
Risk of Pulmonary Fibrosis and Persistent Symptoms Post-COVID-19 in a Cohort of Outpatient Health Workers

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
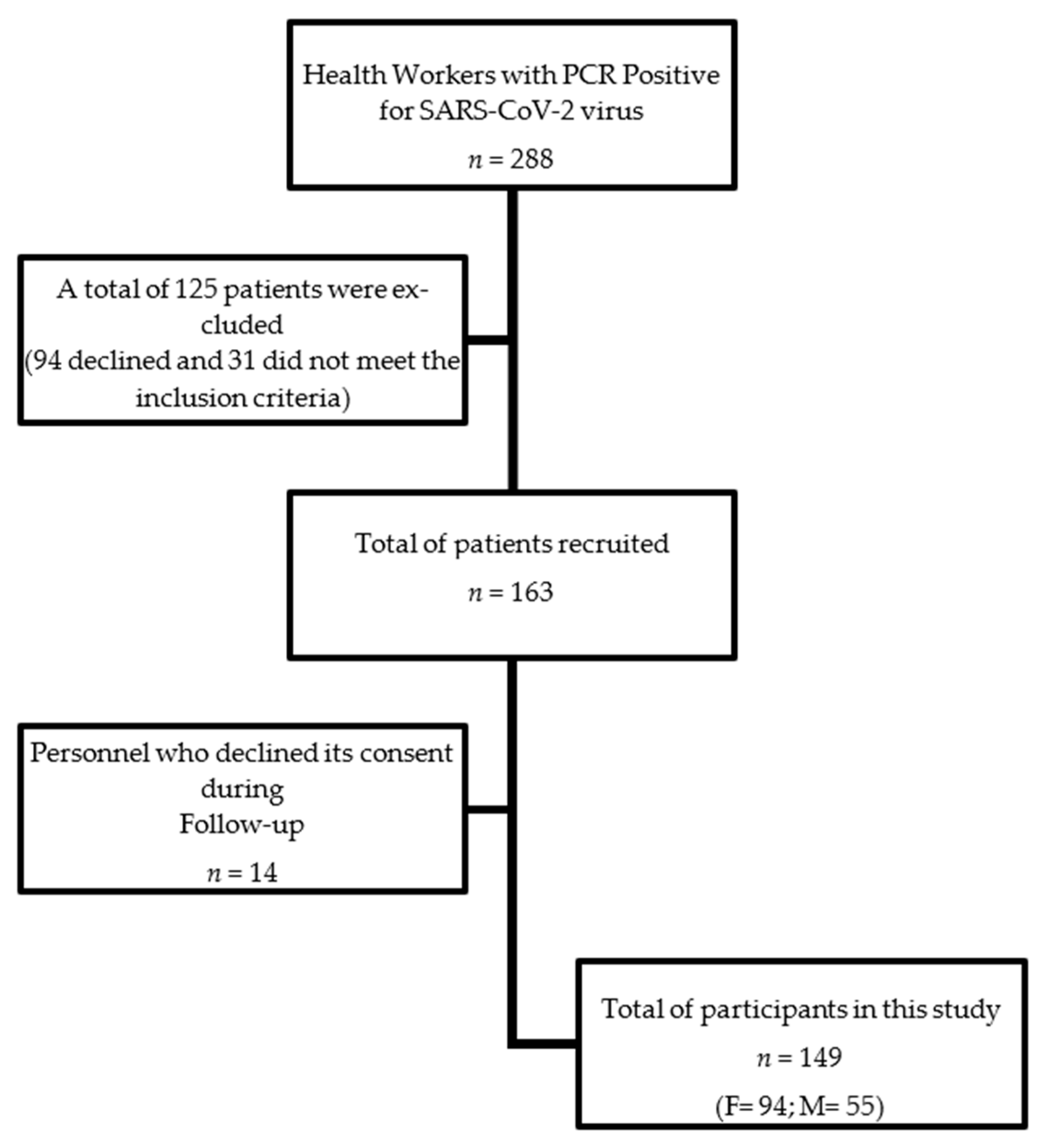
2.1. Design and Study Population
- At baseline, when workers attend to be tested for the first time.
- Three or five days after a positive RT-PCR test (active infection).
- Minimally, six months after a negative RT-PCR test (post-infection period).
2.2. Procedures
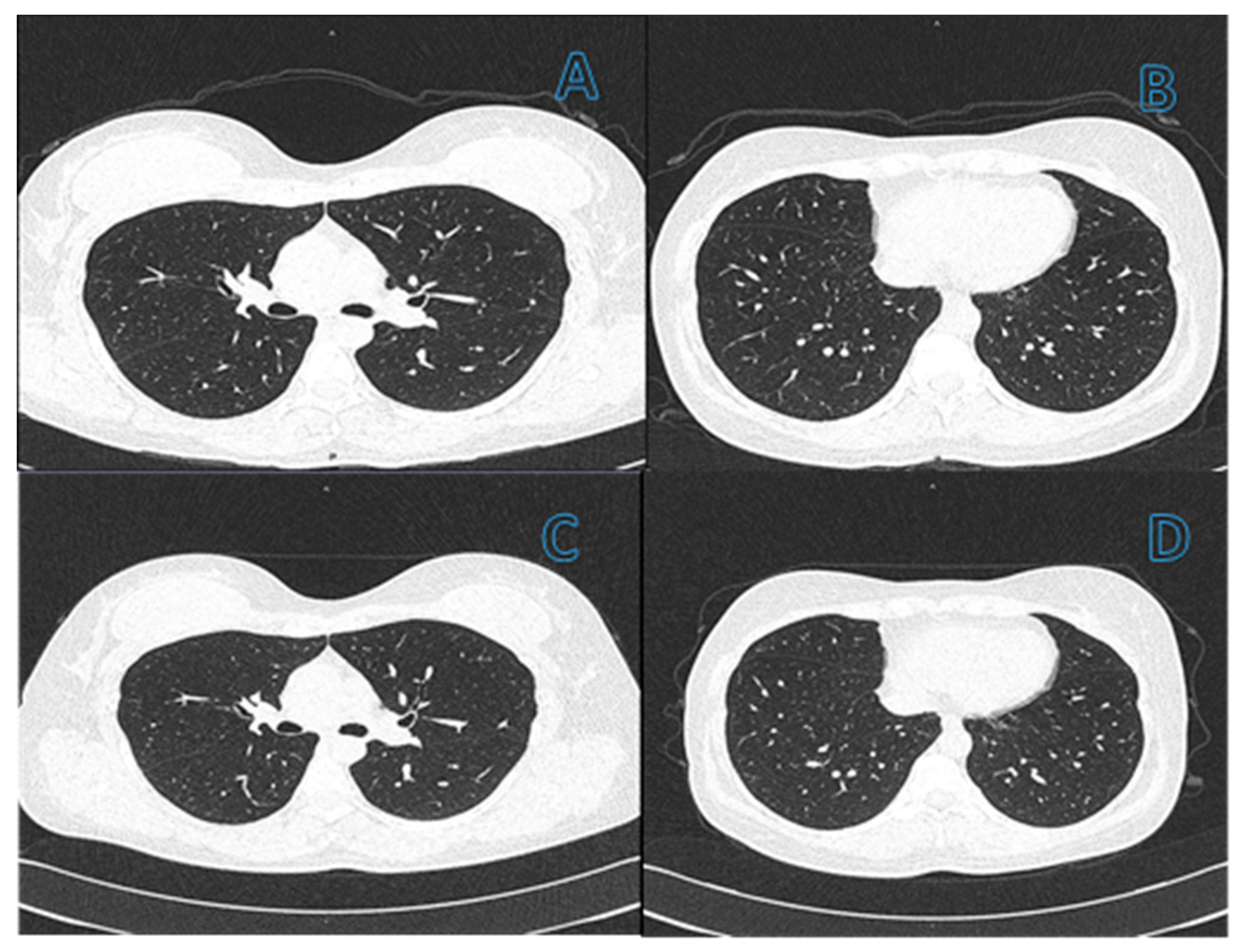
2.3. Post-COVID Assessment of Pulmonary Fibrosis
2.4. Statistical Analysis
3. Results
3.1. Group of Study
3.2. Clinical Characteristics
3.3. Signs and Symptoms Prevalence
- (1)
- Neurological: fatigue or weakness, difficulty concentrating, blurred vision, hair loss, cramps, ear disorders, sleeping problems, and anxiety;
- (2)
- Gastric: bite alteration and weight changes;
- (3)
- Inflammatory and cardiorespiratory: dermatitis, dyspnea, and tachycardia.
3.4. Diagnosis of Pulmonary Fibrosis and Risk Factors for the Development of Post-COVID-19 Pulmonary Fibrosis
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease 2019 (COVID-19): Situation Report, 114. World Health Organization. 2020. Available online: https://apps.who.int/iris/handle/10665/332089 (accessed on 2 May 2021).
- Kim, G.-U.; Kim, M.-J.; Ra, S.; Lee, J.; Bae, S.; Jung, J.; Kim, S.-H. Clinical characteristics of asymptomatic and symptomatic patients with mild COVID-19. Clin. Microbiol. Infect. 2020, 26, 948.e1–948.e3. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, S.; Schell, A.; Berkemann, M.; Jungbauer, F.; Zaubitzer, L.; Huber, L.; Warken, C.; Held, V.; Kusnik, A.; Teufel, A.; et al. post-COVID-19 Impairment of the Senses of Smell, Taste, Hearing, and Balance. Viruses 2022, 14, 849. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Rai, D.K.; Sharma, P.; Kumar, R. Post covid 19 pulmonary fibrosis. Is it real threat? Indian J. Tuberc. 2021, 68, 330–333. [Google Scholar] [CrossRef]
- Zhou, Y.; Yang, Q.; Chi, J.; Dong, B.; Lv, W.; Shen, L.; Wang, Y. Comorbidities and the risk of severe or fatal outcomes associated with coronavirus disease 2019: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 99, 47–56. [Google Scholar] [CrossRef]
- Hall, J.; Myall, K.; Lam, J.L.; Mason, T.; Mukherjee, B.; West, A.; Dewar, A. Identifying patients at risk of post-discharge complications related to COVID-19 infection. Thorax 2021, 76, 408–411. [Google Scholar] [CrossRef]
- Garibaldi, B.T.; Wang, K.; Robinson, M.L.; Zeger, S.L.; Bandeen-Roche, K.; Wang, M.-C.; Alexander, G.C.; Gupta, A.; Bollinger, R.; Xu, Y. Comparison of Time to Clinical Improvement With vs Without Remdesivir Treatment in Hospitalized Patients With COVID-19. JAMA Netw. Open 2021, 4, e213071. [Google Scholar] [CrossRef]
- Ranjbar, K.; Moghadami, M.; Mirahmadizadeh, A.; Fallahi, M.J.; Khaloo, V.; Shahriarirad, R.; Erfani, A.; Khodamoradi, Z.; Gholampoor Saadi, M.H. Methylprednisolone or dexamethasone, which one is superior corticosteroid in the treatment of hospitalized COVID-19 patients: A triple-blinded randomized controlled trial. BMC Infect. Dis. 2021, 21, 337. [Google Scholar] [CrossRef]
- Baricich, A.; Borg, M.B.; Cuneo, D.; Cadario, E.; Azzolina, D.; Balbo, P.E.; Bellan, M.; Zeppegno, P.; Pirisi, M.; Cisari, C.; et al. Midterm functional sequelae and implications in rehabilitation after COVID-19: A cross-sectional study. Eur. J. Phys. Rehabil. Med. 2021, 57, 199–207. [Google Scholar] [CrossRef]
- Riker, R.R.; Shehabi, Y.; Bokesch, P.M.; Ceraso, D.; Wisemandle, W.; Koura, F.; Whitten, P.; Margolis, B.D.; Byrne, D.W.; Ely, E.W.; et al. Dexmedetomidine vs. midazolam for sedation of critically ill patients: A randomized trial. JAMA 2009, 301, 489–499. [Google Scholar] [CrossRef] [Green Version]
- Van den Borst, B.; Peters, J.B.; Brink, M.; Schoon, Y.; Bleeker-Rovers, C.P.; Schers, H.; van Hees, H.W.; van Helvoort, H.; van den Boogaard, M.; van der Hoeven, H.; et al. Comprehensive Health Assessment 3 Months After Recovery from Acute Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2021, 73, e1089–e1098. [Google Scholar] [CrossRef] [PubMed]
- Petersen, M.S.; Kristiansen, M.F.; Hanusson, K.D.; Danielsen, M.E.; Steig, B.Á.; Gaini, S.; Strøm, M.; Weihe, P. Long COVID in the Faroe Islands: A Longitudinal Study Among Non-Hospitalized Patients. Clin. Infect. Dis. 2021, 73, e4058–e4063. [Google Scholar] [CrossRef] [PubMed]
- Hellmuth, J.; Barnett, T.A.; Asken, B.M.; Kelly, J.D.; Torres, L.; Stephens, M.L.; Greenhouse, B.; Martin, J.N.; Chow, F.C.; Deeks, S.G.; et al. Persistent COVID-19-associated neurocognitive symptoms in non-hospitalized patients. J. Neurovirol. 2021, 27, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Romieu, A.C.; Leung, S.; Mbanya, A.; Jackson, B.R.; Cope, J.R.; Bushman, D.; Dixon, M.; Brown, J.; McLeod, T.; Saydah, S.; et al. Health Care Utilization and Clinical Characteristics of Non-hospitalized Adults in an Integrated Health Care System 28-180 Days After COVID-19 Diagnosis—Georgia, May 2020–March 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 644–650. [Google Scholar] [CrossRef]
- Luyt, C.-E.; Combes, A.; Becquemin, M.-H.; Beigelman-Aubry, C.; Hatem, S.; Brun, A.-L.; Zraik, N.; Carrat, F.; Grenier, P.A.; Richard, J.-C.M.; et al. Long-term Outcomes of Pandemic 2009 Influenza A(H1N1)-Associated Severe ARDS. Chest 2012, 142, 583–592. [Google Scholar] [CrossRef]
- Sharifian-Dorche, M.; Huot, P.; Osherov, M.; Wen, D.; Saveriano, A.; Giacomini, P.S.; Antel, J.P.; Mowla, A. Neurological complications of coronavirus infection; a comparative review and lessons learned during the COVID-19 pandemic. J. Neurol. Sci. 2020, 417, 117085. [Google Scholar] [CrossRef]
- Shehata, G.; Lord, K.; Grudzinski, M.; Elsayed, M.; Abdelnaby, R.; Elshabrawy, H. Neurological Complications of COVID-19: Underlying Mechanisms and Management. Int. J. Mol. Sci. 2021, 22, 4081. [Google Scholar] [CrossRef]
- Alonso-Bellido, I.M.; Bachiller, S.; Vázquez, G.; Cruz-Hernández, L.; Martínez, E.; Ruiz-Mateos, E.; Deierborg, T.; Venero, J.L.; Real, L.M.; Ruiz, R. The Other Side of SARS-CoV-2 Infection: Neurological Sequelae in Patients. Front. Aging Neurosci. 2021, 13, 632673. [Google Scholar] [CrossRef]
- Wu, Y.; Guo, C.; Tang, L.; Hong, Z.; Zhou, J.; Dong, X.; Yin, H.; Xiao, Q.; Tang, Y.; Qu, X.; et al. Prolonged presence of SARS-CoV-2 viral RNA in faecal samples. Lancet Gastroenterol. Hepatol. 2020, 5, 434–435. [Google Scholar] [CrossRef]
- Lamers, M.M.; Beumer, J.; Van Der Vaart, J.; Knoops, K.; Puschhof, J.; Breugem, T.I.; Ravelli, R.B.; Paul van Schayck, J.; Mykytyn, A.Z.; Duimel, H.Q. SARS-CoV-2 productively infects human gut enterocytes. Science 2020, 369, 50–54. [Google Scholar] [CrossRef]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in Different Types of Clinical Specimens. JAMA 2020, 323, 1843–1844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, X.; Lian, J.S.; Hu, J.H.; Gao, J.; Zheng, L.; Zhang, Y.M.; Hao, S.R.; Jia, H.Y.; Cai, H.; Zhang, X.L.; et al. Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms. Gut 2020, 69, 1002–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehraeen, E.; Behnezhad, F.; Salehi, M.A.; Noori, T.; Harandi, H.; SeyedAlinaghi, S. Olfactory and gustatory dysfunctions due to the coronavirus disease (COVID-19): A review of current evidence. Eur. Arch. Otorhinolaryngol. 2021, 278, 307–312. [Google Scholar] [CrossRef] [PubMed]
- McDonald, L. Healing after COVID-19: Are survivors at risk for pulmonary fibrosis? Am. J. Physiol.-Lung Cell Mol. Physiol. 2021, 320, L257–L265. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Q.; Xu, M.; Li, J.; Liu, Y.; Zhang, J.; Xu, Y.; Dong, W. Clinical sequelae of COVID-19 survivors in Wuhan, China: A single-centre longitudinal study. Clin. Microbiol. Infect. 2021, 27, 89–95. [Google Scholar] [CrossRef]
- Rumende, C.M.; Susanto, E.C.; Sitorus, T.P. The Management of Pulmonary Fibrosis in COVID-19. Acta Med. Indones. 2021, 53, 233–241. [Google Scholar]
- Antony, T.; Acharya, K.V.; Unnikrishnan, B.; Keerthi, N. A silent march-Post covid fibrosis in asymptomatics—A cause for concern? Indian J. Tuberc. 2022. Epub ahead of print. [Google Scholar] [CrossRef]
- Li, X.; Shen, C.; Wang, L.; Majumder, S.; Zhang, D.; Deen, M.J.; Li, Y.; Qing, L.; Zhang, Y.; Chen, C.; et al. Pulmonary fibrosis and its related factors in discharged patients with new coronavirus pneumonia: A cohort study. Respir. Res. 2021, 22, 203. [Google Scholar] [CrossRef]
- Colarusso, C.; Maglio, A.; Terlizzi, M.; Vitale, C.; Molino, A.; Pinto, A.; Vatrella, A.; Sorrentino, R. Post-COVID-19 Patients Who Develop Lung Fibrotic-like Changes Have Lower Circulating Levels of IFN-β but Higher Levels of IL-1α and TGF-β. Biomedicines 2021, 9, 1931. [Google Scholar] [CrossRef]
- Townsend, L.; Dowds, J.; O’Brien, K.; Sheill, G.; Dyer, A.H.; O’Kelly, B.; Hynes, J.P.; Mooney, A.; Dunne, J.; Ni Cheallaigh, C.; et al. Persistent Poor Health after COVID-19 Is Not Associated with Respiratory Complications or Initial Disease Severity. Ann. Am. Thorac. Soc. 2021, 18, 997–1003. [Google Scholar] [CrossRef]
- Wang, C.; Yu, C.; Jing, H.; Wu, X.; Novakovic, V.A.; Xie, R.; Shi, J. Long COVID: The Nature of Thrombotic Sequelae Determines the Necessity of Early Anticoagulation. Front. Cell. Infect. Microbiol. 2022, 12, 861703. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | n (%) |
|---|---|
| Female | 91 (63.0) |
| Age | 35 (29–45) * |
| Obesity | 8 (5.4) |
| Hypertension | 7 (4.7) |
| Diabetes | 5 (3.4) |
| Smoking | 7 (4.7) |
| BCG vaccine | 142 (95.3) |
| Influenza vaccine | 121 (81.2) |
| Pneumonia | 58 (38.9) |
| Baseline (1) | Active Infection (2) | Post-Infection (3) | 1 vs. 2 | 1 vs. 3 | 2 vs. 3 | |
|---|---|---|---|---|---|---|
| Signs and Symptoms | (%) | (%) | (%) | p-Value | p-Value | p-Value |
| Neurological | ||||||
| General attack | 9.4 | 28.2 | 3.4 | <0.0001 | 0.064 | <0.0001 |
| Arthralgia | 22.2 | 42.3 | 14.8 | <0.0001 | 0.093 | <0.0001 |
| Myalgia | 14.1 | 53.7 | 13.4 | <0.0001 | 0.999 | <0.0001 |
| Dysgeusia/Ageusia | 5.4 | 51.0 | 10.7 | <0.0001 | 0.115 | <0.0001 |
| Anosmia | 4.7 | 55.0 | 13.4 | <0.0001 | 0.011 | <0.0001 |
| Odynophagia | 9.4 | 40.3 | 7.4 | <0.0001 | 0.664 | <0.0001 |
| Abdominal pain | 4 | 18.8 | 6.0 | <0.0001 | 0.581 | <0.0001 |
| Headache | 43.6 | 59.7 | 21.5 | 0.005 | <0.0001 | <0.0001 |
| Fatigue or weakness | 0.7 | 65.1 | 36.9 | <0.0001 | <0.0001 | <0.0001 |
| Difficult concentrating | 0 | 29.5 | 14.8 | <0.0001 | <0.0001 | 0.015 |
| Blurred vision | 0 | 8.7 | 8.1 | <0.0001 | <0.0001 | 0.617 |
| Hair loss | 0 | 24.2 | 21.5 | <0.0001 | <0.0001 | 0.999 |
| Cramps | 0 | 15.4 | 12.1 | <0.0001 | <0.0001 | 0.774 |
| Ear disorders | 1.3 | 26.2 | 12.1 | <0.0001 | <0.0001 | 0.001 |
| Sleeping problems | 0 | 34.9 | 17.5 | <0.0001 | <0.0001 | <0.0001 |
| Anxiety | 0 | 20.8 | 14.1 | <0.0001 | <0.0001 | 0.041 |
| Gastric | ||||||
| Diarrhea | 6.7 | 33.6 | 6.0 | <0.0001 | 0.999 | <0.0001 |
| Vomit | 0 | 7.4 | 0 | 0.001 | 0.999 | 0.001 |
| Nausea | 1.3 | 16.1 | 2.0 | <0.0001 | 0.999 | <0.0001 |
| Xerostomia | 0.7 | 26.9 | 7.4 | <0.0001 | 0.006 | <0.0001 |
| Mouth ulcers | 0 | 6.7 | 3.4 | 0.002 | 0.063 | 0.227 |
| Bite alteration | 0 | 21.5 | 13.4 | <0.0001 | <0.0001 | 0.012 |
| Weight changes | 0 | 14.1 | 10.7 | <0.0001 | <0.0001 | 0.808 |
| Inflammatory | ||||||
| Conjunctivitis | 5.4 | 20.8 | 4.7 | <0.0001 | 0.999 | <0.0001 |
| Lymphadenopathy | 0 | 17.5 | 3.4 | <0.0001 | 0.063 | <0.0001 |
| Dermatitis | 0 | 16.8 | 12.1 | <0.0001 | <0.0001 | 0.167 |
| Irritability | 4.0 | 22.8 | 7.4 | <0.0001 | 0.332 | <0.0001 |
| Diaphoresis | 10.7 | 42.3 | 10.1 | <0.0001 | 0.999 | <0.0001 |
| Fever | 20.8 | 36.2 | 0 | 0.001 | <0.0001 | <0.0001 |
| Cardiorespiratory | ||||||
| Rhinorrhea | 26.9 | 27.5 | 4.7 | 0.882 | <0.0001 | <0.0001 |
| Nasal congestion | 1.3 | 27.5 | 6.7 | <0.0001 | 0.039 | <0.0001 |
| Cough | 38.9 | 40.3 | 7.4 | 0.773 | <0.0001 | <0.0001 |
| Dyspnea (mild/moderate) | 6.0 | 40.3 | 22.8 | <0.0001 | <0.0001 | 0.001 |
| Tachycardia | 0 | 28.2 | 14.8 | <0.0001 | <0.0001 | 0.001 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Variable | HR | CI 95% | p-Value | HR | CI 95% | p-Value |
| Pneumonia | 2.2 | 1.4–3.5 | 0.0007 | 2.41 | 1.51–3.82 | <0.001 |
| PCR positive test > 4 weeks | 4.4 | 2.1–8.7 | <0.0001 | 5.38 | 2.34–12.35 | <0.001 |
| Age | 1.01 | 0.97–1.05 | 0.46 | 0.99 | 0.95–1.04 | 0.96 |
| Sex | 1.2 | 0.59–1.99 | 0.55 | 1.3 | 0.6–1.8 | 0.47 |
| Diabetes | 0.94 | 0.29–3.05 | 0.93 | - | - | - |
| Hypertension | 1.28 | 0.46–3.54 | 0.63 | - | - | - |
| Obesity | 1.9 | 0.69–5.28 | 0.23 | - | - | - |
| Smoking | 1.77 | 0.71–0.44 | 0.21 | - | - | - |
| BCG vaccine | 0.69 | 0.42–1.21 | 0.2 | - | - | - |
| Influenza vaccine | 0.91 | 0.91–2.33 | 0.68 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Plata, R.; Higuera-Iglesias, A.-L.; Torres-Espíndola, L.M.; Aquino-Gálvez, A.; Velázquez Cruz, R.; Camarena, Á.; Chávez Alderete, J.; Romo García, J.; Alvarado-Vásquez, N.; Martínez Briseño, D.; et al. Risk of Pulmonary Fibrosis and Persistent Symptoms Post-COVID-19 in a Cohort of Outpatient Health Workers. Viruses 2022, 14, 1843. https://0-doi-org.brum.beds.ac.uk/10.3390/v14091843
Fernández-Plata R, Higuera-Iglesias A-L, Torres-Espíndola LM, Aquino-Gálvez A, Velázquez Cruz R, Camarena Á, Chávez Alderete J, Romo García J, Alvarado-Vásquez N, Martínez Briseño D, et al. Risk of Pulmonary Fibrosis and Persistent Symptoms Post-COVID-19 in a Cohort of Outpatient Health Workers. Viruses. 2022; 14(9):1843. https://0-doi-org.brum.beds.ac.uk/10.3390/v14091843
Chicago/Turabian StyleFernández-Plata, Rosario, Anjarath-Lorena Higuera-Iglesias, Luz María Torres-Espíndola, Arnoldo Aquino-Gálvez, Rafael Velázquez Cruz, Ángel Camarena, Jaime Chávez Alderete, Javier Romo García, Noé Alvarado-Vásquez, David Martínez Briseño, and et al. 2022. "Risk of Pulmonary Fibrosis and Persistent Symptoms Post-COVID-19 in a Cohort of Outpatient Health Workers" Viruses 14, no. 9: 1843. https://0-doi-org.brum.beds.ac.uk/10.3390/v14091843