
HBV-RNA, Quantitative HBsAg, Levels of HBV in Peripheral Lymphocytes and HBV Mutation Profiles in Chronic Hepatitis B

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. HBsAg Quantitation and Qualitative Determination of HBeAg, Anti-HBeAg and Anti-HBsAg
2.3. Separation of PBMCs, Extraction and Quantitation of HBV-DNA from Plasma and from PBMCs
2.4. HBV-RNA Quantitation
2.5. Sequence Analysis of the HBV BCP/ PC/Pol Region
2.6. Statistics
3. Results
3.1. Patients Characteristics
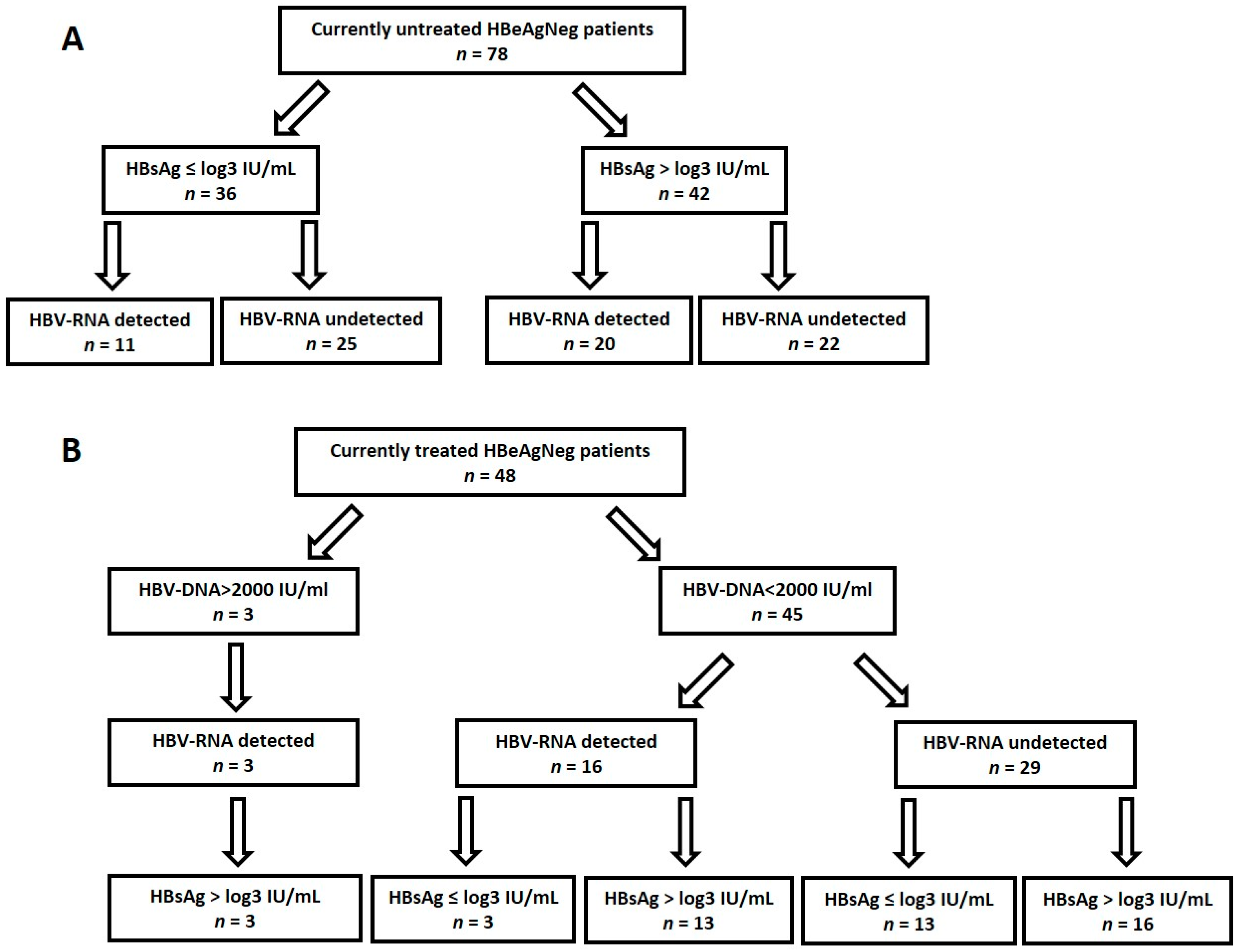
3.2. HBV Biomarkers in HBeAgNeg Patients
3.3. Clinical Impact of Tested Biomarkers in HBeAgNeg Patients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bengsch, B.; Chang, K.M. Evolution in Our Understanding of Hepatitis B Virus Virology and Immunology. Clin. Liver Dis. 2016, 20, 629–644. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.; Koh, S.; Bertoletti, A. Immune Response in Hepatitis B Virus Infection. Cold Spring Harb. Perspect. Med. 2015, 5, a021428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumert, T.F.; Verrier, E.R.; Nassal, M.; Chung, R.T.; Zeisel, M.B. Host-targeting agents for treatment of hepatitis B virus infection. Curr. Opin. Virol. 2015, 14, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Kao, J.H.; Jeng, W.J.; Ning, Q.; Su, T.H.; Tseng, T.C.; Ueno, Y.; Yuen, M.F. APASL guidance on stopping nucleos(t)ide analogues in chronic hepatitis B patients. Hepatol. Int. 2021, 15, 833–851. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Honer Zu Siederdissen, C.; Maasoumy, B.; Cornberg, M. New viral biomarkers for Hepatitis B: Are we able to change practice? J. Viral Hepat. 2018, 25, 1226–1235. [Google Scholar] [CrossRef]
- Brouwer, W.P.; Chan, H.L.; Brunetto, M.R.; Martinot-Peignoux, M.; Arends, P.; Cornberg, M.; Cherubini, B.; Thompson, A.J.; Liaw, Y.F.; Marcellin, P.; et al. Repeated Measurements of Hepatitis B Surface Antigen Identify Carriers of Inactive HBV during Long-term Follow-up. Clin. Gastroenterol. Hepatol. 2016, 14, 1481–1489.e5. [Google Scholar] [CrossRef] [Green Version]
- Su, T.H.; Kao, J.H. Unmet Needs in Clinical and Basic Hepatitis B Virus Research. J. Infect. Dis. 2017, 216 (Suppl. S8), S750–S756. [Google Scholar] [CrossRef]
- Vicenti, I.; Rossetti, B.; Mariano, S.; Saladini, F.; Montagnani, F.; Zazzi, M.; De Luca, A. Distribution of different HBV DNA forms in plasma and peripheral blood mononuclear cells (PBMCs) of chronically infected patients with low or undetectable HBV plasma viremia. New Microbiol. 2018, 41, 302–305. [Google Scholar]
- Ren, X.; Xu, Z.; Liu, Y.; Li, X.; Bai, S.; Ding, N.; Zhong, Y.; Wang, L.; Mao, P.; Zoulim, F.; et al. Hepatitis B virus genotype and basal core promoter/precore mutations are associated with hepatitis B-related acute-on-chronic liver failure without pre-existing liver cirrhosis. J. Viral Hepat. 2010, 17, 887–895. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.L.; Kao, J.H. Natural history of acute and chronic hepatitis B: The role of HBV genotypes and mutants. Best Pract. Res. Clin. Gastroenterol. 2017, 31, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Akrami, H.; Monjezi, M.R.; Ilbeigi, S.; Amiri, F.; Fattahi, M.R. The association between hepatitis B virus mutations and the risk of liver disease and hepatocellular carcinoma. Curr. Mol. Med. 2021. Online Ahead of Print. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Aoyama, K.; Ohno, N.; Iwata, K.; Akahane, Y.; Baba, K.; Yoshizawa, H.; Mishiro, S. The precore/core promoter mutant (T1762A1764) of hepatitis B virus: Clinical significance and an easy method for detection. J. Gen. Virol. 1995, 76 Pt 12, 3159–3164. [Google Scholar] [CrossRef] [PubMed]
- Rajput, M.K. Mutations and methods of analysis of mutations in Hepatitis B virus. AIMS Microbiol. 2020, 6, 401–421. [Google Scholar] [CrossRef] [PubMed]
- Ochwoto, M.; Chauhan, R.; Gopalakrishnan, D.; Chen, C.Y.; Ng’ang’a, Z.; Okoth, F.; Kioko, H.; Kimotho, J.; Kaiguri, P.; Kramvis, A. Genotyping and molecular characterization of hepatitis B virus in liver disease patients in Kenya. Infect. Genet. Evol. 2013, 20, 103–110. [Google Scholar] [CrossRef]
- Tur-Kaspa, R.; Keshet, E.; Eliakim, M.; Shouval, D. Detection and characterization of hepatitis B virus DNA in serum of HBe antigen-negative HBsAg carriers. J. Med. Virol. 1984, 14, 17–26. [Google Scholar] [CrossRef]
- Ben-Ari, Z.; Ashur, Y.; Daudi, N.; Shmilovitz-Wiess, H.; Brown, M.; Sulkes, J.; Klein, A.; Mor, E.; Tur-Kaspa, R.; Shouval, D. Genotype prevalence, viral load and outcome of hepatitis B virus precore mutant infection in stable patients and in patients after liver transplantation. Clin. Transpl. 2004, 18, 415–422. [Google Scholar] [CrossRef]
- Shirazi, R.; Ram, D.; Rakovsky, A.; Bucris, E.; Gozlan, Y.; Lustig, Y.; Shaked-Mishan, P.; Picard, O.; Shemer-Avni, Y.; Ben-Zvi, H.; et al. Characterization of hepatitis B and delta coinfection in Israel. BMC Infect. Dis. 2018, 18, 97. [Google Scholar] [CrossRef]
- Dib, C.; Faure, S.; Fizames, C.; Samson, D.; Drouot, N.; Vignal, A.; Millasseau, P.; Marc, S.; Hazan, J.; Seboun, E.; et al. A comprehensive genetic map of the human genome based on 5264 microsatellites. Nature 1996, 380, 152–154. [Google Scholar] [CrossRef]
- Vachon, A.; Osiowy, C. Novel Biomarkers of Hepatitis B Virus and Their Use in Chronic Hepatitis B Patient Management. Viruses 2021, 13, 951. [Google Scholar] [CrossRef]
- Hadziyannis, S.J. Natural history of chronic hepatitis B in Euro-Mediterranean and African countries. J. Hepatol. 2011, 55, 183–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tur-Kaspa, R.; Klein, A.; Aharonson, S. Hepatitis B virus precore mutants are identical in carriers from various ethnic origins and are associated with a range of liver disease severity. Hepatology 1992, 16, 1338–1342. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Zhu, Z.; Wu, J.; Bi, W.; Xu, W.; Xia, X.; Han, D. Evolutionary Analysis of Pre-S/S Mutations in HBeAg-Negative Chronic Hepatitis B with HBsAg < 100 IU/mL. Front. Public Health 2021, 9, 633792. [Google Scholar] [PubMed]
- Lazarevic, I. Clinical implications of hepatitis B virus mutations: Recent advances. World J. Gastroenterol. 2014, 20, 7653–7664. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Yu, Y.; Li, G.; Shen, C.; Li, J.; Chen, S.; Zhang, X.; Zhu, M.; Zheng, J.; Song, Z.; et al. Natural history of serum HBV-RNA in chronic HBV infection. J. Viral Hepat. 2018, 25, 1038–1047. [Google Scholar] [CrossRef]
- Terrault, N.A.; Wahed, A.S.; Feld, J.J.; Cooper, S.L.; Ghany, M.G.; Lisker-Melman, M.; Perrillo, R.; Sterling, R.K.; Khalili, M.; Chung, R.T.; et al. Incidence and Prediction of HBsAg Seroconversion in a Prospective Multi-ethnic HBeAg-Negative Chronic Hepatitis B Cohort. Hepatology 2021, 75, 709–723. [Google Scholar] [CrossRef]
- Cornberg, M.; Wong, V.W.; Locarnini, S.; Brunetto, M.; Janssen, H.L.A.; Chan, H.L. The role of quantitative hepatitis B surface antigen revisited. J. Hepatol. 2017, 66, 398–411. [Google Scholar] [CrossRef] [Green Version]
- Tang, R.X.; Gao, F.G.; Zeng, L.Y.; Wang, Y.W.; Wang, Y.L. Detection of HBV DNA and its existence status in liver tissues and peripheral blood lymphocytes from chronic hepatitis B patients. World J. Gastroenterol. 1999, 5, 359–361. [Google Scholar] [CrossRef]
- Datta, S.; Panigrahi, R.; Biswas, A.; Chandra, P.K.; Banerjee, A.; Mahapatra, P.K.; Panda, C.K.; Chakrabarti, S.; Bhattacharya, S.K.; Biswas, K.; et al. Genetic characterization of hepatitis B virus in peripheral blood leukocytes: Evidence for selection and compartmentalization of viral variants with the immune escape G145R mutation. J. Virol. 2009, 83, 9983–9992. [Google Scholar] [CrossRef] [Green Version]
- Brunetto, M.R.; Giarin, M.M.; Oliveri, F.; Chiaberge, E.; Baldi, M.; Alfarano, A.; Serra, A.; Saracco, G.; Verme, G.; Will, H.; et al. Wild-type and e antigen-minus hepatitis B viruses and course of chronic hepatitis. Proc. Natl. Acad. Sci. USA 1991, 88, 4186–4190. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, F.; Miyakoshi, H.; Kobayashi, M.; Kumada, H. Correlation between serum hepatitis B virus core-related antigen and intrahepatic covalently closed circular DNA in chronic hepatitis B patients. J. Med. Virol. 2009, 81, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Kusumoto, S.; Iio, E.; Ogawa, S.; Suzuki, T.; Yagi, S.; Kaneko, A.; Matsuura, K.; Aoyagi, K.; Tanaka, Y. Clinical efficacy of a novel, high-sensitivity HBcrAg assay in the management of chronic hepatitis B and HBV reactivation. J. Hepatol. 2021, 75, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Gunning, H.; Adachi, D.; Tang, J.W. Calibration of qualitative HBsAg assay results for quantitative HBsAg monitoring. J. Clin. Virol. 2014, 61, 305–308. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | ||
|---|---|---|
| Males, n (%) | 94.0 (67.6) | |
| Age, Median (IQR) | 48.8 (40.1, 60.1) | |
| Birth country, n (%) | Israel | 52 (37.4) |
| Eastern Europe | 61 (43.9) | |
| Asia | 8 (5.8) | |
| Africa | 13 (9.4) | |
| Unknown | 5 (3.6) | |
| Body mass index, Median (IQR) | 26.6 (23.7, 29.6) | |
| AST, average (range) | 24 (20, 30) | |
| ALT, average (range) | 25 (19, 34) | |
| Fibrosis stage, n (%) | F0–F2 | 109 (78.4) |
| F3–F4 | 17 (12.2) | |
| Unknown | 13 (9.4) | |
| Co-infection *, n (%) | 16 (11.5) | |
| Currently treated, n (%) | 58 (41.7) | |
| HBeAgPos/ HBeAgNeg | 13/126 (9.4/90.6) | |
| HBeAgPos, | HBeAgNeg, | p Value | ||
|---|---|---|---|---|
| n = 13 (9.4%) | n = 126 (90.6%) | |||
| Currently treated, n (%) | 10 (67.9) | 48 (28) | <0.05 | |
| AST, average (range) | 63.2 (25–250) | 25.4 (9–64) | <0.05 | |
| ALT, average (range) | 74.8 (24–423) | 28.4 (5–115) | <0.05 | |
| Fibrosis stage, N (%) | F0–F2 | 9 (69.2) | 100 (79.4) | 0.6 |
| F3–F4 | 2 (15.4) | 15 (11.9) | ||
| Unknown | 2 (15.4) | 11 (8.7) | NA | |
| Plasma HBV-DNA | Undetectable, n (%) | 3 (23.0) | 38 (30.2) | 0.6 |
| Detectable (n = 96) | 4 (2.0–6.7) | 3.3 (2.6, 3.8) | <0.05 | |
| log IU/mL, Median (IQR) | ||||
| Plasma HBV-RNA | Undetectable, n (%) | 2 (15.4) | 75 (59.5) | <0.05 |
| Detectable (n = 63) | 4.4 (4.1–6.6) | 3.0 (2.1, 3.4) | <0.05 | |
| log copies/mL, Median (IQR) | ||||
| PBMCs HBV-DNA | Undetectable, n/N (%) | 5/6 (83.3) | 48/74 (64.5) | 0.4 |
| Detectable (n = 27) | NA | 1.4 (1.2, 3.4) | NA | |
| log copies/106 cells, Median (IQR) | ||||
| HBsAg | Log IU/mL, Median (IQR) | 3.7 (3.4–4.2) | 3.2 (2.3, 3.8) | <0.05 |
| Anti-HBe Antibodies | Yes/No, n (%) | 2/11 (15.4) | 120/6 (95.2) | <0.05 |
| Genotype (N = 68) | A, n/N (%) | 1/5 (20.0) | 5/63 (7.9) | 0.4 |
| C, n/N (%) | 0/5 | 1/63 (1.6) | NA | |
| D, n/N (%) | 4/5 (80.0) | 57/63 (90.4) | 0.5 | |
| Mutations | BCP and PC (n/N, %) | 2/4 (50.0) | 57/58 (98.2) | <0.05 |
| Escape (n/N, %) | 2/5 (40.0) | 11/58 (19.0) | 0.3 | |
| Resistance (n/N, %) | 1/5 (20.0) | 1/58 (1.7) | <0.05 | |
| HBsAg ≤ 3 log (n = 52) | HBsAg > 3 log (n = 74) | p Value | ||
|---|---|---|---|---|
| Age, average (IQR) | 53.9 (41.8,61.8) | 45.8 (39.0,57.5) | <0.05 | |
| ALT, average (range) | 25.3 (9–116) | 30.4 (5–83) | 0.11 | |
| AST, average (range) | 23.8 (12–48) | 26.4 (9–64) | 0.15 | |
| Undetectable plasma HBV-DNA, n (%) | 33 (63.5) | 20 (27.0) | <0.05 | |
| Detectable plasma HBV-DNA log, Median (IQR) | 3.2 (2.6,3.8) | 3.4 (2.8,3.8) | 0.61 | |
| Undetectable HBV-RNA, n (%) | 38 (73.0) | 38 (51.4) | <0.05 | |
| Detectable HBV-RNA log, Median (IQR) | 2.6 (1.8,3.2) | 3.0 (2.3,3.4) | 0.36 | |
| Undetectable PBMC HBV-DNA, n (%) | 22/31 (70.9) | 27/43 (62.8) | 0.46 | |
| Detectable PBMC HBV-DNA log, Median (IQR) * | 1.2 (0.9,3.5) | 1.5(1.2,3.7) | 0.81 | |
| Anti Hbe Antibodies | 50 (96.1) | 70 (94.6) | 0.69 | |
| Genotype | A, n (%) | 1/22 (4.6) | 4/41 (9.8) | 0.47 |
| C, n (%) | 0 | 1/41 (2.4) | NA | |
| D, n (%) | 21/22 (95.5) | 36/41 (87.8) | 0.32 | |
| Mutations | BCP/ PC N = 58 (n/N, %) | 21/21 (100) | 36/37 (98.2) | NA |
| Escape, N = 58 (n/N, %) | 3/20 (15) | 8/38 (21.6) | 0.55 | |
| Resistance, N = 58 (n/N, %) | 0/20 | 1/38 (2.7) | NA | |
| Currently treated, n (%) | 16 (30.8) | 32 (43.2) | 0.16 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gozlan, Y.; Aaron, D.; Davidov, Y.; Likhter, M.; Ben Yakov, G.; Cohen-Ezra, O.; Picard, O.; Erster, O.; Mendelson, E.; Ben-Ari, Z.; et al. HBV-RNA, Quantitative HBsAg, Levels of HBV in Peripheral Lymphocytes and HBV Mutation Profiles in Chronic Hepatitis B. Viruses 2022, 14, 584. https://0-doi-org.brum.beds.ac.uk/10.3390/v14030584
Gozlan Y, Aaron D, Davidov Y, Likhter M, Ben Yakov G, Cohen-Ezra O, Picard O, Erster O, Mendelson E, Ben-Ari Z, et al. HBV-RNA, Quantitative HBsAg, Levels of HBV in Peripheral Lymphocytes and HBV Mutation Profiles in Chronic Hepatitis B. Viruses. 2022; 14(3):584. https://0-doi-org.brum.beds.ac.uk/10.3390/v14030584
Chicago/Turabian StyleGozlan, Yael, Daniella Aaron, Yana Davidov, Maria Likhter, Gil Ben Yakov, Oranit Cohen-Ezra, Orit Picard, Oran Erster, Ella Mendelson, Ziv Ben-Ari, and et al. 2022. "HBV-RNA, Quantitative HBsAg, Levels of HBV in Peripheral Lymphocytes and HBV Mutation Profiles in Chronic Hepatitis B" Viruses 14, no. 3: 584. https://0-doi-org.brum.beds.ac.uk/10.3390/v14030584