
Field Performance of a Rapid Test to Detect Progressive, Regressive, and Abortive Feline Leukemia Virus Infections in Domestic Cats in Australia and Germany
 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Australian Samples (Cohort 1; n = 200)
2.2. German Samples (Cohort 2; n = 170)
2.3. Evaluation of v-RetroFel® Test Results
- p27-positive/p15E antibody-positive results indicate progressive or early regressive FeLV infections;
- p27-negative/p15E antibody-positive results indicate regressive or abortive FeLV infections;
- p27-negative/p15E antibody-negative results indicate no exposure to FeLV;
- p27-positive/p15E antibody-negative results are unlikely to be observed (but would also be considered indicative of progressive infections).
3. Results
3.1. Australian Samples (n = 200)
3.1.1. Results of v-RetroFel®Ag/Ab Testing
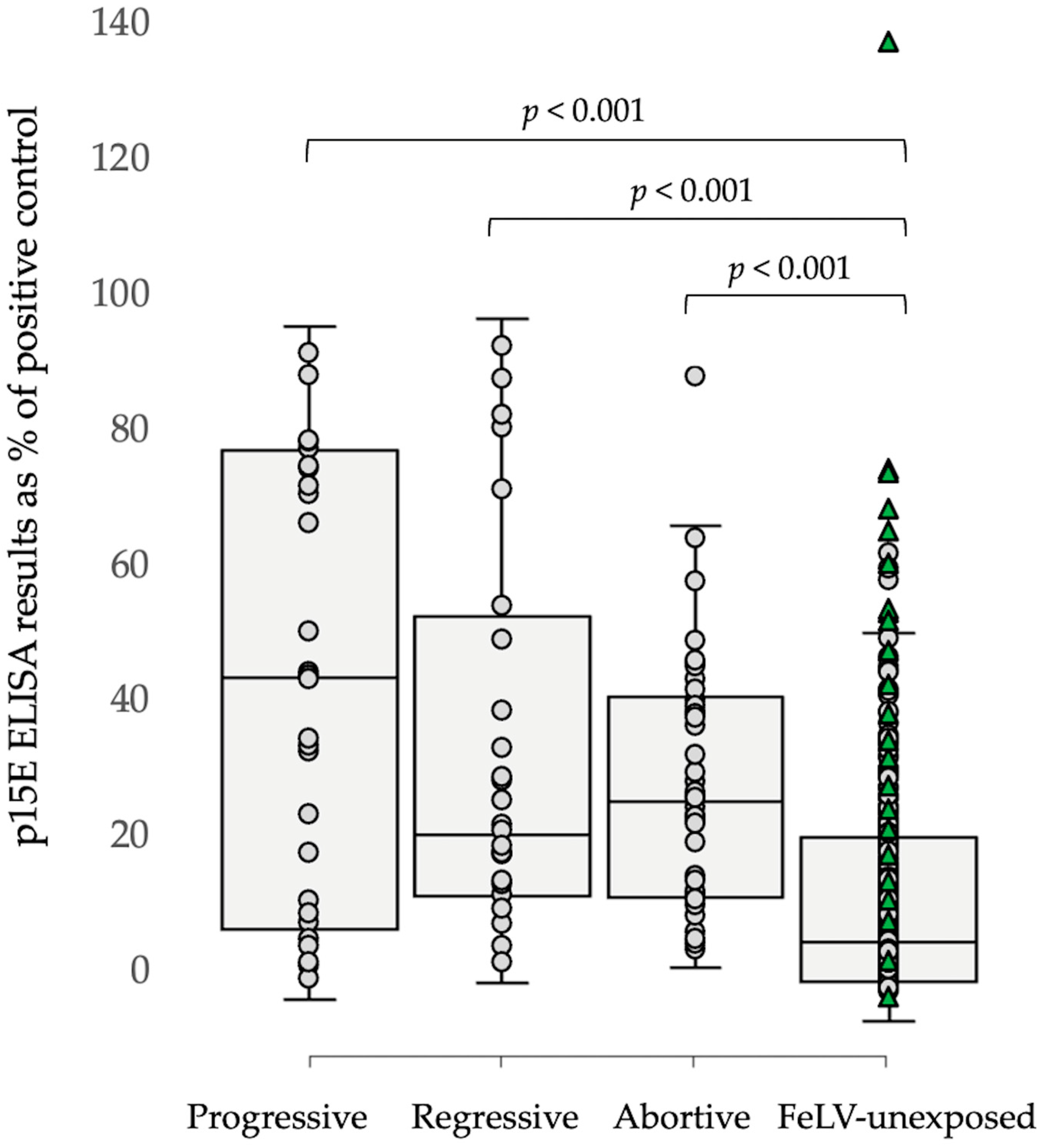
3.1.2. Results of p15E Laboratory ELISA Testing
3.1.3. Results of v-RetroFel®FIV Testing
3.2. German Samples (n = 170)
3.2.1. Results of v-RetroFel®Ag/Ab Testing
3.2.2. Results of p15E Laboratory ELISA Testing
3.2.3. Results of v-RetroFel®FIV Testing
3.3. Comparing Results from Cohorts 1 and 2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Willett, B.J.; Hosie, M.J. Feline leukaemia virus: Half a century since its discovery. Vet. J. 2013, 195, 16–23. [Google Scholar] [CrossRef]
- O’Brien, S.J.; Troyer, J.L.; Brown, M.A.; Johnson, W.E.; Antunes, A.; Roelke, M.E.; Pecon-Slattery, J. Emerging viruses in the Felidae: Shifting paradigms. Viruses 2012, 4, 236–257. [Google Scholar] [CrossRef] [PubMed]
- Meli, M.L.; Cattori, V.; Martínez, F.; López, G.; Vargas, A.; Simón, M.A.; Zorrilla, I.; Muñoz, A.; Palomares, F.; López-Bao, J.V.; et al. Feline leukemia virus and other pathogens as important threats to the survival of the critically endangered Iberian lynx (Lynx pardinus). PLoS ONE 2009, 4, e4744. [Google Scholar] [CrossRef] [PubMed]
- Guimaraes, A.M.S.; Brandão, P.E.; de Moraes, W.; Cubas, Z.S.; Santos, L.C.; Villarreal, L.Y.B.; Robes, R.R.; Coelho, F.M.; Resende, M.; Santos, R.C.F.; et al. Survey of feline leukemia virus and feline coronaviruses in captive neotropical wild felids from Southern Brazil. J. Zoo Wildl. Med. 2009, 40, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Filoni, C.; Helfer-Hungerbuehler, A.K.; Catão-Dias, J.L.; Marques, M.C.; Torres, L.N.; Reinacher, M.; Hofmann-Lehmann, R. Putative progressive and abortive feline leukemia virus infection outcomes in captive jaguarundis (Puma yagouaroundi). Virol. J. 2017, 14, 226. [Google Scholar] [CrossRef]
- Tandon, R.; Cattori, V.; Willi, B.; Lutz, H.; Hofmann-Lehmann, R. Quantification of endogenous and exogenous feline leukemia virus sequences by real-time PCR assays. Vet. Immunol. Immunopathol. 2008, 123, 129–133. [Google Scholar] [CrossRef]
- Jarrett, O.; Hardy, W.D., Jr.; Golder, M.C.; Hay, D. The frequency of occurrence of feline leukaemia virus subgroups in cats. Int. J. Cancer 1978, 21, 334–337. [Google Scholar] [CrossRef]
- Neil, J.; Fulton, R.; Rigby, M.; Stewart, M. Feline leukaemia virus: Generation of pathogenic and oncogenic variants. In Retroviral Insertion and Oncogene Activation; Springer: Berlin/Heidelberg, Germany, 1991; pp. 67–93. [Google Scholar] [CrossRef]
- Erbeck, K.; Gagne, R.B.; Kraberger, S.; Chiu, E.S.; Roelke-Parker, M.; VandeWoude, S. Feline leukemia virus (FeLV) endogenous and exogenous recombination events result in multiple FeLV-B subtypes during natural infection. J. Virol. 2021, 95, e0035321. [Google Scholar] [CrossRef]
- Mackey, L.; Jarrett, W.; Jarrett, O.; Laird, H. Anemia associated with feline leukemia virus infection in cats. J. Natl. Cancer Inst. 1975, 54, 209–217. [Google Scholar] [CrossRef]
- Overbaugh, J.; Riedel, N.; Hoover, E.A.; Mullins, J.I. Transduction of endogenous envelope genes by feline leukaemia virus in vitro. Nature 1988, 332, 731–734. [Google Scholar] [CrossRef]
- Stewart, M.A.; Warnock, M.; Wheeler, A.; Wilkie, N.; Mullins, J.I.; Onions, D.E.; Neil, J.C. Nucleotide sequences of a feline leukemia virus subgroup A envelope gene and long terminal repeat and evidence for the recombinational origin of subgroup B viruses. J. Virol. 1986, 58, 825–834. [Google Scholar] [CrossRef] [PubMed]
- Miyake, A.; Watanabe, S.; Hiratsuka, T.; Ito, J.; Ngo, M.H.; Makundi, I.; Kawasaki, J.; Endo, Y.; Tsujimoto, H.; Nishigaki, K.; et al. Novel feline leukemia virus interference group based on the env gene. J. Virol. 2016, 90, 4832–4837. [Google Scholar] [CrossRef] [PubMed]
- Jarrett, O.; Russell, P.H. Differential growth and transmission in cats of feline leukaemia viruses of subgroups A and B. Int. J. Cancer 1978, 21, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Hofmann-Lehmann, R.; Hartmann, K. Feline leukaemia virus infection: A practical approach to diagnosis. J. Feline Med. Surg. 2020, 22, 831–846. [Google Scholar] [CrossRef]
- Major, A.; Cattori, V.; Boenzli, E.; Riond, B.; Ossent, P.; Meli, M.L.; Hofmann-Lehmann, R.; Lutz, H. Exposure of cats to low doses of FeLV: Seroconversion as the sole parameter of infection. Vet. Res. 2010, 41, 17. [Google Scholar] [CrossRef]
- Flynn, J.N.; Hanlon, L.; Jarrett, O. Feline leukaemia virus: Protective immunity is mediated by virus-specific cytotoxic T lymphocytes. Immunology 2000, 101, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Flynn, J.N.; Dunham, S.P.; Watson, V.; Jarrett, O. Longitudinal analysis of feline leukemia virus-specific cytotoxic T lymphocytes: Correlation with recovery from infection. J. Virol. 2002, 76, 2306–2315. [Google Scholar] [CrossRef]
- Hofmann-Lehmann, R.; Tandon, R.; Boretti, F.S.; Meli, M.L.; Willi, B.; Cattori, V.; Gomes-Keller, M.A.; Ossent, P.; Golder, M.C.; Flynn, J.N.; et al. Reassessment of feline leukaemia virus (FeLV) vaccines with novel sensitive molecular assays. Vaccine 2006, 24, 1087–1094. [Google Scholar] [CrossRef]
- Lutz, H.; Pedersen, N.C.; Theilen, G.H. Course of feline leukemia virus infection and its detection by enzyme-linked immunosorbent assay and monoclonal antibodies. Am. J. Vet. Res. 1983, 44, 2054–2059. [Google Scholar]
- Hartmann, K.; Hofmann-Lehmann, R. What’s new in feline leukemia virus infection. Vet. Clin. N. Am. Small Anim. Pract. 2020, 50, 1013–1036. [Google Scholar] [CrossRef]
- Jarrett, O.; Golder, M.; Stewart, M. Detection of transient and persistent feline leukaemia virus infections. Vet. Rec. 1982, 110, 225–228. [Google Scholar] [CrossRef]
- Miyazawa, T.; Jarrett, O. Feline leukaemia virus proviral DNA detected by polymerase chain reaction in antigenaemic but non-viraemic (‘discordant’) cats. Arch. Virol. 1997, 142, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Beall, M.J.; Buch, J.; Clark, G.; Estrada, M.; Rakitin, A.; Hamman, N.T.; Frenden, M.K.; Jefferson, E.P.; Amirian, E.S.; Levy, J.K. Feline leukemia virus p27 antigen concentration and proviral DNA load are associated with survival in naturally infected cats. Viruses 2021, 13, 302. [Google Scholar] [CrossRef]
- Lutz, H.; Addie, D.; Belak, S.; Boucraut-Baralon, C.; Egberink, H.; Frymus, T.; Gruffydd-Jones, T.; Hartmann, K.; Hosie, M.J.; Lloret, A.; et al. Feline leukaemia: ABCD guidelines on prevention and management. J. Feline Med. Surg. 2009, 11, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Little, S.; Levy, J.; Hartmann, K.; Hofmann-Lehmann, R.; Hosie, M.; Olah, G.; Denis, K.S. 2020 AAFP feline retrovirus testing and management guidelines. J. Feline Med. Surg. 2020, 22, 5–30. [Google Scholar] [CrossRef]
- Hartmann, K. Clinical aspects of feline retroviruses: A review. Viruses 2012, 4, 2684–2710. [Google Scholar] [CrossRef] [PubMed]
- Hardy, W.D.; Hess, P.W.; MacEwen, E.G.; McClelland, A.J.; Zuckerman, E.E.; Essex, M.; Cotter, S.M.; Jarrett, O. Biology of feline leukemia virus in the natural environment. Cancer Res. 1976, 36 Pt 2, 582–588. [Google Scholar]
- Helfer-Hungerbuehler, A.K.; Widmer, S.; Kessler, Y.; Riond, B.; Boretti, F.S.; Grest, P.; Lutz, H.; Hofmann-Lehmann, R. Long-term follow up of feline leukemia virus infection and characterization of viral RNA loads using molecular methods in tissues of cats with different infection outcomes. Virus Res. 2015, 197, 137–150. [Google Scholar] [CrossRef]
- Shelton, G.H.; Grant, C.K.; Cotter, S.M.; Gardner, M.B.; Hardy, W.D., Jr.; DiGiacomo, R.F. Feline immunodeficiency virus and feline leukemia virus infections and their relationships to lymphoid malignancies in cats: A retrospective study (1968–1988). J. Acquir. Immune Defic. Syndr. 1990, 3, 623–630. [Google Scholar]
- Jackson, M.; Haines, D.; Meric, S.; Misra, V. Feline leukemia virus detection by immunohistochemistry and polymerase chain reaction in formalin-fixed, paraffin-embedded tumor tissue from cats with lymphosarcoma. Can. J. Vet. Res. 1993, 57, 269. [Google Scholar]
- Gabor, L.; Jackson, M.; Trask, B.; Malik, R.; Canfield, P. Feline leukaemia virus status of Australian cats with lymphosarcoma. Aust. Vet. J. 2001, 79, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Weiss, A.T.A.; Klopfleisch, R.; Gruber, A.D. Prevalence of feline leukaemia provirus DNA in feline lymphomas. J. Feline Med. Surg. 2010, 12, 929–935. [Google Scholar] [CrossRef] [PubMed]
- McLuckie, A.J.; Barrs, V.R.; Lindsay, S.; Aghazadeh, M.; Sangster, C.; Beatty, J.A. Molecular diagnosis of Felis catus gammaherpesvirus 1 (FcaGHV1) infection in cats of known retrovirus status with and without lymphoma. Viruses 2018, 10, 128. [Google Scholar] [CrossRef] [Green Version]
- Jackson, M.L.; Wood, S.L.; Misra, V.; Haines, D.M. Immunohistochemical identification of B and T lymphocytes in formalin-fixed, paraffin-embedded feline lymphosarcomas: Relation to feline leukemia virus status, tumor site, and patient age. Can. J. Vet. Res. 1996, 60, 199. [Google Scholar] [PubMed]
- Hartmann, K.; Griessmayr, P.; Schulz, B.; Greene, C.E.; Vidyashankar, A.N.; Jarrett, O.; Egberink, H.F. Quality of different in-clinic test systems for feline immunodeficiency virus and feline leukaemia virus infection. J. Feline Med. Surg. 2007, 9, 439–445. [Google Scholar] [CrossRef]
- Studer, N.; Lutz, H.; Saegerman, C.; Gönczi, E.; Meli, M.L.; Boo, G.; Hartmann, K.; Hosie, M.J.; Moestl, K.; Tasker, S.; et al. Pan-European study on the prevalence of the feline leukaemia virus infection—Reported by the European Advisory Board on Cat Diseases (ABCD Europe). Viruses 2019, 11, 993. [Google Scholar] [CrossRef]
- Jarrett, O.; Golder, M.; Weijer, K. A comparison of three methods of feline leukaemia virus diagnosis. Vet. Rec. 1982, 110, 325–328. [Google Scholar] [CrossRef]
- Gomes-Keller, M.A.; Gonczi, E.; Tandon, R.; Riondato, F.; Hofmann-Lehmann, R.; Meli, M.L.; Lutz, H. Detection of feline leukemia virus RNA in saliva from naturally infected cats and correlation of PCR results with those of current diagnostic methods. J. Clin. Microbiol. 2006, 44, 916–922. [Google Scholar] [CrossRef]
- Gomes-Keller, M.A.; Tandon, R.; Gonczi, E.; Meli, M.L.; Hofmann-Lehmann, R.; Lutz, H. Shedding of feline leukemia virus RNA in saliva is a consistent feature in viremic cats. Vet. Microbiol. 2006, 112, 11–21. [Google Scholar] [CrossRef]
- Stephenson, J.R.; Khan, A.S.; Sliski, A.H.; Essex, M. Feline oncornavirus-associated cell membrane antigen: Evidence for an immunologically crossreactive feline sarcoma virus-coded protein. Proc. Natl. Acad. Sci. USA 1977, 74, 5608–5612. [Google Scholar] [CrossRef]
- Parr, Y.A.; Beall, M.J.; Levy, J.K.; McDonald, M.; Hamman, N.T.; Willett, B.J.; Hosie, M.J. Measuring the humoral immune response in cats exposed to feline leukaemia virus. Viruses 2021, 13, 428. [Google Scholar] [CrossRef] [PubMed]
- Hofmann-Lehmann, R.; Cattori, V.; Tandon, R.; Boretti, F.S.; Meli, M.L.; Riond, B.; Pepin, A.C.; Willi, B.; Ossent, P.; Lutz, H. Vaccination against the feline leukaemia virus: Outcome and response categories and long-term follow-up. Vaccine 2007, 25, 5531–5539. [Google Scholar] [CrossRef] [PubMed]
- Hofmann-Lehmann, R.; Huder, J.B.; Gruber, S.; Boretti, F.; Sigrist, B.; Lutz, H. Feline leukaemia provirus load during the course of experimental infection and in naturally infected cats. J. Gen. Virol. 2001, 82, 1589–1596. [Google Scholar] [CrossRef]
- Torres, A.N.; Mathiason, C.K.; Hoover, E.A. Re-examination of feline leukemia virus: Host relationships using real-time PCR. Virology 2005, 332, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Gomes-Keller, M.A.; Gönczi, E.; Grenacher, B.; Tandon, R.; Hofman-Lehmann, R.; Lutz, H. Fecal shedding of infectious feline leukemia virus and its nucleic acids: A transmission potential. Vet. Microbiol. 2009, 134, 208–217. [Google Scholar] [CrossRef]
- Westman, M.; Norris, J.; Malik, R.; Hofmann-Lehmann, R.; Harvey, A.; McLuckie, A.; Perkins, M.; Schofield, D.; Marcus, A.; McDonald, M.; et al. The diagnosis of feline leukaemia virus (FeLV) infection in owned and group-housed rescue cats in Australia. Viruses 2019, 11, 503. [Google Scholar] [CrossRef]
- Lutz, H.; Pedersen, N.; Higgins, J.; Hübscher, U.; Troy, F.A.; Theilen, G.H. Humoral immune reactivity to feline leukemia virus and associated antigens in cats naturally infected with feline leukemia virus. Cancer Res. 1980, 40, 3642–3651. [Google Scholar] [PubMed]
- Boenzli, E.; Hadorn, M.; Hartnack, S.; Huder, J.; Hofmann-Lehmann, R.; Lutz, H. Detection of antibodies to the feline leukemia virus (FeLV) transmembrane protein p15E: An alternative approach for serological FeLV detection based on antibodies to p15E. J. Clin. Microbiol. 2014, 52, 2046–2052. [Google Scholar] [CrossRef]
- Langhammer, S.; Hubner, J.; Kurth, R.; Denner, J. Antibodies neutralizing feline leukaemia virus (FeLV) in cats immunized with the transmembrane envelope protein p15E. Immunology 2006, 117, 229–237. [Google Scholar] [CrossRef]
- Nesina, S.; Helfer-Hungerbuehler, A.K.; Riond, B.; Boretti, F.S.; Willi, B.; Meli, M.L.; Grest, P.; Hofmann-Lehmann, R. Retroviral DNA—The silent winner: Blood transfusion containing latent feline leukemia provirus causes infection and disease in naive recipient cats. Retrovirology 2015, 12, 105. [Google Scholar] [CrossRef]
- Pennisi, M.G.; Hartmann, K.; Addie, D.D.; Lutz, H.; Gruffydd-Jones, T.; Boucraut-Baralon, C.; Egberink, H.; Frymus, T.; Horzinek, M.C.; Hosie, M.J.; et al. Blood transfusion in cats: ABCD guidelines for minimising risks of infectious iatrogenic complications. J. Feline Med. Surg. 2015, 17, 588–593. [Google Scholar] [CrossRef] [PubMed]
- Stone, A.E.; Brummet, G.O.; Carozza, E.M.; Kass, P.H.; Petersen, E.P.; Sykes, J.; Westman, M.E. 2020 AAHA/AAFP Feline Vaccination Guidelines. J. Feline Med. Surg. 2020, 22, 813–830. [Google Scholar] [CrossRef] [PubMed]
- Westman, M.E.; Malik, R.; Hall, E.; Harris, M.; Norris, J.M. The protective rate of the feline immunodeficiency virus vaccine: An Australian field study. Vaccine 2016, 34, 4752–4758. [Google Scholar] [CrossRef] [PubMed]
- Westman, M.E.; Malik, R.; Norris, J.M. Diagnosing feline immunodeficiency virus (FIV) and feline leukaemia virus (FeLV) infection: An update for clinicians. Aust. Vet. J. 2019, 97, 47–55. [Google Scholar] [CrossRef]
- Lutz, H.; Pedersen, N.C.; Durbin, R.; Theilen, G.H. Monoclonal antibodies to three epitopic regions of feline leukemia virus p27 and their use in enzyme-linked immunosorbent assay of p27. J. Immunol. Methods 1983, 56, 209–220. [Google Scholar] [CrossRef]
- Westman, M.E.; Malik, R.; Hall, E.; Sheehy, P.A.; Norris, J.M. Comparison of three feline leukaemia virus (FeLV) point-of-care antigen test kits using blood and saliva. Comp. Immunol. Microbiol. Infect. Dis. 2017, 50, 88–96. [Google Scholar] [CrossRef]
- Tandon, R.; Cattori, V.; Gomes-Keller, M.A.; Meli, M.L.; Golder, M.C.; Lutz, H.; Hofmann-Lehmann, R. Quantitation of feline leukaemia virus viral and proviral loads by TaqMan real-time polymerase chain reaction. J. Virol. Methods 2005, 130, 124–132. [Google Scholar] [CrossRef]
- Jarrett, O.; Ganière, J.-P. Comparative studies of the efficacy of a recombinant feline leukaemia virus vaccine. Vet. Rec. 1996, 138, 7–11. [Google Scholar] [CrossRef]
- Westman, M.E.; Malik, R.; Hall, E.; Sheehy, P.A.; Norris, J.M. Determining the feline immunodeficiency virus (FIV) status of FIV-vaccinated cats using point-of-care antibody kits. Comp. Immunol. Microbiol. Infect. Dis. 2015, 42, 43–52. [Google Scholar] [CrossRef]
- Westman, M.; Coggins, S.; van Dorsselaer, M.; Norris, J.; Squires, R.; Thompson, M.; Malik, R. Feline immunodeficiency virus (FIV) infection in domestic pet cats in Australia and New Zealand: Guidelines for diagnosis, prevention and management. Aust. Vet. J. 2022, 100, 345–359. [Google Scholar] [CrossRef]
- Helfer-Hungerbuehler, A.K.; Widmer, S.; Hofmann-Lehmann, R. GAPDH pseudogenes and the quantification of feline genomic DNA equivalents. Mol. Biol. Int. 2013, 2013, 587680. [Google Scholar] [CrossRef] [PubMed]
- Englert, T.; Lutz, H.; Sauter-Louis, C.; Hartmann, K. Survey of the feline leukemia virus infection status of cats in Southern Germany. J. Feline Med. Surg. 2012, 14, 392–398. [Google Scholar] [CrossRef]
- Lutz, H.; Arnold, P.; Hübscher, U.; Egberink, H.; Pedersen, N.; Horzinek, M.C. Specificity assessment of feline T-lymphotropic lentivirus serology. J. Vet. Med. Ser. B 1988, 35, 773–778. [Google Scholar] [CrossRef] [PubMed]
- Calzolari, M.; Young, E.; Cox, D.; Davis, D.; Lutz, H. Serological diagnosis of feline immunodeficiency virus infection using recombinant transmembrane glycoprotein. Vet. Immunol. Immunopathol. 1995, 46, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Frankenfeld, J.; Meili, T.; Meli, M.L.; Riond, B.; Helfer-Hungerbuehler, A.K.; Bönzli, E.; Pineroli, B.; Hofmann-Lehmann, R. Decreased sensitivity of the serological detection of feline immunodeficiency virus infection potentially due to imported genetic variants. Viruses 2019, 11, 697. [Google Scholar] [CrossRef]
- Horzinek, M.; Egberink, H.; Lutz, H. Use of western blot and radio immunoprecipitation for diagnosis of feline leukemia and fekine immunodeficiency virus infections. J. Am. Vet. Med. Assoc. 1991, 1339–1342. [Google Scholar]
- Hoover, E.A.; Mullins, J.I. Feline leukemia virus infection and diseases. J. Am. Vet. Med. Assoc. 1991, 199, 1287–1297. [Google Scholar]
- Chiu, E.S.; Hoover, E.A.; VandeWoude, S. A retrospective examination of feline leukemia subgroup characterization: Viral interference assays to deep sequencing. Viruses 2018, 10, 29. [Google Scholar] [CrossRef]
- Rojko, J.; Kociba, G. Pathogenesis of infection by the feline leukemia virus. J. Am. Vet. Med. Assoc. 1991, 199, 1305–1310. [Google Scholar]
- Haraguchi, S.; Good, R.A.; Day-Good, N.K. A potent immunosuppressive retroviral peptide: Cytokine patterns and signaling pathways. Immunol. Res. 2008, 41, 46–55. [Google Scholar] [CrossRef]
- Rojko, J.L.; Hoover, E.A.; Mathes, L.E.; Olsen, R.G.; Schaller, J.P. Pathogenesis of experimental feline leukemia virus infection. J. Natl. Cancer Inst. 1979, 63, 759–768. [Google Scholar] [CrossRef]
- Langhammer, S.; Fiebig, U.; Kurth, R.; Denner, J. Neutralising antibodies against the transmembrane protein of feline leukaemia virus (FeLV). Vaccine 2005, 23, 3341–3348. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.K.; Scott, H.M.; Lachtara, J.L.; Crawford, P.C. Seroprevalence of feline leukemia virus and feline immunodeficiency virus infection among cats in North America and risk factors for seropositivity. J. Am. Vet. Med. Assoc. 2006, 228, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Gleich, S.E.; Krieger, S.; Hartmann, K. Prevalence of feline immunodeficiency virus and feline leukaemia virus among client-owned cats and risk factors for infection in Germany. J. Feline Med. Surg. 2009, 11, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Chhetri, B.K.; Berke, O.; Pearl, D.L.; Bienzle, D. Comparison of risk factors for seropositivity to feline immunodeficiency virus and feline leukemia virus among cats: A case-case study. BMC Vet. Res. 2015, 11, 30. [Google Scholar] [CrossRef]
- Hosie, M.J.; Addie, D.; Belak, S.; Boucraut-Baralon, C.; Egberink, H.; Frymus, T.; Gruffydd-Jones, T.; Hartmann, K.; Lloret, A.; Lutz, H.; et al. Feline immunodeficiency: ABCD guidelines on prevention and management. J. Feline Med. Surg. 2009, 11, 575–584. [Google Scholar] [CrossRef]
- Cheang, A.; Westman, M.E.; Green, J. Evaluation of a point-of-care feline immunodeficiency virus (FIV) test kit (RapidSTATUS FIV) to determine the FIV status of FIV-vaccinated and FIV-unvaccinated pet cats in Australia. Vet. Sci. 2022, 9, 618. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| FeLV Infection Status | Results | |||
|---|---|---|---|---|
| PoC p27 Ag | Lab-ELISA p27 Ag | Proviral DNA PCR | NAb | |
| Progressive (n = 23) | + | + 1 | + | − 2 |
| Regressive (n = 23) | − | − 3 | + | + |
| Abortive (n = 32) | − | − 4 | − | + |
| FeLV-unexposed (n = 122) | − | NP | − | − |
| FeLV Infection Status | Results | ||||
|---|---|---|---|---|---|
| Lab-ELISA p27 Ag | Viral RT-PCR | Proviral DNA PCR | Lab-ELISA Anti-SU Ab | Lab-ELISA Anti-Whole Virus Ab | |
| Progressive (n = 4) | + | + | + | − | − |
| Regressive (n = 2) | − | − | + | − | ± 2 |
| Abortive (n = 6) | − | − | − | + | + |
| FeLV-unexposed (n = 158) | − | − | − | ± 1 | ± 3 |
| FeLV Infection Status | Positive Results | ||
|---|---|---|---|
| v-RetroFel®Ag PoC p27 Ag | v-RetroFel®Ab PoC p15E Ab | Lab-ELISA p15E Ab | |
| Progressive | 21 (91%) | 13 (57%) | 16 (70%) |
| (n = 23) | |||
| Regressive | 0 (0%) | 0 (0%) | 16 (70%) |
| (n = 23) | |||
| Abortive | 0 (0%) | 0 (0%) | 25 (78%) |
| (n = 32) | |||
| FeLV-unexposed | 1 (0.8%) | 12 (10%) 1 | 70 (57%) |
| (n = 122) | |||
| FIV Infection Status | v-RetroFel®FIV PoC Result | |
|---|---|---|
| Negative | Positive | |
| Uninfected | 178 | 3 |
| (n = 181) | ||
| Infected | 1 | 18 |
| (n = 19) | ||
| FeLV Infection Status | Positive Results | ||
|---|---|---|---|
| v-RetroFel®Ag PoC p27 Ag | v-RetroFel®Ab PoC p15E Ab | Lab-ELISA p15E Ab | |
| Progressive | 4 (100%) | 0 (0%) | 3 (75%) |
| (n = 4) | |||
| Regressive | 0 (0%) | 0 (0%) | 0 (0%) |
| (n = 2) | |||
| Abortive | 0 (0%) | 1 (17%) 1 | 2 (33%) |
| (n = 6) | |||
| FeLV-unexposed | 0 (0%) | 10 (6%) 2 | 13 (8%) 3 |
| (n = 158) | |||
| FIV Infection Status | v-RetroFel®FIV PoC Result | |
|---|---|---|
| Negative | Positive | |
| Uninfected 1 | 160 | 0 |
| (n = 160) | ||
| Infected | 7 | 3 |
| (n = 10) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Westman, M.E.; Giselbrecht, J.; Norris, J.M.; Malik, R.; Green, J.; Burton-Bradley, E.; Cheang, A.; Meili, T.; Meli, M.L.; Hartmann, K.; et al. Field Performance of a Rapid Test to Detect Progressive, Regressive, and Abortive Feline Leukemia Virus Infections in Domestic Cats in Australia and Germany. Viruses 2023, 15, 491. https://0-doi-org.brum.beds.ac.uk/10.3390/v15020491
Westman ME, Giselbrecht J, Norris JM, Malik R, Green J, Burton-Bradley E, Cheang A, Meili T, Meli ML, Hartmann K, et al. Field Performance of a Rapid Test to Detect Progressive, Regressive, and Abortive Feline Leukemia Virus Infections in Domestic Cats in Australia and Germany. Viruses. 2023; 15(2):491. https://0-doi-org.brum.beds.ac.uk/10.3390/v15020491
Chicago/Turabian StyleWestman, Mark E., Juliana Giselbrecht, Jacqueline M. Norris, Richard Malik, Jennifer Green, Elle Burton-Bradley, Ashley Cheang, Theres Meili, Marina L. Meli, Katrin Hartmann, and et al. 2023. "Field Performance of a Rapid Test to Detect Progressive, Regressive, and Abortive Feline Leukemia Virus Infections in Domestic Cats in Australia and Germany" Viruses 15, no. 2: 491. https://0-doi-org.brum.beds.ac.uk/10.3390/v15020491