
Long-COVID Clinical Features and Risk Factors: A Retrospective Analysis of Patients from the STOP-COVID Registry of the PoLoCOV Study

 ,
,  , ,
, ,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Methodology
- (a)
- diagnosis of COVID-19 (initially by reverse transcription polymerase chain reaction test only, then also by antigen tests—according to the changes to the rules for COVID-19 diagnosis in Poland);
- (b)
- age ≥ 18 years;
- (c)
- written informed consent to participate in the study.
- (a)
- age < 18 years
- (b)
- No consent to participate in the study.
- 0 points (asymptomatic/mild course)
- ○
- asymptomatic course
- ○
- paroxysmal symptoms lasting no more than 3 days
- 1 point (mild course)
- ○
- home isolation
- ○
- subjective assessment by the patient of a score of ‘1’ on a scale of 0–3
- ○
- duration of symptoms less than 7 days
- 2 points (moderate)
- ○
- subjective assessment by the patient of a score of ‘2’ or ‘3’ on a scale of 03
- ○
- duration of symptoms lasting between 7 and 14 days
- ○
- the presence of dyspnea and fever ≥ 38 °C
- 3 points (severe course)
2.2. Statistical Analysis
3. Results
3.1. Characteristics of the Study Group
3.2. Long-COVID Disease Picture and Its Risk Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- COVID Live—Coronavirus Statistics—Worldometer. Available online: https://www.worldometers.info/coronavirus/ (accessed on 11 June 2022).
- SeyedAlinaghi, S.; Mirzapour, P.; Dadras, O.; Pashaei, Z.; Karimi, A.; MohsseniPour, M.; Soleymanzadeh, M.; Barzegary, A.; Afsahi, A.M.; Vahedi, F.; et al. Characterization of SARS-CoV-2 Different Variants and Related Morbidity and Mortality: A Systematic Review. Eur. J. Med. Res. 2021, 26, 51. [Google Scholar] [CrossRef] [PubMed]
- Flisiak, R.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Mastalerz-Migas, A.; Owczuk, R.; Parczewski, M.; Pawłowska, M.; Piekarska, A.; Simon, K.; et al. Management of SARS-CoV-2 Infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists as of February 23, 2022. Pol. Arch. Intern. Med. 2022, 132, 16230. [Google Scholar] [CrossRef] [PubMed]
- Kuter, B.J.; Offit, P.A.; Poland, G.A. The Development of COVID-19 Vaccines in the United States: Why and How so Fast? Vaccine 2021, 39, 2491–2495. [Google Scholar] [CrossRef]
- Hammond, J.; Leister-Tebbe, H.; Gardner, A.; Abreu, P.; Bao, W.; Wisemandle, W.; Baniecki, M.; Hendrick, V.M.; Damle, B.; Simón-Campos, A.; et al. Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with COVID-19. N. Engl. J. Med. 2022, 386, 1397–1408. [Google Scholar] [CrossRef]
- Jayk Bernal, A.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Delos Reyes, V.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of COVID-19 in Nonhospitalized Patients. N. Engl. J. Med. 2022, 386, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Sigal, A.; Milo, R.; Jassat, W. Estimating Disease Severity of Omicron and Delta SARS-CoV-2 Infections. Nat. Rev. Immunol. 2022, 22, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Taquet, M.; Dercon, Q.; Luciano, S.; Geddes, J.R.; Husain, M.; Harrison, P.J. Incidence, Co-Occurrence, and Evolution of Long-COVID Features: A 6-Month Retrospective Cohort Study of 273,618 Survivors of COVID-19. PLoS Med. 2021, 18, e1003773. [Google Scholar] [CrossRef]
- Antonelli, M.; Penfold, R.S.; Merino, J.; Sudre, C.H.; Molteni, E.; Berry, S.; Canas, L.S.; Graham, M.S.; Klaser, K.; Modat, M.; et al. Risk Factors and Disease Profile of Post-Vaccination SARS-CoV-2 Infection in UK Users of the COVID Symptom Study App: A Prospective, Community-Based, Nested, Case-Control Study. Lancet Infect. Dis. 2022, 22, 43–55. [Google Scholar] [CrossRef]
- CDC Long COVID or Post-COVID Conditions. Available online: https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html (accessed on 11 June 2022).
- Yong, S.J. Long COVID or Post-COVID-19 Syndrome: Putative Pathophysiology, Risk Factors, and Treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef] [PubMed]
- Cirulli, E.T.; Schiabor Barrett, K.M.; Riffle, S.; Bolze, A.; Neveux, I.; Dabe, S.; Grzymski, J.J.; Lu, J.T.; Washington, N.L. Long-Term COVID-19 Symptoms in a Large Unselected Population. bioRxiv 2020. [Google Scholar]
- Lu, Y.; Li, X.; Geng, D.; Mei, N.; Wu, P.-Y.; Huang, C.-C.; Jia, T.; Zhao, Y.; Wang, D.; Xiao, A.; et al. Cerebral Micro-Structural Changes in COVID-19 Patients—An MRI-Based 3-Month Follow-up Study. EClinicalMedicine 2020, 25, 100484. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. WHO Clinical Case Definition Working Group on Post-COVID-19 Condition A Clinical Case Definition of Post-COVID-19 Condition by a Delphi Consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef]
- Overview—COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19—Guidance—NICE. Available online: https://www.nice.org.uk/guidance/ng188 (accessed on 5 July 2022).
- Mehandru, S.; Merad, M. Pathological Sequelae of Long-Haul COVID. Nat. Immunol. 2022, 23, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Castanares-Zapatero, D.; Chalon, P.; Kohn, L.; Dauvrin, M.; Detollenaere, J.; Maertens de Noordhout, C.; Primus-de Jong, C.; Cleemput, I.; van den Heede, K. Pathophysiology and Mechanism of Long COVID: A Comprehensive Review. Ann. Med. 2022, 54, 1473–1487. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and Predictors of Long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef]
- Thompson, E.J.; Williams, D.M.; Walker, A.J.; Mitchell, R.E.; Niedzwiedz, C.L.; Yang, T.C.; Huggins, C.F.; Kwong, A.S.F.; Silverwood, R.J.; Gessa, G.D.; et al. Risk Factors for Long COVID: Analyses of 10 Longitudinal Studies and Electronic Health Records in the UK. bioRxiv 2021. [Google Scholar]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-Month Consequences of COVID-19 in Patients Discharged from Hospital: A Cohort Study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Wong, A.W.; Shah, A.S.; Johnston, J.C.; Carlsten, C.; Ryerson, C.J. Patient-Reported Outcome Measures after COVID-19: A Prospective Cohort Study. Eur. Respir. J. 2020, 56, 2003276. [Google Scholar] [CrossRef]
- Truffaut, L.; Demey, L.; Bruyneel, A.V.; Roman, A.; Alard, S.; de Vos, N.; Bruyneel, M. Post-Discharge Critical COVID-19 Lung Function Related to Severity of Radiologic Lung Involvement at Admission. Respir. Res. 2021, 22, 29. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Martín-Guerrero, J.D.; Pellicer-Valero, Ó.J.; Navarro-Pardo, E.; Gómez-Mayordomo, V.; Cuadrado, M.L.; Arias-Navalón, J.A.; Cigarán-Méndez, M.; Hernández-Barrera, V.; Arendt-Nielsen, L. Female Sex Is a Risk Factor Associated with Long-Term Post-COVID Related-Symptoms but Not with COVID-19 Symptoms: The LONG-COVID-EXP-CM Multicenter Study. J. Clin. Med. 2022, 11, 413. [Google Scholar] [CrossRef]
- Jacobson, K.B.; Rao, M.; Bonilla, H.; Subramanian, A.; Hack, I.; Madrigal, M.; Singh, U.; Jagannathan, P.; Grant, P. Patients with Uncomplicated Coronavirus Disease 2019 (COVID-19) Have Long-Term Persistent Symptoms and Functional Impairment Similar to Patients with Severe COVID-19: A Cautionary Tale during a Global Pandemic. Clin. Infect. Dis. 2021, 73, e826–e829. [Google Scholar] [CrossRef] [PubMed]
- Wood, E.; Hall, K.H.; Tate, W. Role of Mitochondria, Oxidative Stress and the Response to Antioxidants in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Possible Approach to SARS-CoV-2 “long-Haulers? Chronic Dis. Transl. Med. 2021, 7, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Tancheva, L.; Petralia, M.C.; Miteva, S.; Dragomanova, S.; Solak, A.; Kalfin, R.; Lazarova, M.; Yarkov, D.; Ciurleo, R.; Cavalli, E.; et al. Emerging Neurological and Psychobiological Aspects of COVID-19 Infection. Brain Sci. 2020, 10, 852. [Google Scholar] [CrossRef] [PubMed]
- Ayoubkhani, D.; Bermingham, C.; Pouwels, K.B.; Glickman, M.; Nafilyan, V.; Zaccardi, F.; Khunti, K.; Alwan, N.A.; Walker, A.S. Trajectory of Long COVID Symptoms after COVID-19 Vaccination: Community Based Cohort Study. BMJ 2022, 377, e069676. [Google Scholar] [CrossRef] [PubMed]
- Al-Aly, Z.; Bowe, B.; Xie, Y. Long COVID after Breakthrough SARS-CoV-2 Infection. Nat. Med. 2022, 28, 1461–1467. [Google Scholar] [CrossRef]
- Siripanthong, B.; Nazarian, S.; Muser, D.; Deo, R.; Santangeli, P.; Khanji, M.Y.; Cooper, L.T., Jr.; Chahal, C.A.A. Recognizing COVID-19-Related Myocarditis: The Possible Pathophysiology and Proposed Guideline for Diagnosis and Management. Heart Rhythm 2020, 17, 1463–1471. [Google Scholar] [CrossRef]
- Asadi-Pooya, A.A.; Akbari, A.; Emami, A.; Lotfi, M.; Rostamihosseinkhani, M.; Nemati, H.; Barzegar, Z.; Kabiri, M.; Zeraatpisheh, Z.; Farjoud-Kouhanjani, M.; et al. Long COVID Syndrome-Associated Brain Fog. J. Med. Virol. 2022, 94, 979–984. [Google Scholar] [CrossRef]
- Gennaro, D.; Belati, F.; Tulone, A.; Diella, O.; Bavaro, L.; Bonica, D.F.; Genna, R.; Smith, V.; Trott, L.; Bruyere, M. Long COVID: A Systematic Review and Meta-Analysis of 120,970 Patients. SSRN Electron. J. 2022. [Google Scholar] [CrossRef]
- Batabyal, R.; Freishtat, N.; Hill, E.; Rehman, M.; Freishtat, R.; Koutroulis, I. Metabolic Dysfunction and Immunometabolism in COVID-19 Pathophysiology and Therapeutics. Int. J. Obes. 2021, 45, 1163–1169. [Google Scholar] [CrossRef]
- Stefano, G.B.; Ptacek, R.; Ptackova, H.; Martin, A.; Kream, R.M. Selective Neuronal Mitochondrial Targeting in SARS-CoV-2 Infection Affects Cognitive Processes to Induce “Brain Fog” and Results in Behavioral Changes That Favor Viral Survival. Med. Sci. Monit. 2021, 27, e930886-1–e930886-4. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | The Whole Group N = 2218 (%) | Female | Male | p | |
|---|---|---|---|---|---|
| Sex | Female | 1410 (63.5) | --- | --- | --- |
| Male | 808 (36.5) | --- | --- | --- | |
| Age (M ± SD) | 53.8 ± 13.5 | 53.84 ± 13.3 | 53.72 ± 13.7 | 0.923 | |
| Weight [kg] (M ± SD) | 79.6 ± 17.2 | 73.3 ± 15.1 | 90.69 ± 14.9 | <0.001 | |
| Height [cm] (M ± SD) | 169.1 ± 9.1 | 164.5 ± 6.2 | 177.1 ± 7.8 | <0.001 | |
| BMI (M ± SD) | 21.3 ± 9.1 | 20.4 ± 9.1 | 22.7 ± 8.9 | <0.001 | |
| Chronic diseases | 1569 (70.7) | 981 (69.6) | 588 (72.7) | 0.123 | |
| Chronic diseases | Hypertension | 826 (37.2) | 476 (33.8) | 350 (43.3) | <0.001 |
| BMI > 30 | 692 (31.2) | 388 (28.0) | 304 (38.3) | <0.001 | |
| Diabetes | 230 (10.4) | 125 (8.9) | 105 (13.0) | 0.002 | |
| Coronary artery disease | 134 (6.0) | 66 (4.7) | 68 (8.4) | 0.005 | |
| DCM | 17 (0.8) | 5 (0.4) | 12 (1.5) | 0.007 | |
| Heart failure | 26 (1.2) | 12 (0.9) | 14 (1.7) | 0.100 | |
| Venous thromboembolism | 24 (1.1) | 16 (1.1) | 8 (1.0) | 0.917 | |
| Hyperlipidemia | 440 (19.8) | 269 (19.1) | 171 (21.2) | 0.258 | |
| Asthma | 217 (9.8) | 155 (10.9) | 62 (7.7) | 0.014 | |
| COPD | 51 (2.3) | 30 (2.1) | 21 (2.6) | 0.571 | |
| Thyroid disease | 374 (18.9) | 328 (23.3) | 46 (5.7) | <0.001 | |
| Place of Isolation | Home | 1887 (85.0) | 1229 (86.9) | 658 (79.5) | |
| Hospital—without pneumonia | 33 (1.5) | 17 (1.2) | 16 (1.9) | 0.204 | |
| Hospital—with pneumonia | 279 (12.6) | 140 (9.9) | 139 (17.2) | <0.001 | |
| Hospital—ICU | 19 (0.9) | 11 (0.8) | 8 (1.0) | 0.781 | |
| Flu vaccinations in the previous season | 166 (7.5) | 110 (7.8) | 56 (6.9) | 0.505 | |
| Vaccination against COVID-19 (n = 697) | 494 (70.9) | 341 (72.9) | 153 (66.81) | 0.118 | |
| Symptom | N (%) |
|---|---|
| Long-COVID | 1444 (65.1) |
| Chronic fatigue | 789 (35.6) |
| Headache | 661 (29.8) |
| Cought | 510 (23.0) |
| Brain fog | 268 (12.1) |
| Dyspnoea | 137 (6.2) |
| Hair loss | 104 (4.7) |
| Olfactory dysfunction | 98 (4.4) |
| Osteoarticular pain | 91 (4.1) |
| Variable | Long-COVID | Brain Fog | Chronic Fatigue | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Percentage (%) | OR (95%Cl) | p | Percentage (%) | OR (95%Cl) | p | Percentage (%) | OR (95%Cl) | p | ||
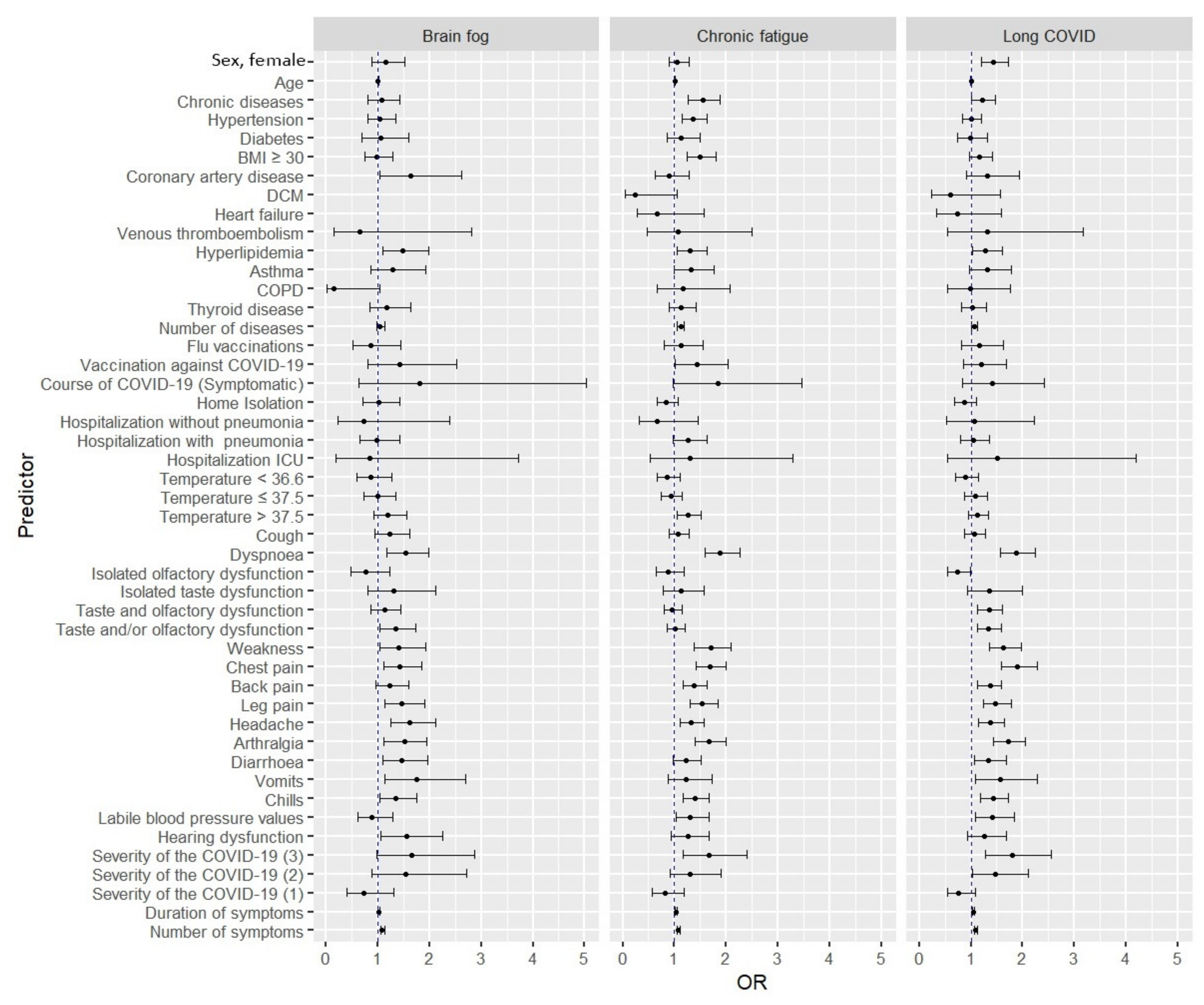
| Sex | Female | 961 (66.6) | 1.44 (1.20–1.72) | <0.001 | 178 (12.6) | 1.15 (0.88–1.51) | 0.301 | 509 (36.1) | 1.06 (0.89–1.28) | 0.493 |
| Male | 483 (59.8) | Ref. | Ref. | 90 (11.1) | Ref. | Ref. | 280 (34.7) | Ref. | Ref. | |
| Age | ----- | 1.00 (0.99–1.01) | 0.261 | ---- | 1.00 (0.99–1.01) | 0.582 | ---- | 1.02 (1.00–1.02) | <0.001 | |
| Chronic diseases | Yes | 1043 (66.5) | 1.23 (1.01–1.48) | 0.035 | 193 (12.3) | 1.07 (0.81–1.43) | 0.624 | 603 (38.4) | 1.55 (1.27–1.89) | <0.001 |
| No | 401 (61.8) | Ref. | Ref. | 75 (11.6) | Ref. | Ref. | 186 (28.7) | Ref. | Ref. | |
| Hypertension | Yes | 538 (61.8) | 1.00 (0.84–1.21) | 0.982 | 102 (12.4) | 1.04 (0.80–1.35) | 0.767 | 331 (40.1) | 1.36 (1.14–1.63) | <0.001 |
| No | 906 (65.1) | Ref. | Ref. | 166 (11.9) | Ref. | Ref. | 458 (32.9) | Ref. | Ref. | |
| Diabetes | Yes | 149 (64.8) | 0.98 (0.74–1.31) | 0.914 | 29 (12.6) | 1.05 (0.69–1.59) | 0.796 | 88 (38.3) | 1.13 (0.86–1.50) | 0.368 |
| No | 1295 (65.1) | Ref. | Ref. | 239 (12.0) | Ref. | Ref. | 701 (35.3) | Ref. | Ref. | |
| Obesity (BMI ≥ 30) | Yes | 468 (67.6) | 1.16 (0.96–1.41) | 0.122 | 82 (11.9) | 0.97 (0.74–1.28) | 0.856 | 291 (42.1) | 1.49 (1.24–1.80) | <0.001 |
| No | 954 (64.2) | Ref. | Ref. | 180 (12.1) | Ref. | Ref. | 486 (32.7) | Ref. | Ref. | |
| Coronary artery disease | Yes | 95 (70.9) | 1.32 (0.91–1.94) | 0.148 | 24 (17.9) | 1.64 (1.03–2.61) | 0.034 | 51 (38.1) | 0.89 (0.62–1.28) | 0.535 |
| No | 1349 (64.7) | Ref. | Ref. | 244 (11.7) | Ref. | Ref. | 738 (35.4) | Ref. | Ref. | |
| DCM | Yes | 9 (52.9) | 0.61 (0.23–1.57) | 0.296 | 0 (0.0) | ---- | --- | 2 (11.8) | 0.24 (0.05–1.05) | 0.058 |
| No | 1435 (65.2) | Ref. | Ref. | 268 (12.2) | Ref. | Ref. | 787 (35.8) | Ref. | Ref. | |
| Heart failure | Yes | 15 (57.7) | 0.73 (0.33–1.59) | 0 (0.0) | ---- | --- | 7 (26.9) | 0.66 (0.27–1.58) | 0.357 | |
| No | 1429 (65.2) | Ref. | Ref. | 268 (12.2) | Ref. | Ref. | 782 (35.7) | Ref. | Ref. | |
| Venous thromboembolism | Yes | 17 (70.8) | 1.31 (0.54–3.17) | 0.555 | 2 (8.3) | 0.66 (0.15–2.81) | 0.574 | 9 (37.5) | 1.08 (0.48–2.50) | 0.842 |
| No | 1427 (65.0) | Ref. | Ref. | 266 (12.1) | Ref. | Ref. | 780 (35.6) | Ref. | Ref. | |
| Hyperlipidemia | Yes | 306 (69.6) | 1.28 (1.03–1.61) | 0.029 | 69 (15.7) | 1.48 (1.10–1.98) | 0.010 | 179 (40.7) | 1.31 (1.06–1.63) | 0.012 |
| No | 1138 (64.0) | Ref. | Ref. | 199 (11.2) | Ref. | Ref. | 610 (34.3) | Ref. | Ref. | |
| Asthma | Yes | 154 (70.5) | 1.31 (0.97–1.79) | 0.079 | 32 (14.8) | 1.29 (0.87–1.93) | 0.206 | 90 (41.5) | 1.32 (0.99–1.76) | 0.056 |
| No | 1291 (64.5) | Ref. | Ref. | 236 (11.8) | Ref. | Ref. | 699 (34.9) | Ref. | Ref. | |
| COPD | Yes | 33 (64.7) | 0.98 (0.55–1.76) | 0.951 | 1 (2.0) | 0.14 (0.01–1.03) | 0.054 | 20 (39.2) | 1.17 (0.66–2.07) | 0.582 |
| No | 1411 (65.1) | Ref. | Ref. | 267 (12.3) | Ref. | Ref. | 769 (35.5) | Ref. | Ref. | |
| Thyroid disease | Yes | 245 (65.5) | 1.02 (0.81–1.29) | 0.857 | 51 (13.6) | 1.18 (0.85–1.64) | 0.312 | 141 (37.7) | 1.12 (0.89–1.41) | 0.346 |
| No | 1199 (65.0) | Ref. | Ref. | 217 (11.8) | Ref. | Ref. | 648 (35.1) | Ref. | Ref. | |
| Number of diseases | --- | 1.06 (1.00–1.12) | 0.049 | ---- | 1.04 (0.97–1.13 | 0.246 | ---- | 1.12 (1.06–1.18) | <0.001 | |
| Flu vaccinations | Yes | 113 (68.1) | 1.16 (0.82–1.62) | 0.404 | 18 (10.8) | 0.87 (0.52–1.45) | 0.610 | 63 (37.9) | 1.12 (0.81–1.55) | 0.505 |
| No | 1331 (64.9) | Ref. | Ref. | 250 (12.2) | Ref. | Ref. | 726 (35.4) | Ref. | Ref. | |
| Vaccination against COVID-19 | Yes | 326 (66.0) | 1.21 (0.86–1.69) | 0.268 | 57 (11.5) | 1.42 (0.81–2.52) | 0.219 | 197 (39.9) | 1.44 (1.02–2.04) | 0.038 |
| No | 125 (61.6) | Ref. | Ref. | 17 (8.4) | Ref. | Ref. | 64 (31.5) | Ref. | Ref. | |
| Course of COVID-19 | Symptomatic | 1412 (65.1) | 1.41 (0.83–2.42) | 0.207 | 264 (12.2) | 1.81 (0.64–5.04) | 0.257 | 776 (35.9) | 1.85 (0.98–3.46) | 0.054 |
| Asymptomatic | 32 (57.1) | Ref. | Ref. | 4 (7.1) | Ref. | Ref. | 13 (23.2) | Ref. | Ref. | |
| Home Isolation | Yes | 1202 (64.6) | 0.87 (0.68–1.11) | 0.280 | 225 (12.1) | 1.01 (0.71–1.43) | 0.963 | 650 (35.0) | 0.84 (0.67–1.07) | 0.160 |
| No | 242 (67.6) | Ref. | Ref. | 43 (12.0) | Ref. | Ref. | 139 (38.8) | Ref. | Ref. | |
| Hospitalization without pneumonia | Yes | 22 (66.7) | 1.07 (0.52–2.22) | 0.849 | 3 (9.1) | 0.72 (0.22–2.39) | 0.596 | 9 (27.3) | 0.67 (0.31–1.46) | 0.319 |
| No | 1422 (65.1) | Ref. | Ref. | 265 (12.1) | Ref. | Ref. | 780 (35.7) | Ref. | Ref. | |
| Hospitalization with pneumonia | Yes | 184 (66.0) | 1.04 (0.80–1.36) | 0.751 | 33 (11.8) | 0.97 (0.66–1.43) | 0.889 | 113 (40.5) | 1.27 (0.98–1.64) | 0.066 |
| No | 1260 (65.0) | Ref. | Ref. | 235 (12.1) | Ref. | Ref. | 676 (34.9) | Ref. | Ref. | |
| Hospitalization ICU | Yes | 14 (73.7) | 1.51 (0.54–4.2) | 0.434 | 2 (10.5) | 0.85 (0.19–3.72) | 0.834 | 8 (42.12) | 1.31 (0.53–3.30) | 0.552 |
| No | 1430 (65.0) | Ref. | Ref. | 266 (12.1) | Ref. | Ref. | 781 (35.5) | Ref. | Ref. | |
| Temperature< 36.6 | Yes | 198 (63.1) | 0.90 (0.70–1.15) | 0.418 | 34 (10.8) | 0.87 (0.59–1.27) | 0.461 | 102 (32.5) | 0.85 (0.66–1.10) | 0.217 |
| No | 1246 (65.4) | Ref. | Ref. | 234 (12.4) | Ref. | Ref. | 687 (36.1) | Ref. | Ref. | |
| Temperature≤ 37.5 | Yes | 332 (66.4) | 1.08 (0.87–1.32) | 0.486 | 60 (12.0) | 0.99 (0.73–1.34) | 0.948 | 171 (34.2) | 0.93(0.75–1.14) | 0.466 |
| No | 1112 (64.7) | Ref. | Ref. | 208 (12.1) | Ref. | Ref. | 618 (35.9) | Ref. | Ref. | |
| Temperature> 37.5 | Yes | 782 (66.4) | 1.13 (0.95–1.34) | 0.178 | 153 (13.0) | 1.20 (0.93–1.55) | 0.164 | 449 (38.1) | 1.27 (1.06–1.51) | 0.007 |
| No | 662 (63.7) | Ref. | Ref. | 115 (11.1) | Ref. | Ref. | 340 (32.7) | Ref. | Ref. | |
| Cough | Yes | 927 (65.6) | 1.06 (0.88–1.27) | 0.551 | 182 (12.9) | 1.23 (0.94–1.62) | 0.131 | 512 (36.2) | 1.08 (0.90–1.29) | 0.407 |
| No | 517 (64.3) | Ref. | Ref. | 86 (110.7) | Ref. | Ref. | 277 (34.5) | Ref. | Ref. | |
| Dyspnoea | Yes | 767 (74.4) | 1.87 (1.56–2.24) | <0.001 | 153 (14.5) | 1.53 (1.18–1.98) | 0.001 | 457 (43.2) | 1.89 (1.59–2.26) | <0.001 |
| No | 677 (58.4) | Ref. | Ref. | 115 (9.9) | Ref. | Ref. | 332 (28.7) | Ref. | Ref. | |
| Isolated olfactory dysfunction | Yes | 126 (58.6) | 0.74 (0.55–0.98) | 0.035 | 21 (9.8) | 0.77 (0.48–1.23) | 0.274 | 71 (33.0) | 0.88 (0.65–1.19) | 0.411 |
| No | 1318 (65.8) | Ref. | Ref. | 247 (12.3) | Ref. | Ref. | 718 (35.9) | Ref. | Ref. | |
| Isolated taste dysfunction | Yes | 100 (71.4) | 1.36 (0.94–1.99) | 0.105 | 21 (15.0) | 1.31 (0.81–2.12) | 0.275 | 53 (37.9) | 1.12 (0.78–1.58) | 0.559 |
| No | 1344 (64.7) | Ref. | Ref. | 247 (11.9) | Ref. | Ref. | 736 (35.4) | Ref. | Ref. | |
| Taste and olfactory dysfunction | Yes | 684 (68.8) | 1.35 (1.13–1.61) | <0.001 | 127 (12.8) | 1.13 (0.87–1.45) | 0.366 | 349 (35.1) | 0.96 (0.81–1.15) | 0.682 |
| No | 760 (62.1) | Ref. | Ref. | 141 (11.5) | Ref. | Ref. | 440 (36.0) | Ref. | Ref. | |
| Taste and/or olfactory dysfunction | Yes | 717 (68.6) | 1.34 (1.12–1.59) | 0.001 | 144 (13.8) | 1.35 (1.04–1.74) | 0.022 | 374 (35.8) | 1.02 (0.86–1.20) | 0.865 |
| No | 727 (62.0) | Ref. | Ref. | 124 (10.6) | Ref. | Ref. | 415 (35.4) | Ref. | Ref. | |
| Weakness | Yes | 1107 (68.2) | 1.63 (1.35–1.98) | <0.001 | 211 (13.0) | 1.41 (1.03–1.92) | 0.030 | 628 (38.7) | 1.70 (1.38–2.09) | <0.001 |
| No | 337 (56.7) | Ref. | Ref. | 57 (9.6) | Ref. | Ref. | 161 (27.1) | Ref. | Ref. | |
| Chest pain | Yes | 708 (73.1) | 1.90 (1.59–2.28) | <0.001 | 138 (14.3) | 1.43 (1.11–1.85) | 0.005 | 409 (42.3) | 1.68 (1.41–2.00) | <0.001 |
| No | 736 (58.9) | Ref. | Ref. | 130 (10.4) | Ref. | Ref. | 380 (30.4) | Ref. | Ref. | |
| Back pain | Yes | 795 (68.2) | 1.38 (1.13–1.59) | 0.001 | 153 (13.1) | 1.23 (0.95–1.60) | 0.111 | 455 (39.1) | 1.38 (1.16–1.64) | <0.001 |
| No | 649 (61.6) | Ref. | Ref. | 115 (10.9) | Ref. | Ref. | 334 (31.7) | Ref. | Ref. | |
| Leg pain | Yes | 670 (70.2) | 1.48 (1.24–1.78) | <0.001 | 139 (14.5) | 1.47 (1.14–1.90) | 0.003 | 394 (41.3) | 1.54 (1.30–1.84) | <0.001 |
| No | 774 (61.3) | Ref. | Ref. | 130 (10.3) | Ref. | Ref. | 395 (31.3) | Ref. | Ref. | |
| Headache | Yes | 837 (68.3) | 1.37 (1.15–1.64) | <0.001 | 175 (14.3) | 1.61 (1.24–2.11) | <0.001 | 471 (38.5) | 1.33 (1.11–1.58) | 0.002 |
| No | 607 (61.1) | Ref. | Ref. | 93 (9.4) | Ref. | Ref. | 318 (32.0) | Ref. | Ref. | |
| Arthralgia | Yes | 651 (72.3) | 1.72 (1.43–2.06) | <0.001 | 133 (14.8) | 1.52 (1.12–1.95) | 0.001 | 384 (42.6) | 1.67 (1.40–2.00) | <0.001 |
| No | 793 (60.2) | Ref. | Ref. | 135 (10.3) | Ref. | Ref. | 405 (30.8) | Ref. | Ref. | |
| Diarrhoea | Yes | 302 (70.2) | 1.33 (1.06–1.68) | 0.013 | 67 (15.6) | 1.46 (1.09–1.96) | 0.014 | 169 (39.3) | 1.22 (0.98–1.51) | 0.072 |
| No | 1142 (63.9) | Ref. | Ref. | 201 (11.2) | Ref. | Ref. | 620 (34.7) | Ref. | Ref. | |
| Vomits | Yes | 111 (74.0) | 1.57 (108–2.29) | 0.015 | 28 (18.7) | 1.75 (1.13–2.69) | 0.011 | 60 (40.0) | 1.22 (0.87–1.72) | 0.241 |
| No | 1333 (64.5) | Ref. | Ref. | 240 (11.6) | Ref. | Ref. | 729 (35.3) | Ref. | Ref. | |
| Chills | Yes | 559 (70.1) | 1.43 (1.18–1.72) | <0.001 | 113 (14.2) | 1.35 (1.04–1.75) | 0.024 | 323 (40.5) | 1.40 (1.17–1.67) | <0.001 |
| No | 885 (62.3) | Ref. | Ref. | 155 (10.9) | Ref. | Ref. | 466 (32.8) | Ref. | Ref. | |
| Labile blood pressure values | Yes | 234 (71.6) | 1.41 (1.09–1.83) | 0.008 | 36 (11.0) | 0.89 (0.61–1.28) | 0.519 | 134 (41.0) | 1.31 (1.03–1.67) | 0.027 |
| No | 1210 (64.0) | Ref. | Ref. | 232 (12.3) | Ref. | Ref. | 655 (34.6) | Ref. | Ref. | |
| Hearing dysfunction | Yes | 153 (69.6) | 1.25 (0.93–1.69) | 0.146 | 37 (16.8) | 1.55 (1.06–2.26) | 0.024 | 89 (40.5) | 1.26 (0.94–1.67) | 0.111 |
| No | 1291 (64.6) | Ref. | Ref. | 231 (11.6) | Ref. | Ref. | 700 (35.0) | Ref. | Ref. | |
| Severity of the COVID-19 | 3 | 567 (72.9) | 1.80 (1.27–2.55) | <0.001 | 117 (15.1) | 1.65 (0.97–2.87) | 0.075 | 333 (42.9) | 1.67 (1.17–2.40) | 0.004 |
| 2 | 416 (68.8) | 1.47 (1.03–2.10) | 0.011 | 86 (14.2) | 1.54 (0.88–2.71) | 0.131 | 224 (37.0) | 1.31 (0.91–1.90) | 0.146 | |
| 1 | 348 (53.5) | 0.76 (0.54–1.08) | <0.001 | 47 (7.2) | 0.72 (0.39–1.31) | 0.288 | 174 (26.7) | 0.82 (0.56–1.18) | 0.284 | |
| 0 | 99 (60.0) | Ref. | Ref. | 16 (9.7) | Ref. | Ref. | 51 (30.9) | Ref. | Ref. | |
| Duration of symptoms | ---- | 1.05(1.03–1.07) | <0.001 | ---- | 1.02 (1.00-1.04) | 0.037 | ---- | 1.03 (1.01–1.05) | <0.001 | |
| Number of symptoms | ---- | 1.09 (10.7–1.12) | <0.001 | ---- | 1.08 (1.05–1.13) | <0.001 | ---- | 1.08 (1.06–1.11) | <0.001 | |
| Variable | Long-COVID | Brain Fog | Chronic Fatigue | ||||
|---|---|---|---|---|---|---|---|
| OR (95%Cl) | p | OR (95%Cl) | p | OR (95%Cl) | p | ||
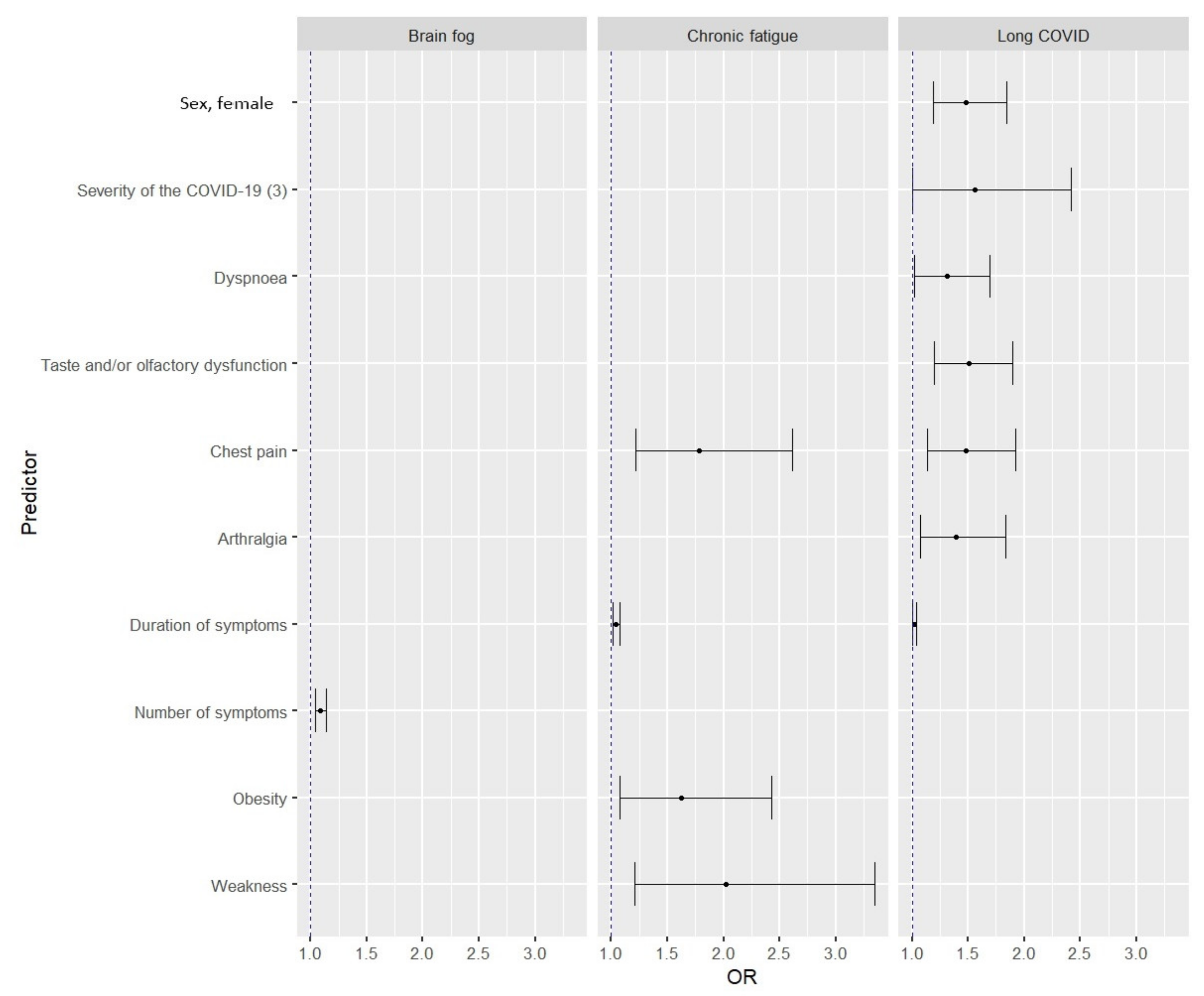
| Sex, Female | 1.48 (1.19–1.84) | <0.001 | --- | --- | --- | --- | |
| Severity of the COVID-19 | 3 | 1.56 (1.00–2.42) | 0.045 | --- | --- | --- | --- |
| Dyspnoea | 1.31 (1.02–1.69) | 0.035 | --- | --- | --- | --- | |
| Taste and/or olfactory dysfunction | 1.51 (1.20–1.90) | <0.001 | --- | --- | --- | --- | |
| Chest pain | 1.48 (1.14–1.92) | 0.003 | --- | --- | 1.78 (1.22–2.61) | 0.002 | |
| Arthralgia | 1.39 (1.07–1.83) | 0.015 | --- | --- | --- | --- | |
| Duration of symptoms | 1.02 (1.00–1.04) | 0.049 | --- | --- | 1.04 (1.01–1.08) | 0.015 | |
| Number of symptoms | --- | --- | 1.09 (1.04–1.14) | <0.001 | --- | --- | |
| Obesity | --- | --- | --- | --- | 1.62 (1.08–2.43) | 0.019 | |
| Weakness | --- | --- | --- | --- | 2.02 (1.21–3.35) | 0.007 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chudzik, M.; Babicki, M.; Kapusta, J.; Kałuzińska-Kołat, Ż.; Kołat, D.; Jankowski, P.; Mastalerz-Migas, A. Long-COVID Clinical Features and Risk Factors: A Retrospective Analysis of Patients from the STOP-COVID Registry of the PoLoCOV Study. Viruses 2022, 14, 1755. https://0-doi-org.brum.beds.ac.uk/10.3390/v14081755
Chudzik M, Babicki M, Kapusta J, Kałuzińska-Kołat Ż, Kołat D, Jankowski P, Mastalerz-Migas A. Long-COVID Clinical Features and Risk Factors: A Retrospective Analysis of Patients from the STOP-COVID Registry of the PoLoCOV Study. Viruses. 2022; 14(8):1755. https://0-doi-org.brum.beds.ac.uk/10.3390/v14081755
Chicago/Turabian StyleChudzik, Michał, Mateusz Babicki, Joanna Kapusta, Żaneta Kałuzińska-Kołat, Damian Kołat, Piotr Jankowski, and Agnieszka Mastalerz-Migas. 2022. "Long-COVID Clinical Features and Risk Factors: A Retrospective Analysis of Patients from the STOP-COVID Registry of the PoLoCOV Study" Viruses 14, no. 8: 1755. https://0-doi-org.brum.beds.ac.uk/10.3390/v14081755