
Allergy Associated Myocardial Infarction: A Comprehensive Report of Clinical Presentation, Diagnosis and Management of Kounis Syndrome

 ,
,
Abstract
:1. Introduction
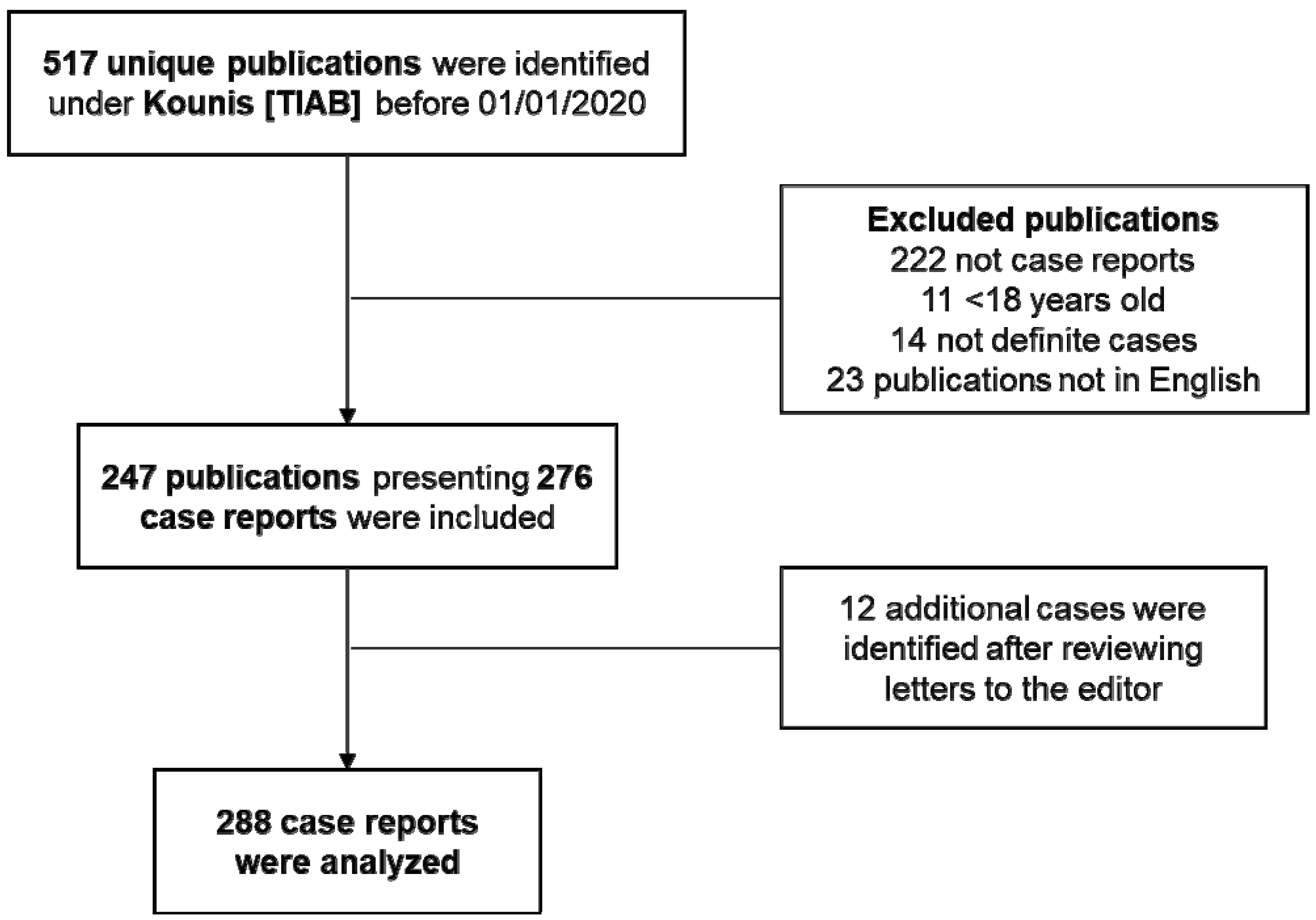
2. Materials and Methods
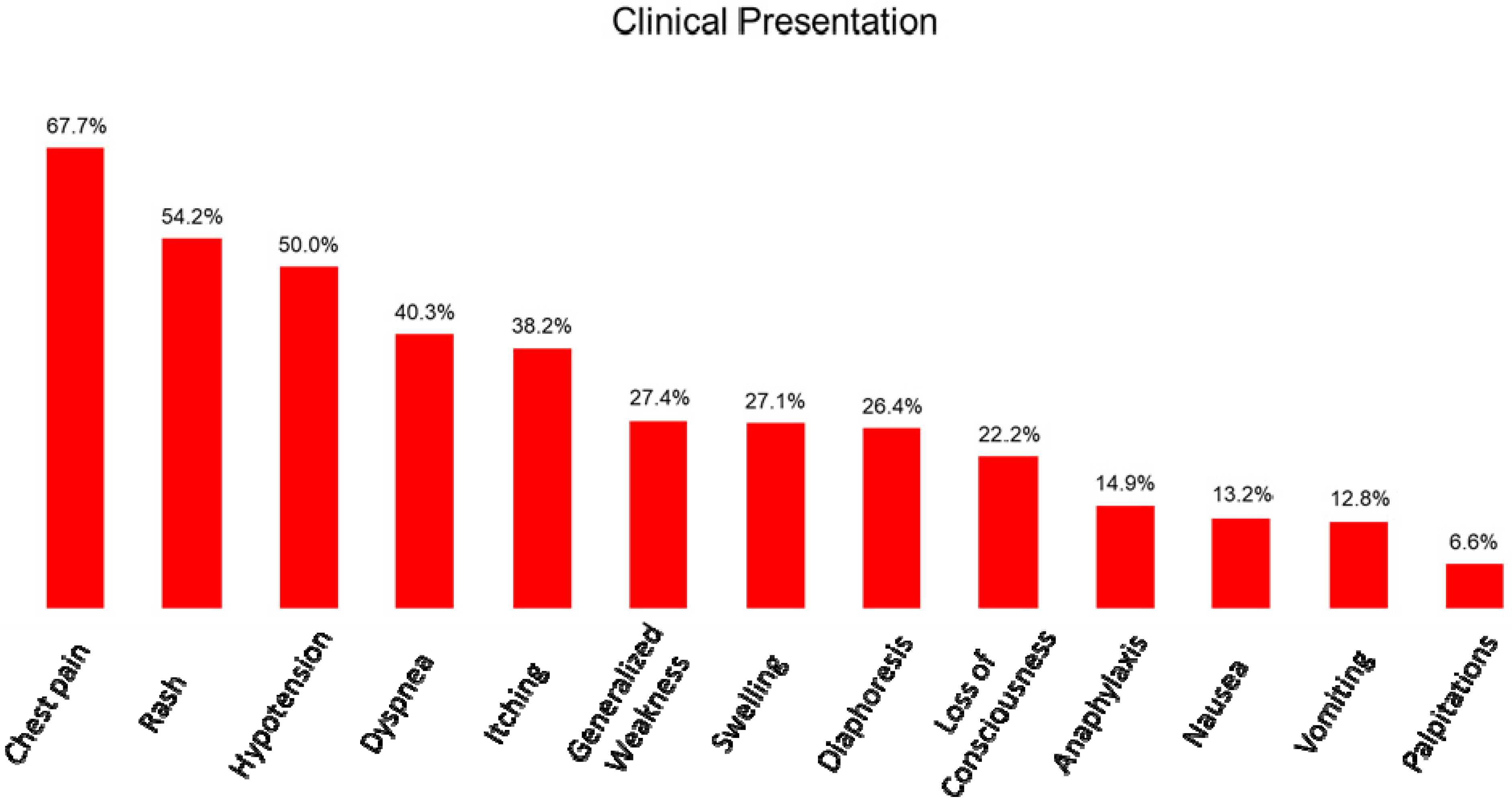
3. Results
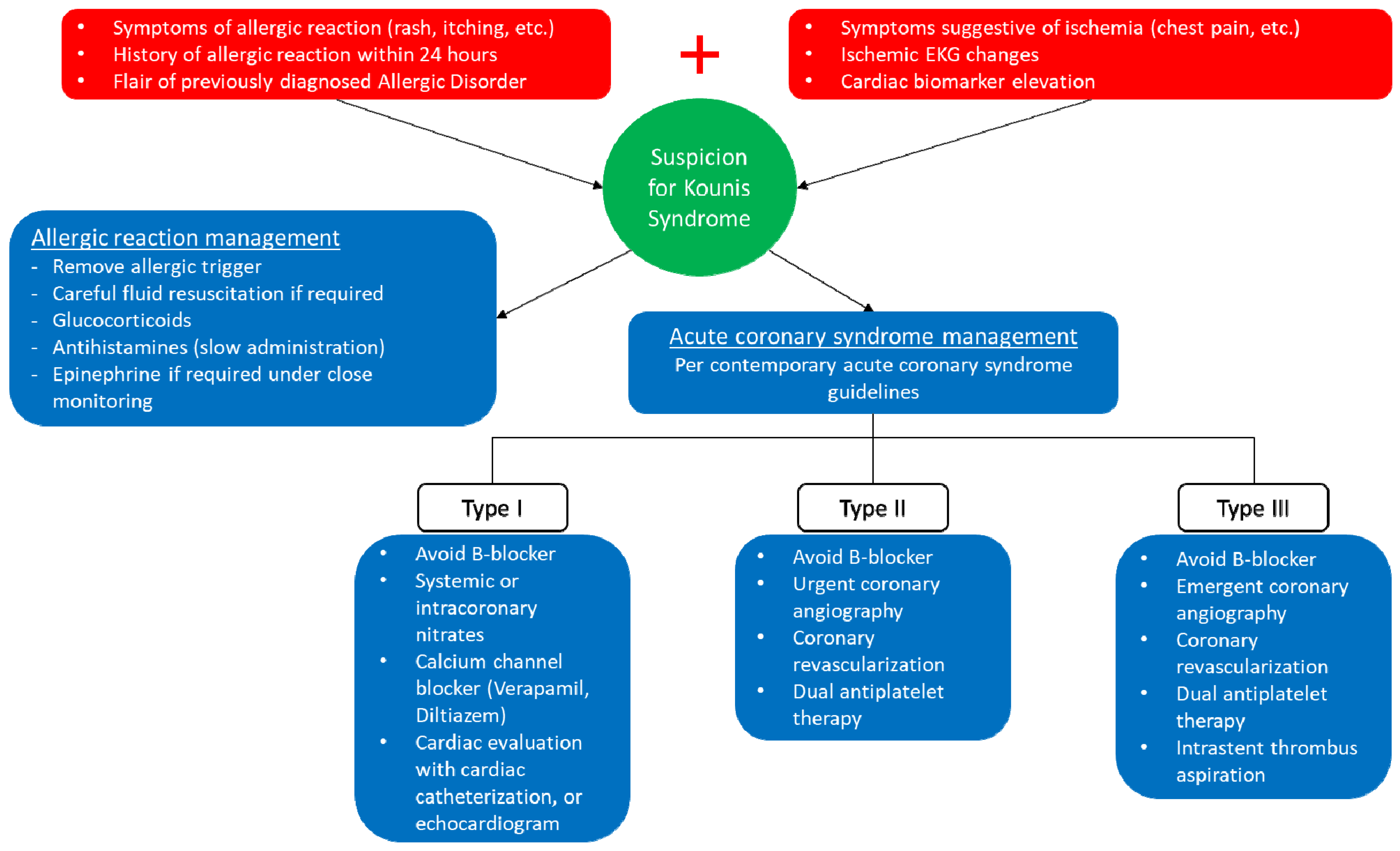
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACS | Acute coronary syndrome |
| CAD | Coronary artery disease |
| IgE | Immunoglobulin E |
| KS | Kounis syndrome |
| MINOCA | Myocardial infarction with non- obstructive coronary arteries |
References
- Golden, D.B. What is anaphylaxis? Curr. Opin. Allergy Clin. Immunol. 2007, 7, 331–336. [Google Scholar] [CrossRef]
- Mueller, U.R. Cardiovascular disease and anaphylaxis. Curr. Opin. Allergy Clin. Immunol. 2007, 7, 337–341. [Google Scholar] [CrossRef]
- Brawnwald, E. Unstable angina. An etiologic approach to management. Circulation 1998, 98, 2219–2222. [Google Scholar] [CrossRef]
- Kounis, N.G.; Zavras, G.M. Histamine-induced coronary artery spasm: The concept of allergic angina. Br. J. Clin. Pract. 1991, 45, 121–128. [Google Scholar]
- Kounis, N.G.; Hahalis, G.; Theoharides, T.C. Coronary Stents, Hypersensitivity Reactions, and the Kounis Syndrome. J. Interv. Cardiol. 2007, 20, 314–323. [Google Scholar] [CrossRef]
- Kovanen, P.T.; Kaartinen, M.; Paavonen, T. Infiltrates of Activated Mast Cells at the Site of Coronary Atheromatous Erosion or Rupture in Myocardial Infarction. Circulation 1995, 92, 1084–1088. [Google Scholar] [CrossRef]
- Kounis, N.G. Kounis syndrome: An update on epidemiology, pathogenesis, diagnosis and therapeutic management. Clin. Chem. Lab. Med. 2016, 54, 1545–1559. [Google Scholar] [CrossRef]
- Desai, R.; Parekh, T.; Patel, U.; Fong, H.K.; Samani, S.; Patel, C.; Savani, S.; Doshi, R.; Kumar, G.; Sachdeva, R. Epidemiology of acute coronary syndrome co-existent with allergic/hypersensitivity/anaphylactic reactions (Kounis syndrome) in the United States: A nationwide inpatient analysis. Int. J. Cardiol. 2019, 292, 35–38. [Google Scholar] [CrossRef]
- Li, J.; Zheng, J.; Zhou, Y.; Liu, X.; Peng, W. Acute coronary syndrome secondary to allergic coronary vasospasm (Kounis Syndrome): A case series, follow-up and literature review. BMC Cardiovasc. Disord. 2018, 18, 42. [Google Scholar] [CrossRef]
- Abdelghany, M.; Subedi, R.; Shah, S.; Kozman, H. Kounis syndrome: A review article on epidemiology, diagnostic findings, management and complications of allergic acute coronary syndrome. Int. J. Cardiol. 2017, 232, 1–4. [Google Scholar] [CrossRef]
- Ross, R. Atherosclerosis—An Inflammatory Disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef]
- Guedeney, P.; Claessen, B.E.; Kalkman, D.N.; Aquino, M.; Sorrentino, S.; Giustino, G.; Farhan, S.; Vogel, B.; Sartori, S.; Montalescot, G.; et al. Residual Inflammatory Risk in Patients With Low LDL Cholesterol Levels Undergoing Percutaneous Coronary Intervention. J. Am. Coll. Cardiol. 2019, 73, 2401–2409. [Google Scholar] [CrossRef]
- Kalkman, D.N.; Aquino, M.; Claessen, B.E.; Baber, U.; Guedeney, P.; Sorrentino, S.; Vogel, B.; De Winter, R.J.; Sweeny, J.; Kovacic, J.C.; et al. Residual inflammatory risk and the impact on clinical outcomes in patients after percutaneous coronary interventions. Eur. Hear. J. 2018, 39, 4101–4108. [Google Scholar] [CrossRef]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef]
- Krause, K.; Metz, M.; Makris, M.; Zuberbier, T.; Maurer, M. The role of interleukin-1 in allergy-related disorders. Curr. Opin. Allergy Clin. Immunol. 2012, 12, 477–484. [Google Scholar] [CrossRef]
- Kounis, N.G.; Koniari, I.; Velissaris, D.; Tzanis, G.; Hahalis, G. Kounis Syndrome—not a Single-organ Arterial Disorder but a Multisystem and Multidisciplinary Disease. Balk. Med. J. 2019, 36, 212–221. [Google Scholar] [CrossRef]
- Kang, Y.H.; Wei, H.M.; Fisher, H.; Merrill, G.F. Histamine-induced changes in coronary circulation and myocardial oxygen consumption: Influences of histamine receptor antagonists. FASEB J. 1987, 1, 483–490. [Google Scholar] [CrossRef]
- Raggi, P.; Genest, J.; Giles, J.T.; Rayner, K.; Dwivedi, G.; Beanlands, R.S.; Gupta, M. Role of inflammation in the pathogenesis of atherosclerosis and therapeutic interventions. Atherosclerosis 2018, 276, 98–108. [Google Scholar] [CrossRef]
- Chen, J.P.; Hou, D.; Pendyala, L.; Goudevenos, J.A.; Kounis, N.G. Drug-Eluting Stent Thrombosis: The Kounis Hypersensitivity-Associated Acute Coronary Syndrome Revisited. JACC Cardiovasc. Interv. 2009, 2, 583–593. [Google Scholar] [CrossRef]
- Rigger, J.; Ehl, N.F.; Nägele, R.; Rickli, H.; Maeder, M.T. Kounis syndrome revisited: Systemic mastocytosis and severe coronary artery disease. Int. J. Cardiol. 2016, 214, 510–511. [Google Scholar] [CrossRef]
- Paratz, E.D.; Khav, N.; Burns, A.T. Systemic Mastocytosis, Kounis Syndrome and Coronary Intervention: Case Report and Systematic Review. Hear. Lung Circ. 2017, 26, 772–778. [Google Scholar] [CrossRef] [PubMed]
- Wada, T.; Abe, M.; Yagi, N.; Kokubu, N.; Kasahara, Y.; Kataoka, Y.; Otsuka, Y.; Goto, Y.; Nonogi, H. Coronary vasospasm secondary to allergic reaction following food ingestion: A case of type I variant Kounis syndrome. Heart Vessel. 2010, 25, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.-H.; Hung, M.-J.; Yeh, K.-Y.; Yang, S.-Y.; Wang, C.-H. Oxaliplatin-Induced Coronary Vasospasm Manifesting As Kounis Syndrome: A Case Report. J. Clin. Oncol. 2011, 29, e776–e778. [Google Scholar] [CrossRef] [PubMed]
- Fassio, F.; Losappio, L.; Antolin-Amerigo, D.; Peveri, S.; Pala, G.; Preziosi, D.; Massaro, I.; Giuliani, G.; Gasperini, C.; Caminati, M.; et al. Kounis syndrome: A concise review with focus on management. Eur. J. Intern. Med. 2016, 30, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Fein, M.N.; Fischer, D.A.; O’Keefe, A.W.; Sussman, G.L. CSACI position statement: Newer generation H1-antihistamines are safer than first-generation H1-antihistamines and should be the first-line antihistamines for the treatment of allergic rhinitis and urticaria. Allergy Asthma Clin. Immunol. 2019, 15, 61. [Google Scholar] [CrossRef] [PubMed]
- Campbell, R.L.; Bellolio, F.; Knutson, B.D.; Bellamkonda, V.R.; Fedko, M.G.; Nestler, D.M.; Hess, E.P. Epinephrine in Anaphylaxis: Higher Risk of Cardiovascular Complications and Overdose After Administration of Intravenous Bolus Epinephrine Compared with Intramuscular Epinephrine. J. Allergy Clin. Immunol. Pract. 2015, 3, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef] [PubMed]
- Lang, D.M. Anaphylactoid and Anaphylactic Reactions Hazards of β-Blockers. Drug Saf. 1995, 12, 299–304. [Google Scholar] [CrossRef]
- Çeliker, M.; Tuncer, M.; Şekeralmaz, A. A Case with Repeated Recurrent Acute Coronary Syndrome due to Pseudoephedrine Use: Kounis Syndrome. Case Rep. Med. 2014, 2014, 742905. [Google Scholar] [CrossRef]
- Tamis-Holland, J.E.; Jneid, H.; Reynolds, H.R.; Agewall, S.; Brilakis, E.S.; Brown, T.M.; Lerman, A.; Cushman, M.; Kumbhani, D.J.; Arslanian-Engoren, C.; et al. Contemporary Diagnosis and Management of Patients With Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease: A Scientific Statement From the American Heart Association. Circulation 2019, 139, e891–e908. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Kounis Syndrome Type | Past Medical History |
|---|---|
| Patient Age | Coronary artery disease |
| Trigger of the allergic reaction | Prior percutaneous coronary intervention |
| Antibiotics | Peripheral arterial disease |
| Anesthetic drugs | Diabetes mellitus type I |
| Cardiac drugs | Diabetes mellitus type II |
| Other drugs | Chronic kidney disease |
| Insect bite | Hypertension |
| Food | Smoking |
| Systemic disease | Dyslipidemia |
| Symptomatology on presentation | Family history of coronary artery disease |
| Dyspnea | Overweight |
| Itching | History of allergy |
| Rash | Other |
| Swelling | Laboratory results |
| Sweating | Troponin |
| Nausea | CPK |
| Vomiting | CK-MB |
| Hypotension | Eosinophils |
| Anaphylactic shock | IgE |
| Cardiac symptoms | Specific IgE |
| Squeezing pain | Tryptase |
| Loss of consciousness | Medication at discharge |
| General symptoms | Aspirin |
| Palpitations | P2Y12 |
| Electrocardiographic changes | Heparin |
| ST elevation | Calcium channel blockers |
| Other acute ischemic changes | Nitrates |
| Bundle branch block | Antihistamine |
| Other ECG | Catheterization results |
| Allergic reaction management | Left anterior descending involvement |
| Epinephrine | Left circumflex involvement |
| Cortisone | Right coronary artery involvement |
| Antihistamine | Left main involvement |
| Nitrates | Atheromatosis/thrombosis |
| Echocardiography | Spasm |
| Previous Known EF | Clean coronary arteries |
| Present EF | Acute coronary syndrome management |
| Thrombolysis | |
| Coronary revascularization |
| Clinical Characteristics | Prevalence |
|---|---|
| Sex | |
| Male | 71.20% |
| Female | 28.80% |
| Kounis syndrome type | |
| I | 57.60% |
| II | 24.70% |
| III | 6.60% |
| Unclassified | 11.10% |
| Past medical history | |
| Coronary artery disease | 21.90% |
| Vascular disease | 4.50% |
| Diabetes mellitus | 15.30% |
| Chronic kidney disease | 1.70% |
| Hypertension | 31.40% |
| Smoking | 21.50% |
| Dyslipidemia | 18.60% |
| Overweight | 5.80% |
| Prior allergic reaction | 31.40% |
| Troponin elevation | 77.50% |
| Electrocardiographic findings | |
| ST segment elevation | 76.20% |
| T waves inversion and/or ST segment depression | 20.40% |
| Normal EKG | 3.30% |
| Coronary artery involved | |
| Left main | 2.50% |
| Left anterior descending | 27.30% |
| Left circumflex | 12.20% |
| Right coronary artery | 26.50% |
| Catheterization findings | |
| No changes | 50.60% |
| Coronary thrombosis/atheromatosis | 33.10% |
| Coronary spasm | 16.30% |
| Triggers | Incidence |
|---|---|
| Unknown | 6.3% |
| Medications | 51.7% |
| - Antibiotics | 44.3% |
| - Anesthetics | 9.4% |
| - Cardiovascular | 6.7% |
| - Other | 39.6% |
| Insect bite | 18.8% |
| - Bee | 50.0% |
| - Wasp | 29.6% |
| - Other | 20.4% |
| Food | 9.7% |
| - Seafood | 42.9% |
| - Fruit | 17.9% |
| - Other | 39.2% |
| Systemic disease | 2.4% |
| Environment | 1.4% |
| Contrast | 6.3% |
| Other | 3.5% |
| MEDICATIONS | |
|---|---|
| Antimicrobials | Other |
| Amoxicillin/clavulanic acid | Ranitidine |
| Ampicillin/sulbactam | Dextran 40 |
| Cefazolin | Viper antiserum |
| Penicillin | Gelofusine |
| Penicillin G | Succinylated gelatin |
| Amoxicillin | Recombinant human insulin |
| Cefotaxime | Triamcinolone |
| Cephalosporin | Hyoscine butylbromide |
| Ceftriaxone | Cervus and cucumis polypeptide |
| Cefuroxime | Dextromethorphan |
| Cefaclor | Progesterone |
| Cefuroxime axetil | Low molecular weight dextran |
| Ceftazidime | FOOD |
| Piperacillin/tazobactam | Blue crab |
| Cefditoren pivoxil | Gilthead |
| Moxifloxacin | Canned tuna fish |
| Ciprofloxacin | Cephalus fish |
| Levofloxacin | Tuna |
| Gemifloxacin | Tuna sandwich |
| Metronidazole | Shellfish |
| Fluconazole | Prawns |
| Clarithromycin | Anchovies |
| Brivudine | Fish |
| Telithromycin | Fish eggs |
| Trimethoprim/sulfamethoxazole | Undercooked fish |
| Clindamycin | Blue skinned fish |
| Vancomycin | Pleurotus ostreatus |
| Cardiac Medications | Mushrooms |
| Amiodarone | Rice pudding |
| Lidocaine hydrochloride | Lentil |
| Aspirin | Kiwi |
| Clopidogrel | Mango |
| ACE I | Pineapple |
| Epinephrine | Pea salad |
| Chemotherapeutic Agents | Salad with mustard |
| Cisplatin | Milk |
| Capecitabine | Wheat |
| Rituximab | Scallion |
| Oxaliplatin | Meat |
| Carboplatin | SYSTEMIC DISEASE |
| Daratumumab | Systemic macrocytosis |
| Paclitaxel | Asthma exacerbations |
| Cyclophosphamide | Urticaria flair |
| 5-fluorodeoxyuridylate | Chronic recurrent urticaria |
| Anesthetics | Idiopathic autoimmune urticaria |
| Bupivacaine | INSECT BITE |
| Cisatracurium | Bee sting |
| Succinylcholine | Bumblebee sting |
| Rocuronium | Honeybee sting |
| Mepivacaine | Wasp sting |
| Atracurium | Hornet sting |
| Propofol | Viper bite |
| Rocuronium-sugammadex | Adder bite |
| Analgesics | Snake venom |
| Ibuprofen | Cobra bite |
| Acetaminophen | Scorpion |
| Celecoxib | Spider bite |
| Metamizole | Warble fly bite |
| Diclofenac sodium | Fire ant bite |
| Diclofenac potassium | Fly carvaria |
| Ketoprofen | Larvae |
| Paracetamol | ENVIRONMENTAL FACTORS |
| Naproxen sodium | Dust |
| Acemetacin | Cold sea water contact |
| Propyphenazone | Kinds of metal |
| Flavoxate | Physical exercise |
| Tramadol | Post viral |
| Meperidine | Fishbone injury |
| Remifentanil | Plant |
| Morphine | Chinese herbs |
| Ketorolac | Pesticide sprays |
| Cannabinoids | Tree’s fluff |
| Marijuana | OTHER TRIGGERS |
| Bonsai type synthetic drugs | Leech therapy |
| Proton Pump Inhibitors | Latex |
| Pantoprazole | Ruptured hepatic echinococcal cyst |
| Lansoprazole | Combination of animal protein |
| Decongestants | Hemodialysis apparatus |
| Pseudoephedrine | Food-dependent exercise-induced anaphylaxis |
| Antipsychotics | Unknown |
| Ziprasidone | |
| Midazolam | |
| Contrast Media | |
| Iopromide | |
| Echo contrast media | |
| Iodinated contrast media | |
| Radioiodine contrast media | |
| Gadolinium contrast media | |
| Gadoteric acid |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roumeliotis, A.; Davlouros, P.; Anastasopoulou, M.; Tsigkas, G.; Koniari, I.; Mplani, V.; Hahalis, G.; Kounis, N.G. Allergy Associated Myocardial Infarction: A Comprehensive Report of Clinical Presentation, Diagnosis and Management of Kounis Syndrome. Vaccines 2022, 10, 38. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10010038
Roumeliotis A, Davlouros P, Anastasopoulou M, Tsigkas G, Koniari I, Mplani V, Hahalis G, Kounis NG. Allergy Associated Myocardial Infarction: A Comprehensive Report of Clinical Presentation, Diagnosis and Management of Kounis Syndrome. Vaccines. 2022; 10(1):38. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10010038
Chicago/Turabian StyleRoumeliotis, Anastasios, Periklis Davlouros, Maria Anastasopoulou, Grigorios Tsigkas, Ioanna Koniari, Virginia Mplani, Georgios Hahalis, and Nicholas G. Kounis. 2022. "Allergy Associated Myocardial Infarction: A Comprehensive Report of Clinical Presentation, Diagnosis and Management of Kounis Syndrome" Vaccines 10, no. 1: 38. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10010038