
Molnupiravir and Nirmatrelvir/Ritonavir: Tolerability, Safety, and Adherence in a Retrospective Cohort Study
 , , , , , and
, , , , , and
Abstract
:1. Introduction
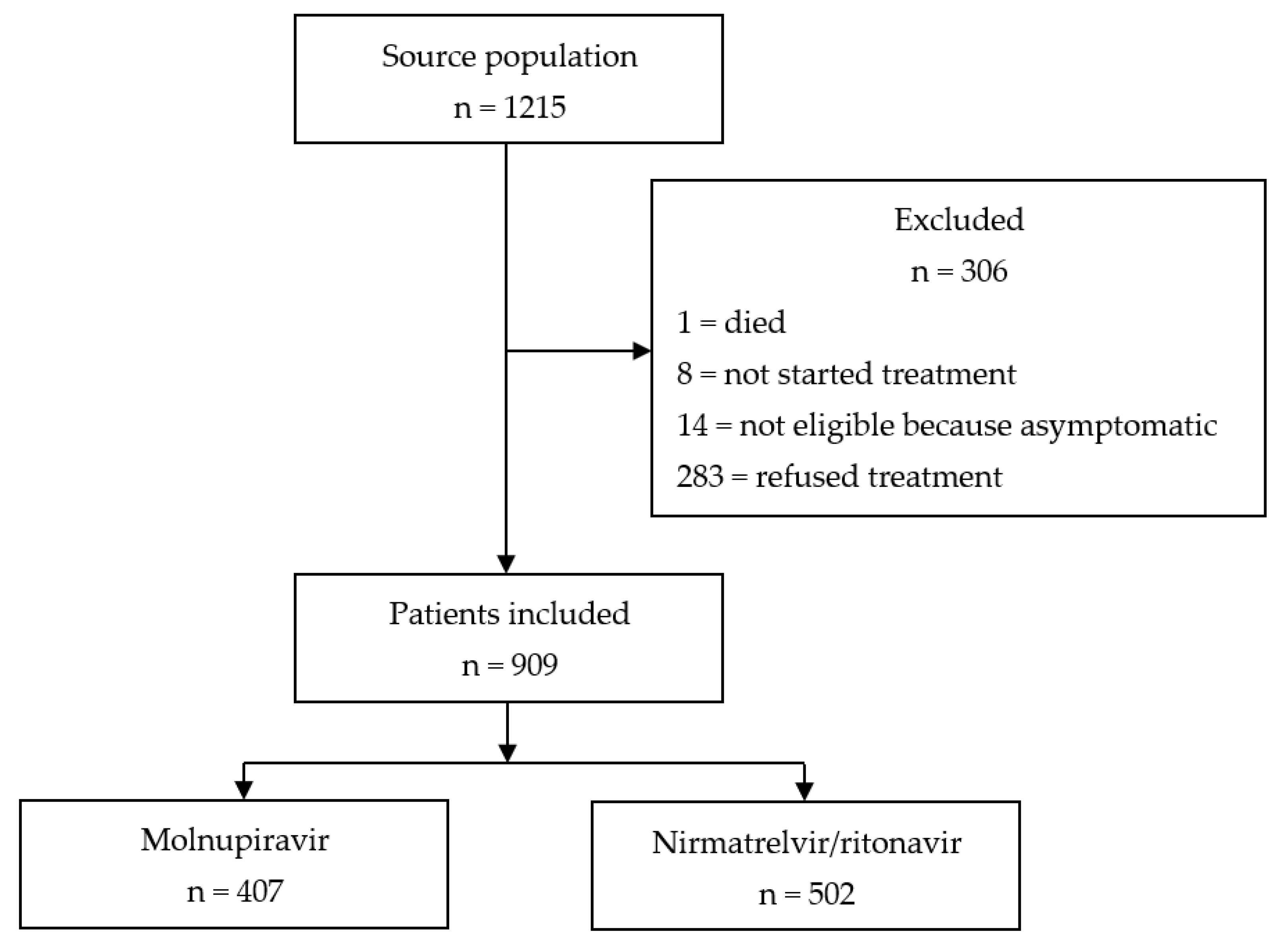
2. Materials and Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zeng, H.; Ma, Y.; Zhou, Z.; Liu, W.; Huang, P.; Jiang, M.; Liu, Q.; Chen, P.; Luo, H.; Chen, Y. Spectrum and Clinical Characteristics of Symptomatic and Asymptomatic Coronavirus Disease 2019 (COVID-19) With and Without Pneumonia. Front. Med. 2021, 8, 645651. [Google Scholar] [CrossRef] [PubMed]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Robertson, C.; Stowe, J.; Tessier, E.; Simmons, R.; Roberts, R.; O’Doherty, M.; Brown, K.; et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on COVID-19 related symptoms, hospital admissions, and mortality in older adults in England: Test negative case-control study. BMJ 2021, 373, n1088. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Vangeel, L.; Chiu, W.; De Jonghe, S.; Maes, P.; Sletchen, B.; Raymenants, J.; Andre, E.; Leyssen, P.; Neyts, J.; Jochmans, D. Remdesivir, Molnupiravir and Nirmatrelvir remain active against SARS-CoV-2 Omicron and other variants of concern. Antivir. Res. 2022, 198, 105252. [Google Scholar] [CrossRef] [PubMed]
- Jayk Bernal, A.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; De los Reyes, V.; Martin-Quiros, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of COVID-19 in Nonhospitalized Patients. N. Engl. J. Med. 2022, 386, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Hammond, J.; Leister-Tebbe, H.; Gardner, A.; Abreu, P.; Bao, W.; Wisemandle, W.; Baniecki, M.; Hendrick, V.M.; Damle, B.; Simón-Campos, A.; et al. Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with COVID-19. N. Engl. J. Med. 2022, 386, 1397–1408. [Google Scholar] [CrossRef] [PubMed]
- Burdet, C.; Ader, F. Real-world effectiveness of oral antivirals for COVID-19. Lancet 2022, 400, 1175–1176. [Google Scholar] [CrossRef] [PubMed]
- Scaglione, V.; Rotundo, S.; Marascio, N.; De Marco, C.; Lionello, R.; Veneziano, C.; Berardelli, L.; Quirino, A.; Olivadese, V.; Serapide, F.; et al. Lessons learned and implications of early therapies for coronavirus disease in a territorial service centre in the Calabria region: A retrospective study. BMC Infect Dis. 2022, 22, 793. [Google Scholar]
- Pontolillo, M.; Ucciferri, C.; Borrelli, P.; Di Nicola, M.; Vecchiet, J.; Falasca, K. Molnupiravir as an Early Treatment for COVID-19: A Real Life Study. Pathogens. 2022, 11, 1121. [Google Scholar] [CrossRef] [PubMed]
- Gentile, I.; Scotto, R.; Shiano Moriello, N.; Pinchera, B.; Villari, R.; Trucillo, E.; Ametrano, L.; Fusco, L.; Castaldo, G.; Buonomo, A.R.; et al. Nirmatrelvir/Ritonavir and Molnupiravir in the Treatment of Mild/Moderate COVID-19: Results of a Real-Life Study. Vaccines 2022, 10, 1731. [Google Scholar] [CrossRef] [PubMed]
- De Vito, A.; Colpani, A.; Bitti, A.; Zauli, B.; Meloni, M.C.; Fois, M.; Denti, L.; Bacciu, S.; Marcia, C.; Maida, I.; et al. Safety and efficacy of molnupiravir in SARS-CoV-2-infected patients: A real-life experience. J. Med. Virol. 2022, 94, 5582–5588. [Google Scholar] [CrossRef] [PubMed]
- Wen, W.; Chen, C.; Tang, J.; Wang, C.; Zhou, M.; Cheng, Y.; Zhou, X.; Wu, Q.; Zhang, X.; Feng, Z.; et al. Efficacy and safety of three new oral antiviral treatment (molnupiravir, fluvoxamine and Paxlovid) for COVID-19a meta-analysis. Ann. Med. 2022, 54, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Izcovich, A.; Siemieniuk, R.A.; Bartoszko, J.J.; Ge, L.; Zeraatkar, D.; Kum, E.; Qasim, A.; Khamis, A.M.; Rochwerg, B.; Agoritsas, T.; et al. Adverse effects of remdesivir, hydroxychloroquine and lopinavir/ritonavir when used for COVID-19: Systematic review and meta-analysis of randomised trials. BMJ Open 2022, 12, e048502. [Google Scholar] [CrossRef] [PubMed]
- Najjar-Debbiny, R.; Gronich, N.; Weber, G.; Khoury, J.; Amar, M.; Stein, N.; Goldstein, L.H.; Saliba, W. Effectiveness of molnupiravir in high-risk patients: A propensity score matched analysis. Clin. Infect. Dis. 2022, ciac781. [Google Scholar] [CrossRef] [PubMed]
- Anderson, G.D. Gender differences in pharmacological response. Int. Rev. Neurobiol. 2008, 83, 1–10. [Google Scholar] [PubMed]
- Miller, A.M. Gender-based differences in the toxicity of pharmaceuticals. The food and drug administration’s perspectives. Int. J. Toxicol. 2001, 20, 149–152. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Overall N = 909 | Molnupiravir N = 407 | Nirmatrelvir/Ritonavir N = 502 | p Value | |
|---|---|---|---|---|---|
| Age, median (IQR) | 73 (62–82) | 80 (71–86) | 68 (56–76) | <0.05 | |
| Gender, male, n (%) | 439 (48.3) | 198 (48.6) | 241 (48.0) | 0.85 | |
| Vaccination against SARS-CoV-2, n (%) | 865 (95.2) | 391 (96.0) | 474 (94.4) | 0.25 | |
| Age ≥ 65 years, n (%) | 674 (74.2) | 353 (86.7) | 321 (63.9) | <0.05 | |
| Obesity, n (%) | 125 (13.7) | 42 (10.3) | 83 (16.5) | <0.05 | |
| Diabetes, n (%) | 175 (19.3) | 84 (20.6) | 91 (18.1) | 0.33 | |
| Cardiovascular diseases, n (%) | 467 (51.4) | 271 (66.6) | 196 (39.0) | <0.05 | |
| Cancer, n (%) | 60 (6.6) | 25 (6.1) | 35 (7.0) | 0.62 | |
| Renal disease, n (%) | 33 (3.6) | 22 (5.4) | 11 (2.2) | <0.05 | |
| Lung disease, n (%) | 162 (17.8) | 65 (16.0) | 97 (19.3) | 0.20 | |
| Neurological disease, n (%) | 59 (6.5) | 38 (9.3) | 21 (4.2) | <0.05 | |
| Immunosuppression, n (%) | 75 (8.3) | 29 (7.1) | 46 (9.2) | 0.27 | |
| Other comorbidities, n (%) | 96 (10.6) | 53 (13.0) | 43 (8.6) | 0.03 | |
| N comorbidities/patients, median (IQR) | 1 (1–2) | 1 (1–2) | 1 (1–2) | <0.05 | |
| N comorbidities/patients, mean (±SD) | 1.4 (1.0) | 1.6 (1.0) | 1.2 (0.9) | 0.04 | |
| Time from symptom onset to diagnosis, days, median (IQR) | 1 (0–2) | 1 (0–2) | 1 (0–2) | 0.21 | |
| Time from symptom onset to treatment, days, median (IQR) | 3 (2–4) | 3 (2–4) | 3 (2–4) | 0.24 | |
| Number of symptoms at presentation, median (IQR) | 3 (2–4) | 3 (2–3) | 3 (2–4) | 0.02 | |
| Symptoms at presentation, n (%) | Fever | 509 (56.0) | 219 (53.8) | 290 (57.8) | 0.23 |
| Shortness of breath | 9 (1.0) | 5 (1.2) | 4 (0.8) | 0.51 | |
| Headache | 183 (20.1) | 119 (23.7) | 64 (15.7) | <0.05 | |
| Anosmia | 16 (1.8) | 8 (2.0) | 8 (1.6) | 0.67 | |
| Ageusia | 21 (2.3) | 6 (1.5) | 15 (3.0) | 0.13 | |
| Sore throat | 319 (35.1) | 135 (33.2) | 184 (36.7) | 0.27 | |
| Cold | 143 (15.7) | 54 (13.3) | 89 (17.7) | 0.07 | |
| Myalgia | 259 (28.5) | 95 (23.3) | 164 (32.7) | <0.05 | |
| Tachypnoea | 9 (1.0) | 5 (1.2) | 4 (0.8) | 0.51 | |
| Asthenia | 392 (43.1) | 186 (45.7) | 206 (41.0) | 0.16 | |
| Gastrointestinal disorders | 62 (6.8) | 31 (7.6) | 31 (6.2) | 0.39 | |
| Characteristic | Overall N = 909 | Molnupiravir N = 407 | Nirmatrelvir/Ritonavir N = 502 | p Value | |
|---|---|---|---|---|---|
| Side effects, yes, n (%) | 124 (13.6) | 28 (6.9) | 96 (19.1) | <0.05 | |
| Side effect/patient, median (IQR) | 1 (1–1) | 1 (1–1) | 1 (1–1) | 0.98 | |
| Patients with ADE >1, n (%) | 24 (2.6) | 6 (1.5) | 18 (3.6) | 0.06 | |
| Type of side effects, n (%) | Dysgeusia | 67 (7.4) | 5 (1.2) | 62 (12.4) | <0.05 |
| Bloating | 21 (2.3) | 7 (1.7) | 14 (2.8) | 0.29 | |
| Allergy | 3 (0.3) | 2 (0.5) | 1 (0.2) | 0.44 | |
| Nausea/vomiting | 18 (2.0) | 8 (2.0) | 10 (2.0) | 0.98 | |
| Diarrhoea | 19 (2.1) | 4 (1.0) | 15 (3.0) | <0.05 | |
| Headache | 9 (0.9) | 2 (0.5) | 7 (1.4) | 0.17 | |
| Other | 11 (1.2) | 5 (1.2) | 6 (1.2) | 0.96 | |
| Adverse event grading | Grade 1 | 98 (10.8) | 18 (4.4) | 80 (13.9) | <0.05 |
| Grade 2 | 23 (2.5) | 8 (1.9) | 15 (2.9) | 0.398 | |
| Grade 3 | 3 (0.33) | 2 (0.4) | 1 (0.2) | 0.589 | |
| Completed treatment, n (%) | 865 (95.6) | 390 (95.8) | 475 (94.6) | 0.40 | |
| Median proportion of doses taken, median (IQR) | 100 (100–100) | 100 (100–100) | 100 (100–100) | 0.40 | |
| Proportion of doses taken, mean (±SD) | 97.7 (11.2) | 98.0 (10.6) | 97.6 (11.7) | 0.52 | |
| Proportion of subjects taken expected antiviral doses: | ≤50%, n (%) | 26 (2.9) | 9 (2.2) | 17 (3.4) | 0.42 |
| >50%, n (%) | 883 (97.1) | 398 (97.8) | 485 (96.6) | 0.42 | |
| Access to ED, yes, n (%) | 27 (3.0) | 14 (3.4) | 13 (2.6) | 0.45 | |
| Admission, yes, n (%) | 4 (0.4) | 1 (0.2) | 3 (0.6) | 0.42 | |
| Death, yes, n (%) | 2 (0.2) | 2 (0.5) | 0 (0.0) | 0.11 | |
| Symptom’s’ resolution within 5 days, n (%) | 618 (68.0) | 293 (71.9) | 325 (64.8) | 0.02 | |
| Characteristic | Univariate Analysis | Multivariable Analysis | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | Lower 95% CI | Upper 95% CI | p Value | OR | Lower 95% CI | Upper 95% CI | p Value | ||
| Age, median (IQR) | 0.973 | 0.946 | 1.000 | 0.050 | 0.993 | 0.939 | 1.050 | 0.803 | |
| Gender, male, n (%) | 0.328 | 0.136 | 0.790 | <0.05 | 0.242 | 0.084 | 0.693 | 0.008 | |
| Vaccination against SARS-CoV-2, n (%) | 0.138 | 0.044 | 0.429 | <0.05 | 0.148 | 0.031 | 0.704 | 0.016 | |
| Age ≥ 65 years, n (%) | 0.345 | 0.144 | 0.829 | 0.02 | 0.243 | 0.042 | 1.390 | 0.112 | |
| Obesity, n (%) | 1.050 | 0.302 | 3.620 | 0.943 | 0.279 | 0.03 | 2.140 | 0.219 | |
| Diabetes, n (%) | 0.623 | 0.210 | 1.850 | 0.393 | 0.581 | 0.1150 | 2.930 | 0.511 | |
| Cardiovascular diseases, n (%) | 2.43 | 0.903 | 6.540 | 0.072 | 2.560 | 0.541 | 12.11 | 0.236 | |
| Cancer, n (%) | 0.548 | 0.071 | 4.200 | 0.563 | 0.232 | 0.018 | 2.890 | 0.256 | |
| Renal disease, n (%) | 0.000 | 0.000 | Inf | 0.986 | 0 | 0 | inf | 0.993 | |
| Lung disease, n (%) | 1.160 | 0.423 | 3.160 | 0.778 | 0.715 | 0.112 | 4.570 | 0.723 | |
| Neurological disease, n (%) | 1.180 | 0.339 | 4.100 | 0.795 | 1.210 | 0.199 | 7.330 | 0.837 | |
| Immunosuppression, n (%) | 1.630 | 0.461 | 5.760 | 0.448 | 1.450 | 0.226 | 9.320 | 0.695 | |
| Other comorbidities, n (%) | 0.790 | 0.230 | 2.710 | 0.707 | 0.351 | 0.0501 | 2.470 | 0.293 | |
| N comorbidities/patients, median (IQR) | 1.070 | 0.824 | 1.390 | 0.601 | 1.600 | 0.494 | 5.200 | 0.432 | |
| Time from symptom onset to diagnosis, days, median (IQR) | 1.400 | 1.020 | 1.930 | 0.036 | 1.250 | 0.803 | 1.930 | 0.326 | |
| Time from symptom onset to treatment, days, median (IQR) | 1.210 | 0.905 | 1.620 | 0.198 | 1.070 | 0.713 | 1.590 | 0.755 | |
| Number of symptoms at presentation, median (IQR) | 1.070 | 0.824 | 1.390 | 0.601 | 1.040 | 0.325 | 3.310 | 0.953 | |
| Symptoms at presentation, n (%) | Fever | 1.35 | 0.618 | 2.970 | 0.449 | 1.450 | 0.328 | 6.400 | 0.626 |
| Shortness of breath | 0.000 | 0.000 | Inf | 0.990 | 0 | 0 | inf | 0.993 | |
| Headache | 2.31 | 0.969 | 5.490 | 0.058 | 2.660 | 0.486 | 14.600 | 0.259 | |
| Anosmia | 1.97 | 0.234 | 16.600 | 0.533 | 13.300 | 0.647 | 272 | 0.093 | |
| Ageusia | 0.000 | 0.000 | Inf | 0.989 | 0 | 0 | inf | 0.096 | |
| Sore throat | 0.794 | 0.340 | 1.850 | 0.593 | 0.974 | 0.195 | 4.860 | 0.975 | |
| Cold | 0.772 | 0.225 | 2.650 | 0.681 | 0.817 | 0.240 | 5.618 | 0.819 | |
| Myalgia | 0.889 | 0.349 | 2.260 | 0.804 | 0.369 | 0.068 | 2 | 0.248 | |
| Tachypnoea | 3.47 | 0.375 | 32.200 | 0.273 | 5.020 | 0.2740 | 92 | 0.277 | |
| Asthenia | 1.03 | 0.478 | 2.230 | 0.936 | 1.34 | 0.293 | 6.090 | 0.708 | |
| Gastrointestinal disorders | 0.431 | 0.057 | 3.280 | 0.416 | 0.29 | 0.017 | 4.770 | 0.386 | |
| Characteristic | Univariate Analysis | Multivariable Analysis | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | Lower 95% CI | Upper 95% CI | p Value | OR | Lower 95% CI | Upper 95% CI | p Value | ||
| Age, median (IQR) | 0.974 | 0.961 | 0.988 | <0.05 | 0.980 | 0.955 | 1.010 | 0.11 | |
| Gender, male, n (%) | 0.621 | 0.394 | 0.979 | <0.05 | 0.542 | 0.326 | 0.900 | 0.017 | |
| Vaccination against SARS-CoV-2, n (%) | 0.694 | 0.286 | 1.680 | 0.418 | 0.655 | 0.246 | 1.750 | 0.398 | |
| Age ≥ 65 years, n (%) | 0.416 | 0.265 | 0.653 | <0.05 | 0.680 | 0.319 | 1.450 | 0.318 | |
| Obesity, n (%) | 1.550 | 0.892 | 2.70 | 0.119 | 1.130 | 0.502 | 2.550 | 0.767 | |
| Diabetes, n (%) | 0.591 | 0.308 | 1.14 | 0.115 | 0.656 | 0.269 | 1.600 | 0.353 | |
| Cardiovascular diseases, n (%) | 1.14 | 0.728 | 1.800 | 0.558 | 1.640 | 0.735 | 3.640 | 0.228 | |
| Cancer, n (%) | 0.689 | 0.260 | 1.820 | 0.453 | 0.826 | 0.253 | 2.700 | 0.751 | |
| Renal disease, n (%) | 0.939 | 0.199 | 4.420 | 0.936 | 1.480 | 0.243 | 9.04 | 0.670 | |
| Lung disease, n (%) | 1.220 | 0.705 | 2.100 | 0.482 | 0.923 | 0.071 | 11.900 | 0.951 | |
| Neurological disease, n (%) | 2.200 | 0.864 | 5.620 | 0.098 | 1.710 | 0.524 | 5.590 | 0.374 | |
| Immunosuppression, n (%) | 1.200 | 0.571 | 2.500 | 0.636 | 0.759 | 0.274 | 2.100 | 0.596 | |
| Other comorbidities, n (%) | 1.330 | 0.631 | 2.800 | 0.454 | 1.380 | 0.512 | 3.730 | 0.524 | |
| N comorbidities/patients, median (IQR) | 1.140 | 0.900 | 1.430 | 0.282 | 0.963 | 0.517 | 1.790 | 0.904 | |
| Time from symptom onset to diagnosis, days, median (IQR) | 0.993 | 0.800 | 1.230 | 0.946 | 0.927 | 0.715 | 1.20 | 0.569 | |
| Time from symptom onset to treatment, days, median (IQR) | 1.060 | 0.908 | 1.240 | 0.448 | 1.060 | 0.875 | 1.280 | 0.567 | |
| Number of symptoms at presentation, median (IQR) | 1.120 | 0.972 | 1.290 | 0.118 | 1.060 | 0.606 | 1.84 | 0.848 | |
| Symptoms at presentation, n (%) | Fever | 1.350 | 0.851 | 2.13 | 1.35 | 1.200 | 0.561 | 2.580 | 0.633 |
| Shortness of breath | 2.700 | 1.400 | 5.220 | <0.05 | 2.080 | 0.778 | 5.570 | 0.144 | |
| Headache | 1.340 | 0.808 | 2.210 | 0.259 | 1.170 | 0.518 | 2.650 | 0.705 | |
| Anosmia | 2.590 | 0.607 | 11.000 | 0.199 | 2.340 | 0.366 | 14.900 | 0.369 | |
| Ageusia | 1.560 | 0.486 | 5.010 | 1.560 | 0.859 | 0.187 | 3.940 | 0.844 | |
| Sore throat | 0.990 | 0.623 | 1.570 | 0.990 | 0.912 | 0.423 | 1.970 | 0.813 | |
| Cold | 0.998 | 0.557 | 1.790 | 0.998 | 0.946 | 0.400 | 2.240 | 0.899 | |
| Myalgia | 1.460 | 0.919 | 2.310 | 1.460 | 1.180 | 0.537 | 2.600 | 0.679 | |
| Tachypnoea | 1.410 | 0.145 | 13.700 | 1.41 | 0.956 | 0.085 | 10.720 | 0.871 | |
| Asthenia | 0.705 | 0.443 | 1.120 | 0.705 | 0.541 | 0.252 | 1.160 | 0.116 | |
| Gastrointestinal disorders | 0.609 | 0.208 | 1.780 | 0.609 | 0.405 | 0.112 | 1.460 | 0.168 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazzitelli, M.; Mengato, D.; Sasset, L.; Ferrari, A.; Gardin, S.; Scaglione, V.; Bonadiman, N.; Calandrino, L.; Cavinato, S.; Trivellato, S.; et al. Molnupiravir and Nirmatrelvir/Ritonavir: Tolerability, Safety, and Adherence in a Retrospective Cohort Study. Viruses 2023, 15, 384. https://0-doi-org.brum.beds.ac.uk/10.3390/v15020384
Mazzitelli M, Mengato D, Sasset L, Ferrari A, Gardin S, Scaglione V, Bonadiman N, Calandrino L, Cavinato S, Trivellato S, et al. Molnupiravir and Nirmatrelvir/Ritonavir: Tolerability, Safety, and Adherence in a Retrospective Cohort Study. Viruses. 2023; 15(2):384. https://0-doi-org.brum.beds.ac.uk/10.3390/v15020384
Chicago/Turabian StyleMazzitelli, Maria, Daniele Mengato, Lolita Sasset, Anna Ferrari, Samuele Gardin, Vincenzo Scaglione, Nicola Bonadiman, Lucrezia Calandrino, Silvia Cavinato, Sabrina Trivellato, and et al. 2023. "Molnupiravir and Nirmatrelvir/Ritonavir: Tolerability, Safety, and Adherence in a Retrospective Cohort Study" Viruses 15, no. 2: 384. https://0-doi-org.brum.beds.ac.uk/10.3390/v15020384