
Evidence for Benefits of Early Treatment Initiation for Chronic Hepatitis B
 , , , , , and
, , , , , and
Abstract
:1. Introduction
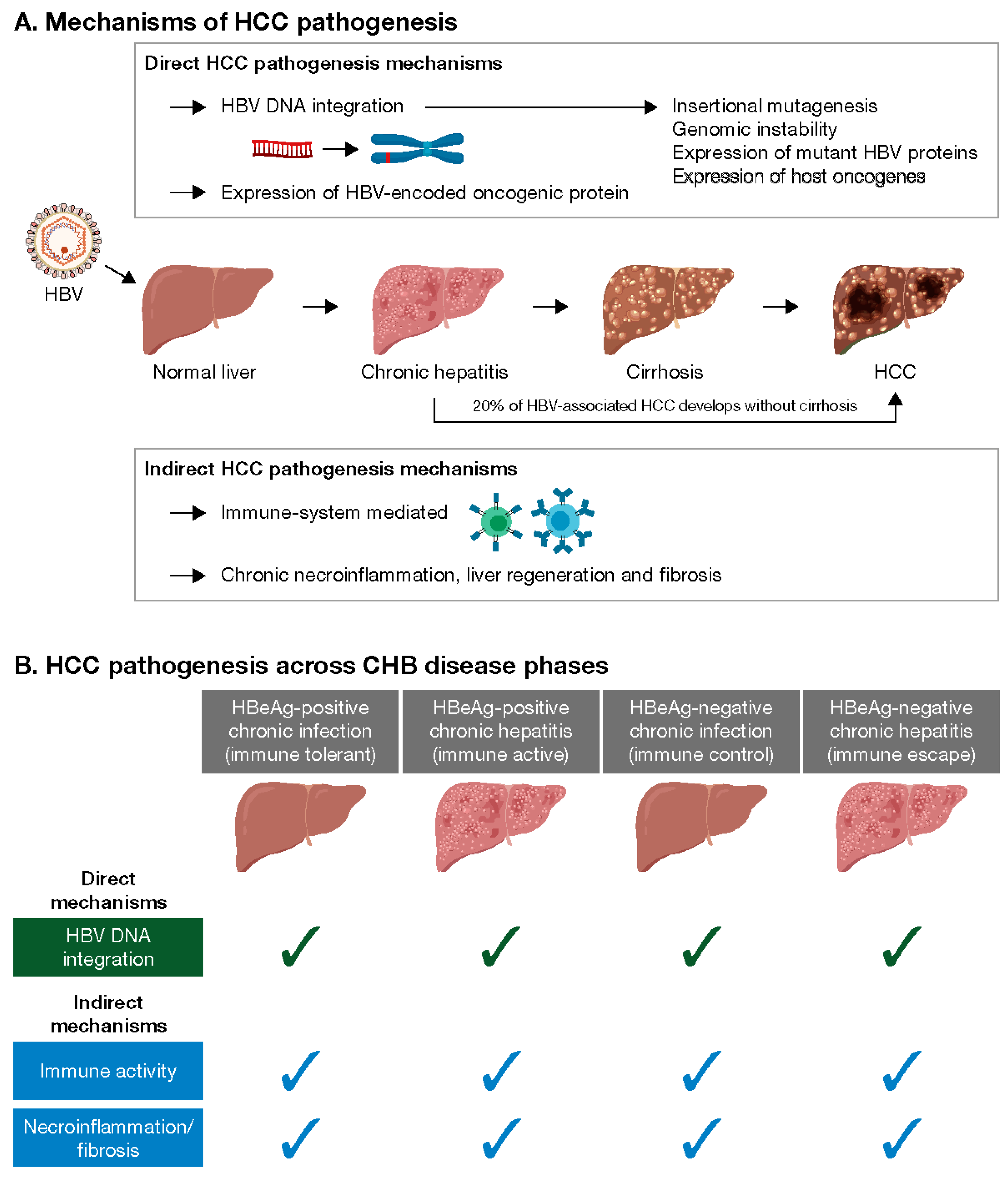
2. Mechanisms of Hepatocarcinogenesis in CHB Patients
2.1. Direct Hepatocarcinogenesis
2.2. Indirect Hepatocarcinogenesis
3. Virological Risk Factors for HCC and Impact of Antiviral Therapy
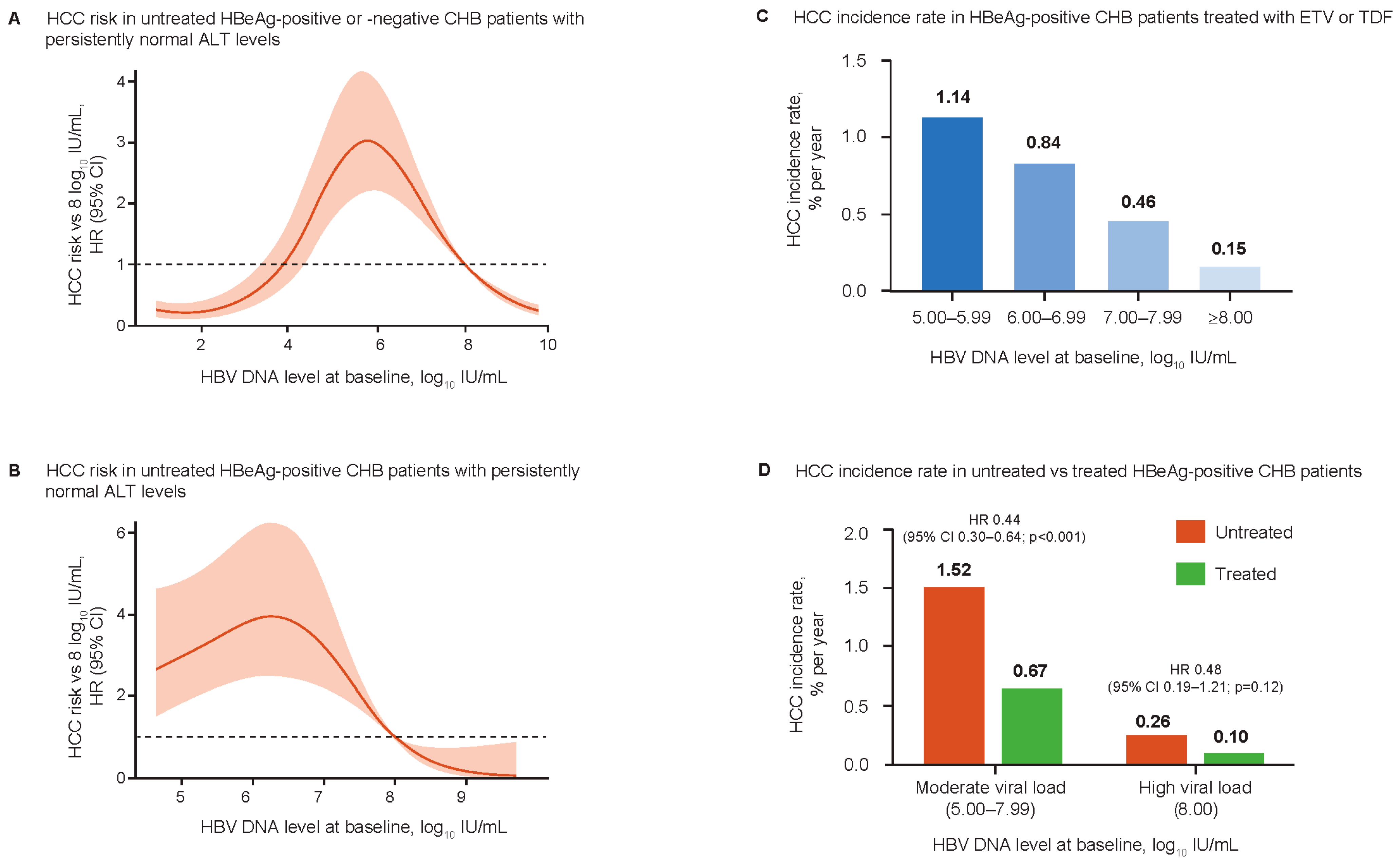
3.1. Reappraisal of the Association between Viral Load and HCC Risk
3.2. Impact of Antiviral Treatment
4. Evidence for Risk of Disease Progression across CHB Disease Phases
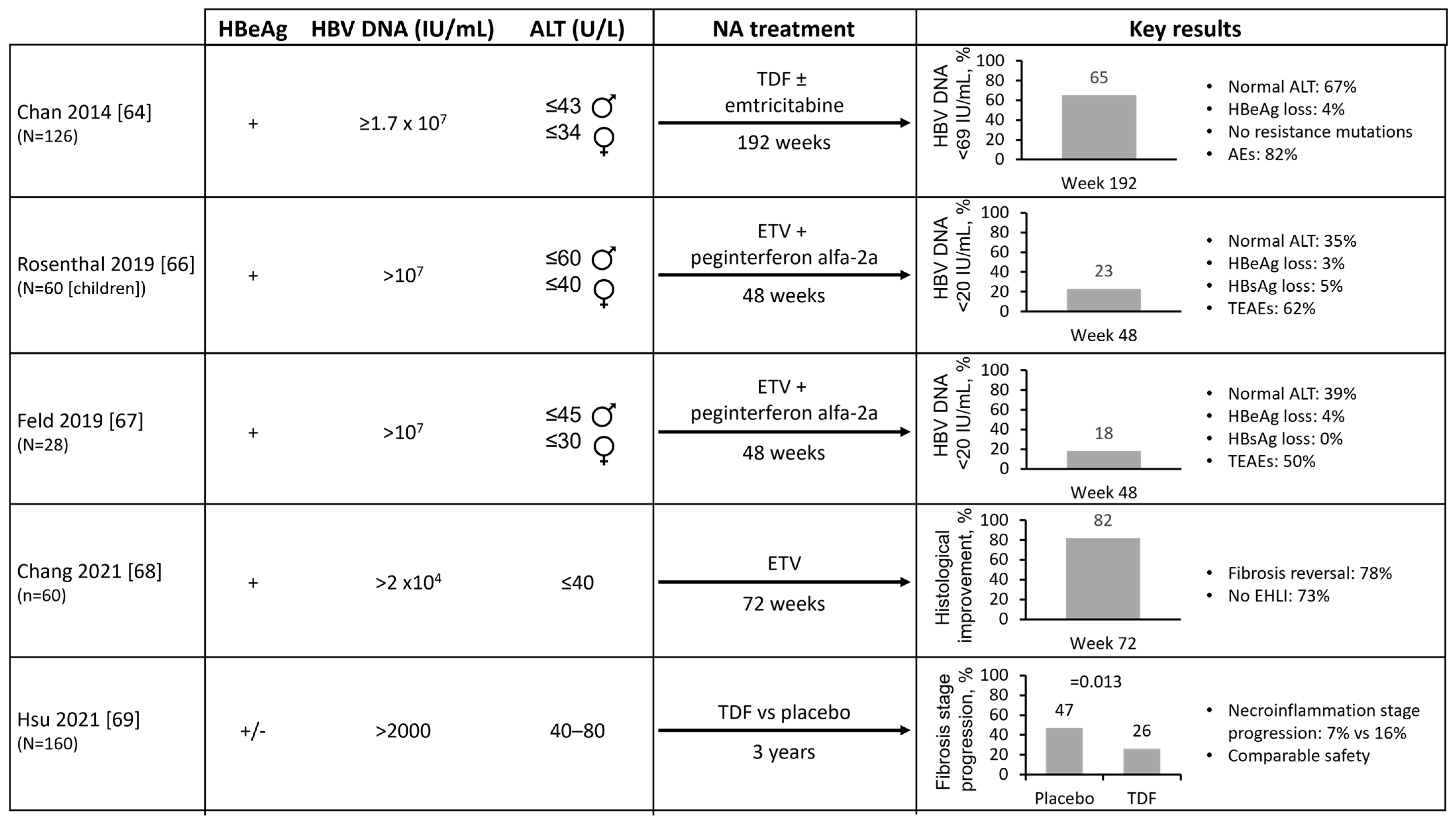
4.1. Risks in Untreated, HBeAg-Positive CHB Patients in the IT Phase (Normal ALT and High HBV DNA Levels)
4.2. Risks in Untreated, HBeAg-Negative CHB Patients in the IC Phase (Normal ALT and Low HBV DNA Levels)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author and Year | Study Type | Patient Population | HCC Risk |
|---|---|---|---|
| HBeAg-positive IT disease phase | |||
| Kim 2018 [48] | Historical cohort study | Untreated IT (n = 413): HBV DNA ≥20,000 IU/mL and ALT < 1× ULN * (mean age 38 years, median HBV DNA 108 IU/mL) vs. NA-treated IA (n = 1497): HBV DNA ≥20,000 IU/mL and ALT > 2× ULN * (mean age 40 years, median HBV DNA 108 IU/mL) | 10-year estimated cumulative HCC incidence:
|
| Kwon 2019 [49] | Multicenter cohort study | Untreated IT (n = 522): HBV DNA > 106 IU/mL and ALT < 80 U/L (mean age 36 years) vs. NA-treated IA (n = 609): HBV DNA > 106 IU/mL and ALT > 80 U/L (mean age 41 years) | 5- and 10-year cumulative HCC risk
|
| Seong 2022 [50] | Retrospective cohort study | Untreated IT (n = 651): HBV DNA > 107 IU/mL and ALT < 80 U/L (median age 36 years, median HBV DNA 108 IU/mL) | After a median follow-up of 5.2 years, 3.7% of patients developed HCC Patients who developed HCC were significantly older than those who did not (49 years vs. 35 years; p < 0.001) 5-year HCC incidence rate:
|
| Lee 2020 [51] | Multicenter, retrospective cohort study | Untreated IT (n = 946): HBV DNA > 20,000 IU/mL and ALT ≤ 40 U/L (mean age 37 years, mean HBV DNA 109 IU/mL) | 10-year cumulative HCC risk
|
| HBeAg-negative IC disease phase | |||
| Chen 2010 [52] | Retrospective analysis of REVEAL-HBV cohort | Untreated IC (n = 1932): HBV DNA < 1900 IU/mL and ALT < 45 U/L (mean age 47 years) vs. uninfected controls (n = 18,137; mean age 46 years) | Annual HCC incidence rate:
|
| Cho 2014 [56] | Retrospective study | Untreated IC (n = 1014): HBV DNA < 2000 IU/mL and ALT ≤ 40 IU/mL (mean age 52 years, mean HBV DNA 102 IU/mL) vs. NA-treated (n = 1378): HBeAg positive, HBV DNA ≥20,000 IU/mL, ALT ≥ 2× ULN † or HBeAg negative, HBV DNA ≥2000 IU/mL, ALT ≥ 2× ULN † or compensated cirrhosis, HBV DNA ≥2000 IU/mL, any ALT or decompensated cirrhosis, any ALT (mean age 48 years, mean HBV DNA 106 IU/mL) NA-treated patients with HBV DNA < 2000 IU/mL during follow-up were classified as complete responders (CR; n = 1132) | HCC incidence after median follow-up of 42 months:
|
| Seo 2020 [54] | Single-center study | Untreated IC (n = 337): HBV DNA < 2000 IU/mL and ALT ≤ 40 U/L (mean age 49 years, mean HBV DNA 309 IU/mL) | After a mean follow-up of 63 months, 4.5% of patients developed HCC Patients who developed HCC were significantly older than those who did not (62 years vs. 56 years; p = 0.035) |
| Liu 2021 [55] | Retrospective analysis of REAL-B registry | Untreated IC ‡ (n = 7977) vs. untreated IA ‡ (n = 549) | Annual HCC incidence:
|
| ‘Gray zone’ or indeterminate disease phase | |||
| Huang 2022 [57] | Retrospective cohort study | Non-cirrhotic, untreated patients (n = 3366) classified by disease phase ¶ at baseline (inactive [n = 1370], indeterminate [n = 1303], IA [n = 481], IT [n = 212]) | By up to 10 years of follow-up, of the 1303 indeterminate patients:
|
| Tseng 2021 [58] | Retrospective analysis of ERADICATE-B cohort | Patients (n = 2150) stratified by HBV DNA levels (<2000 IU/mL/2000–<20,000 IU/mL/≥20,000 IU/mL) and ALT levels (≤ULN §/1–2× ULN/≥2× ULN) | HCC risk per ‘treatment grey zone’ group compared with HBV DNA <2000 IU/mL and ALT ≤ ULN group:
|
| Choi 2019 [59] | Historical cohort study | Untreated inactive phase (n = 3572): HBV DNA < 2000 IU/mL and ALT < ULN † (mean age 47 years, median HBV DNA undetectable) Untreated replicative phase (n = 900): HBV DNA ≥2000 IU/mL and ALT < ULN † (mean age 47 years, median HBV DNA 104 IU/mL) Untreated mildly active phase (n = 396): HBV DNA ≥2000 IU/mL and ALT 1–<2× ULN † (mean age 46 years, median HBV DNA 105 IU/mL) NA-treated active phase (n = 546): HBV DNA ≥2000 IU/mL and ALT ≥ 2× ULN † (mean age 47 years, median HBV DNA 107 IU/mL) | HCC cases per 100 patient-years (95% CI):
|
4.3. Risks in Untreated ‘Gray Zone’ Patients (HBV DNA ≥2000 IU/mL and Minimally Raised Serum ALT Levels)
5. Potential Impact of Early HBV Treatment on Hepatocarcinogenesis and Clinical HBV Parameters
5.1. Potential Impact of HBV Treatment on HBV DNA Integration
5.2. Potential Impact of Early HBV Treatment on Clinical HBV Parameters
5.3. Impact of Treatment on ‘Gray Zone’ Patients
5.4. Impact of Early HBV Treatment in Patients with HBV/HIV Co-Infection
6. Cost Effectiveness of Expanded HBV Treatment Strategies
| Author and Year | Model Population and Selected Input Parameters | Treatment Strategies | Key Results |
|---|---|---|---|
| Zhang 2023 [74] | Chinese model of 136 scenarios based on cross combination of:
|
|
|
| Lepers 2020 [76] | CHB patients in French ANRS CO22 HEPATHER cohort
|
|
|
| Razavi-Shearer 2021 [77] | U.S. model including historical and future impact of immigration using 164 country-specific disease burden and transmission models |
|
|
| Razavi 2020 [78] | Economic impact analysis |
|
|
| Kim 2021 [79] | Hypothetical CHB patients
|
|
|
| Crossan 2016 [80] | Hypothetical CHB patients with suspected fibrosis (n = 1000) Separate Markov models constructed for HBeAg-positive (starting age 31 years) and -negative (starting age 40 years) patients Transition probabilities:
|
|
|
| Shim 2016 [81] | CHB patients in Korea
|
|
|
| Lim 2021 [82] | Virtual CHB cohort based on Korean data
|
|
|
| Sanai 2020 [83] | CHB patients in Saudi Arabia using estimated national prevalence in 2017
|
|
|
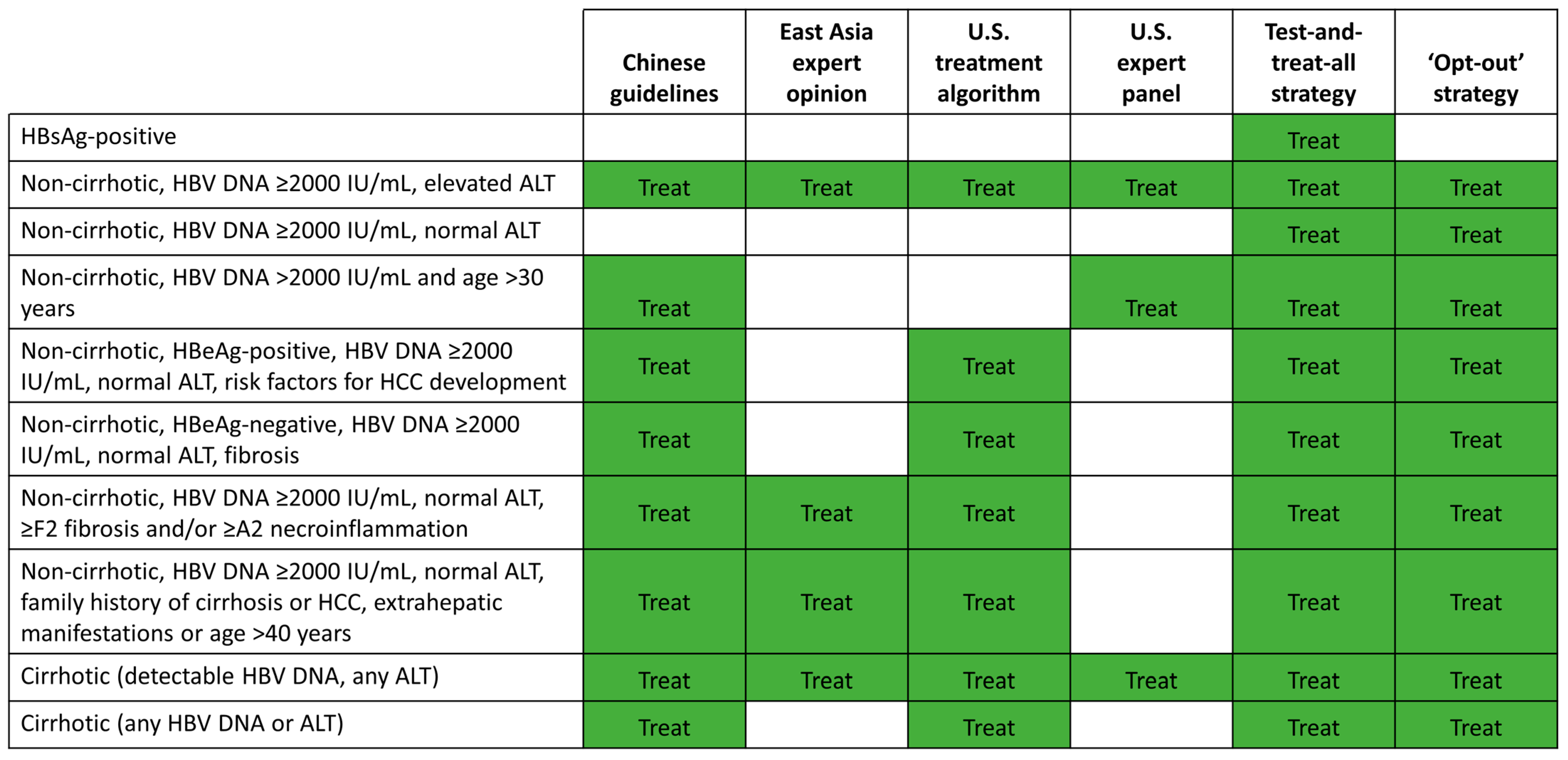
7. Potential Strategies for Expanded HBV Treatment
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Hepatitis B Fact Sheet; Published Online 27 July 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b (accessed on 3 September 2021).
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.-W.; et al. Forecasting life expectancy, years of life lost, and all-Cause and cause-Specific mortality for 250 causes of death: Reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver (EASL). EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef]
- Sarin, S.K.; Kumar, M.; Lau, G.K.; Abbas, Z.; Chan, H.L.Y.; Chen, C.J.; Chen, D.S.; Chen, H.L.; Chen, P.J.; Chien, R.N.; et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: A 2015 update. Hepatol. Int. 2016, 10, 1–98. [Google Scholar] [CrossRef]
- Lin, C.L.; Kao, J.H. Prevention of hepatitis B virus-related hepatocellular carcinoma. Hepatoma Res. 2021, 7, S303–S309. [Google Scholar] [CrossRef]
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.-M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef] [PubMed]
- Seto, W.K.; Lo, Y.R.; Pawlotsky, J.M.; Yuen, M.F. Chronic hepatitis B virus infection. Lancet 2018, 392, 2313–2324. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.B.; Wu, J.F.; Du, Y.; Cao, G.W. Cancer Evolution–Development: Experience of Hepatitis B Virus-Induced Hepatocarcinogenesis. Curr. Oncol. 2016, 23, 49–56. [Google Scholar] [CrossRef]
- Ringelhan, M.; McKeating, J.A.; Protzer, U. Viral hepatitis and liver cancer. Philos. Trans. R. Soc. B Biol. Sci. 2017, 372, 20160274. [Google Scholar] [CrossRef]
- Chemin, I.; Zoulim, F. Hepatitis B virus induced hepatocellular carcinoma. Cancer Lett. 2009, 286, 52–59. [Google Scholar] [CrossRef]
- An, P.; Xu, J.; Yu, Y.; Winkler, C.A. Host and Viral Genetic Variation in HBV-Related Hepatocellular Carcinoma. Front. Genet. 2018, 9, 261. [Google Scholar] [CrossRef]
- Ramirez, R.; van Buuren, N.; Gamelin, L.; Soulette, C.; May, L.; Han, D.; Yu, M.; Choy, R.; Cheng, G.; Bhardwaj, N.; et al. Targeted Long-Read Sequencing Reveals Comprehensive Architecture, Burden, and Transcriptional Signatures from Hepatitis B Virus-Associated Integrations and Translocations in Hepatocellular Carcinoma Cell Lines. J. Virol. 2021, 95, e0029921. [Google Scholar] [CrossRef]
- Pan, D.; Soulette, C.; Han, D.; Ramirez, R.; Van Buuren, N.; Lin, J.-T.; Tseng, C.-H.; Li, L.; Fletcher, S.; Mo, H.; et al. Decrease in the burden of integrated hepatitis B virus DNA in chronic hepatitis B patients with minimally elevated alanine aminotransferase on tenofovir disoproxil fumarate as revealed by long-read DNA-sequencing. J. Hepatol. 2022, 77, S841–S842. [Google Scholar] [CrossRef]
- The Cancer Genome Atlas Research; The Cancer Genome Atlas Research Network. Comprehensive and Integrative Genomic Characterization of Hepatocellular Carcinoma. Cell 2017, 169, 1327–1341. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.B.; Tripodi, G.; Raimondo, G.; Saitta, C.; Norkrans, G.; Pollicino, T.; Lindh, M. Integration of hepatitis B virus DNA in chronically infected patients assessed by Alu-PCR. J. Med. Virol. 2018, 90, 1568–1575. [Google Scholar] [CrossRef] [PubMed]
- Erken, R.; Loukachov, V.; van Dort, K.; Hurk, A.V.D.; Takkenberg, R.B.; de Niet, A.; Jansen, L.; Willemse, S.; Reesink, H.W.; Kootstra, N. Quantified integrated hepatitis B virus is related to viral activity in chronic hepatitis B patients. Hepatology 2022, 76, 196–206. [Google Scholar] [CrossRef]
- Svicher, V.; Salpini, R.; Piermatteo, L.; Carioti, L.; Battisti, A.; Colagrossi, L.; Scutari, R.; Surdo, M.; Cacciafesta, V.; Nuccitelli, A.; et al. Whole exome HBV DNA integration is independent of the intrahepatic HBV reservoir in HBeAg-negative chronic hepatitis B. Gut 2021, 70, 2337–2348. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.-C.; Suri, V.; Nguyen, M.H.; Huang, Y.-T.; Chen, C.-Y.; Chang, I.-W.; Tseng, C.-H.; Wu, C.-Y.; Lin, J.-T.; Pan, D.Z.; et al. Inhibition of Viral Replication Reduces Transcriptionally Active Distinct Hepatitis B Virus Integrations with Implications on Host Gene Dysregulation. Gastroenterology 2022, 162, 1160–1170. [Google Scholar] [CrossRef]
- Chow, N.; Wong, D.; Lai, C.-L.; Mak, L.-Y.; Fung, J.; Ma, H.-T.; Lei, M.-W.; Seto, W.-K.; Yuen, M.-F. Effect of Antiviral Treatment on Hepatitis B Virus Integration and Hepatocyte Clonal Expansion. Clin. Infect. Dis. 2023, 76, e801–e809. [Google Scholar] [CrossRef]
- Tu, T.; Mason, W.S.; Clouston, A.D.; Shackel, N.A.; McCaughan, G.W.; Yeh, M.M.; Schiff, E.R.; Ruszkiewicz, A.R.; Chen, J.W.; Harley, H.A.J.; et al. Clonal expansion of hepatocytes with a selective advantage occurs during all stages of chronic hepatitis B virus infection. J. Viral Hepat. 2015, 22, 737–753. [Google Scholar] [CrossRef]
- Mason, W.S.; Gill, U.S.; Litwin, S.; Zhou, Y.; Peri, S.; Pop, O.; Hong, M.L.; Naik, S.; Quaglia, A.; Bertoletti, A.; et al. HBV-DNA Integration and Clonal Hepatocyte Expansion in Chronic Hepatitis B Patients Considered Immune Tolerant. Gastroenterology 2016, 151, 986–998. [Google Scholar] [CrossRef]
- Duan, M.; Hao, J.; Cui, S.; Worthley, D.L.; Zhang, S.; Wang, Z.; Shi, J.; Liu, L.; Wang, X.; Ke, A.; et al. Diverse modes of clonal evolution in HBV-related hepatocellular carcinoma revealed by single-cell genome sequencing. Cell Res. 2018, 28, 359–373. [Google Scholar] [CrossRef] [PubMed]
- Shin, E.-C.; Sung, P.S.; Park, S.-H. Immune responses and immunopathology in acute and chronic viral hepatitis. Nat. Rev. Immunol. 2016, 16, 509–523. [Google Scholar] [CrossRef]
- Kennedy, P.T.F.; Sandalova, E.; Jo, J.; Gill, U.; Ushiro–Lumb, I.; Tan, A.T.; Naik, S.; Foster, G.R.; Bertoletti, A. Preserved T-Cell Function in Children and Young Adults with Immune-Tolerant Chronic Hepatitis B. Gastroenterology 2012, 143, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-J.; Wong, D.K.; Wahed, A.S.; Lee, W.M.; Feld, J.J.; Terrault, N.; Khalili, M.; Sterling, R.K.; Kowdley, K.V.; Bzowej, N.; et al. Hepatitis B Virus–Specific and Global T-Cell Dysfunction in Chronic Hepatitis B. Gastroenterology 2016, 150, 684–695. [Google Scholar] [CrossRef]
- van Buuren, N.; Ramirez, R.; Turner, S.; Chen, D.; Suri, V.; Aggarwal, A.; Moon, C.; Kim, S.; Kornyeyev, D.; Bui, N.; et al. Characterization of the liver immune microenvironment in liver biopsies from patients with chronic HBV infection. JHEP Rep. 2022, 4, 100388. [Google Scholar] [CrossRef]
- Yang, H.I.; Lu, S.N.; Liaw, Y.F.; You, S.L.; Sun, C.A.; Wang, L.Y.; Hsiao, C.K.; Chen, P.J.; Chen, D.S.; Chen, C.J.; et al. Hepatitis B e Antigen and the Risk of Hepatocellular Carcinoma. N. Engl. J. Med. 2002, 347, 168–174. [Google Scholar] [CrossRef]
- Zhou, T.-C.; Lai, X.; Feng, M.-H.; Tang, Y.; Zhang, L.; Wei, J. Systematic review and meta-analysis: Development of hepatocellular carcinoma in chronic hepatitis B patients with hepatitis e antigen seroconversion. J. Viral Hepat. 2018, 25, 1172–1179. [Google Scholar] [CrossRef] [PubMed]
- Wiseman, E.; Fraser, M.A.; Holden, S.; Glass, A.; Rn, B.L.K.; Heron, L.G.; Maley, M.W.; Ayres, A.; Locarnini, S.A.; Levy, M.T. Perinatal transmission of hepatitis B virus: An Australian experience. Med. J. Aust. 2009, 190, 489–492. [Google Scholar] [CrossRef]
- Seck, A.; Maylin, S.; Akbar, S.M.F.; Funk, A.L.; Bercion, R.; Mishiro, S.; Ndiaye, B.; Fontanet, A.; Vray, M.; Simon, F.; et al. Poor Sensitivity of Commercial Rapid Diagnostic Tests for Hepatitis B e Antigen in Senegal, West Africa. Am. J. Trop. Med. Hyg. 2018, 99, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-J.; Yang, H.-I.; Su, J.; Jen, C.-L.; You, S.-L.; Lu, S.-N.; Huang, G.-T.; Iloeje, U.H.; REVEAL-HBV Study Group. Risk of Hepatocellular Carcinoma Across a Biological Gradient of Serum Hepatitis B Virus DNA Level. JAMA 2006, 295, 65–73. [Google Scholar] [CrossRef]
- Iloeje, U.H.; Yang, H.I.; Su, J.; Jen, C.L.; You, S.L.; Chen, C.J. Predicting Cirrhosis Risk Based on the Level of Circulating Hepatitis B Viral Load. Gastroenterology 2006, 130, 678–686. [Google Scholar] [CrossRef]
- Iloeje, U.H.; Yang, H.I.; Jen, C.L.; Su, J.; Wang, L.; You, S.; Chen, C. Risk and Predictors of Mortality Associated with Chronic Hepatitis B Infection. Clin. Gastroenterol. Hepatol. 2007, 5, 921–931. [Google Scholar] [CrossRef]
- Kim, G.-A.; Han, S.; Choi, G.H.; Choi, J.; Lim, Y.-S. Moderate levels of serum hepatitis B virus DNA are associated with the highest risk of hepatocellular carcinoma in chronic hepatitis B patients. Aliment. Pharmacol. Ther. 2020, 51, 1169–1179. [Google Scholar] [CrossRef]
- Choi, W.-M.; Kim, G.-A.; Choi, J.; Han, S.; Lim, Y.-S. Increasing on-treatment hepatocellular carcinoma risk with decreasing baseline viral load in HBeAg-positive chronic hepatitis B. J. Clin. Investig. 2022, 132, e154833. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wang, J.; Yan, X.; Xue, R.; Zhan, J.; Jiang, S.; Geng, Y.; Liu, Y.; Mao, M.; Xia, J.; et al. Presence of Liver Inflammation in Asian Patients with Chronic Hepatitis B with Normal ALT and Detectable HBV-DNA in Absence of Liver Fibrosis. Hepatol. Commun. 2021, 6, 855–866. [Google Scholar] [CrossRef]
- Zoulim, F.; Mason, W.S. Reasons to consider earlier treatment of chronic HBV infections. Gut 2012, 61, 333–336. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.-A.; Lim, Y.-S. Editorial: Hepatitis B DNA thresholds and risk of hepatocellular carcinoma: Different number patterns in HBeAg-positive versus HBeAg-negative patients. Authors’ reply. Aliment. Pharmacol. Ther. 2020, 51, 1440–1441. [Google Scholar] [CrossRef]
- Ford, N.; Scourse, R.; Lemoine, M.; Hutin, Y.; Bulterys, M.; Shubber, Z.; Donchuk, D.; Wandeler, G. Adherence to Nucleos(t)ide Analogue Therapies for Chronic Hepatitis B Infection: A Systematic Review and Meta-Analysis. Hepatol. Commun. 2018, 2, 1160–1167. [Google Scholar] [CrossRef]
- Liu, K.; Choi, J.; Le, A.; Yip, T.C.-F.; Wong, V.W.-S.; Chan, S.; Chan, H.L.-Y.; Nguyen, M.H.; Lim, Y.-S.; Wong, G.L.-H. Tenofovir disoproxil fumarate reduces hepatocellular carcinoma, decompensation and death in chronic hepatitis B patients with cirrhosis. Aliment. Pharmacol. Ther. 2019, 50, 1037–1048. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.R.; Loomba, R.; Berg, T.; Schall, R.E.A.; Yee, L.J.; Dinh, P.V.; Flaherty, J.F.; Martins, E.B.; Therneau, T.M.; Jacobson, I.; et al. Impact of long-term tenofovir disoproxil fumarate on incidence of hepatocellular carcinoma in patients with chronic hepatitis B. Cancer 2015, 121, 3631–3638. [Google Scholar] [CrossRef] [PubMed]
- Papatheodoridis, G.V.; Idilman, R.; Dalekos, G.N.; Buti, M.; Chi, H.; van Boemmel, F.; Calleja, J.L.; Sypsa, V.; Goulis, J.; Manolakopoulos, S.; et al. The risk of hepatocellular carcinoma decreases after the first 5 years of entecavir or tenofovir in Caucasians with chronic hepatitis B. Hepatology 2017, 66, 1444–1453. [Google Scholar] [CrossRef]
- Sinn, D.H.; Kim, S.E.; Kim, B.K.; Kim, J.H.; Choi, M.S. The risk of hepatocellular carcinoma among chronic hepatitis B virus-infected patients outside current treatment criteria. J. Viral Hepat. 2019, 26, 1465–1472. [Google Scholar] [CrossRef]
- Alshuwaykh, O.; Daugherty, T.; Cheung, A.; Goel, A.; Dhanasekaran, R.; Ghaziani, T.T.; Ahmed, A.; Dronamraju, D.; Kumari, R.; Kwong, A.; et al. Incidence of hepatocellular carcinoma in chronic hepatitis B virus infection in those not meeting criteria for antiviral therapy. Hepatol. Commun. 2022, 6, 3052–3061. [Google Scholar] [CrossRef]
- Wang, C.Y.; Deng, Y.; Guo, C.; Ji, D. Nomogram for predicting significant liver injury in chronic hepatitis B patients with immune tolerance. J. Hepatol. 2021, 75, S730–S731. [Google Scholar]
- Zeng, D.-W.; Huang, Z.-X.; Lin, M.-X.; Kang, N.-L.; Lin, X.; Li, Y.-N.; Zhu, Y.-Y.; Liu, Y.-R. A novel HBsAg-based model for predicting significant liver fibrosis among Chinese patients with immune-tolerant phase chronic hepatitis B: A multicenter retrospective study. Ther. Adv. Gastroenterol. 2021, 14, 17562848211010675. [Google Scholar] [CrossRef]
- Lin, M.-H.; Li, H.-Q.; Zhu, L.; Su, H.-Y.; Peng, L.-S.; Wang, C.-Y.; He, C.-P.; Liang, X.-E.; Wang, Y. Liver Fibrosis in the Natural Course of Chronic Hepatitis B Viral Infection: A Systematic Review with Meta-Analysis. Dig. Dis. Sci. 2022, 67, 2608–2626. [Google Scholar] [CrossRef]
- Kim, G.-A.; Lim, Y.-S.; Han, S.; Choi, J.; Shim, J.H.; Kim, K.M.; Lee, H.C.; Lee, Y.S. High risk of hepatocellular carcinoma and death in patients with immune-tolerant-phase chronic hepatitis B. Gut 2018, 67, 945–952. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.H.; Lee, S.W.; Jang, J.W.; Yoo, S.H.; Song, D.S.; Kim, H.Y. Low risk of liver disease progression in untreated immune tolerant phase chronic hepatitis B patients compared to treated immune active phase patients: Multi-center cohort study up to 15 years. Hepatology 2019, 71, 574A. [Google Scholar]
- Seong, G.; Sinn, D.H.; Kang, W.; Gwak, G.-Y.; Choi, M.S.; Lee, J.H.; Koh, K.C.; Paik, S.W.; Paik, Y.-H. Age and fibrosis index for the prediction of hepatocellular carcinoma risk in patients with high hepatitis B virus DNA but normal alanine aminotransferase. Eur. J. Gastroenterol. Hepatol. 2022, 34, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.A.; Lee, H.W.; Kim, I.H.; Park, S.Y.; Sinn, D.H.; Yu, J.H.; Seo, Y.S.; Um, S.H.; Lee, J.I.; Lee, K.S.; et al. Extremely low risk of hepatocellular carcinoma development in patients with chronic hepatitis B in immune-tolerant phase. Aliment. Pharmacol. Ther. 2020, 52, 196–204. [Google Scholar] [CrossRef]
- Chen, J.D.; Yang, H.I.; Iloeje, U.H.; You, S.-L.; Lu, S.; Wang, L.; Su, J.; Sun, C.; Liaw, Y.; Chen, C. Carriers of Inactive Hepatitis B Virus Are Still at Risk for Hepatocellular Carcinoma and Liver-Related Death. Gastroenterology 2010, 138, 1747–1754. [Google Scholar] [CrossRef]
- Graf, C.; Knop, V.; Peiffer, K.H.; Dietz, J.; Berg, T.; Wedemeyer, H.; Cornberg, M.; Petersen, J.; Hueppe, D.; Sprinzl, M.; et al. Clinical outcomes in untreated European patients with chronic hepatitis B virus infection after seven years: A prospective longitudinal study (ALBATROS study). Hepatology 2019, 70, 409A–410A. [Google Scholar]
- Seo, S.I.; Kim, H.S.; Yang, B.K.; Kang, J.G.; Shin, W.G.; Lee, J.H.; Kim, H.Y.; Jang, M.K. Predictive factors for risk of hepatocellular carcinoma in immune inactive chronic hepatitis B. Clin. Res. Hepatol. Gastroenterol. 2020, 44, 711–717. [Google Scholar] [CrossRef]
- Liu, M.; Tseng, T.-C.; Jun, D.W.; Yeh, M.-L.; Trinh, H.; Wong, G.L.H.; Chen, C.-H.; Peng, C.-Y.; Kim, S.E.; Oh, H.; et al. Transition rates to cirrhosis and liver cancer by age, gender, disease and treatment status in Asian chronic hepatitis B patients. Hepatol. Int. 2021, 15, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.-Y.; Paik, Y.-H.; Sohn, W.; Cho, H.C.; Gwak, G.-Y.; Choi, M.S.; Lee, J.H.; Koh, K.C.; Paik, S.W.; Yoo, B.C. Patients with chronic hepatitis B treated with oral antiviral therapy retain a higher risk for HCC compared with patients with inactive stage disease. Gut 2014, 63, 1943–1950. [Google Scholar] [CrossRef]
- Huang, D.Q.; Li, X.; Le, M.H.; Le, A.K.; Yeo, Y.H.; Trinh, H.N.; Zhang, J.; Li, J.; Wong, C.; Wong, C.; et al. Natural History and Hepatocellular Carcinoma Risk in Untreated Chronic Hepatitis B Patients with Indeterminate Phase. Clin. Gastroenterol. Hepatol. 2022, 20, 1803–1812.e5. [Google Scholar] [CrossRef] [PubMed]
- Tseng, T.-C.; Hosaka, T.; Liu, C.-J.; Suzuki, F.; Hong, C.-M.; Kumada, H.; Yang, W.-T.; Hsu, C.-Y.; Su, T.-H.; Yang, H.-C.; et al. Hepatitis B Core-Related Antigen Stratifies the Risk of Liver Cancer in HBeAg-Negative Patients with Indeterminate Phase. Am. J. Gastroenterol. 2022, 117, 748–757. [Google Scholar] [CrossRef]
- Choi, G.H.; Kim, G.-A.; Choi, J.; Han, S.; Lim, Y.-S. High risk of clinical events in untreated HBeAg-negative chronic hepatitis B patients with high viral load and no significant ALT elevation. Aliment. Pharmacol. Ther. 2019, 50, 215–226. [Google Scholar] [CrossRef]
- McGill, M.R. The past and present of serum aminotransferases and the future of liver injury biomarkers. EXCLI J. 2016, 15, 817–828. [Google Scholar] [CrossRef] [PubMed]
- Kao, J.-H.; Hu, T.-H.; Jia, J.; Kurosaki, M.; Lim, Y.-S.; Lin, H.-C.; Sinn, D.H.; Tanaka, Y.; Wong, V.W.-S.; Yuen, M.-F. East Asia expert opinion on treatment initiation for chronic hepatitis B. Aliment. Pharmacol. Ther. 2020, 52, 1540–1550. [Google Scholar] [CrossRef]
- Tu, T.; Budzinska, M.A.; Shackel, N.A.; Urban, S. HBV-DNA Integration: Molecular Mechanisms and Clinical Implications. Viruses 2017, 9, 75. [Google Scholar] [CrossRef]
- Lok, A.S.F.; McMahon, B.J.; Brown, R.S., Jr.; Wong, J.B.; Ahmed, A.T.; Farah, W.; Almasri, J.; Alahdab, F.; Benkhadra, K.; Mouchli, M.A.; et al. Antiviral therapy for chronic hepatitis B viral infection in adults: A systematic review and meta-analysis. Hepatology 2016, 63, 284–306. [Google Scholar] [CrossRef]
- Chan, H.L.Y.; Chan, C.K.; Hui, A.J.; Chan, S.; Poordad, F.; Chang, T.-T.; Mathurin, P.; Flaherty, J.F.; Lin, L.; Corsa, A.; et al. Effects of Tenofovir Disoproxil Fumarate in Hepatitis B e Antigen-Positive Patients with Normal Levels of Alanine Aminotransferase and High Levels of Hepatitis B Virus DNA. Gastroenterology 2014, 146, 1240–1248. [Google Scholar] [CrossRef]
- Chan, H.L.Y.; Lim, Y.S.; Hou, J.; Hui, A.J.; Seto, W.K.; Chang, T.T.; Chuang, W.L.; Janssen, H.L.; Fung, S.K.; Ning, Q.; et al. Impact of long-term oral antiviral (OAV) treatment on hepatocellular carcinoma (HCC) risk in immune-tolerant and immune-active chronic hepatitis B patients (CHB) utilizing aMAP, a recently validated risk prediction tool. Hepatology 2021, 74, 487A–488A. [Google Scholar]
- Rosenthal, P.; Ling, S.C.; Belle, S.H.; Murray, K.F.; Rodriguez-Baez, N.; Schwarzenberg, S.J.; Teckman, J.; Lin, H.S.; Schwarz, K.B.; Hepatitis B Research Network (HBRN). Combination of Entecavir/Peginterferon Alfa-2a in Children With Hepatitis B e Antigen–Positive Immune Tolerant Chronic Hepatitis B Virus Infection. Hepatology 2019, 69, 2326–2337. [Google Scholar] [CrossRef]
- Feld, J.J.; Terrault, N.A.; Lin, H.S.; Belle, S.H.; Chung, R.T.; Tsai, N.; Khalili, M.; Perrillo, R.; Cooper, S.L.; Ghany, M.G.; et al. Entecavir and Peginterferon Alfa-2a in Adults With Hepatitis B e Antigen–Positive Immune-Tolerant Chronic Hepatitis B Virus Infection. Hepatology 2019, 69, 2338–2348. [Google Scholar] [CrossRef] [PubMed]
- Chang, X.; Wang, J.; Chen, Y.; Long, Q.; Song, L.; Li, Q.; Liu, H.; Shang, Q.; Yu, Z.; Jiang, L.; et al. A novel nomogram to predict evident histological liver injury in patients with HBeAg-positive chronic hepatitis B virus infection. Ebiomedicine 2021, 67, 103389. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.-C.; Chen, C.-Y.; Chang, I.-W.; Chang, C.-Y.; Wu, C.-Y.; Lee, T.-Y.; Wu, M.-S.; Bair, M.-J.; Chen, J.-J.; Chen, C.-C.; et al. Once-daily tenofovir disoproxil fumarate in treatment-naive Taiwanese patients with chronic hepatitis B and minimally raised alanine aminotransferase (TORCH-B): A multicentre, double-blind, placebo-controlled, parallel-group, randomised trial. Lancet Infect. Dis. 2021, 21, 823–833. [Google Scholar] [CrossRef] [PubMed]
- Leoni, M.C.; Ustianowski, A.; Farooq, H.; Arends, J.E. HIV, HCV and HBV: A Review of Parallels and Differences. Infect. Dis. Ther. 2018, 7, 407–419. [Google Scholar] [CrossRef]
- Wandeler, G.; Mauron, E.; Atkinson, A.; Dufour, J.-F.; Kraus, D.; Reiss, P.; Peters, L.; Dabis, F.; Fehr, J.; Bernasconi, E.; et al. Incidence of hepatocellular carcinoma in HIV/HBV-coinfected patients on tenofovir therapy: Relevance for screening strategies. J. Hepatol. 2019, 71, 274–280. [Google Scholar] [CrossRef]
- Lui, G.; Yip, T.; Yuen, B.; Sze, A.; Hui, Y.-T.; Tse, Y.-K.; Wong, V.; Wong, G. 358. HIV Infection and the Risk of Hepatocellular Carcinoma in Patients with Hepatitis B Virus (HBV) Co-infection: A Propensity Score-matched Cohort Study. Open Forum Infect. Dis. 2019, 6 (Suppl. 2), S188. [Google Scholar] [CrossRef]
- Naggie, S.; Telep, L.; McQuaid, T.; Ramroth, H.; Gaggar, A.; Flaherty, J.F.; Chokkalingam, A.P.; Sulkowski, M.S. Risk of HCC in patients with HBV infection with and without HIV co-infection: A US administrative claims analysis. Hepatology 2020, 72, 494A. [Google Scholar]
- Zhang, S.; Wang, C.; Liu, B.; Lu, Q.-B.; Shang, J.; Zhou, Y.; Jia, J.; Xu, X.; Rao, H.; Han, B.; et al. Cost-effectiveness of expanded antiviral treatment for chronic hepatitis B virus infection in China: An economic evaluation. Lancet Reg. Health-West. Pac. 2023, 100738. [Google Scholar] [CrossRef]
- Chinese Society of Hepatology; Chinese Medical Association; Chinese Society of Infectious Diseases. Guidelines for the prevention and treatment of chronic hepatitis B (version 2022). Chin. J. Hepatol. 2022, 30, 1309–1331. [Google Scholar] [CrossRef]
- Lepers, C.; Fontaine, H.; Carrat, F.; Mathurin, P.; Pol, S.; Zoulim, F.; Yazdanpanah, Y.; Deuffic-Burban, S. Cost-effectiveness of scaling-up treatment with nucleoside analogue (NA) for chronic HBV infection: Towards a simplification of recommendations? (ANRS study). J. Hepatol. 2020, 73, S797–S798. [Google Scholar] [CrossRef]
- Razavi-Shearer, D.; Estes, C.; Gamkrelidze, I.; Razavi, H. Cost-effectiveness analysis of treating all HBsAg+ individuals in the United States. Hepatology 2021, 74, 22A. [Google Scholar]
- Razavi, H.; Sadirova, S.; Bakieva, S.; Razavi-Shearer, K.; Dunn, R.; Musabaev, E. The case for testing and treating all HBV patients. J. Hepatol. 2020, 73, S807. [Google Scholar] [CrossRef]
- Kim, H.-L.; Kim, G.-A.; Park, J.-A.; Kang, H.-R.; Lee, E.-K.; Lim, Y.-S. Cost-effectiveness of antiviral treatment in adult patients with immune-tolerant phase chronic hepatitis B. Gut 2021, 70, 2172–2182. [Google Scholar] [CrossRef]
- Crossan, C.; Tsochatzis, E.A.; Longworth, L.; Gurusamy, K.; Papastergiou, V.; Thalassinos, E.; Mantzoukis, K.; Rodriguez-Peralvarez, M.; O’Brien, J.; Noel-Storr, A.; et al. Cost-effectiveness of noninvasive liver fibrosis tests for treatment decisions in patients with chronic hepatitis B in the UK: Systematic review and economic evaluation. J. Viral Hepat. 2016, 23, 139–149. [Google Scholar] [CrossRef]
- Shim, J.-J.; Oh, I.H.; Kim, S.B.; Kim, J.W.; Lee, C.K.; Jang, J.Y.; Lee, J.-S.; Kim, B.-H. Predictive Value of Antiviral Effects in the Development of Hepatocellular Carcinoma in the General Korean Population with Chronic Hepatitis B. Gut Liver 2016, 10, 962–968. [Google Scholar] [CrossRef]
- Lim, Y.S.; Ahn, S.H.; Shim, J.J.; Razavi, H.; Razavi-Shearer, D.; Sinn, D.H. Impact of expanding antiviral treatment criteria at a population level in the Republic of Korea: A modeling analysis. Hepatol. Int. 2021, 15, S31. [Google Scholar]
- Sanai, F.M.; Alghamdi, M.; Dugan, E.; Alalwan, A.; Al-Hamoudi, W.; Abaalkhail, F.; AlMasri, N.; Razavi-Shearer, D.; Razavi, H.; Schmelzer, J.; et al. A tool to measure the economic impact of Hepatitis B elimination: A case study in Saudi Arabia. J. Infect. Public Health 2020, 13, 1715–1723. [Google Scholar] [CrossRef]
- Martin, P.; Nguyen, M.H.; Dieterich, D.T.; Lau, D.T.-Y.; Janssen, H.L.; Peters, M.G.; Jacobson, I.M. Treatment Algorithm for Managing Chronic Hepatitis B Virus Infection in the United States: 2021 Update. Clin. Gastroenterol. Hepatol. 2022, 20, 1766–1775. [Google Scholar] [CrossRef]
- Dieterich, D.; Graham, C.; Wang, S.; Kwo, P.; Lim, Y.-S.; Liu, C.-J.; Agarwal, K.; Sulkowski, M. It Is Time for a Simplified Approach to Hepatitis B Elimination. Gastro Hep Adv. 2023, 2, 209–218. [Google Scholar] [CrossRef]
- Musabaev, E.; Sadirova, S.; Bakieva, S. Simplified test and treat protocols for population level screening and elimination of hepatitis B and hepatitis C in Uzbekistan. J Hepatol. 2021, 75, S642–S643. [Google Scholar]
- Razavi, H. Cost-effectiveness analysis of HCV/HBV elimination in the world. In Proceedings of the Global Hepatitis Summit, Virtual Meeting, 18 June 2021. [Google Scholar]




| EASL 2017 [3] | AASLD 2018 [6] | APASL 2016 [4] | |
|---|---|---|---|
| No cirrhosis | HBeAg-positive/negative AND HBV DNA > 2000 IU/mL AND ALT > ULN * and/or moderate liver necroinflammation or fibrosis † | HBeAg-positive AND HBV DNA > 20,000 IU/mL AND ALT ≥ 2× ULN * | HBeAg-positive AND HBV DNA > 20,000 IU/mL AND ALT > 2× ULN * |
| HBV DNA > 20,000 IU/mL AND ALT > 2× ULN * | HBeAg-negative AND HBV DNA ≥2000 IU/mL AND ALT ≥ 2× ULN * | HBeAg-negative AND HBV DNA > 2000 IU/mL AND ALT > 2× ULN * | |
| HBeAg-positive/negative AND family history of HCC or cirrhosis and extrahepatic manifestations | HBV DNA ≥2000 IU/mL AND ALT > ULN * AND significant necroinflammation or fibrosis ‡ or age > 40 years | Any HBV DNA or ALT if moderate to severe inflammation or significant fibrosis | |
| Cirrhosis | Detectable HBV DNA Any ALT level | HBV DNA < 2000 IU/mL § Any ALT level | HBV DNA > 2000 IU/mL § Any ALT level |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, Y.-S.; Kim, W.R.; Dieterich, D.; Kao, J.-H.; Flaherty, J.F.; Yee, L.J.; Roberts, L.R.; Razavi, H.; Kennedy, P.T.F. Evidence for Benefits of Early Treatment Initiation for Chronic Hepatitis B. Viruses 2023, 15, 997. https://0-doi-org.brum.beds.ac.uk/10.3390/v15040997
Lim Y-S, Kim WR, Dieterich D, Kao J-H, Flaherty JF, Yee LJ, Roberts LR, Razavi H, Kennedy PTF. Evidence for Benefits of Early Treatment Initiation for Chronic Hepatitis B. Viruses. 2023; 15(4):997. https://0-doi-org.brum.beds.ac.uk/10.3390/v15040997
Chicago/Turabian StyleLim, Young-Suk, W. Ray Kim, Douglas Dieterich, Jia-Horng Kao, John F. Flaherty, Leland J. Yee, Lewis R. Roberts, Homie Razavi, and Patrick T. F. Kennedy. 2023. "Evidence for Benefits of Early Treatment Initiation for Chronic Hepatitis B" Viruses 15, no. 4: 997. https://0-doi-org.brum.beds.ac.uk/10.3390/v15040997