
Estimation of Serial Interval and Reproduction Number to Quantify the Transmissibility of SARS-CoV-2 Omicron Variant in South Korea

 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Source of Data
2.2. Serial Interval and Reproduction Number
3. Results
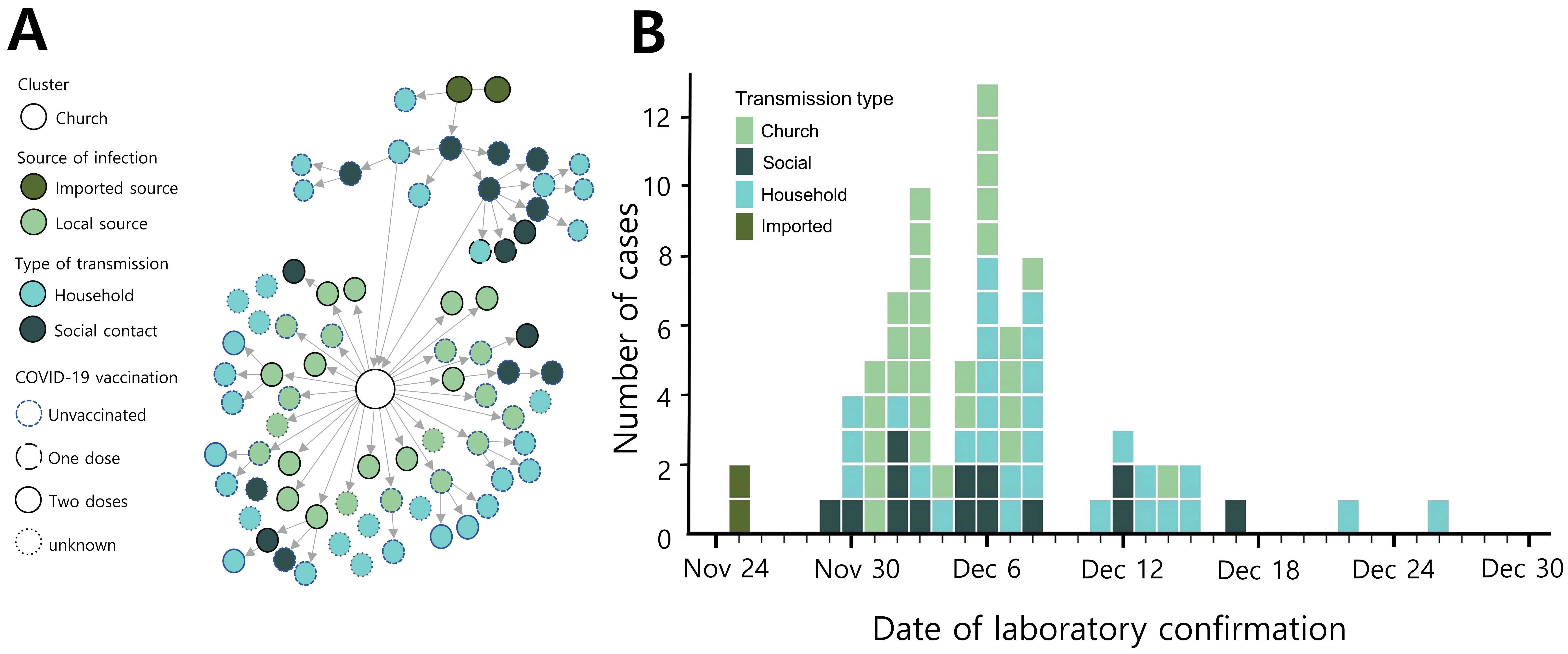
3.1. Description of First Community Outbreak Transmitted from Imported Cases
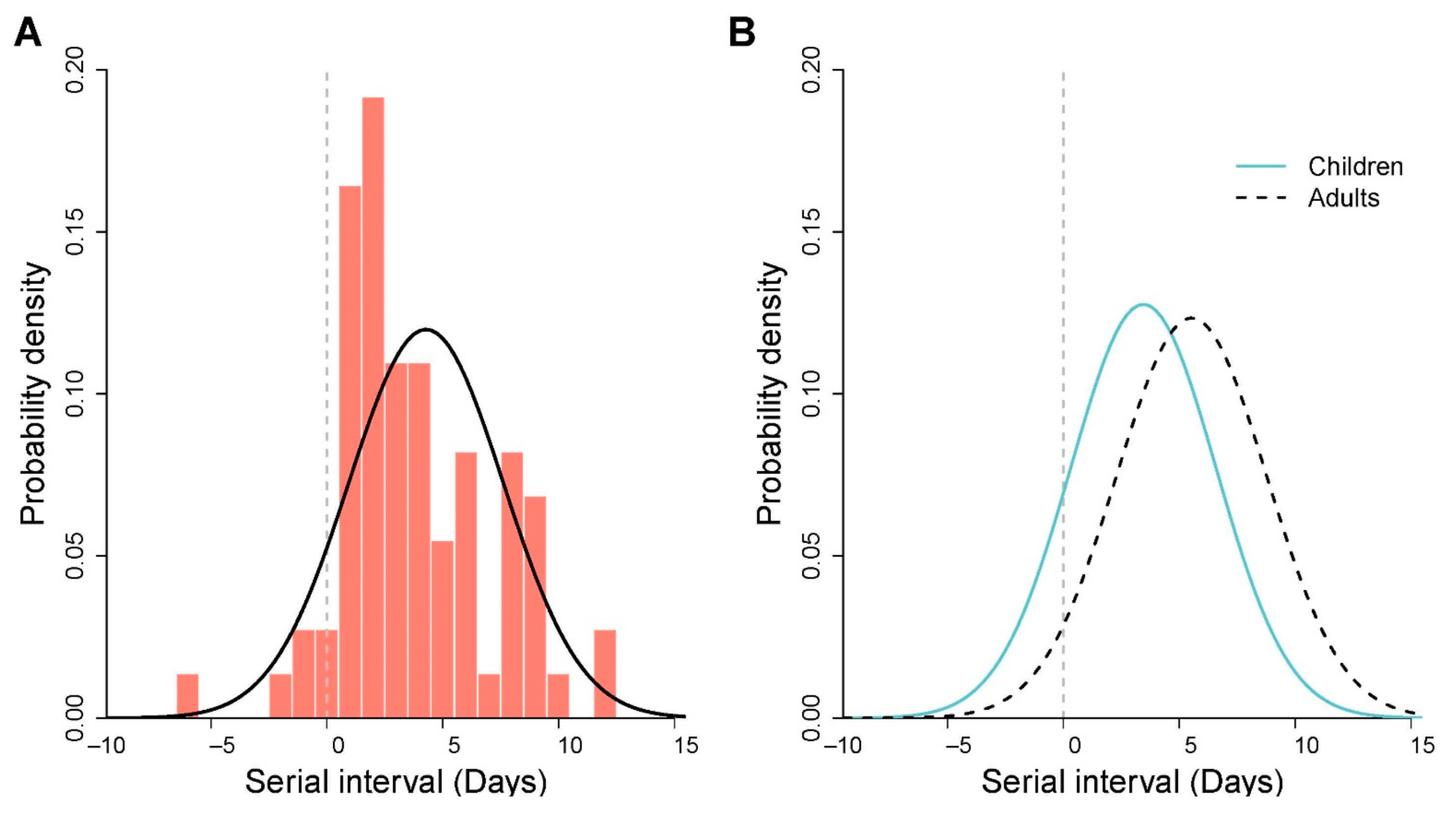
3.2. Estimation of Serial Interval and Reproduction Number
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kim, A. Omicron dominant in South Korea. The Korea Herald. 2022. Available online: http://www.koreaherald.com/view.php?ud=20220124000957 (accessed on 1 March 2022).
- Mannar, D.; Saville, J.W.; Zhu, X.; Srivastava, S.S.; Berezuk, A.M.; Tuttle, K.S.; Marquez, A.C.; Sekirov, I.; Subramaniam, S. SARS-CoV-2 Omicron variant: Antibody evasion and cryo-EM structure of spike protein-ACE2 complex. Science 2022, 375, 760–764. [Google Scholar] [CrossRef] [PubMed]
- Brandal, L.T.; MacDonald, E.; Veneti, L.; Ravlo, T.; Lange, H.; Naseer, U.; Feruglio, S.; Bragstad, K.; Hungnes, O.; Odeskaug, L.E.; et al. Outbreak caused by the SARS-CoV-2 Omicron variant in Norway, November to December 2021. Eurosurveillance 2021, 26, 2101147. [Google Scholar] [CrossRef] [PubMed]
- Jansen, L.; Tegomoh, B.; Lange, K.; Showalter, K.; Figliomeni, J.; Abdalhamid, B.; Iwen, P.C.; Fauver, J.; Buss, B.; Donahue, M. Investigation of a SARS-CoV-2 B.1.1.529 (Omicron) Variant Cluster—Nebraska, November-December 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1782–1784. [Google Scholar] [CrossRef] [PubMed]
- Korea Centers for Disease Control and Prevention Agency. A Total of 5 Confirmed Cases of Omicron Mutated Virus in Korea Urgent Implementation of Additional Measures to Block Inflow and Prevent Spread. Available online: https://nih.go.kr/board/board.es?mid=a40303010000&bid=0015&act=view&list_no=717719 (accessed on 26 January 2022).
- Korea Centers for Disease Control and Prevention Agency. Press Release. Available online: https://www.kdca.go.kr/board/board.es?mid=a20501010000&bid=0015 (accessed on 26 January 2022).
- Incheon Metropolitan City. Incheon City Corona 19 Outbreak and Response Status. Available online: https://www.incheon.go.kr/fileviewer/v/p7PiJFwsAu2 (accessed on 9 December 2021).
- Du, Z.; Xu, X.; Wu, Y.; Wang, L.; Cowling, B.J.; Meyers, L.A. Serial Interval of COVID-19 among Publicly Reported Confirmed Cases. Emerg. Infect. Dis. 2020, 26, 1341–1343. [Google Scholar] [CrossRef] [PubMed]
- Ryu, S.; Ali, S.T.; Jang, C.; Kim, B.; Cowling, B.J. Effect of Nonpharmaceutical Interventions on Transmission of Severe Acute Respiratory Syndrome Coronavirus 2, South Korea, 2020. Emerg. Infect. Dis. 2020, 26, 2406–2410. [Google Scholar] [CrossRef]
- Wallinga, J.; Lipsitch, M. How generation intervals shape the relationship between growth rates and reproductive numbers. Proc. R. Soc. B Biol. Sci. 2007, 274, 599–604. [Google Scholar] [CrossRef]
- Wakefield, J.; Dong, T.Q.; Minin, V.N. Spatio-Temporal Analysis of Surveillance Data; CRC Press: New York, NY, USA, 2020. [Google Scholar]
- Gostic, K.M.; McGough, L.; Baskerville, E.B.; Abbott, S.; Joshi, K.; Tedijanto, C.; Kahn, R.; Niehus, R.; Hay, J.A.; De Salazar, P.M.; et al. Practical considerations for measuring the effective reproductive number, Rt. PLoS Comput. Biol. 2020, 16, e1008409. [Google Scholar] [CrossRef]
- Dietz, K. The estimation of the basic reproduction number for infectious diseases. Stat. Methods Med. Res. 1993, 2, 23–41. [Google Scholar] [CrossRef]
- Times, N.S. South Korea moves to higher alert over Omicron variant. New Straits Times. 2021. Available online: https://www.straitstimes.com/asia/east-asia/south-korea-study-omicron-covid-19-variant-75-less-likely-to-kill-than-delta (accessed on 1 March 2022).
- See, J.-E. Omicron makes leap to Seoul in 3 int’l students. Korea JoongAng Daily. 2021. Available online: https://koreajoongangdaily.joins.com/2021/12/07/national/socialAffairs/omicron-foreign-students-Seoul-National-University/20211207183322795.html (accessed on 1 March 2022).
- Cho, G.; Kim, S. The first omicron case. Donga. 2021. Available online: https://www.donga.com/news/article/all/20211203/110578739/1 (accessed on 1 March 2022).
- Korea Tourism Organization. Quarantine Exemption for Fully Vaccinated Visitors Starting. 2021. Available online: https://english.visitkorea.or.kr/enu/AKR/FU_EN_15.jsp?gotoPage=5&cid=2723907 (accessed on 9 December 2021).
- Ali, S.T.; Wang, L.; Lau, E.H.Y.; Xu, X.K.; Du, Z.; Wu, Y.; Leung, G.M.; Cowling, B.J. Serial interval of SARS-CoV-2 was shortened over time by nonpharmaceutical interventions. Science 2020, 369, 1106–1109. [Google Scholar] [CrossRef]
- Xu, X.K.; Liu, X.F.; Wu, Y.; Ali, S.T.; Du, Z.; Bosetti, P.; Lau, E.H.Y.; Cowling, B.J.; Wang, L. Reconstruction of Transmission Pairs for Novel Coronavirus Disease 2019 (COVID-19) in Mainland China: Estimation of Superspreading Events, Serial Interval, and Hazard of Infection. Clin. Infect. Dis. 2020, 71, 3163–3167. [Google Scholar] [CrossRef]
- Hwang, H.; Lim, J.S.; Song, S.A.; Achangwa, C.; Sim, W.; Kim, G.; Ryu, S. Transmission dynamics of the Delta variant of SARS-CoV-2 infections in South Korea. J. Infect. Dis. 2021, 225, 793–799. [Google Scholar] [CrossRef]
- Ryu, S.; Ali, S.T.; Noh, E.; Kim, D.; Lau, E.H.Y.; Cowling, B.J. Transmission dynamics and control of two epidemic waves of SARS-CoV-2 in South Korea. BMC Infect. Dis. 2021, 21, 485. [Google Scholar] [CrossRef]
- Lee, J.J.; Choe, Y.J.; Jeong, H.; Kim, M.; Kim, S.; Yoo, H.; Park, K.; Kim, C.; Choi, S.; Sim, J.; et al. Importation and Transmission of SARS-CoV-2 B.1.1.529 (Omicron) Variant of Concern in Korea, November 2021. J. Korean Med. Sci. 2021, 36, e346. [Google Scholar] [CrossRef]
- Sadarangani, M.; Marchant, A.; Kollmann, T.R. Immunological mechanisms of vaccine-induced protection against COVID-19 in humans. Nat. Rev. Immunol. 2021, 21, 475–484. [Google Scholar] [CrossRef]
- Zimmermann, P.; Curtis, N. Why is COVID-19 less severe in children? A review of the proposed mechanisms underlying the age-related difference in severity of SARS-CoV-2 infections. Arch. Dis. Child. 2020, 106, 429–439. [Google Scholar] [CrossRef]
- Lyngse, F.P.; Kirkeby, C.; Halasa, T.; Andreasen, V.; Skov, R.L.; Moller, F.T.; Krause, T.G.; Molbak, K. Nationwide study on SARS-CoV-2 transmission within households from lockdown to reopening, Denmark, 27 February 2020 to 1 August 2020. Euro Surveill 2022, 27, 2001800. [Google Scholar] [CrossRef]
- Ryu, S.; Kim, D.; Lim, J.S.; Ali, S.T.; Cowling, B.J. Serial Interval and Transmission Dynamics during SARS-CoV-2 Delta Variant Predominance, South Korea. Emerg. Infect. Dis. 2021, 28, 407–410. [Google Scholar] [CrossRef]
- Wolter, N.; Jassat, W.; Walaza, S.; Welch, R.; Moultrie, H.; Groome, M.; Amoako, D.G.; Everatt, J.; Bhiman, J.N.; Scheepers, C.; et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: A data linkage study. Lancet 2022, 399, 437–446. [Google Scholar] [CrossRef]
- Nishiura, H.; Ito, K.; Anzai, A.; Kobayashi, T.; Piantham, C.; Rodriguez-Morales, A.J. Relative Reproduction Number of SARS-CoV-2 Omicron (B.1.1.529) Compared with Delta Variant in South Africa. J. Clin. Med. 2021, 11, 30. [Google Scholar] [CrossRef]
- Bhattacharyya, R.P.; Hanage, W.P. Challenges in Inferring Intrinsic Severity of the SARS-CoV-2 Omicron Variant. N. Engl. J. Med. 2022, 386, e14. [Google Scholar] [CrossRef]
- Torjesen, I. COVID-19: Omicron may be more transmissible than other variants and partly resistant to existing vaccines, scientists fear. BMJ 2021, 375, n2943. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Overall | Total (%) | Church-Related | Other Settings † |
|---|---|---|---|
| 427 | 76 | 351 | |
| Age group (years) | |||
| 0–9 | 93 (21.8%) | 9 (11.8%) | 84 (23.9%) |
| 10–19 | 12 (2.8%) | 5 (6.6%) | 7 (2.0%) |
| 20–59 | 123 (28.8%) | 43 (56.6%) | 80 (22.8%) |
| Above 60 | 20(4.7%) | 6 (7.9%) | 14 (4.0%) |
| Unknown | 179 (41.9%) | 13 (17.1%) | 166 (47.3%) |
| COVID-19 vaccination | |||
| None | 84 (19.7%) | 38 (50.0%) | 46 (13.1%) |
| One dose | 2 (0.5%) | 2 (2.6%) | 0 |
| Two doses | 70 (16.4%) | 23 (30.3%) | 47 (13.4%) |
| Unknown | 271 (63.5%) | 13 (17.1%) | 258 (73.5%) |
| Type of transmission | |||
| Imported | 5 (1.2%) | 2 (2.6%) | 3 (0.9%) |
| Church | 26 (6.1%) | 26 (34.2%) | 0 |
| Household | 110 (25.8%) | 33 (43.4%) | 77 (21.9%) |
| Social contact | 285 (66.7%) | 15 (19.7%) | 270 (76.9%) |
| Unknown | 1 (0.2%) | 0 | 1 (0.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.; Ali, S.T.; Kim, S.; Jo, J.; Lim, J.-S.; Lee, S.; Ryu, S. Estimation of Serial Interval and Reproduction Number to Quantify the Transmissibility of SARS-CoV-2 Omicron Variant in South Korea. Viruses 2022, 14, 533. https://0-doi-org.brum.beds.ac.uk/10.3390/v14030533
Kim D, Ali ST, Kim S, Jo J, Lim J-S, Lee S, Ryu S. Estimation of Serial Interval and Reproduction Number to Quantify the Transmissibility of SARS-CoV-2 Omicron Variant in South Korea. Viruses. 2022; 14(3):533. https://0-doi-org.brum.beds.ac.uk/10.3390/v14030533
Chicago/Turabian StyleKim, Dasom, Sheikh Taslim Ali, Sungchan Kim, Jisoo Jo, Jun-Sik Lim, Sunmi Lee, and Sukhyun Ryu. 2022. "Estimation of Serial Interval and Reproduction Number to Quantify the Transmissibility of SARS-CoV-2 Omicron Variant in South Korea" Viruses 14, no. 3: 533. https://0-doi-org.brum.beds.ac.uk/10.3390/v14030533