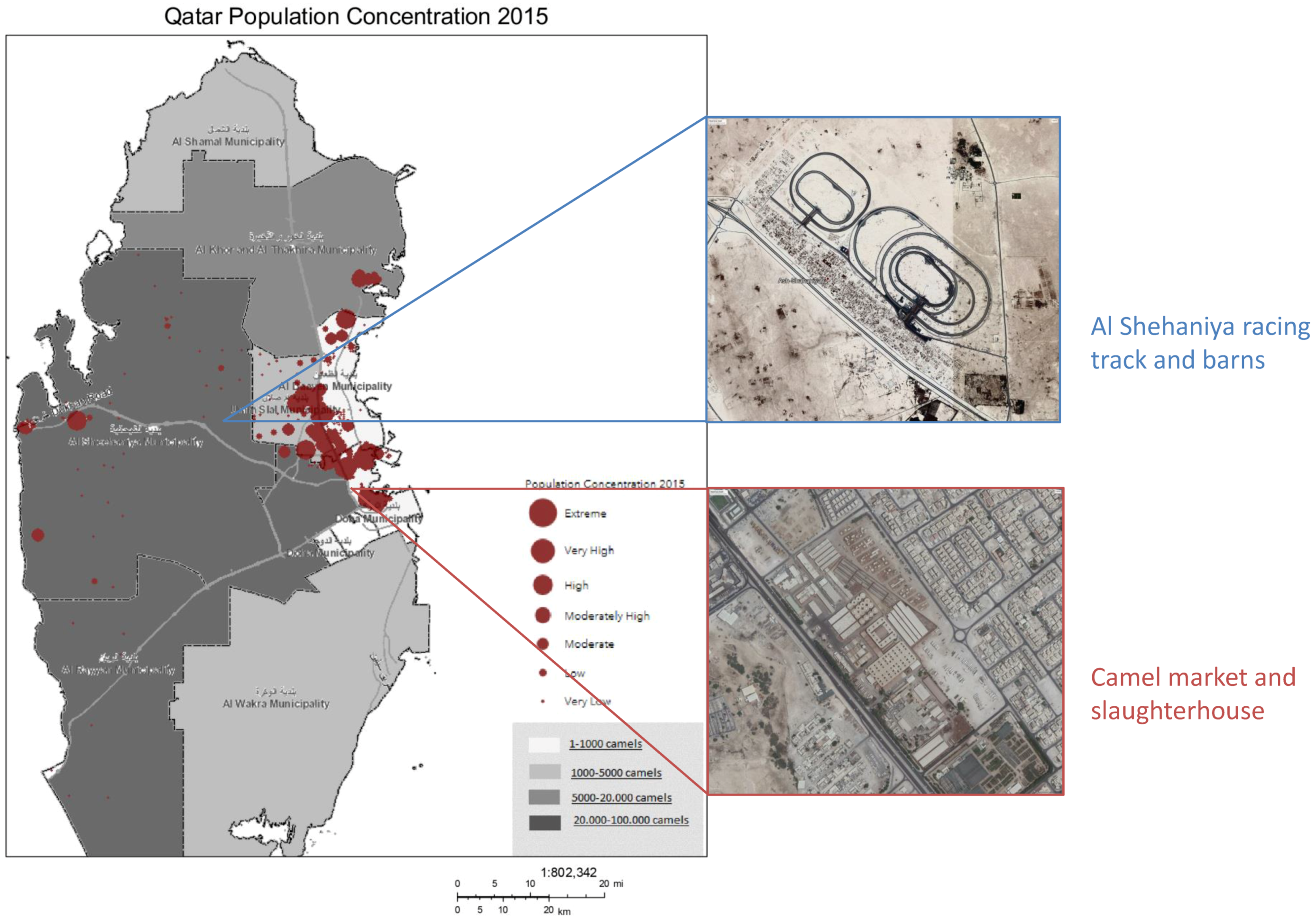
3.3. Changes in Camel Husbandry and Practices
3.4. Changes in Race Camel Farming and Practices
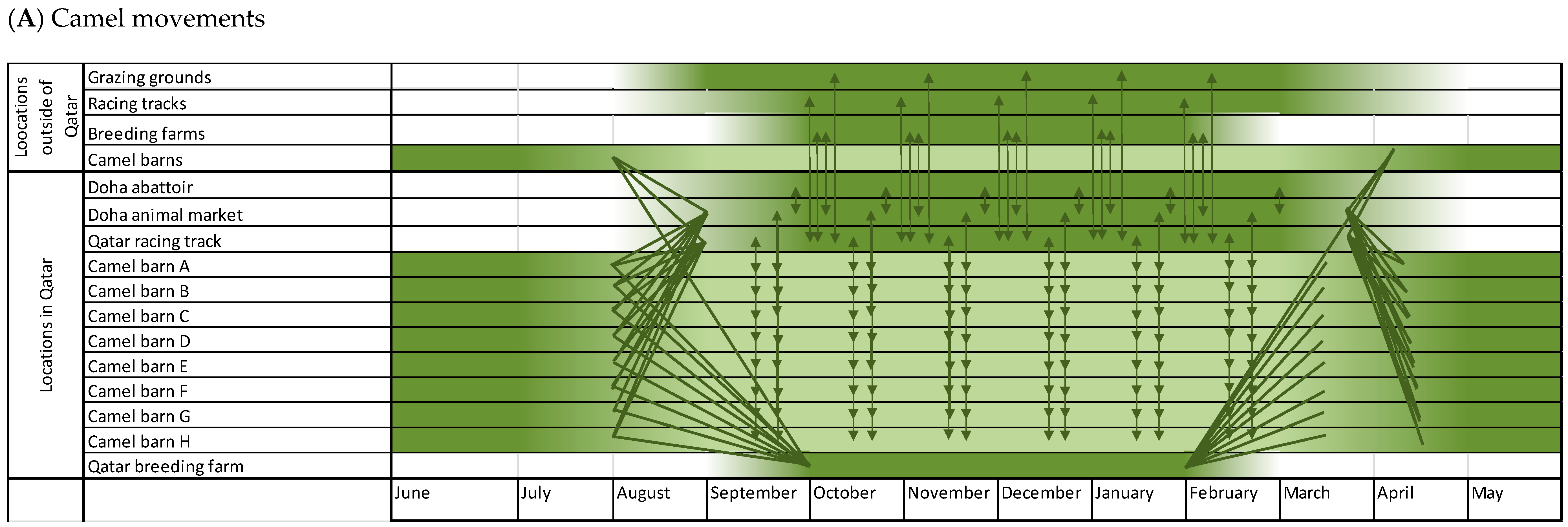
3.5. Changes in International Camel Movements and Travel
3.6. Changes in Camel Trade
3.7. Changes in Use of Camel Meat, Milk, and Urine
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Jones, K.E.; Patel, N.G.; Levy, M.A.; Storeygard, A.; Balk, D.; Gittleman, J.L.; Daszak, P. Global trends in emerging infectious diseases. Nature 2008, 451, 990–994. [Google Scholar] [CrossRef]
- Coltart, C.E.M.; Lindsey, B.; Ghinai, I.; Johnson, A.M.; Heymann, D.L. The Ebola outbreak, 2013–2016: Old lessions for new epidemics. Philos. Trans. R. Soc. B 2017, 372, 20160297. [Google Scholar] [CrossRef]
- Zumla, A.; Hui, D.S.; Perlman, S. Middle East respiratory syndrome. Lancet 2015, 386, 995–1007. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Middle East Respiratory Syndrome Coronavirus. Available online: http://www.who.int/emergencies/mers-cov/en/ (accessed on 13 June 2018).
- Reusken, C.B.; Raj, V.S.; Koopmans, M.P.; Haagmans, B.L. Cross host transmission in the emergency of MERS coronavirus. Curr. Opin. Virol. 2016, 16, 55–62. [Google Scholar] [CrossRef]
- Azhar, E.I.; El-Kafrawy, S.A.; Farraj, S.A.; Hassan, A.M.; Al-Saeed, M.S.; Hashem, A.M.; Madani, T.A. Evidence for camel-to-human transmission of MERS coronavirus. N. Engl. J. Med. 2014, 370, 2499–2505. [Google Scholar] [CrossRef]
- Arwady, M.A.; Alraddadi, B.; Basler, C.; Azhar, E.I.; Abuelzein, E.; Sindy, A.I.; Sadiq, B.M.B.; Althaqafi, A.O.; Shabouni, O.; Banjar, A.; et al. Middle East respiratory syndrome coronavirus transmission coronavirus transmission in extended family, Saudi Arabia, 2014. Emerg. Infect. Dis. 2016, 22, 1395–1402. [Google Scholar] [CrossRef]
- Cho, S.Y.; Kang, J.; Ha, Y.E.; Park, G.E.; Lee, J.Y.; Ko, J.; Lee, J.Y.; Kim, J.M.; Kang, C.; Jo, I.J.; et al. MERS-CoV outbreak following a single patient exposure in an emergency room in South Korea: An epidemiological outbreak study. Lancet 2016, 388, 994–1001. [Google Scholar] [CrossRef]
- Alagaili, A.N.; Briese, T.; Mishra, N.; Kapoor, V.; Sameroff, S.C.; Wit, E.; Munster, V.J.; Hensley, L.E.; Zalmout, I.S.; Kapoor, A.; et al. Middle East respiratory syndrome coronavirus infection in dromedary camels in Saudi Arabia. mBio 2014, 5, e00884-14. [Google Scholar] [CrossRef]
- Lee, J.Y.; Kim, Y.; Chung, E.H.; Kim, D.; Jeong, I.; Lee, J.Y.; Kim, Y.; Chung, E.H.; Kim, D.; Jeong, I.; et al. The clinical and virological features of the first imported case causing MERS-CoV outbreak in South Korea, 2015. BMC Infect. Dis. 2017, 17, 498. [Google Scholar] [CrossRef] [Green Version]
- Müller, M.A.; Corman, V.M.; Jores, J.; Meyer, B.; Younan, M.; Liljander, A.; Bosch, B.; Lattwein, E.; Hilali, M.; Musa, B.E.; et al. MERS coronavirus neutralizing antibodies in camels, Eastern Africa, 1983–1997. Emerg. Infect. Dis. 2014, 20, 2093–2095. [Google Scholar] [CrossRef]
- Hassell, J.M.; Begon, M.; Ward, M.J.; Fèvre, E.M. Urbanization and disease emergence: Dynamics at the wildlife-livestock-human interface. Trends Ecol. Evol. 2017, 32, 55–67. [Google Scholar] [CrossRef]
- Jones, B.A.; Grace, D.; Kock, R.; Alonso, S.; Rushton, J.; Said, M.Y.; KcKeever, D.; Mutua, F.; Young, J.; McDermott, J.; et al. Zoonosis emergence linked to agricultural intensification and environmental change. Proc. Natl. Acad. Sci. USA 2013, 110, 8399–8404. [Google Scholar] [CrossRef] [Green Version]
- Hui, E.K. Reasons for the increase in emerging and re-emerging viral infectious diseases. Microbes Infect. 2006, 8, 905–916. [Google Scholar] [CrossRef]
- Hemida, M.G.; Elmoslemany, A.; Al-Hizab, F.; Alnaeem, A.; Almathen, F.; Faye, B.; Chu, D.K.W.; Perera, R.A.P.M.; Peiris, M. Dromedary camels and the transmission of Middle East respiratory syndrome coronavirus (MERS-CoV). Transbound. Emerg. Dis. 2017, 64, 344–353. [Google Scholar] [CrossRef]
- Cauchemez, S.; Nouvellet, P.; Cori, A.; Jombart, T.; Garske, T.; Clapham, H.; Moore, S.; Mills, H.L.; Salje, H.; Collins, C.; et al. Unraveling the drivers of MERS-CoV transmission. Proc. Natl. Acad. Sci. USA 2016, 113, 9081–9086. [Google Scholar] [CrossRef]
- Hobbs, M. Divers Are a Pearl’s Best Friend: Pearl Diving in the Gulf 1840S–1930S. Qatar Digital Library. Available online: https://www.qdl.qa/en/divers-are-pearl%E2%80%99s-best-friend-pearl-diving-gulf-1840s%E2%80%931930s (accessed on 6 May 2017).
- Al Janahi, B.M. National Identity Formation in Modern Qatar: New Perspective. Master’s Thesis. Available online: http://hdl.handle.net/10576/3247 (accessed on 6 May 2017).
- Crystal, J. Oil and Politics in the Gulf. In Rulers and Merchants in Kuwait and Qatar; CUP: Melbourne, Australia; Cambridge, UK, 1990. [Google Scholar] [CrossRef]
- World Bank. Qatar Country Indicators. Available online: http://data.worldbank.org/country/qatar (accessed on 30 July 2017).
- Embassy of the State of Qatar in Brussels. Qatar History. Available online: http://www.qatarembassy.be/QatarEmbassy/English/History.html (accessed on 6 May 2017).
- Dougherty, R.L. Bedouins of Qatar, Klaus Ferdinand; Thames and Hudson: London, UK, 1995. [Google Scholar] [CrossRef]
- Ministry of Development Planning and Statistics. Quarterly Bulletin for Population and Social Statistics—Third Quarter 2016. Available online: https://www.mdps.gov.qa/en/statistics1/pages/lateststats/20170320.aspx (accessed on 6 May 2017).
- Ministry of Development Planning and Statistics. Labor Force Survey 2016. Available online: http://www.mdps.gov.qa/en/statistics/Statistical Releases/Social/LaborForce/2016/Labour_force_2016_AE.pdf (accessed on 28 June 2017).
- Snoj, J. Population of Qatar by Nationality—2017 Report. Available online: http://priyadsouza.com/population-of-qatar-by-nationality-in-2017 (accessed on 25 July 2017).
- Ministry of Development Planning and Statistics. Population and Social Statistics 2016. Available online: http://www.mdps.gov.qa/en/statistics/Statistical Releases/Population/Population/2016/Population_social_1_2016_AE.pdf (accessed on 26 June 2017).
- Qatar Tourism Authority. Annual Tourism Performance Report. Available online: https://www.visitqatar.qa/corporate/planning/data-and-statistics.html (accessed on 26 June 2017).
- Bakri, A.H. Chronic Disease Risk Factor Surveillance: Qatar Stepwise Report 2012; Supreme Council of Health: Doha, Qatar, 2013. [Google Scholar]
- World Health Organization. Global Health Observatory (GHO) Data: Overweight and Obesity. 2017. Available online: http://www.who.int/gho/ncd/risk_factors/overweight/en/ (accessed on 26 June 2017).
- National Health Authority Qatar. World Health Survey Qatar. Available online: https://0-static--content-springer-com.brum.beds.ac.uk/esm/art%3A10.1186%2F1478-7954-12-18/MediaObjects/12963_2013_244_MOESM1_ESM.pdf (accessed on 26 June 2017).
- World Health Organization. Noncommunicable Diseases and Their Risk Factors; STEPwise Approach to Surveillance (STEPS). Available online: http://www.who.int/ncds/surveillance/steps/en/ (accessed on 26 June 2017).
- World Bank. Death Rate, Crude Death. Available online: https://data.worldbank.org/indicator/SP.DYN.CDRT.IN (accessed on 26 June 2017).
- Camel Racing Committee. The Reports of The Camel Racing Organizing Committee; Ministry of Culture and Sport: Doha, Qatar, 2016.
- Department of Animal Resources. Yearbook of Animal Statistics 2015; Ministry of Municipality and Environment: Doha, Qatar, 2016.
- World Organisation for Animal Health (OIE). Animal Population; World Animal Health Information Database (WAHIS Interface)—Version 1. Available online: https://www.oie.int/wahis_2/public/wahid.php/Countryinformation/Animalpopulation (accessed on 26 June 2017).
- Ministry of Municipality and Environment. Doha, Qatar. Available online: http://www.mme.gov.qa/cui/index.dox?siteID=2 ,2014 (accessed on 26 June 2017).
- Ministry of Development Planning and Statics. Environment Statistics Annual Report. 2013; Ministry of Development Planning and Statics: Doha, Qatar, 2014.
- Ministry of Development Planning and Statistics. Environment Statistics in the State of Qatar. Doha-Qatar 2015. Available online: https://www.mdps.gov.qa/en/statistics/Statistical%20Releases/Environmental/EnvironmentalStatistics/Environment_QSA_EN_2015.pdf (accessed on 26 June 2017).
- Supreme Council for Environment and Natural Reserves. Protected Area Action Plan 2008–2013, Conversion of Biological Diversity (CBD). Available online: https://www.cbd.int/doc/world/qa/qa-nbsap-oth-en.pdf (accessed on 26 June 2017).
- Elford, C.J. Opportunities for the Sustainable Use of the Camel in Qatar. Master’s Thesis, Virginia Commonwealth University, Richmond, VA, USA, 2013. Available online: https://core.ac.uk/download/pdf/51293060.pdf (accessed on 17 July 2017).
- Zaki, A.M.; Boheemen, S.V.; Bestebroer, T.M.; Osterhaus, A.D.; Fouchier, R.A. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N. Engl. J. Med. 2012, 367, 1814–1820. [Google Scholar] [CrossRef]
- Khalfallah, A.I.; Lu, X.; Mubarak, A.I.A.; Dalab, A.H.S.; Al-Busadah, K.A.S.; Erdman, D.D. MERS-CoV in upper respiratory tract and lungs of dromedary camels, Saudi Arabia, 2013–2014. Emerg. Infect. Dis. 2015, 21, 1153–1158. [Google Scholar] [CrossRef]
- Badawi, A.; Ryo, S.G. Prevalence of comorbidities in the Middle East respiratory syndrome coronavirus (MERS-CoV): A systematic review and meta-analysis. Int. J. Infect. Dis. 2016, 49, 129–133. [Google Scholar] [CrossRef]
- Lu, G.; Wang, Q.; Gao, G.F. Bat-to-human: Spike features determining ‘host jump’ of coronaviruses SARS-CoV, MERS-CoV, and beyond. Trends Microbiol. 2015, 23, 468–478. [Google Scholar] [CrossRef]
- Letko, M.; Miazgowicz, K.; McMinn, R.; Seifert, S.N.; Sola, I.; Enjuanes, L.; Carmody, A.; van Doremalen, N.; Munster, V. Adaptive Evolution of MERS-CoV to Species Variation in DPP4. Cell Rep. 2018, 24, 1730–1737. [Google Scholar] [CrossRef]
- Adney, D.R.; Doremalen, N.V.; Brown, V.R.; Bushmaker, T.; Scott, D.; Wit, E.D.; Bowen, R.A.; Munster, V.J. Replication and shedding of MERS-CoV in upper respiratory tract of inoculated dromedary camels. Emerg. Infect. Dis. 2014, 20, 1999–2005. [Google Scholar] [CrossRef]
- Chu, D.K.W.; Hui, K.P.Y.; Perera, R.A.P.M.; Miguel, E.; Niemeyer, D.; Zhao, J.; Channappanavar, R.; Dudas, G.; Oladipo, J.O.; Traoré, A.; et al. MERS coronaviruses from camels in Africa exhibit region-dependent genetic diversity. Proc. Natl. Acad. Sci. USA 2018, 115, 3144–3149. [Google Scholar] [CrossRef] [Green Version]








© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farag, E.; Sikkema, R.S.; Vinks, T.; Islam, M.M.; Nour, M.; Al-Romaihi, H.; Al Thani, M.; Atta, M.; Alhajri, F.H.; Al-Marri, S.; et al. Drivers of MERS-CoV Emergence in Qatar. Viruses 2019, 11, 22. https://0-doi-org.brum.beds.ac.uk/10.3390/v11010022
Farag E, Sikkema RS, Vinks T, Islam MM, Nour M, Al-Romaihi H, Al Thani M, Atta M, Alhajri FH, Al-Marri S, et al. Drivers of MERS-CoV Emergence in Qatar. Viruses. 2019; 11(1):22. https://0-doi-org.brum.beds.ac.uk/10.3390/v11010022
Chicago/Turabian StyleFarag, Elmoubasher, Reina S. Sikkema, Tinka Vinks, Md Mazharul Islam, Mohamed Nour, Hamad Al-Romaihi, Mohammed Al Thani, Muzzamil Atta, Farhoud H. Alhajri, Salih Al-Marri, and et al. 2019. "Drivers of MERS-CoV Emergence in Qatar" Viruses 11, no. 1: 22. https://0-doi-org.brum.beds.ac.uk/10.3390/v11010022