
Detection of SARS-CoV-2 Nucleocapsid, Spike, and Neutralizing Antibodies in Vaccinated Japanese

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Sera
2.2. SARS-CoV-2 Ab Analyses
2.3. Statistical Analysis
3. Results
3.1. SARS-CoV-2 Abs in the Sera
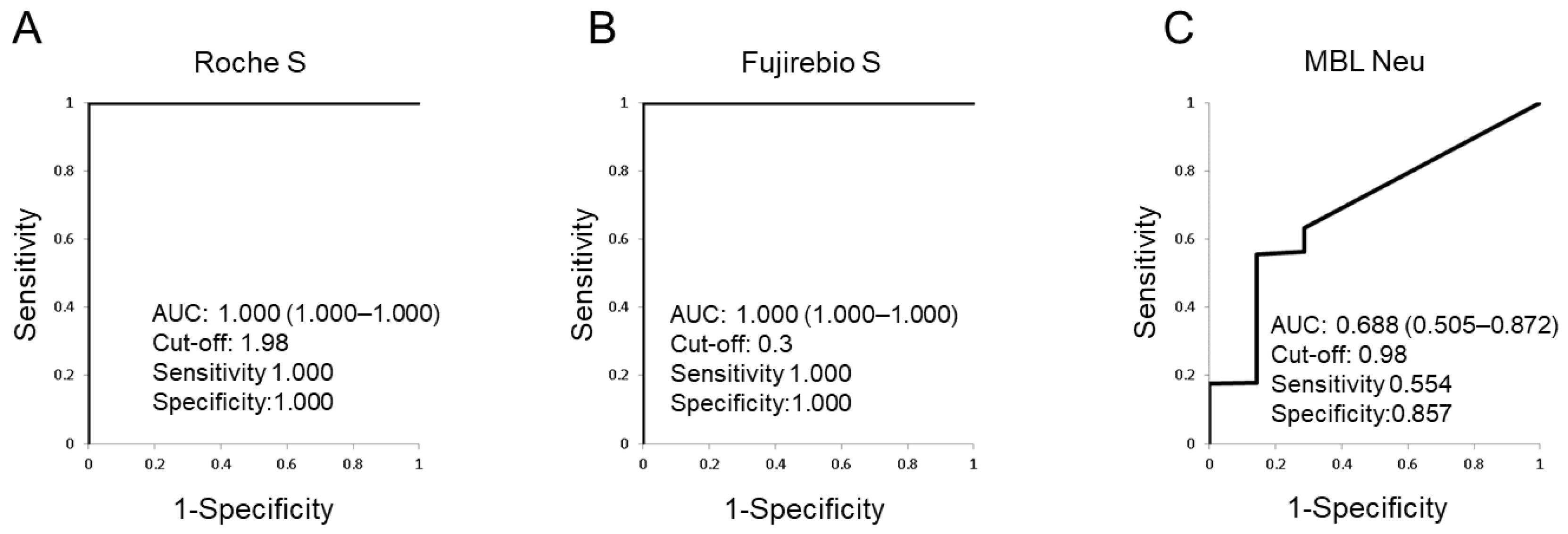
3.2. ROC Analyses
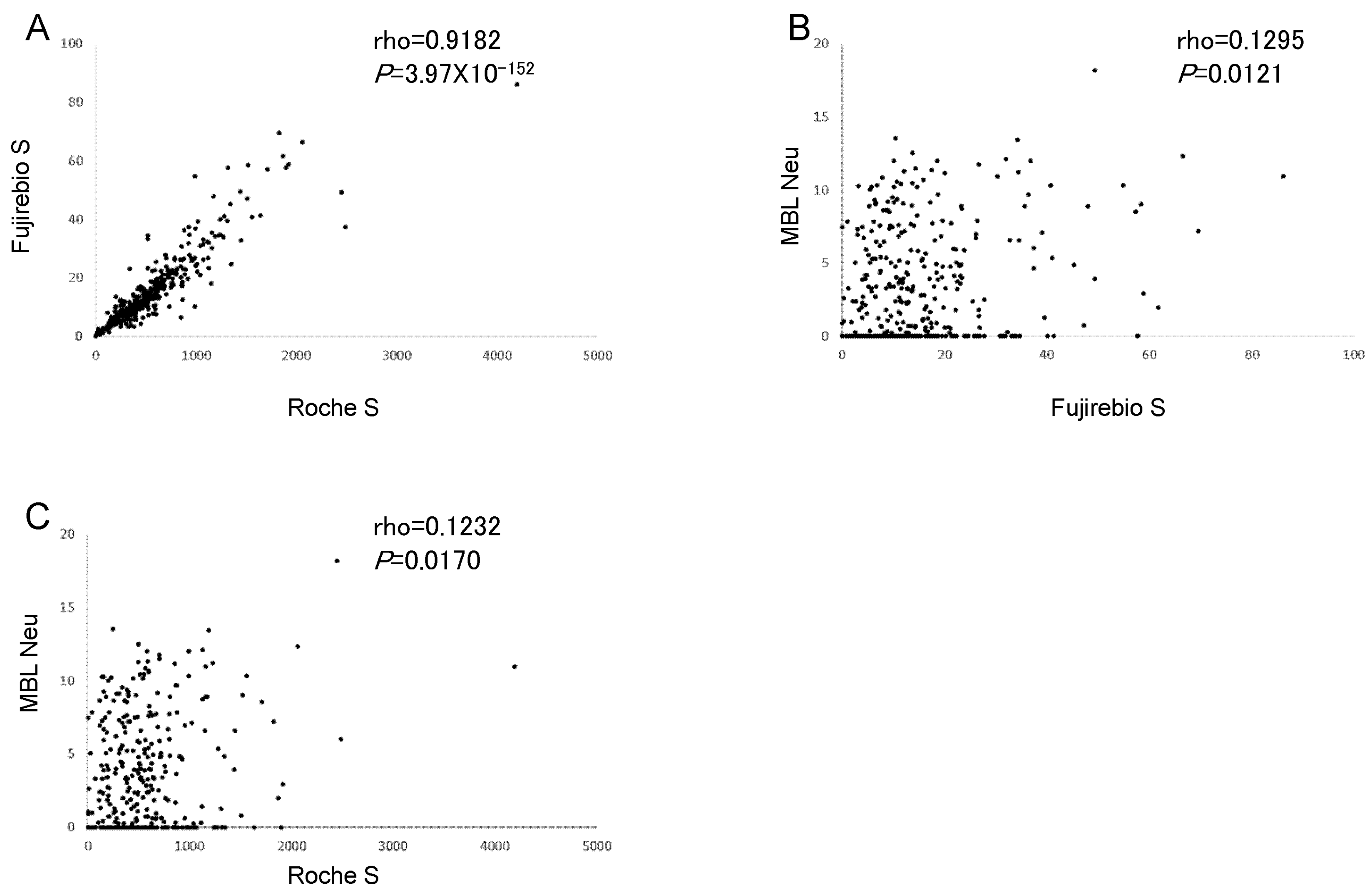
3.3. Correlations between SARS-CoV-2 Ab Assays
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 diagnosis and management: A comprehensive review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef] [PubMed]
- Che, X.Y.; Qiu, L.W.; Pan, Y.X.; Wen, K.; Hao, W.; Zhang, L.Y.; Wang, Y.D.; Liao, Z.Y.; Hua, X.; Cheng, V.C.; et al. Sensitive and specific monoclonal antibody-based capture enzyme immunoassay for detection of nucleocapsid antigen in sera from patients with severe acute respiratory syndrome. J. Clin. Microbiol. 2004, 42, 2629–2635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woo, P.C.; Lau, S.K.; Wong, B.H.; Tsoi, H.W.; Fung, A.M.; Kao, R.Y.; Chan, K.H.; Peiris, J.S.; Yuen, K.Y. Differential sensitivities of severe acute respiratory syndrome (SARS) coronavirus spike polypeptide enzyme-linked immunosorbent assay (ELISA) and SARS coronavirus nucleocapsid protein ELISA for serodiagnosis of SARS coronavirus pneumonia. J. Clin. Microbiol. 2005, 43, 3054–3058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, B.; Drosten, C.; Müller, M.A. Serological assays for emerging coronaviruses: Challenges and pitfalls. Virus Res. 2014, 194, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Rikhtegaran Tehrani, Z.; Saadat, S.; Saleh, E.; Ouyang, X.; Constantine, N.; DeVico, A.L.; Harris, A.D.; Lewis, G.K.; Kottilil, S.; Sajadi, M.M. Performance of nucleocapsid and spike-based SARS-CoV-2 serologic assays. PLoS ONE 2020, 15, e0237828. [Google Scholar] [CrossRef] [PubMed]
- Noda, K.; Matsuda, K.; Yagishita, S.; Maeda, K.; Akiyama, Y.; Terada-Hirashima, J.; Matsushita, H.; Iwata, S.; Yamashita, K.; Atarashi, Y.; et al. A novel highly quantitative and reproducible assay for the detection of anti-SARS-CoV-2 IgG and IgM antibodies. Sci. Rep. 2021, 11, 5198. [Google Scholar] [CrossRef] [PubMed]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Meyer, B.; Reimerink, J.; Torriani, G.; Brouwer, F.; Godeke, G.J.; Yerly, S.; Hoogerwerf, M.; Vuilleumier, N.; Kaiser, L.; Eckerle, I.; et al. Validation and clinical evaluation of a SARS-CoV-2 surrogate virus neutralisation test (sVNT). Emerg. Microbes Infect. 2020, 9, 2394–2403. [Google Scholar] [CrossRef]
- Murray, M.J.; McIntosh, M.; Atkinson, C.; Mahungu, T.; Wright, E.; Chatterton, W.; Gandy, M.; Reeves, M.B. Validation of a commercially available indirect assay for SARS-CoV-2 neutralising antibodies using a pseudotyped virus assay. J. Infect. 2021, 82, 170–177. [Google Scholar] [CrossRef]
- Papenburg, J.; Cheng, M.P.; Corsini, R.; Caya, C.; Mendoza, E.; Manguiat, K.; Lindsay, L.R.; Wood, H.; Drebot, M.A.; Dibernardo, A.; et al. Evaluation of a Commercial Culture-Free Neutralization Antibody Detection Kit for Severe Acute Respiratory Syndrome-Related Coronavirus-2 and Comparison With an Antireceptor-Binding Domain Enzyme-Linked Immunosorbent Assay. Open Forum Infect. Dis. 2021, 8, ofab220. [Google Scholar] [CrossRef]
- Jung, K.; Shin, S.; Nam, M.; Hong, Y.J.; Roh, E.Y.; Park, K.U.; Song, E.Y. Performance evaluation of three automated quantitative immunoassays and their correlation with a surrogate virus neutralization test in coronavirus disease 19 patients and pre-pandemic controls. J. Clin. Lab. Anal. 2021, 35, e23921. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, H.; Oka, S.; Higuchi, T.; Yamaguchi, M.; Uchiyama, S.; Koiwa, T.; Nakama, M.; Minegishi, M.; Nagai, H.; Tohma, S. Detection of anti-SARS-CoV-2 nucleocapsid and spike antibodies in patients with Coronavirus Disease 2019 in Japan. Clin. Med. Insights Circ. Respir. Pulm. Med. 2022, 16, 11795484221075492. [Google Scholar] [CrossRef] [PubMed]
- SARS-CoV-2 Neutralization Antibody Detection Kit. Available online: https://ruo.mbl.co.jp/bio/product/sars-cov-2/pickup/SARS-CoV-2-neutralizing-antibody.html (accessed on 9 March 2022).
- Favresse, J.; Gillot, C.; Di Chiaro, L.; Eucher, C.; Elsen, M.; Van Eeckhoudt, S.; David, C.; Morimont, L.; Dogné, J.M.; Douxfils, J. Neutralizing Antibodies in COVID-19 Patients and Vaccine Recipients after Two Doses of BNT162b2. Viruses 2021, 13, 1364. [Google Scholar] [CrossRef] [PubMed]
- Hartley, G.E.; Edwards, E.S.J.; Aui, P.M.; Varese, N.; Stojanovic, S.; McMahon, J.; Peleg, A.Y.; Boo, I.; Drummer, H.E.; Hogarth, P.M.; et al. Rapid generation of durable B cell memory to SARS-CoV-2 spike and nucleocapsid proteins in COVID-19 and convalescence. Sci. Immunol. 2020, 5, eabf8891. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Karalis, V.; Ntanasis-Stathopoulos, I.; Apostolakou, F.; Gumeni, S.; Gavriatopoulou, M.; Papadopoulos, D.; Malandrakis, P.; Papanagnou, E.D.; Korompoki, E.; et al. Sustained but Declining Humoral Immunity Against SARS-CoV-2 at 9 Months Postvaccination With BNT162b2: A Prospective Evaluation in 309 Healthy Individuals. Hemasphere 2021, 6, e677. [Google Scholar] [CrossRef] [PubMed]
- Willyard, C. What the Omicron wave is revealing about human immunity. Nature 2022, 602, 22–25. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Vaccinated Subjects | Non-Vaccinated Subjects | p | |
|---|---|---|---|
| Number | 368 | 7 | |
| Roche S, U/mL (SD) | 561.4 (431.5) | 0.4 (0.0) | 5.80 × 10−6 |
| Fujirebio N, AU/mL (SD) | 0.0 (0.0) | 0.0 (0.0) | 0.9748 |
| Fujirebio S, AU/mL (SD) | 15.6 (12.5) | 0.1 (0.0) | 5.80 × 10−6 |
| MBL Neu, inhibition rate (%) (SD) | 3.3 (3.8) | 1.2 (2.8) | 0.0792 |
| Vaccinated Subjects | Non-Vaccinated Subjects | Sensitivity (95%CI) | Specificity (95%CI) | ||
|---|---|---|---|---|---|
| Roche S | positive | 368 | 0 | 100.0 (99.0–100.0) | 100.0 (59.0–100.0) |
| negative | 0 | 7 | |||
| Fujirebio S | positive | 364 | 0 | 98.9 (97.2–99.7) | 100.0 (59.0–100.0) |
| negative | 4 | 7 | |||
| MBL Neu | positive | 10 | 0 | 2.7 (1.3–4.9) | 100.0 (59.0–100.0) |
| negative | 358 | 7 |
| Fujirebio S Compared with Roche S | MBL Neu Compared with Fujirebio S | MBL Neu Compared with Roche S | ||||
| OPA, n, %, (95%CI) | 371/375 | 98.9 (97.3–99.7) | 21/375 | 5.6 (3.5–8.4) | 17/375 | 4.5 (2.7–7.2) |
| PPA, n, %, (95%CI) | 364/368 | 98.9 (97.2–99.7) | 10/364 | 2.7 (1.3–5.0) | 10/368 | 2.7 (1.3–4.9) |
| NPA, n, %, (95%CI) | 7/7 | 100.0 (59.0–100.0) | 11/11 | 100.0 (71.5–100.0) | 7/7 | 100.0 (59.0–100.0) |
| Cohen’s kappa, (95%CI) | 0.773 (0.557–0.988) | 0.002 (0.000–0.003) | 0.001 (0.000–0.002) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Midorikawa, R.; Nakama, M.; Furukawa, H.; Oka, S.; Higuchi, T.; Nagai, H.; Nagai, N.; Tohma, S. Detection of SARS-CoV-2 Nucleocapsid, Spike, and Neutralizing Antibodies in Vaccinated Japanese. Viruses 2022, 14, 965. https://0-doi-org.brum.beds.ac.uk/10.3390/v14050965
Midorikawa R, Nakama M, Furukawa H, Oka S, Higuchi T, Nagai H, Nagai N, Tohma S. Detection of SARS-CoV-2 Nucleocapsid, Spike, and Neutralizing Antibodies in Vaccinated Japanese. Viruses. 2022; 14(5):965. https://0-doi-org.brum.beds.ac.uk/10.3390/v14050965
Chicago/Turabian StyleMidorikawa, Rie, Moriyuki Nakama, Hiroshi Furukawa, Shomi Oka, Takashi Higuchi, Hideaki Nagai, Nobuhiro Nagai, and Shigeto Tohma. 2022. "Detection of SARS-CoV-2 Nucleocapsid, Spike, and Neutralizing Antibodies in Vaccinated Japanese" Viruses 14, no. 5: 965. https://0-doi-org.brum.beds.ac.uk/10.3390/v14050965