
COVID-19 Vaccination in Cancer Patients Older Than 70 Years Undergoing Active Treatment. Seroconversion Rate and Safety

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Times of Vaccination
2.2. Endpoints
- Safety;
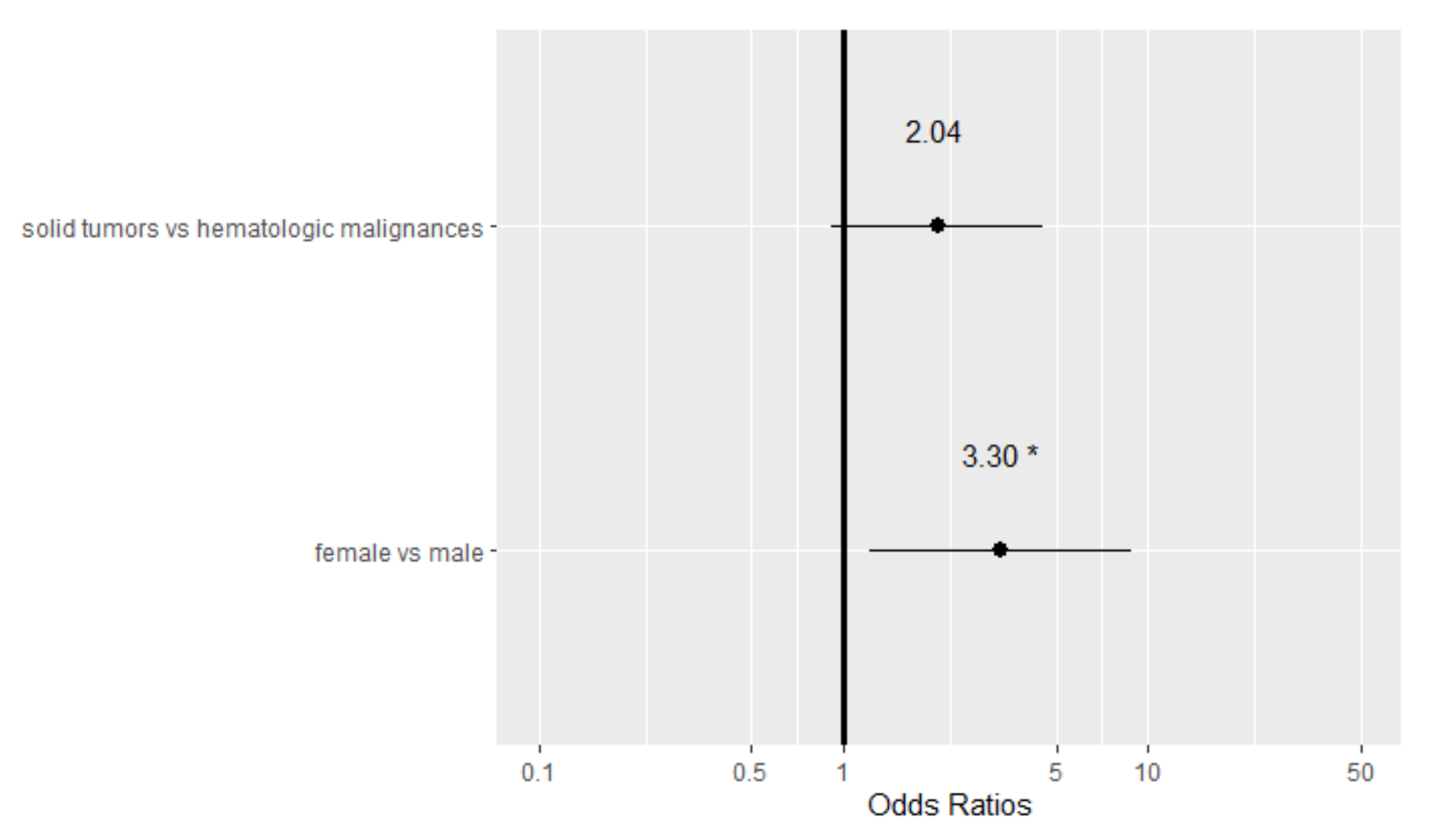
- Factors influencing vaccine seropositivity;
- Diagnosis of symptomatic or asymptomatic post-vaccine COVID-19 infection;
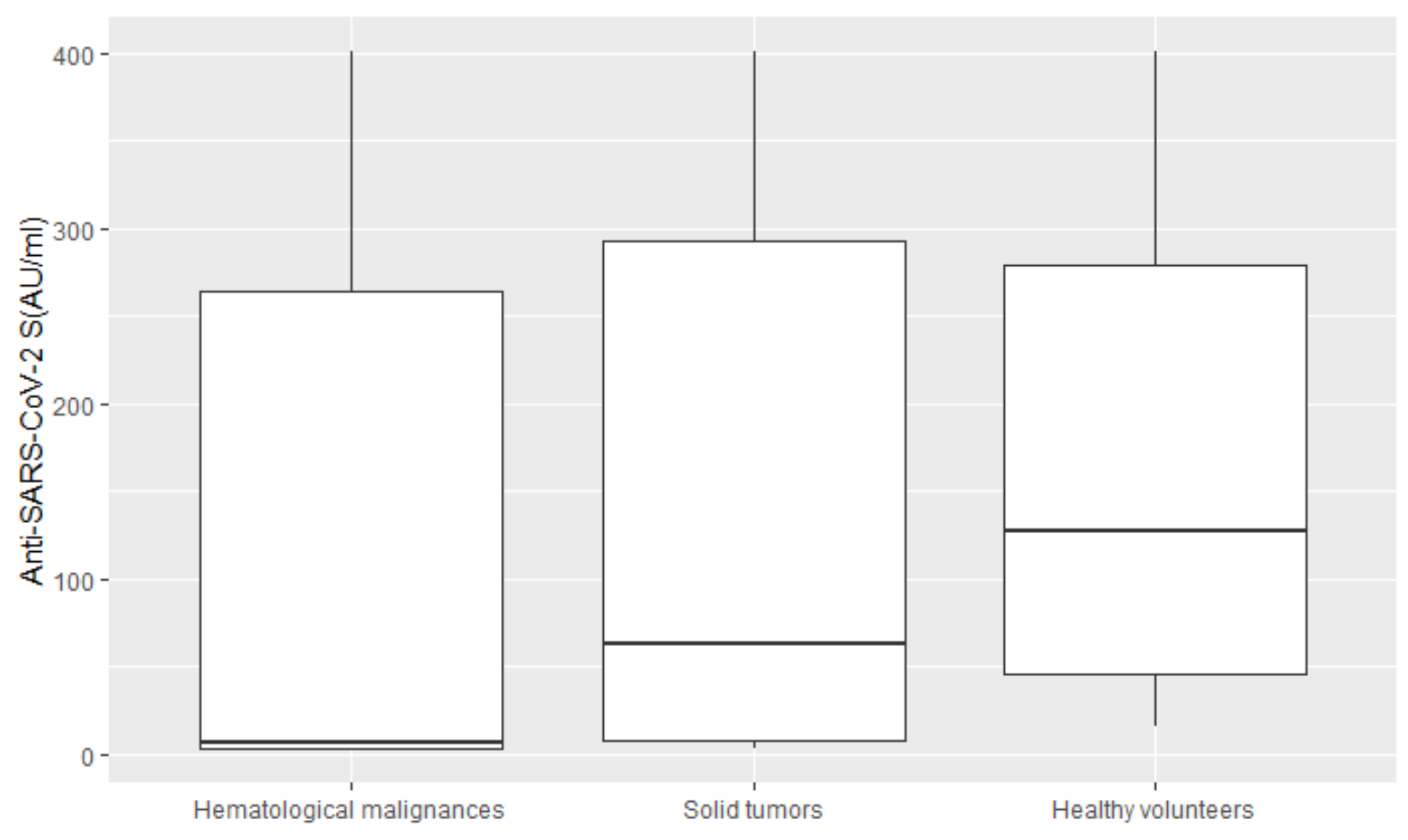
- Median IgG titer of patients versus healthy volunteers.
2.3. Safety of the Vaccine
2.4. Serological Assessment
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China. N. Engl. J. Med. 2019, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Stroppa, E.M.; Toscani, I.; Citterio, C.; Anselmi, E.; Zaffignani, E.; Codeluppi, M.; Cavanna, L. Coronavirus disease-2019 in cancer patients. A report of the first 25 cancer patients in a western country (Italy). Future Oncol. 2020, 16, 1425–1432. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Xu, Y.; Sun, C.; Wang, X.; Guo, Y.; Qiu, S.; Ma, K. A systematic review of asymptomatic infections with COVID-19. J. Microbiol. Immunol. Infect. 2021, 54, 12–16. [Google Scholar] [CrossRef]
- Garibaldi, B.T.; Fiksel, J.; Muschelli, J.; Robinson, M.L.; Rouhizadeh, M.; Perin, J.; Schumock, G.; Nagy, P.; Gray, J.H.; Malapati, H.; et al. Patient Trajectories among Persons Hospitalized for COVID-19: A Cohort Study. Ann. Intern. Med. 2020, 174, 33–41. [Google Scholar] [CrossRef]
- Cavanna, L.; Citterio, C.; Toscani, I.; Franco, C.; Magnacavallo, A.; Caprioli, S.; Cattadori, E.; Di Nunzio, C.; Pane, R.; Schiavo, R.; et al. Cancer patients with COVID-19: A retrospective study of 51 patients in the district of Piacenza, Northern Italy. Future Sci. OA 2020, 7, FSO645. [Google Scholar] [CrossRef]
- Chamilos, G.; Lionakis, M.S.; Kontoyiannis, D.P. Are all patients with cancer at heightened risk for severe Coronavirus Disease 2019. Clin. Infect. Dis. 2021, 72, 351–356. [Google Scholar] [CrossRef]
- El Saghir, N.S.; Oncology Care and Education during the Coronavirus (COVID-19) Pandemic. ASCO Connection. Available online: http://www.lsmo-lb.org/news/caring-for-cancer-patients-during-the-covid-19-pandemic (accessed on 4 November 2021).
- Wu, C.; Chen, X.; Cai, Y.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; Zhang, Y.; et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 1031. [Google Scholar] [CrossRef] [Green Version]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef]
- Chen, Y.; Klein, S.L.; Garibaldi, B.T.; Li, H.; Wu, C.; Osevala, N.M.; Li, T.; Margolick, J.B.; Pawelec, G.; Leng, S.X. Aging in COVID-19: Vulnerability, immunity and intervention. Ageing Res. Rev. 2021, 65, 101205. [Google Scholar] [CrossRef]
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and immunogenicity of two RNA-based COVID-19 vaccine candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef]
- Jackson, L.A.; Anderson, E.J.; Rouphael, N.G.; Roberts, P.C.; Makhene, M.; Coler, R.N.; McCullough, M.P.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; et al. An mRNA vaccine against SARS-CoV-2-preliminary report. N. Engl. J. Med. 2020, 383, 1920–1931. [Google Scholar] [CrossRef]
- Massarweh, A.; Eliakim-Raz, N.; Stemmer, A.; Levy-Barda, A.; Yust-Katz, S.; Zer, A.; Benouaich-Amiel, A.; Ben-Zvi, H.; Moskovits, N.; Brenner, B.; et al. Evaluation of seropositivity following BNT162b2 messenger RNA vaccination for SARS-CoV-2 in patients undergoing treatment for cancer. JAMA Oncol. 2021, 28, e212155. [Google Scholar] [CrossRef]
- Revon-Riviere, G.; Ninove, L.; Min, V.; Rome, A.; Coze, C.; Verschuur, A.; de Lamballerie, X.; André, N. The BNT162b2 mRNA COVID-19 vaccine in adolescents and young adults with cancer: A monocentric experience. Eur. J. Cancer 2021, 154, 30–34. [Google Scholar] [CrossRef]
- Thakkar, A.; Gonzalez-Lugo, J.D.; Goradia, N.; Gali, R.; Shapiro, L.C.; Pradhan, K.; Rahman, S.; Kim, S.Y.; Ko, B.; Sica, R.A.; et al. Seroconversion rates following COVID-19 vaccination among patients with cancer. Cancer Cell 2021, 39, 1081–1090.e2. [Google Scholar] [CrossRef]
- Monin, L.; Laing, A.G.; Muñoz-Ruiz, M.; McKenzie, D.R.; del Molino del Barrio, I.; Alaguthurai, T.; Domingo-Vila, C.; Hayday, T.S.; Graham, C.; Seow, J.; et al. Safety and immunogenicity of one versus two doses of the COVID-19 vaccine BNT162b2 for patients with cancer: Interim analysis of a prospective observational study. Lancet Oncol. 2021, 22, 765–778. [Google Scholar] [CrossRef]
- Barriere, J.; Chemorey, E.; Adjtoutah, Z. Impired immunogenicity of BNT162b2 anti-SARS-CoV-2 vaccine in patients treated for solid tumors. Ann. Oncol. 2021, 32, 1053–1055. [Google Scholar] [CrossRef]
- Desai, A.; Sachdeva, S.; Parekh, T.; Desai, R. COVID-19 and cancer: Lessons from a pooled meta-analysis. JCO Glob. Oncol. 2020, 6, 557–559. [Google Scholar] [CrossRef]
- Cavanna, L.; Citterio, C.; Di Nunzio, C.; Biasini, C.; Palladino, M.A.; Ambroggi, M.; Madaro, S.; Bidin, L.; Porzio, R.; Proietto, M. Prevalence of COVID-19 Infection in Asymptomatic Cancer Patients in a District with High Prevalence of SARS-CoV-2 in Italy. Cureus 2021, 13, e13774. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Interim Guidelines for Collecting, Handling, and Testing Clinical Specimens from Patients under Investigation (PUIs) for 2019 Novel Coronavirus (2019-nCoV). Available online: www.cdc.gov/coronavirus/2019-ncov/lab/guidelines-clinical-specimens.html (accessed on 17 June 2021).
- Bonelli, F.; Sarasini, A.; Zierold, C.; Calleri, M.; Bonetti, A.; Vismara, C.; Blocki, F.A.; Pallavicini, L.; Chinali, A.; Campisi, D.; et al. Clinical and analytical performance of an automated serological test that identifies S1/S2-neutralizing IgG in COVID-19 patients semiquantitatively. J. Clin. Microbiol. 2020, 58, e01224-20. [Google Scholar] [CrossRef]
- Lewis, M.A. Between Scylla and Charibdis: Oncologic Decision Making in the time of COVID-19. N. Engl. J. Med. 2020, 382, 2285–2287. [Google Scholar] [CrossRef]
- Kutikov, A.; Weinberg, D.S.; Edelman, M.; Horwitz, E.M.; Uzzo, R.G.; Fisher, R.I. A war on two fronts: Cancer care in the time of COVID-19. Ann. Intern. Med. 2020, 172, 756–758. [Google Scholar] [CrossRef] [Green Version]
- Balducci, L. Geriatric Oncology, Sprirituality, and Palliative Care. J. Pain Symptom Manag. 2019, 57, 171–175. [Google Scholar] [CrossRef]
- Desai, A.; Gainor, J.F.; Hegde, A.; Schram, A.M.; Curigliano, G.; Pal, S.; Liu, S.V.; Halmos, B.; Groisberg, R.; Grande, E.; et al. COVID-19 vaccine guidance for patients with cancer participating in oncology clinical trials. Nat. Rev. Clin. Oncol. 2021, 18, 313–319. [Google Scholar] [CrossRef]
- Palich, R.; Veyry, M.; Vozy, A.; Marot, S.; Gligorov, J.; Benderra, M.A.; Maingon, P.; Morand-Joubert, L.; Adjoutah, Z.; Marcelin, A.-G.; et al. High seroconversion rate but low antibody titer after two injections of BNT162b2 (Pfizer-BioNTech) vaccine in patients treated with chemotherapy for solid cancers. Ann. Oncol. 2021, 32, 1294–1295. [Google Scholar] [CrossRef]
- Pimpinelli, F.; Marchesi, F.; Piaggio, G.; Giannarelli, D.; Papa, E.; Falcucci, P.; Pontone, M.; Di Pontone, S.; Laquintana, V.; La Malfa, A.; et al. Fifth-week immunogenicity and safety of anti-SARS-CoV-2 BNT162b2 vaccine in patients with multiple myeloma and myeloproliferative malignancies on active treatment: Preliminary data from a single institution. J. Hematol. Oncol. 2021, 14, 81. [Google Scholar] [CrossRef] [PubMed]
- Herishanu, Y.; Avivi, I.; Aharon, A.; Shefer, G.; Levi, S.; Bronstein, Y.; Morales, M.; Ziv-Baran, T.; Arbel, Y.S.; Scarfò, L.; et al. Efficacy of the BNT162b2 mRNA COVID-19 vaccine in patients with chronic lymphocytic leukemia. Clinical Trials and Observations. Blood 2021, 137, 3165–3173. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Gavriatopoulou, M.; Ntanasis-Stathopoulos, I.; Briasoulis, A.; Gumeni, S.; Malandrakis, P.; Fotiou, D.; Papanagnou, E.-D.; Migkou, M.; Theodorakakou, F.; et al. The neutralizing antibody response psot COVID-19 vaccination in patients with myeloma is highly dependent on the type of anti-myeloma treatment. Blood Cancer J. 2021, 11, 138. [Google Scholar] [CrossRef] [PubMed]
- Iacono, D.; Cerbone, L.; Palombi, L.; Cavalieri, E.; Sperduti, I.; Cocchiara, R.A.; Mariani, B.; Parisi, G.; Garfuli, C. Serological response to COVID-19 vaccination in patients with cancer older than 80 years. J. Geriatr. Oncol. 2021, 12, 123–125. [Google Scholar] [CrossRef]
- Cavanna, L.; Citterio, C.; Biasini, C.; Madaro, S.; Bacchetta, N.; Lis, A.; Cremona, G.; Muroni, M.; Bernuzzi, P.; Cascio, G.L.; et al. COVID-19 vaccines in adult cancer patients with solid tumours undergoing active treatment: Seropositivity and safety. A prospective observational study in Italy. Eur. J. Cancer 2021, 157, 441–449. [Google Scholar] [CrossRef]
- Shmueli, E.S.; Itay, A.; Margalit, O.; Berger, R.; Halperin, S.; Jurkowicz, M.; Levin, E.G.; Levy, I.; Olmer, L.; Regev-Yochay, G.; et al. Efficacy and safety of BNT162b2 vaccination in patients with solid cancer receiving anticancer therapy—A single centre prospective study. Eur. J. Cancer 2021, 157, 124–131. [Google Scholar] [CrossRef]
- Cavanna, L.; Citterio, C.; Toscani, I. COVID-19 Vaccines in Cancer Patients. Seropositivity and Safety. Systematic Review and Meta-Analysis. Vaccines 2021, 9, 1048. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Patients N = 115 (100%) | Positive Serologic Response n = 75 (65.22%) | Negative Serologic Response n = 40 (34.78%) | p-Value |
|---|---|---|---|---|
| Median age |IQR| (range) years | 73 |72–76| (70–86) | 73 (71–76) | 74.35 (72–78) | 0.52 |
| Sex | ||||
| Female n(%) | 64 (55.65) | 46 (71.88) | 18 (28.12) | 0.09 |
| Male n(%) | 51 (44.35) | 29 (56.86) | 22 (43.14) | |
| BMI (kg/m2) median |IQR| | 24.08 |21.86–26.70| | 23.78 |21.5–27.06| | 24.69 |22.68–26.67| | 0.29 |
| Stage | ||||
| Non-metastatic n(%) | 40 (34.78) | 27 (67.50) | 13 (32.50) | 0.71 |
| Metastatic n(%) | 75 (65.22) | 48 (64.00) | 27 (36.00) | |
| IgG T1 (AU/mL) median |IQR| | 55.5 |4.6–268| | 189 |60–280| | 3.8 |3.8–5.55| | <0.01 |
| Cancer | ||||
| Solid tumors | 94 (81.74) | 66 (70.21) | 28 (29.79) | 0.02 |
| Hematological malignances | 21 (18.26) | 9 (42.86) | 12 (57.14) | |
| Primary solid tumor location | ||||
| Gastrointestinal n(%) | 31 (32.98) | 20 (64.52) | 11 (35.48) | 0.18 |
| Genitourinary n(%) | 7 (7.45) | 4 (57.14) | 3 (42.85) | |
| Breast n(%) | 19 (20.21) | 16 (84.21) | 3 (15.79) | |
| Lung n(%) | 16 (17.02) | 10 (62.50) | 6 (37.50) | |
| Gynecological n(%) | 8 (8.51) | 6 (75.00) | 2 (25.00) | |
| Other n(%) | 13 (13.83) | 10 (76.92) | 3 (23.08) | |
| Active anticancer treatment | ||||
| Yes n(%) | 100 (86.95) | 64 (64.00) | 36 (36.00) | 0.50 |
| No n(%) | 15 (13.04) | 11 (73.33) | 4 (26.67) | |
| Treatment | ||||
| Chemotherapy n(%) | 66 (57.39) | 42 (63.64) | 24 (36.36) | 0.68 |
| Immunotherapy n(%) | 17 (14.78) | 9 (52.94) | 8 (47.06) | |
| Hormone therapy n(%) | 4 (3.48) | 3 (75.00) | 1 (25.00) | |
| Biological therapy n(%) | 13 (11.30) | 10 (76.92) | 3 (23.08) | |
| No treatment n(%) | 15 (13.04) | 11 (73.33) | 4 (26.67) | |
| Anti CD-20 | 7(6.09) | 1 (14.29) | 6 (85.71) | 0.01 |
| Line n(%) | ||||
| Neoadiuvant/adiuvant | 13 (13.54) | 8 (61.54) | 5 (38.46) | 0.46 |
| I line | 51 (53.13) | 30 (58.82) | 21 (41.18) | |
| >I line | 32 (33.33) | 23 (71.88) | 9 (28.13) | |
| Comorbidities | ||||
| No n(%) | 41 (35.65) | 25 (60.98) | 16 (39.02) | 0.48 |
| Yes n(%) | 74 (64.35) | 50 (67.57) | 24 (32.43) | |
| Hypertension n(%) | 45 (39.13) | 28 (62.22) | 17 (37.78) | 0.69 |
| Diabetes n(%) | 14 (12.17) | 6 (42.86) | 8 (57.14) | 0.08 |
| Cardiovascular n(%) | 28 (24.35) | 20 (71.43) | 8 (28.57) | 0.43 |
| Endocrine n(%) | 12 (10.43) | 5 (41.67) | 7 (58.33) | 0.11 |
| Other n(%) | 38 (33.04) | 21 (55.26) | 17 (44.74) | 0.12 |
| Laboratory | ||||
| Neutrophil count (×103/μL) median|IQR| | 3.15 |2.4–4.65| | 3.15 |2.36–4.65| | 3.23 |2.49–4.49| | 0.98 |
| Lymphocyte count (×103/μL) median|IQR| | 1.45 |0.9–1.89| | 1.5 |0.9–1.97| | 1.36 |0.87–1.89| | 0.59 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavanna, L.; Proietto, M.; Citterio, C.; Anselmi, E.; Zaffignani, E.; Stroppa, E.M.; Borsotti, M.T.; Contini, A.; Di Girolamo, G.; Quitadamo, V.M.; et al. COVID-19 Vaccination in Cancer Patients Older Than 70 Years Undergoing Active Treatment. Seroconversion Rate and Safety. Vaccines 2022, 10, 164. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10020164
Cavanna L, Proietto M, Citterio C, Anselmi E, Zaffignani E, Stroppa EM, Borsotti MT, Contini A, Di Girolamo G, Quitadamo VM, et al. COVID-19 Vaccination in Cancer Patients Older Than 70 Years Undergoing Active Treatment. Seroconversion Rate and Safety. Vaccines. 2022; 10(2):164. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10020164
Chicago/Turabian StyleCavanna, Luigi, Manuela Proietto, Chiara Citterio, Elisa Anselmi, Elena Zaffignani, Elisa Maria Stroppa, Maria Teresa Borsotti, Andrea Contini, Gabriella Di Girolamo, Vincenzo Matteo Quitadamo, and et al. 2022. "COVID-19 Vaccination in Cancer Patients Older Than 70 Years Undergoing Active Treatment. Seroconversion Rate and Safety" Vaccines 10, no. 2: 164. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10020164