
Long-Term Longitudinal Evaluation of Six Commercial Immunoassays for the Detection of IgM and IgG Antibodies against SARS CoV-2

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Assays
2.3. Analysis
3. Results
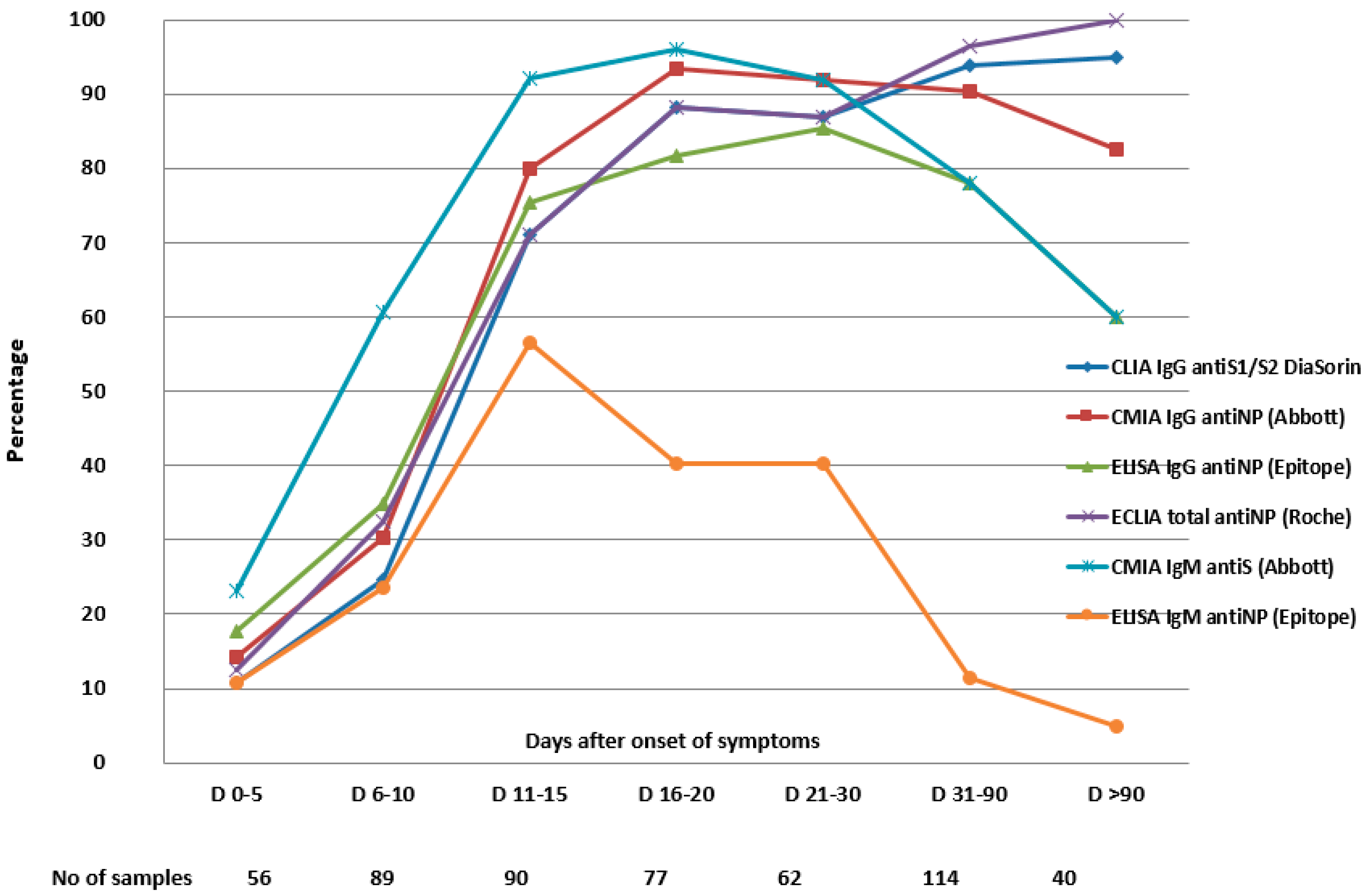
3.1. Sensitivity Dynamics and Specificity of the Assays Detecting IgG Antibodies
3.2. The Sensitivity Dynamics and the Specificity of the Assays Detecting IgM Antibodies
3.3. The Agreement between the Assays
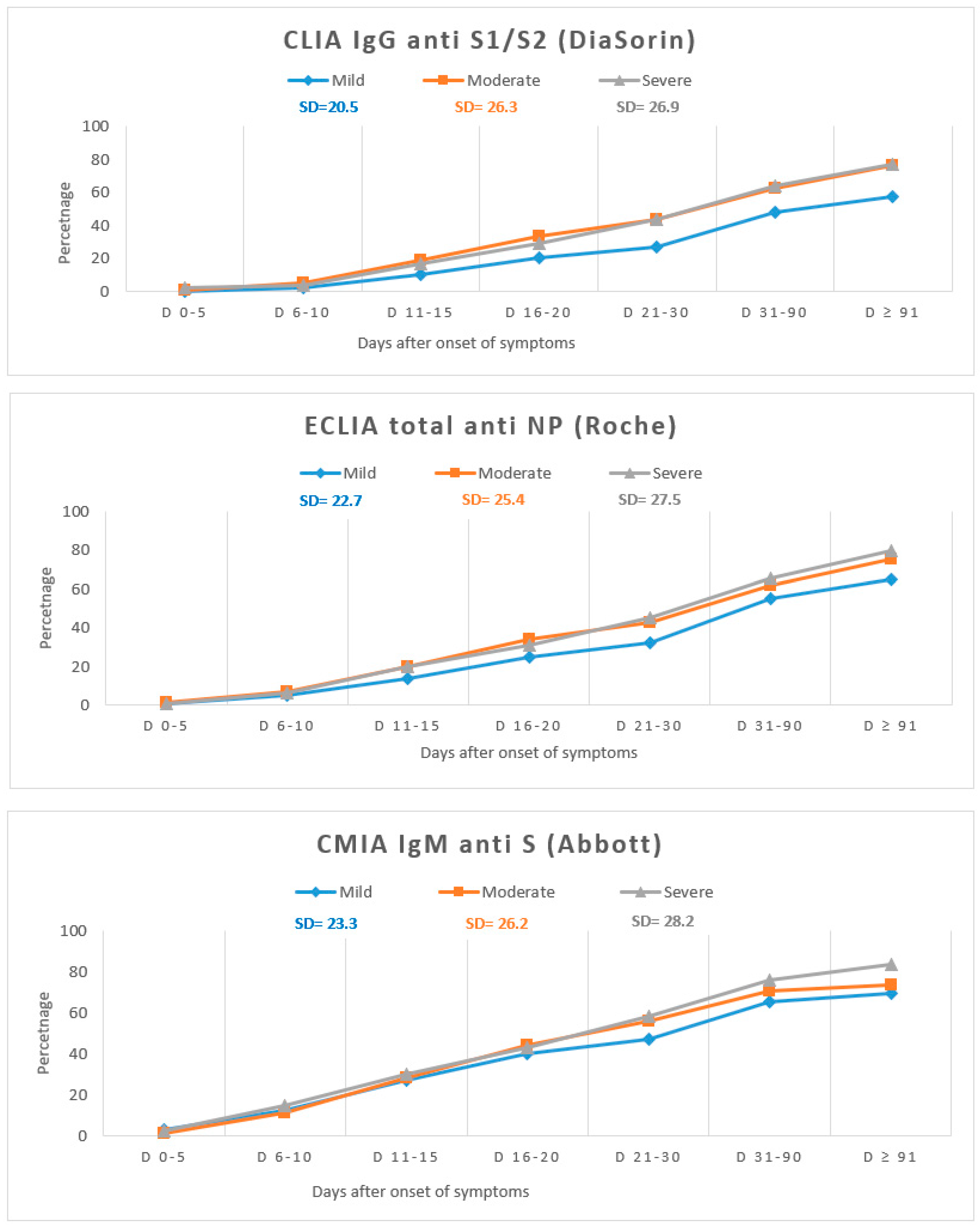
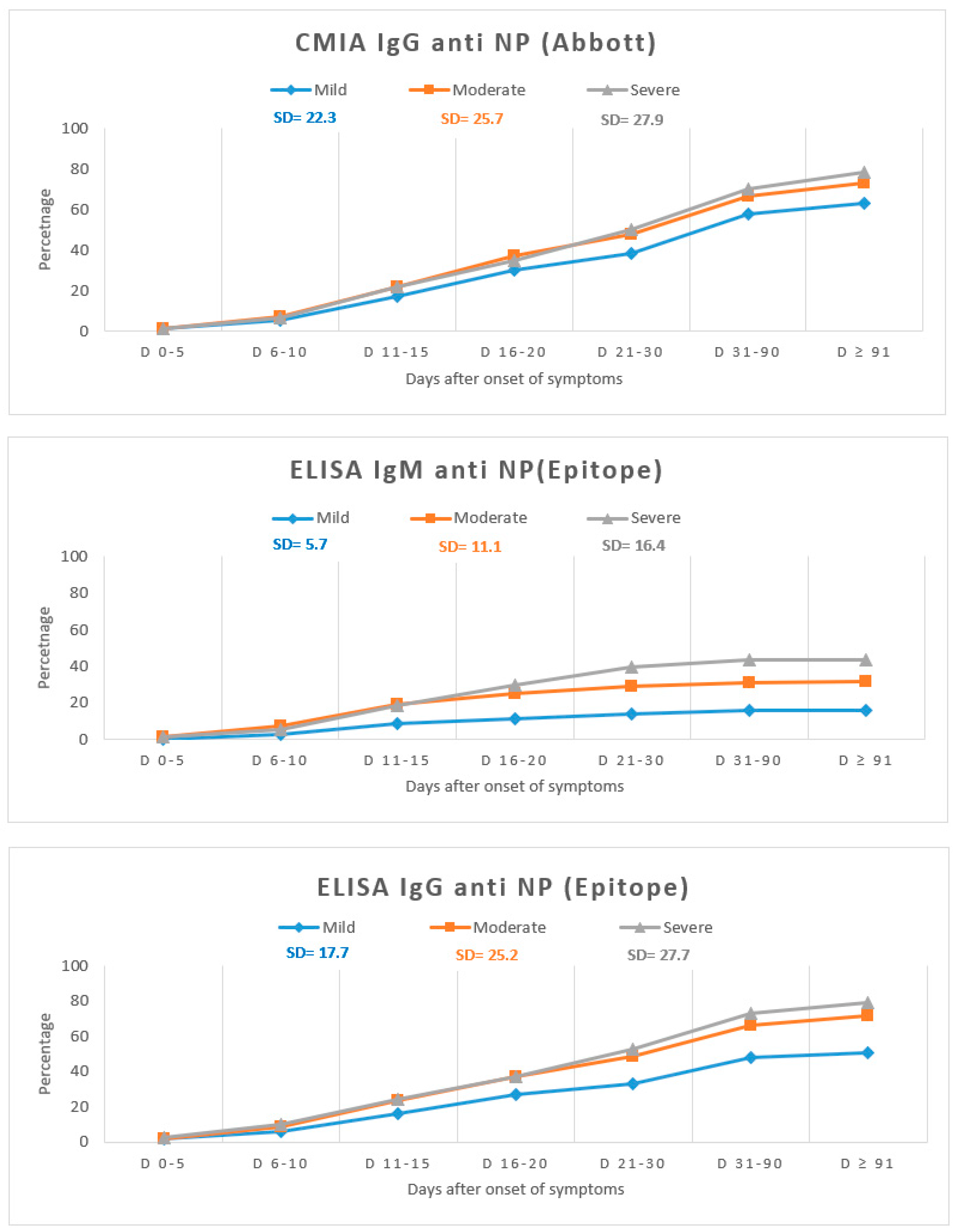
3.4. Antibody Dynamics According to the Disease Severity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Acuti Martellucci, C.; Flacco, M.E.; Cappadona, R.; Bravi, F.; Mantovani, L.; Manzoli, L. SARS-CoV-2 pandemic: An overview. Adv. Biol. Regul. 2020, 77, 100736. [Google Scholar] [CrossRef] [PubMed]
- Theel, E.S.; Harring, J.; Hilgart, H.; Granger, D. Performance Characteristics of Four High-Throughput Immunoassays for Detection of IgG Antibodies against SARS-CoV-2. J. Clin. Microbiol. 2020, 58, e01243-2. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.; Liu, S.; Potula, H.H.; Bhargava, P.; Cruz, I.; Force, D.; Bazerbashi, A.; Ramasamy, R. IgG and IgM antibody formation to spike and nucleocapsid proteins in COVID-19 characterized by multiplex immunoblot assays. BMC Infect. Dis. 2021, 325. [Google Scholar] [CrossRef]
- Meyer, B.; Drosten, C.; Müller, M.A. Serological assays for emerging coronaviruses: Challenges and pitfalls. Virus Res. 2014, 194, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.J.Y.; Lee, K.S.; Ong, C.W.; Chan, M.Y.; Ang, L.W.; Leo, Y.S.; Chen, M.I.; Lye, D.C.B.; Young, B.E. Diagnostic performance of COVID-19 serological assays during early infection: A systematic review and meta-analysis of 11 516 samples. Influenza Respir. Viruses 2021, 20, 10. [Google Scholar] [CrossRef]
- Garcia-Beltran, W.F.; Lam, E.C.; Astudillo, M.G.; Yang, D.; Miller, T.E.; Feldman, J.; Hauser, B.M.; Caradonna, T.M.; Clayton, K.L.; Nitido, A.D.; et al. COVID-19-neutralizing antibodies predict disease severity and survival. Cell 2021, 184, 476–488. [Google Scholar] [CrossRef] [PubMed]
- Venter, M.; Richter, K. Towards effective diagnostic assays for COVID-19: A review. J. Clin. Pathol. 2020, 73, 370–377. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease (COVID19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 10 April 2021).
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Wang, X.; Yuan, J.; Li, T.; Li, J.; et al. Antibody Responses to SARS-CoV-2 in Patients with Novel Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 71, 2027–2034. [Google Scholar] [CrossRef] [PubMed]
- Wolfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [Green Version]
- Long, Q.X.; Liu, B.Z.; Deng, H.J.; Wu, G.C.; Deng, K.; Chen, Y.K.; Liao, P.; Qiu, J.F.; Lin, Y.; Cai, X.F.; et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat. Med. 2020, 26, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Wang, M.; Zuo, Z.; Fan, C.; Ye, F.; Cai, Z.; Wang, Y.; Cui, H.; Pan, K.; Xu, A. Diagnostic value and dynamic variance of serum antibody in coronavirus disease 2019. Int. J. Infect. Dis. 2020, 94, 49–52. [Google Scholar] [CrossRef]
- Hanson, K.E.; Caliendo, A.M.; Arias, C.A.; Englund, J.A.; Hayden, M.K.; Lee, M.J.; Loeb, M.; Patel, R.; Altayar, O.; El Alayli, A.; et al. Infectious Diseases Society of America Guidelines on the Diagnosis of COVID-19: Serologic Testing; Version 2.0.0; Infectious Diseases Society of America: Arlington, VA, USA, 2020; Available online: https://www.idsociety.org/practice-guideline/covid-19-guideline-diagnostics/ (accessed on 6 May 2021).
- Orner, E.P.; Rodgers, M.A.; Hock, K.; Tang, M.S.; Taylor, R.; Gardiner, M.; Olivo, A.; Fox, A.; Prostko, J.; Cloherty, G.; et al. Comparison of SARS-CoV-2 IgM and IgG seroconversion profiles among hospitalized patients in two US cities. Diagn. Microbiol. Infect. Dis. 2021, 99, 115300. [Google Scholar] [CrossRef] [PubMed]
- Ng, D.L.; Goldgof, G.M.; Shy, B.R.; Levine, A.G.; Balcerek, J.; Bapat, S.P.; Prostko, J.; Rodgers, M.; Coller, K.; Pearce, S.; et al. SARS-CoV-2 seroprevalence and neutralizing activity in donor and patient blood from the San Francisco Bay Area. Nat. Commun. 2020, 11, 4698. [Google Scholar] [CrossRef]
- Mackey, K.; Arkhipova-Jenkins, I.; Armstrong, C.; Gean, E.; Anderson, J.; Paynter, R.A.; Helfand, M. Antibody Response Following SARS-CoV-2 Infection and Implications for Immunity: A Rapid Living Review; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2021. [Google Scholar] [CrossRef]
- Risch, M.; Weber, M.; Thiel, S.; Grossmann, K.; Wohlwend, N.; Lung, T.; Hillmann, D.; Ritzler, M.; Ferrara, F.; Bigler, S.; et al. Temporal Course of SARS-CoV-2 Antibody Positivity in Patients with COVID-19 following the First Clinical Presentation. BioMed Res. Int. 2020, 2020, 9878453. [Google Scholar] [CrossRef] [PubMed]
- Brochot, E.; Demey, B.; Touzé, A.; Belouzard, S.; Dubuisson, J.; Schmit, J.L.; Duverlie, G.; Francois, C.; Castelain, S.; Helle, F. Anti-spike; Anti-nucleocapsid and Neutralizing Antibodies in SARS-CoV-2 Inpatients and Asymptomatic Individuals. Front. Microbiol. 2020, 11, 2468. [Google Scholar] [CrossRef]
- To, K.K.; Tsang, O.T.; Leung, W.S.; Tam, A.R.; Wu, T.C.; Lung, D.C.; Yip, C.C.; Cai, J.P.; Chan, J.M.; Chik, T.S.; et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: An observational cohort study. Lancet Infect. Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Favresse, J.; Eucher, C.; Elsen, M.; Gillot, C.; Van Eeckhoudt, S.; Dogné, J.M.; Douxfils, J. Persistence of Anti-SARS-CoV-2 Antibodies Depends on the Analytical Kit: A Report for Up to 10 Months after Infection. Microorganisms 2021, 9, 556. [Google Scholar] [CrossRef] [PubMed]
- Muecksch, F.; Wise, H.; Batchelor, B.; Squires, M.; Semple, E.; Richardson, C.; McGuire, J.; Clearly, S.; Furrie, E.; Neil, G.; et al. Longitudinal analysis of clinical serology assay performance and neutralising antibody levels in COVID19 convalescents. J. Infect. Dis. 2021, 223, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Whitman, J.D.; Hiatt, J.; Mowery, C.T.; Shy, B.R.; Yu, R.; Yamamoto, T.N.; Rathore, U.; Goldgof, G.M.; Whitty, C.; Woo, J.M.; et al. Evaluation of SARS-CoV-2 serology assays reveals a range of test performance. Nat. Biotechnol. 2020, 38, 1174–1183. [Google Scholar] [CrossRef]
- Lagerqvist, N.; Maleki, K.T.; Verner-Carlsson, J.; Olausson, M.; Dillner, J.; Wigren Byström, J.; Monsen, T.; Eriksson, J.; Bogdanovic, G.; Muschiol, S.; et al. Evaluation of 11 SARS-CoV-2 antibody tests by using samples from patients with defined IgG antibody titers. Sci. Rep. 2021, 7614. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Spijker, R.; Taylor-Phillips, S.; Adriano, A.; Beese, S.; Dretzke, J.; Ferrante di Ruffano, L.; et al. Antibody tests for identification of current and past infection with SARS-CoV-2. Cochrane Database Syst. Rev. 2020, CD013652. [Google Scholar] [CrossRef]
- Favresse, J.; Cadrobbi, J.; Eucher, C.; Elsen, M.; Laffineur, K.; Dogné, J.M.; Douxfils, J. Clinical performance of three fully automated anti-SARS-CoV-2 immunoassays targeting the nucleocapsid or spike proteins. J. Med. Virol. 2020, 93, 2262–2269. [Google Scholar] [CrossRef] [PubMed]
- Van Elslande, J.; Decru, B.; Jonckheere, S.; Van Wijngaerden, E.; Houben, E.; Vandecandelaere, P.; Indevuyst, C.; Depypere, M.; Desmet, S.; André, E.; et al. Antibody response against SARS-CoV-2 spike protein and nucleoprotein evaluated by four automated immunoassays and three ELISAs. Clin. Microbiol Infect. 2020, 26, 1557.e1–1557.e7. [Google Scholar] [CrossRef]
- National SARS-CoV-2 Serology Assay Evaluation Group. Performance characteristics of five immunoassays for SARS-CoV-2: A head-to-head benchmark comparison. Lancet Infect. Dis. 2020, 20, 1390–1400. [Google Scholar] [CrossRef]
- Gudbjartsson, D.F.; Norddahl, G.L.; Melsted, P.; Gunnarsdottir, K.; Holm, H.; Eythorsson, E.; Arnthorsson, A.O.; Helgason, D.; Bjarnadottir, K.; Ingvarsson, R.F.; et al. Humoral Immune Response to SARS-CoV-2 in Iceland. N. Engl. J. Med. 2020, 383, 1724–1734. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.; Feng, Y.; Mo, X.; Zheng, P.; Wang, Q.; Li, P.; Peng, P.; Liu, X.; Chen, Z.; Huang, H.; et al. Kinetics of SARS-CoV-2 specific IgM and IgG responses in COVID-19 patients. Emerg. Microbes Infect. 2020, 9, 940–948. [Google Scholar] [CrossRef]
- Choe, P.G.; Kim, K.H.; Kang, C.K.; Suh, H.J.; Kang, E.; Lee, S.Y.; Kim, N.J.; Yi, J.; Park, W.B.; Oh, M.D. Antibody Responses 8 Months after Asymptomatic or Mild SARS-CoV-2 Infection. Emerg. Infect. Dis. 2021, 27, 928–931. [Google Scholar] [CrossRef] [PubMed]
- Peluso, M.J.; Takahashi, S.; Hakim, J.; Kelly, J.D.; Torres, L.; Iyer, N.S.; Turcios, K.; Janson, O.; Munter, S.E.; Thanh, C.; et al. SARS-CoV-2 antibody magnitude and detectability are driven by disease severity, timing, and assay. medRxiv 2021. [Google Scholar] [CrossRef]
- Gorse, G.J.; Patel, G.B.; Vitale, J.N.; O’Connor, T.Z. Prevalence of antibodies to four human coronaviruses is lower in nasal secretions than in serum. Clin. Vaccine Immunol. 2010, 17, 1875–1880. [Google Scholar] [CrossRef] [Green Version]
- Watson, J.; Richter, A.; Deeks, J. Testing for SARS-CoV-2 antibodies. BMJ. 2020, 370, m3325. [Google Scholar] [CrossRef]
- Hu, W.T.; Howell, J.C.; Ozturk, T.; Benameur, K.; Bassit, L.C.; Ramonell, R.; Cashman, K.S.; Pirmohammed, S.; Roback, J.D.; Marconi, V.C.; et al. Antibody Profiles According to Mild or Severe SARS-CoV-2 Infection, Atlanta, Georgia, USA. Emerg. Infect. Dis. 2020, 26, 2974–2978. [Google Scholar] [CrossRef] [PubMed]
- Young, B.E.; Ong, S.W.X.; Ng, L.F.P.; Anderson, D.E.; Chia, W.N.; Chia, P.Y.; Ang, L.W.; Mak, T.M.; Kalimuddin, S.; Chai, L.Y.A.; et al. Singapore 2019 Novel Coronavirus Outbreak Research team. Viral dynamics and immune correlates of COVID-19 disease severity. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic COVID-19 Study Population (n = 156) | |
|---|---|
| Age, median IQR) | 50.5 (40–59) |
| Male sex N (%) | 93 (59.6) |
| Chronic Medical Condition | |
| Hypertension N (%) | 49 (31.4) |
| Congestive heart failure N (%) | 6 (3.8) |
| Coronary artery disease N (%) | 12 (7.6) |
| Prior stroke N (%) | 6 (3.8) |
| Type 2 diabetes mellitus (%) | 25 (16) |
| Obesity N (%) | 22 (14.1) |
| Cancer (solid or hematological) | 8 (5.1) |
| Chronic liver disease N (%) | 7 (4.4) |
| Chronic kidney disease N (%) | 3 (1.9) |
| Asthma or other chronic respiratory diseases N (%) | 7 (4.4) |
| Systemic inflammatory diseases N (%) | 1 (0.6) |
| Other immunosuppression conditions N (%) | 2 (1.2) |
| Duration of Symptoms at Inclusion in the Study, Median (IQR) | |
| Disease severity | 16 (10–22) |
| Mild N (%) | 62 (39.7%) |
| Moderate N (%) | 53 (33.9%) |
| Severe N (%) | 41 (26.2%) |
| Overall Sensitivity N, % (95% CI) | D 0–5 N, % (95% CI) | D 6–10 % (95% CI) | D 11–15 % (95% CI) | D 16–20 % (95% CI) | D 21–30 % (95% CI) | D 31–90 % (95% CI) | D ≥ 91 % (95% CI) | Specificity % (95% CI) | |
|---|---|---|---|---|---|---|---|---|---|
| Sample No. | 528 | 56 | 89 | 90 | 77 | 62 | 114 | 40 | 161 |
| CMIA (Abbott) | |||||||||
| IgM antiS | 394 74.6 (70.6–78.2) | 13 23.2 (12.9–36.4) | 54 60.6 (49.7–70.8) | 83 92.2 (84.6–96.8) | 74 96.1 (89–99.1) | 57 91.9 (82.1–97.3) | 89 78 (69.3–85.2) | 24 60 (43.3–75.1) | 2 98,7 (95.5–99.8) |
| IgG antiNP | 372 70.4 (66.3–74.3) | 8 14.2 (6.3–26.2) | 27 30.3 (21–40.9) | 72 80 (70.2–87.6) | 72 93.5 (85.4–97.8) | 57 91.9 (82,1–97.3) | 103 90.3 (83.3–95) | 33 82.5 (67.2–92.6) | 2 98,7 (95.5–99.8) |
| IgM/IgG * | 437 82.7 (79.2–85.8) | 13 23.2 (12.9–36.4) | 56 62.9 (52–72.9) | 86 95.5 (89–98.7) | 75 97.4 (90.9–99.6) | 60 96.7 (88.8–99.6) | 111 97.3 (92.5–99.4) | 36 90 (76.3–97.2) | 4 97.5 (93.7–99.3) |
| ELISA (Epitope) | |||||||||
| IgM antiNP | 149 28.2 (24.4–32.2) | 6 10.7 (4–21.8) | 21 23.5 (15.2–33.7) | 51 56.6 (45.8–67) | 31 40.2 (29.2–52) | 25 40.3 (28.5–53.5) | 13 11.4 (6.21–18.87) | 2 5 (0.6–16.9) | 4 97.5 (93.7–99.3) |
| IgG antiNP | 343 64.9 (60.7–69) | 10 17.8 (8.9–30.4) | 31 34.8 (25–45.6) | 68 75.5 (65.3–84) | 65 81.8 (71.3–89.6) | 54 85.4 (74.2–93.1) | 90 78 (69.3–85.2) | 25 60 (43.3–75.1) | 3 98.1 (94.6–99.6) |
| IgM/IgG * | 359 68 (63.8–72) | 10 17.9 (8.9–30.4) | 33 37.1 (27.1–48) | 73 81.1 (71.5–88.6) | 66 85.7 (75.9–93) | 58 93.5 (84.3–98.2) | 92 80.7 (72.2–87.5) | 27 67.5 (50.9–81.4) | 5 96.2 (92–98.6) |
| Sample No. | 559 | 56 | 89 | 90 | 77 | 62 | 114 | 71 | 161 |
| CLIA IgG antiS1/S2 DiaSorin | 390 69.8 (65.7–73.5) | 6 10.7 (4–21.8) | 22 24.7 (16.1–35) | 64 71.1 (60.6–80.1) | 68 88.3 (78.9–94.5) | 54 87 (76.1–94.2) | 107 93.8 (87.7–97.5) | 69 97.2 (83–99.3) | 2 98.7 (95.5–99.8) |
| Sample No. | 559 | 56 | 89 | 90 | 77 | 62 | 114 | 71 | 158 |
| ECLIA total antiNP Roche | 403 70.4 (66.3–74.3) | 7 12.5 (5.1–24) | 29 32.5 (23–43.3) | 64 71.1 (60.6–80.1) | 68 88.3 (78.9–94.5) | 54 87 (76.1–94.2) | 110 96.4 (91.2–99) | 71 100 (91.1–100) | 0 100 (97.7–100) |
| CLIA IgG antiS1/S2 (DiaSorin) | CMIA IgG antiNP (Abbott) | ELISA IgG antiNP (Epitope) | ECLIA Total antiNP (Roche) | CMIA IgM antiS (Abbott) | ELISA IgM antiNP (Epitope) | |
|---|---|---|---|---|---|---|
| IgG/IgM persistently negative N * (%) | 3 (2.3) | 4 (3.1) | 9 (7.0) | 2 (1.5) | 3 (2.3) | 44 (34.3) |
| Patients with seroconversion N * (%) | 112 (87.5) | 110 (85.9) | 107 (83.6) | 108 (84.3) | 102 (79.6) | 70 (54.6) |
| IgG positive patients at inclusion N * (%) | 13 (10.1) | 14 (10.9) | 12 (9.3) | 18 (14.0) | 13 (10.1) | 14 (10.9) |
| Median time (min, max) PSO until seroconversion (days) | 13 (2.36) | 13 (2.35) | 11 (2.30) | 13 (3.36) | 10 (2.22) | 11.5 (3.32) |
| Simultaneous seroconversion N (%) | 47 (57.3%) | IgM and IgG positive at inclusion N (%) | 4 (4.9%) |
| IgM before IgG N (%) | 23 (28.0%) | IgM positive but IgG persistently negative N (%) | 4 (4.9%) |
| IgG before IgM N (%) | 2 (2.4%) | IgG positive but IgM persistently negative N (%) | 2 (2.4%) |
| ELISA IgG antiNP (Epitope) k, SE of k (95% CI) | CLIA IgG antiS1/S2 (DiaSorin) k, SE of k, (95% CI) | CMIA IgG antiNP (Abbott) k, SE of k, (95% CI) | CMIA IgM antiS (Abbott) k, SE of k (95% CI) | |
|---|---|---|---|---|
| ECLIA total antiNP (Roche) | 0.624, 0.036 (0.55–0.69) moderate | 0.697, 0.034, (0.63–0.76) substantial | 0.773, 0.030 (0.71–0.83) substantial | |
| ELISA IgG antiNP (Epitope) | 0.622, 0.036, (0.55–0.69) moderate | 0.780, 0.029 (0.72–0.83) substantial | ||
| CLIA IgG antiS1/S2 (DiaSorin) | 0.706, 0.034, (0.64–0.77) substantial | |||
| ELISA IgM antiNP (Epitope) | 0.192, 0.024, (0.14–0.23) fair |
| D 0–10 | D 11–15 | D 16–20 | D 21–30 | D 31–90 | D ≥ 91 | TOTAL | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Disease severity | N | Median (AU/mL) [IQR] | N | Median (AU/mL) [IQR] | N | Median (AU/mL) [IQR] | N | Median (AU/mL) [IQR] | N | Median (AU/mL) [IQR] | N | Median (AU/mL) [IQR] | N | Median (AU/mL) [IQR] |
| Mild | 66 | 3.8 [3.8–13] | 36 | 11.6 [3.8–88.6] | 33 | 32.4 [7.8–108.7] | 21 | 31.8 [4.6–114.4] | 57 | 61.4 [10.7–112.8] | 25 | 65.2 [15.9–157.6] | 237 | 21.1 [4.3–64.3] |
| Moderate | 48 | 3.8 [3.8–51.6] | 35 | 30.8 [3.8–163] | 31 | 60.5 [13.9–165.4] | 24 | 72.3 [12.8–139.3] | 41 | 102 [52.9–206] | 29 | 131.5 [25.1–511.9] | 208 | 54.4 [13.9– 105] |
| Severe | 31 | 3.8 [3.8–55.5] | 20 | 79 [10.6–156] | 16 | 109.5 [25.3-223.9] | 20 | 135 [49.8–246.1] | 28 | 170 [98.2–340] | 19 | 202 [91.7–806] | 134 | 108 [21.2–177.5] |
| TOTAL | 145 | 3.8 [3.8–30.2] | 91 | 29.2 [3.8–121.6] | 80 | 55 [11.5–152] | 65 | 76.6 [8–186.4] | 126 | 92.2 [22.3–220] | 73 | 96.9 [20.5–462.2] | 581 | 44.6 [7.8–104] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nedelcu, I.; Jipa, R.; Vasilescu, R.; Băicuș, C.; Popescu, C.-I.; Manea, E.; Stoichițoiu, L.E.; Pinte, L.; Damalan, A.; Simulescu, O.; et al. Long-Term Longitudinal Evaluation of Six Commercial Immunoassays for the Detection of IgM and IgG Antibodies against SARS CoV-2. Viruses 2021, 13, 1244. https://0-doi-org.brum.beds.ac.uk/10.3390/v13071244
Nedelcu I, Jipa R, Vasilescu R, Băicuș C, Popescu C-I, Manea E, Stoichițoiu LE, Pinte L, Damalan A, Simulescu O, et al. Long-Term Longitudinal Evaluation of Six Commercial Immunoassays for the Detection of IgM and IgG Antibodies against SARS CoV-2. Viruses. 2021; 13(7):1244. https://0-doi-org.brum.beds.ac.uk/10.3390/v13071244
Chicago/Turabian StyleNedelcu, Iulia, Raluca Jipa, Roxana Vasilescu, Cristian Băicuș, Costin-Ioan Popescu, Eliza Manea, Laura E. Stoichițoiu, Larisa Pinte, Anca Damalan, Oana Simulescu, and et al. 2021. "Long-Term Longitudinal Evaluation of Six Commercial Immunoassays for the Detection of IgM and IgG Antibodies against SARS CoV-2" Viruses 13, no. 7: 1244. https://0-doi-org.brum.beds.ac.uk/10.3390/v13071244