
Efficacy and Safety of Third Dose of the COVID-19 Vaccine among Solid Organ Transplant Recipients: A Systemic Review and Meta-Analysis



Abstract
:1. Background
2. Patients and Methods
2.1. Study Design
2.2. Inclusion Criteria and Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Outcomes
2.6. Assessment of Study Quality
2.7. Statistical Analysis
3. Results
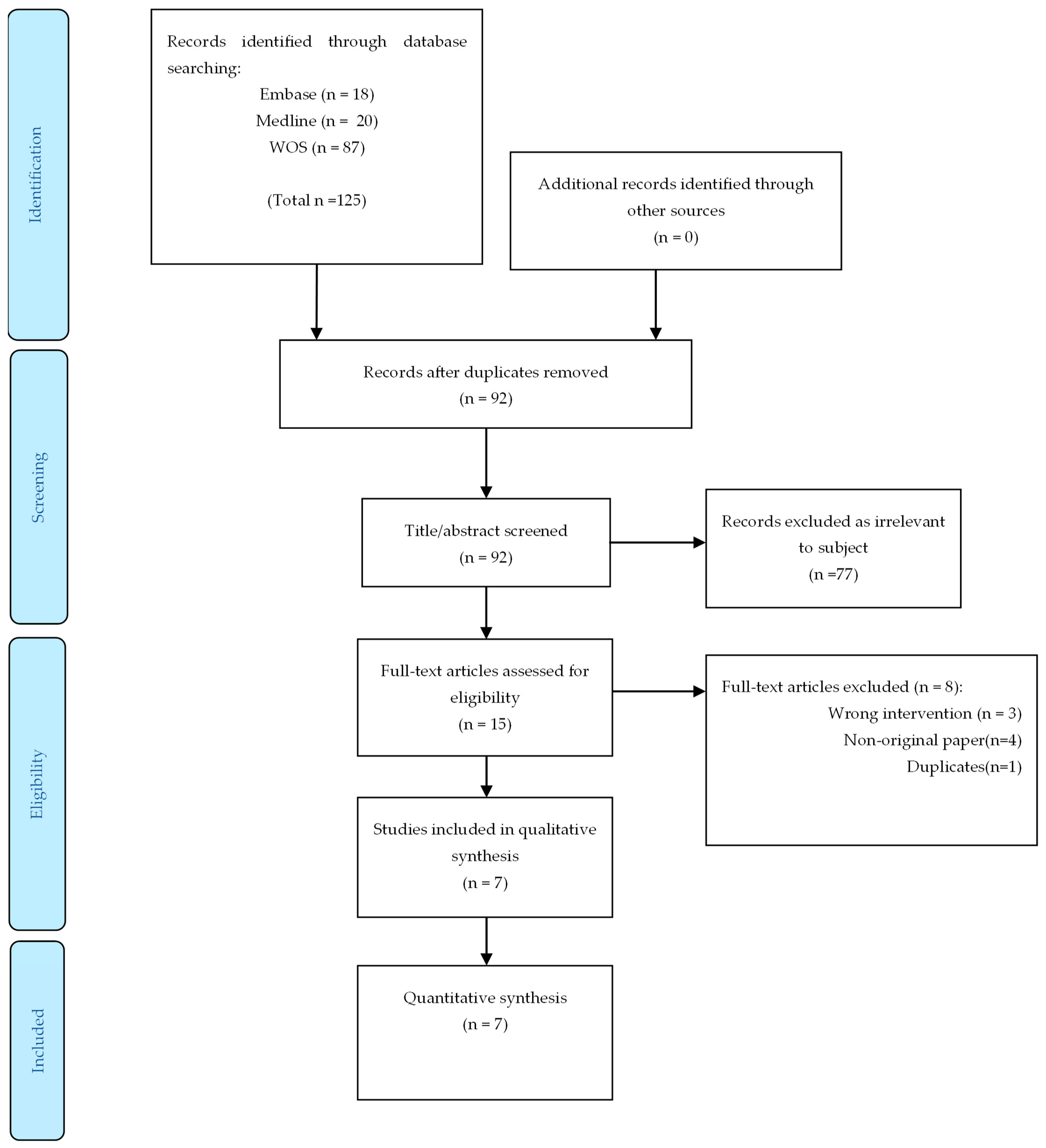
3.1. Bibliographic Search and Study Selection
3.2. Characteristics of the Included Studies
3.3. Patient Characteristics
3.4. Primary Endpoint Measurement
3.5. Safety
3.6. Quality of Evidence and Risk of Bias Assessments
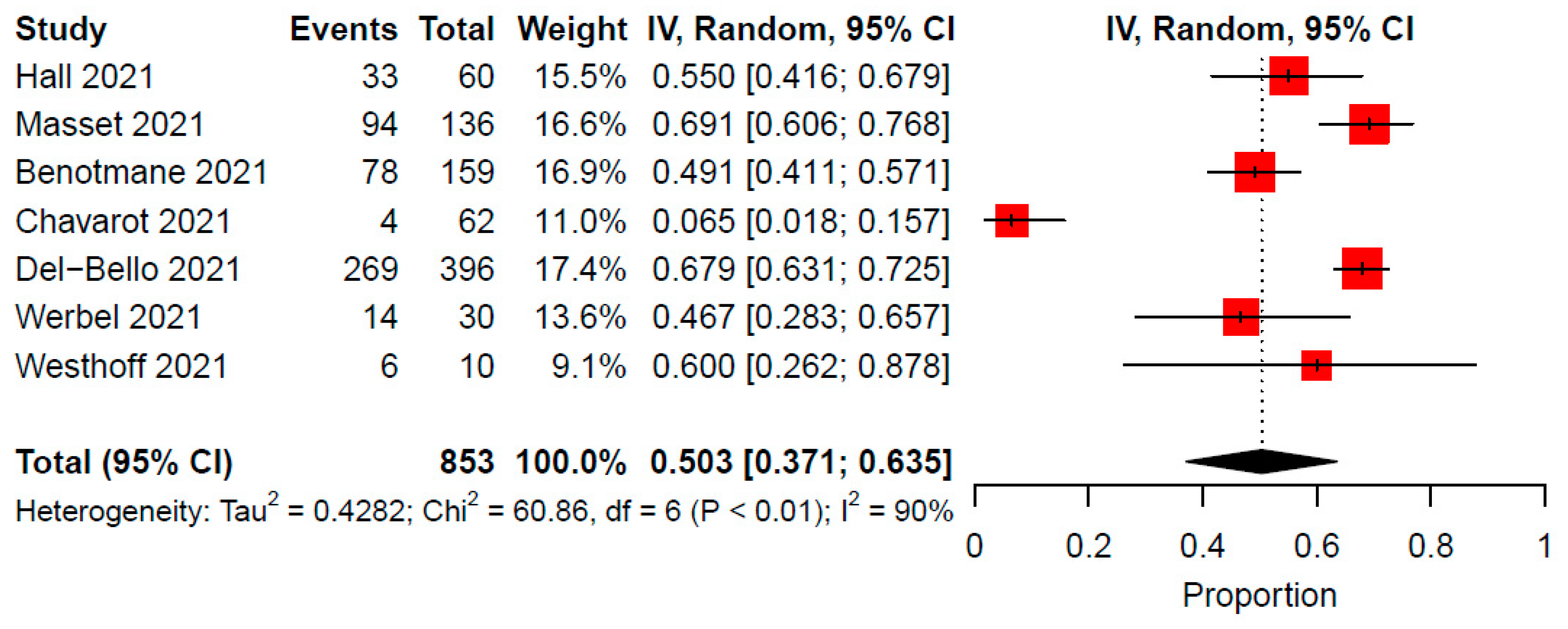
3.7. Antibody Response Following a Third Dose
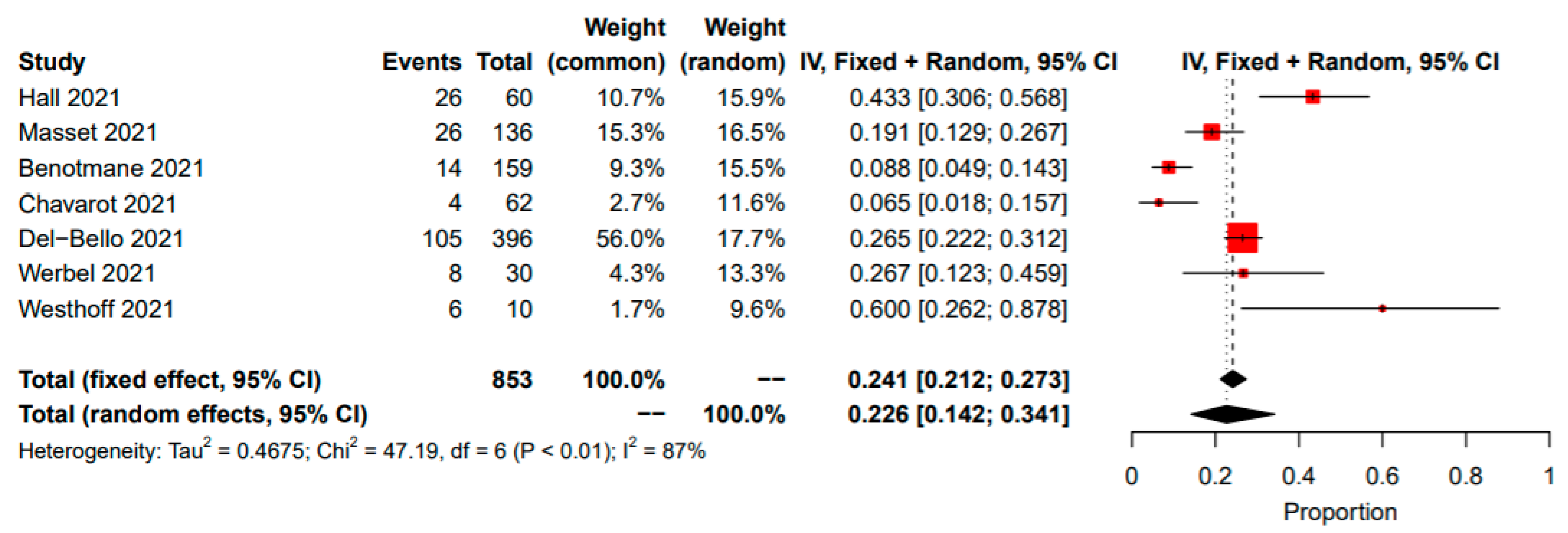
3.8. Seroconversion Rate between the Second and Third Vaccine Doses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| FDA | The United States Food and Drug Administration |
| GLMM | Generalized linear mixed models |
| GRADE | Grading of Recommendations, Assessment, Development, and Evaluation |
| IQR | Interquartile range |
| MMF/MPA | Mycophenolic acid |
| mTOR | Mammalian target of rapamycin |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines |
| PROSPERO | Prospective International Register of Systematic Reviews |
| RCT | Randomized controlled trial |
| ROBINS-I | Risk of Bias in Nonrandomized Studies of Intervention |
| SD | Standard deviation |
References
- Kates, O.S.; Haydel, B.M.; Florman, S.S.; Rana, M.M.; Chaudhry, Z.S.; Ramesh, M.S.; Safa, K.; Kotton, C.N.; Blumberg, E.A.; Besharatian, B.D.; et al. COVID-19 in solid organ transplant: A multi-center cohort study. Clin. Infect. Dis. 2020, 73, e4090–e4099. [Google Scholar] [CrossRef] [PubMed]
- Caillard, S.; Chavarot, N.; Francois, H.; Matignon, M.; Greze, C.; Kamar, N.; Gatault, P.; Thaunat, O.; Legris, T.; Frimat, L.; et al. Is COVID-19 infection more severe in kidney transplant recipients? Arab. Archaeol. Epigr. 2021, 21, 1295–1303. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, B.; et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 2020, 283, 2603–2615. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Antibody response to 2-dose SARS-CoV-2 mRNA vaccine series in solid organ transplant recipients. JAMA 2021, 325, 2204–2206. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Immunogenicity of a single dose of SARS-CoV-2 messenger RNA vaccine in solid organ transplant recipients. JAMA 2021, 325, 1784–1786. [Google Scholar] [CrossRef] [PubMed]
- Grupper, A.; Rabinowich, L.; Schwartz, D.; Schwartz, I.F.; Ben-Yehoyada, M.; Shashar, M.; Katchman, E.; Halperin, T.; Turner, D.; Goykhman, Y.; et al. Reduced humoral response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients without prior exposure to the virus. Arab. Archaeol. Epigr. 2021, 21, 2719–2726. [Google Scholar] [CrossRef]
- Shostak, Y.; Shafran, N.; Heching, M.; Rosengarten, D.; Shtraichman, O.; Shitenberg, D.; Amor, S.M.; Yahav, D.; Ben Zvi, H.; Pertzov, B.; et al. Early humoral response among lung transplant recipients vaccinated with BNT162b2 vaccine. Lancet Respir. Med. 2021, 9, e52–e53. [Google Scholar] [CrossRef]
- Marion, O.; Del Bello, A.; Abravanel, F.; Couat, C.; Faguer, S.; Esposito, L.; Hebral, A.L.; Izopet, J.; Kamar, N. Safety and Immunogenicity of Anti–SARS-CoV-2 Messenger RNA Vaccines in Recipients of Solid Organ Transplants. Ann. Intern. Med. 2021, 174, 1336–1338. [Google Scholar] [CrossRef]
- Kar-gupta, S.; Copley, C. Ignoring WHO Call, Major Nations Stick to Vaccine Booster Plans. Available online: https://www.reuters.com/world/europe/french-president-macron-third-covid-vaccine-doses-likely-elderly-vulnerable-2021-08-05/ (accessed on 5 August 2021).
- Del Bello, A.; Abravanel, F.; Marion, O.; Couat, C.; Esposito, L.; Lavayssière, L.; Izopet, J.; Kamar, N. Efficiency of a boost with a third dose of anti-SARS-CoV-2 messenger RNA-based vaccines in solid organ transplant recipients. Am. J. Transplant. 2021, 22, 322–323. [Google Scholar] [CrossRef] [PubMed]
- Werbel, W.A.; Boyarsky, B.J.; Ou, M.T.; Massie, A.B.; Tobian, A.A.; Garonzik-Wang, J.M.; Segev, D.L. Safety and Immunogenicity of a Third Dose of SARS-CoV-2 Vaccine in Solid Organ Transplant Recipients: A Case Series. Ann. Intern. Med. 2021, 174, 1330–1332. [Google Scholar] [CrossRef]
- Benotmane, I.; Gautier, G.; Perrin, P.; Olagne, J.; Cognard, N.; Fafi-Kremer, S.; Caillard, S. Antibody Response After a Third Dose of the mRNA-1273 SARS-CoV-2 Vaccine in Kidney Transplant Recipients With Minimal Serologic Response to 2 Doses. JAMA 2021, 326, 1063. [Google Scholar] [CrossRef] [PubMed]
- Masset, C.; Kerleau, C.; Garandeau, C.; Ville, S.; Cantarovich, D.; Hourmant, M.; Kervella, D.; Houzet, A.; Guillot-Gueguen, C.; Guihard, I.; et al. A third injection of the BNT162b2 mRNA COVID-19 vaccine in kidney transplant recipients improves the humoral immune response. Kidney Int. 2021, 100, 1132–1135. [Google Scholar] [CrossRef]
- Westhoff, T.H.; Seibert, F.S.; Anft, M.; Blazquez-Navarro, A.; Skrzypczyk, S.; Zgoura, P.; Meister, T.L.; Pfaender, S.; Stumpf, J.; Hugo, C.; et al. third vaccine dose substantially improves humoral and cellular SARS-CoV-2 immunity in renal transplant recipients with primary humoral nonresponse. Kidney Int. 2021, 100, 1135–1136. [Google Scholar] [CrossRef]
- Hall, V.G.; Ferreira, V.H.; Ku, T.; Ierullo, M.; Majchrzak-Kita, B.; Chaparro, C.; Selzner, N.; Schiff, J.; McDonald, M.; Tomlinson, G.; et al. Randomized Trial of a Third Dose of mRNA-1273 Vaccine in Transplant Recipients. N. Engl. J. Med. 2021, 385, 1244–1246. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Warton, D.I.; Hui, F.K.C. The arcsine is asinine: The analysis of proportions in ecology. Ecology 2011, 92, 3–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, L.; Xu, C.; Chu, H. Empirical Comparisons of 12 Meta-analysis Methods for Synthesizing Proportions of Binary Outcomes. J. Gen. Intern. Med. 2021, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA Covid-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef]
- Chavarot, N.; Morel, A.; Leruez-Ville, M.; Villain, E.; Divard, G.; Burger, C.; Serris, A.; Sberro-Soussan, R.; Martinez, F.; Amrouche, L.; et al. Weak antibody response to three doses of mRNA vaccine in kidney transplant recipients treated with belatacept. Arab. Archaeol. Epigr. 2021, 21, 4043–4051. [Google Scholar] [CrossRef] [PubMed]
- Couzin-Frankel, J. ‘This Gives Hope’: A Third COVID-19 Vaccine Dose Can Boost Protection for Organ Transplant Recipients. Available online: https://www.science.org/content/article/gives-hope-third-covid-19-vaccine-dose-can-boost-protection-organ-transplant-recipients (accessed on 14 June 2021).
- Coronavirus (COVID-19) Update: FDA Authorizes Additional Vaccine Dose for Certain Immunocompromised Individuals. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-additional-vaccine-dose-certain-immunocompromised (accessed on 12 August 2021).
- Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Approved or Authorized in the United States. Available online: https://www.cdc.gov/vaccines/covid-19/clinical-considerations/covid-19-vaccines-us.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fvaccines%2Fcovid-19%2Finfo-by-product%2Fclinical-considerations.html#pfizer-booster (accessed on 27 September 2021).
- Moderbacher, C.R.; Ramirez, S.I.; Dan, J.M.; Grifoni, A.; Hastie, K.M.; Weiskopf, D.; Belanger, S.; Abbott, R.K.; Kim, C.; Choi, J.; et al. Antigen-Specific Adaptive Immunity to SARS-CoV-2 in Acute COVID-19 and Associations with Age and Disease Severity. Cell 2020, 19, 996–1012. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author (Month Year) | Country | Design | Participants | No. of Participants | Males (%) | Age Median/Mean (Range/SD) | Organ Transplanted | Immunosuppression | Time from Transplantation (Median, IQR) | Third Vaccine Dose | Time from 2nd to 3rd Dose | Antibody Titer before 3rd Dose |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hall (Sep 2021) | Canada | RCT | Solid-organ transplant recipients | 120 | 61.7% | 66.6 (63.3–71.4) | Lung (11%), heart (10%), kidney (20%), pancreas, kidney–pancreas (15%), liver (4%) | Steroids (83.3%), calcineurin inhibitor (98.3%), MMF/mycophenolate sodium (73.3%), azathioprine (13.3%), sirolimus (10%) | 3.16 (1.71–6.12) years | mRNA-1273 (Moderna) | Two months | 11.70% |
| Masset (Aug 2021) | France | Retrospective | Kidney transplant recipients | 136 | 63.20% | 63.7 (±11.7) | Kidney (100%) | Calcineurin inhibitor (85.8%), mTOR inhibitor (14.9%), antimetabolite (75.4%), steroids (32.1%) | 10.5 (±8.5) years | mRNA-BNT162b2 (Pfizer/BioNTech) | 50 days | 49.70% |
| Benotmane (Jul 2021) | France | Retrospective | Kidney transplant recipients with minimal serologic response to two doses | 159 | 61.60% | 57.6 (49.6-66.1) | Kidney (100%) | Tacrolimus + MMF/MPA + steroids (52.8%) | 5.3 (1.9–11.1) years | mRNA-1273 (Moderna) | 51 days (IQR, 48–59 days) | 40.3% (0 patients were considered positive) |
| Chavarot (Aug 2021) | France | Retrospective | Belatacept-treated kidney transplant recipients | 62 | 58% | 63.5 (51–72) | Kidney (100%) | Belatacept + MPA (71%), mTOR inhibitor (13%), azathioprine (5%), steroids (100%) | 47.5 (25.3–79) months | mRNA-BNT162b2 (Pfizer/BioNTech) | 69.5 days (IQR 40-84) | 0.00% |
| Del Bello (Jul 2021) | France | Retrospective | Solid organ transplant recipients | 396 | 65% | 59 ± 15 | Kidney (69.9%), liver (14.2%), heart or lung (8.5%), pancreas (1.5%), combined (2.5%) | Calcineurin inhibitor (86.1%), MPA (71.9%) mTOR inhibitor (26.7%), belatacept (6.3%), steroids (82.0%) | mRNA-BNT162b2 (Pfizer/BioNTech) | 59 days (IQR 47–67) | 41.4% (95% CI, 36.5% to 46.3% | |
| Werbel (Sep 2021) | USA | Retrospective | Solid organ transplant recipients | 30 | 43% | 57 (44–62) | Kidney (73.3%), liver (10%), heart (6.6%), pancreas (3.3%), lung (3.3%), combined (3.3%) | Tacrolimus or cyclosporine + MPA (83.3%), steroids (80%), sirolimus (3.3%), belatacept (3.3%) | 4.5 (2.3–10.5) years | Ad26.COV2. S (50%)(J&J/Janssen), mRNA-1273 (30%) (Moderna), 162b2 (20%) (Pfizer/BioNTech) | 67 days (IQR, 54 to 81) | 20% |
| Westhoff (Sep 2021) | Germany | Retrospective | Kidney transplant recipients | 10 | 80% | 60 (51.5–67.5) | Kidney (100%) | Calcineurin inhibitor (80.0%), MPA (90%), mTOR inhibitor (10.0%), belatacept (10.0%), steroids (100.0%) | 41.5 (21.75–89.25) months | mRNA-1273 (Moderna) | 10 (10–10) weeks | 0 |
| Author (Month Year) | Primary Outcome | Time from 3rd Vaccine to Outcome Measuring | Primary Outcome Measuring Technique | Seropositive Rate (%) | Secondary Outcome | Secondary Outcome Results | Factors Associated with Reduced Response | Safety |
|---|---|---|---|---|---|---|---|---|
| Hall (Sep 2021) | Serologic response | One month | Electrochemiluminescence immunoassay (Roche Elecsys®) | 55% | 1. The median percent virus neutralization 2. The polyfunctional T-cell response | 1. 71% 2. The median SARS-CoV-2–specific T-cell counts were greater, with a minimal polyfunctional CD8+ T-cell response | Local and systemic events were slightly more common after the third dose of mRNA-1273. No grade 3 or 4 events and no cases of acute rejection occurred. | |
| Masset (Aug 2021) | Serologic response | One month | Chemiluminescent microparticle immunoassay (Abbott Architect®) or chemiluminescence immunoassay (Siemens Atellica®), or electrochemiluminescence immunoassay (Roche Elecsys®) | 69.2% | Antibody titer concentration | Low antibody titers (median 209, IQR (20-409) AU/mL) | 1. Lymphocyte count < 1500/mm3 2. Impairment of allograft function 3. Female recipients | |
| Benotmane (Jul 2021) | Serologic response | 28 days (IQR, 27–33) | Chemiluminescent microparticle immunoassay (Abbott Architect®) | 49% | 1. Patients without an antibody response 2. Patients receiving tacrolimus, mycophenolate, and steroids | No severe adverse events were observed after the third dose. | ||
| Chavarot (Aug 2021) | Serologic response | 28 days (IQR, 28-33) | Chemiluminescent microparticle immunoassay (Abbott Architect®) | 6.4% | No patient presented severe systemic events. | |||
| Del Bello (Jul 2021) | Serologic response | Four weeks | Enzyme-linked immunosorbent assay (Beijing Wantai Biological Pharmacy Enterprise) | 67.9% | 1. Older patients 2. Patients receiving mycophenolic acid, belatacept 3. Patients receiving at least a triple immunosuppression | No serious adverse event or acute rejection episode was observed. | ||
| Werbel (Sep 2021) | Serologic response | 14 days (IQR, 14–17) | Electrochemiluminescence immunoassay (Roche Elecsys® or Quantitative ELISA (EUROIMMUN) | 46.6% | No patient presented severe systemic events. One heart transplant recipient had a biopsy-proven, antibody- mediated rejection seven days after the third dose in the setting of acute volume overload. | |||
| Westhoff (Sep 2021) | Serologic response | Two weeks | Electrochemiluminescence immunoassay (Roche Elecsys®) | 60% | 1. Antibody titer concentration 2. Reactive T cells response | 1. Median antibody titer concentration of 542 (IQR, 478–923) U/mL 2. A substantial increase in the magnitude of SARS-CoV-2 spike (S) protein–reactive T-cell immunity in 90% of subjects |
| Author (Month Year) | Certainty of the Evidence (GRADE) 20 * | Risk of Bias Assessment (ROBINS-I) 21 # |
|---|---|---|
| Hall (Sep. 2021) | High | N/A |
| Masset (Aug. 2021) | Moderate Due to the risk of bias | Moderate |
| Benotmane (Jul. 2021) | Moderate Due to the risk of bias | Moderate |
| Chavarot (Aug. 2021) | Low Due to risk of bias and inconsistency | Moderate |
| Del Bello (Jul. 2021) | Moderate Due to the risk of bias | Serious |
| Werbel (Sep. 2021) | Low Due to the risk of bias and imprecision | Moderate |
| Westhoff (Sep. 2021) | Low Due to the risk of bias and imprecision | Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Efros, O.; Anteby, R.; Halfon, M.; Meisel, E.; Klang, E.; Soffer, S. Efficacy and Safety of Third Dose of the COVID-19 Vaccine among Solid Organ Transplant Recipients: A Systemic Review and Meta-Analysis. Vaccines 2022, 10, 95. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10010095
Efros O, Anteby R, Halfon M, Meisel E, Klang E, Soffer S. Efficacy and Safety of Third Dose of the COVID-19 Vaccine among Solid Organ Transplant Recipients: A Systemic Review and Meta-Analysis. Vaccines. 2022; 10(1):95. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10010095
Chicago/Turabian StyleEfros, Orly, Roi Anteby, Mirit Halfon, Eshcar Meisel, Eyal Klang, and Shelly Soffer. 2022. "Efficacy and Safety of Third Dose of the COVID-19 Vaccine among Solid Organ Transplant Recipients: A Systemic Review and Meta-Analysis" Vaccines 10, no. 1: 95. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10010095