
Humoral Immune Response of SARS-CoV-2 Infection and Anti-SARS-CoV-2 Vaccination in Renal Transplant Recipients

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Recruitments
2.2. Anti-SARS-CoV-2 Spike Protein IgG Titer Measurement
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of Patients
3.2. Seroconversion Rate in Different Groups
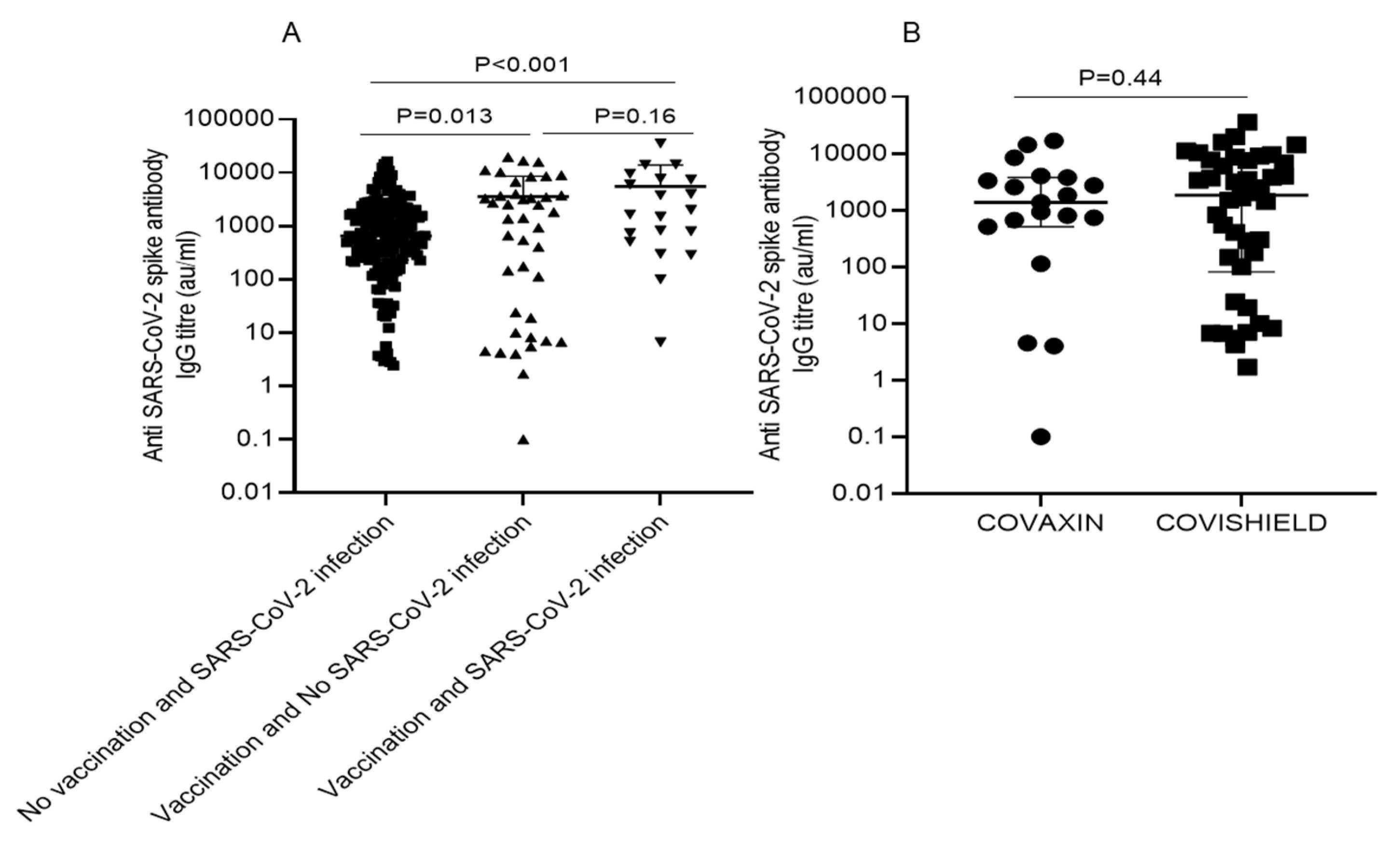
3.3. Anti-SARS-CoV-2 Spike Protein IgG Antibody Titer in Different Groups
3.4. Covaxin™ Versus Covishield™ Seroconversion Rate
3.5. Clinical Variables Associated with Seroconversion
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Benotmane, I.; Gautier-Vargas, G.; Cognard, N.; Olagne, J.; Heibel, F.; Braun-Parvez, L.; Martzloff, J.; Perrin, P.; Moulin, B.; Fafi-Kremer, S.; et al. Low immunization rates among kidney transplant recipients who received 2 doses of the mRNA-1273 SARS-CoV-2 vaccine. Kidney Int. 2021, 99, 1498–1500. [Google Scholar] [CrossRef]
- Singh, A.K.; Phatak, S.R.; Singh, R.; Bhattacharjee, K.; Singh, N.K.; Gupta, A.; Sharma, A. Antibody response after first and second-dose of ChAdOx1-nCOV (CovishieldTM®) and BBV-152 (CovaxinTM®) among health care workers in India: The final results of cross-sectional coronavirus vaccine-induced antibody titre (COVAT) study. Vaccine 2021, 44, 6492–6509. [Google Scholar] [CrossRef]
- Favresse, J.; Bayart, J.-L.; Mullier, F.; Elsen, M.; Eucher, C.; Van Eeckhoudt, S.; Roy, T.; Wieers, G.; Laurent, C.; Dogné, J.-M.; et al. Antibody titres decline 3-month post-vaccination with BNT162b2. Emerg. Microbes Infect. 2021, 10, 1495–1498. [Google Scholar] [CrossRef]
- Rincon-Arevalo, H.; Choi, M.; Stefanski, A.-L.; Halleck, F.; Weber, U.; Szelinski, F.; Jahrsdörfer, B.; Schrezenmeier, H.; Ludwig, C.; Sattler, A.; et al. Impaired humoral immunity to SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients and dialysis patients. Sci. Immunol. 2021, 6, eabj1031. [Google Scholar] [CrossRef]
- Benotmane, I.; Gautier-Vargas, G.; Cognard, N.; Olagne, J.; Heibel, F.; Braun-Parvez, L.; Martzloff, J.; Perrin, P.; Moulin, B.; Fafi-Kremer, S.; et al. Weak anti–SARS-CoV-2 antibody response after the first injection of an mRNA COVID-19 vaccine in kidney transplant recipients. Kidney Int. 2021, 99, 1487–1489. [Google Scholar] [CrossRef]
- Ng, J.H.; Hirsch, J.S.; Wanchoo, R.; Sachdeva, M.; Sakhiya, V.; Hong, S.; Jhaveri, K.D.; Fishbane, S.; Abate, M.; Andrade, H.P.; et al. Outcomes of patients with end-stage kidney disease hospitalized with COVID-19. Kidney Int. 2020, 98, 1530–1539. [Google Scholar] [CrossRef]
- Grupper, A.; Rabinowich, L.; Schwartz, D.; Schwartz, I.F.; Ben-Yehoyada, M.; Shashar, M.; Katchman, E.; Halperin, T.; Turner, D.; Goykhman, Y.; et al. Reduced humoral response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients without prior exposure to the virus. Arab. Archaeol. Epigr. 2021, 21, 2719–2726. [Google Scholar] [CrossRef]
- Del Bello, A.; Marion, O.; Delas, A.; Congy-Jolivet, N.; Colombat, M.; Kamar, N. Acute rejection after anti–SARS-CoV-2 mRNA vaccination in a patient who underwent a kidney transplant. Kidney Int. 2021, 100, 238–239. [Google Scholar] [CrossRef]
- Phylactou, M.; Li, J.-P.O.; Larkin, D.F.P. Characteristics of endothelial corneal transplant rejection following immunisation with SARS-CoV-2 messenger RNA vaccine. Br. J. Ophthalmol. 2021, 105, 893–896. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Coates, P.T.; Rovin, B.H.; Ronco, P. Immune response to SARS-CoV-2 infection and vaccination in patients receiving kidney replacement therapy. Kidney Int. 2021, 99, 1275–1279. [Google Scholar] [CrossRef]
- Wiedinger, K.; Bitsaktsis, C.; Chang, S. Reactivation of human polyomaviruses in immunocompromised states. J. Neurovirol. 2014, 20, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Scadden, J.R.; Sharif, A.; Skordilis, K.; Borrows, R. Polyoma virus nephropathy in kidney transplantation. World J. Transplant. 2017, 7, 329–338. [Google Scholar] [CrossRef]
- Mazziotta, C.; Pellielo, G.; Tognon, M.; Martini, F.; Rotondo, J.C. Significantly Low Levels of IgG Antibodies Against Oncogenic Merkel Cell Polyomavirus in Sera from Females Affected by Spontaneous Abortion. Front. Microbiol. 2021, 12, 789991. [Google Scholar] [CrossRef]
- Keehner, J.; Horton, L.E.; Pfeffer, M.A.; Longhurst, C.A.; Schooley, R.T.; Currier, J.S.; Abeles, S.R.; Torriani, F.J. SARS-CoV-2 Infection after Vaccination in Health Care Workers in California. N. Engl. J. Med. 2021, 384, 1774–1775. [Google Scholar] [CrossRef]
- AdviseDx SARS-CoV-2 IgG II. Available online: https://www.fda.gov/media/146371/download (accessed on 15 October 2021).
- McKay, P.F.; Hu, K.; Blakney, A.K.; Samnuan, K.; Brown, J.C.; Penn, R.; Zhou, J.; Bouton, C.R.; Rogers, P.; Polra, K.; et al. Self-amplifying RNA SARS-CoV-2 lipid nanoparticle vaccine candidate induces high neutralizing antibody titers in mice. Nat. Commun. 2020, 11, 3523. [Google Scholar] [CrossRef]
- Lindstrand, A.; Cherian, T.; Chang-Blanc, D.; Feikin, D.; O’Brien, K.L. The World of Immunization: Achievements, Challenges, and Strategic Vision for the Next Decade. J. Infect. Dis. 2021, 224, S452–S467. [Google Scholar] [CrossRef]
- Benotmane, I.; Gautier, G.; Perrin, P.; Olagne, J.; Cognard, N.; Fafi-Kremer, S.; Caillard, S. Antibody Response after a Third Dose of the mRNA-1273 SARS-CoV-2 Vaccine in Kidney Transplant Recipients with Minimal Serologic Response to 2 Doses. JAMA J. Am. Med Assoc. 2021, 326, 1063. [Google Scholar] [CrossRef]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA COVID-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef]
- Prendecki, M.; Thomson, T.; Clarke, C.L.; Martin, P.; Gleeson, S.; De Aguiar, R.C.; Edwards, H.; Mortimer, P.; McIntyre, S.; Mokreri, D.; et al. Immunological responses to SARS-CoV-2 vaccines in kidney transplant recipients. Lancet 2021, 398, 1482–1484. [Google Scholar] [CrossRef]
- Schmidt, T.; Klemis, V.; Schub, D.; Schneitler, S.; Reichert, M.C.; Wilkens, H.; Sester, U.; Sester, M.; Mihm, J. Cellular immunity predominates over humoral immunity after homologous and heterologous mRNA and vector-based COVID-19 vaccine regimens in solid organ transplant recipients. Am. J. Transplant. 2021, 21, 3990–4002. [Google Scholar] [CrossRef]
- Charmetant, X.; Espi, M.; Benotmane, I.; Heibel, F.; Buron, F.; Gautier-Vargas, G.; Delafosse, M.; Perrin, P.; Koenig, A.; Cognard, N.; et al. Comparison of infected and vaccinated transplant recipients highlights the role of Tfh and neutralizing IgG in COVID-19 protection. MedRxiv 2021, 1–44. [Google Scholar] [CrossRef]
- Benotmane, I.; Vargas, G.G.; Gallais, F.; Gantner, P.; Cognard, N.; Olagne, J.; Velay, A.; Heibel, F.; Braun-Parvez, L.; Martzloff, J.; et al. Strong antibody response after a first dose of a SARS-CoV-2 mRNA-based vaccine in kidney transplant recipients with a previous history of COVID-19. Am. J. Transplant. 2021, 21, 3808–3810. [Google Scholar] [CrossRef]
- Rauch, S.; Jasny, E.; Schmidt, K.E.; Petsch, B. New Vaccine Technologies to Combat Outbreak Situations. Front. Immunol. 2018, 9, 1963. [Google Scholar] [CrossRef] [Green Version]
- Ibarrondo, F.J.; Fulcher, J.A.; Goodman-Meza, D.; Elliott, J.; Hofmann, C.; Hausner, M.A.; Ferbas, K.G.; Tobin, N.H.; Aldrovandi, G.M.; Yang, O.O. Rapid Decay of Anti–SARS-CoV-2 Antibodies in Persons with Mild COVID-19. N. Engl. J. Med. 2020, 383, e74. [Google Scholar] [CrossRef]
- COVID 19 Situations in the WHO South-East Asia Region. Available online: https://covid19.who.int/region/searo/country/in (accessed on 15 October 2021).
- COVID-19 INDIA. Available online: https://www.mohfw.gov.in/ (accessed on 15 October 2021).
- Available online: https://www.covid19india.org/#MapExplorer (accessed on 15 October 2021).
- Frieman, M.; Harris, A.D.; Herati, R.S.; Krammer, F.; Mantovani, A.; Rescigno, M.; Sajadi, M.M.; Simon, V. SARS-CoV-2 vaccines for all but a single dose for COVID-19 survivors. EBioMedicine 2021, 68, 1–2. [Google Scholar] [CrossRef]
- Wang, Z.; Muecksch, F.; Schaefer-Babajew, D.; Finkin, S.; Viant, C.; Gaebler, C.; Hoffmann, H.-H.; Barnes, C.O.; Cipolla, M.; Ramos, V.; et al. Naturally enhanced neutralizing breadth against SARS-CoV-2 one year after infection. Nature 2021, 595, 426–431. [Google Scholar] [CrossRef]
- Mueller, T. Antibodies against severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2) in individuals with and without COVID-19 vaccination: A method comparison of two different commercially available serological assays from the same manufacturer. Clin. Chim. Acta 2021, 518, 9–16. [Google Scholar] [CrossRef]
- Caillard, S.; Thaunat, O. COVID-19 vaccination in kidney transplant recipients. Nat. Rev. Nephrol. 2021, 17, 785–787. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Total | No Vaccination and SARS-CoV-2 Infection (n = 161) | Vaccination and No SARS-CoV-2 Infection (n = 41) | Vaccination and SARS-CoV-2 Infection (n = 20) | p Value | |
|---|---|---|---|---|---|---|
| Age (Years) | 41.23 ± 10.20 | 39.28 ± 9.69 | 45.95 ± 8.22 | 47.30 ± 10.61 | <0.001 * | |
| Gender | M | 195 | 142 | 35 | 18 | 0.83 *** |
| F | 27 | 19 | 6 | 2 | ||
| Post-transplant interval in Month (range) | 74.33 (2.0–276) | 65.0 (2.0–216.0) | 96 (20.0–240.0) | 94.10 (12.0–276.0) | 0.04 ** | |
| BMI(Kg/M2) | 24.28 ± 5.21 | 23.76 ± 5.20 | 25.32 ± 4.51 | 26.36 ± 6.04 | 0.04 * | |
| Hemoglobin (g/dL) | 12.98 ± 1.82 | 13.05 ± 1.88 | 13.03 ± 1.45 | 12.28 ± 1.96 | 0.19 * | |
| Baseline serum creatinine (mg/dL) | 1.01 ± 0.37 | 1.02 ± 0.37 | 0.95 ± 0.33 | 1.05 ± 0.40 | 0.48 * | |
| Serum creatinine (mg/dL) | 1.41 ± 0.71 | 1.46 ± 0.79 | 1.20 ± 0.34 | 1.40 ± 0.49 | 0.11 * | |
| TLC (×103/µL) | 8.32 ± 2.48 | 8.25 ± 2.61 | 8.57 ± 1.86 | 8.41 ± 2.53 | 0.75 * | |
| BUN (mg/dL) | 17.85 (5.80–59.80) | 17.80 (5.80–59.80) | 16.0(7.16–35.0) | 20.20(6.60–48.10) | 0.32 ** | |
| eGFR (mL/min) | 70.13 ± 33.31 | 69.33 ± 36.28 | 74.56 ± 22.01 | 67.45 ± 27.23 | 0.62 * | |
| Tacrolimus level (µg/L) | 5.20 (2.0–16.90) | 5.40 (2.10–16.90) | 4.85 (2.40–11.80) | 4.80 (2.0–16.60) | 0.48 ** | |
| Systolic BP (mmhg) | 130.88 ± 14.47 | 130.55 ± 14.86 | 133.27 ± 13.68 | 128.65 ± 12.82 | 0.43 * | |
| Diastolic BP (mmhg) | 80.73 ± 9.90 | 80.82 ± 9.95 | 80.39 ± 10.27 | 80.75 ± 9.08 | 0.97 * | |
| Vaccine Brand recipients | Covishiled | 42 | 0 | 26 | 16 | <0.001 *** |
| Covaxin | 19 | 0 | 15 | 4 | ||
| Patient blood group | A+ | 44 | 44 | 4 | 6 | 0.13 *** |
| B+ | 75 | 81 | 20 | 4 | ||
| O+ | 64 | 47 | 10 | 7 | ||
| AB+ | 29 | 19 | 7 | 3 | ||
| Induction regimen | None | 104 | 66 | 25 | 13 | 0.028 *** |
| Basiliximab | 93 | 78 | 10 | 5 | ||
| ATG | 25 | 17 | 6 | 2 | ||
| MMF+ Steroid+ | Tacrolimus | 212 | 156 | 38 | 18 | 0.23 *** |
| Cyclosporin | 10 | 5 | 3 | 2 | ||
| Sr. No | No Vaccination and SARS-CoV-2 Infection (n = 161) | Vaccination and No SARS-CoV-2 Infection (n = 41) | Vaccination and SARS-CoV-2 Infection (n = 20) | p Value | |||
|---|---|---|---|---|---|---|---|
| Median and IQR of antibody titer (AU/mL) | 647.0 (IQR: 229.1–1819.65) a | 1409.0 (IQR: 14.50–3882.55) b | 1831.30 (IQR: 565.25–7644.65) c | a vs. b, p = 0.013 a vs. c, p < 0.001 b vs. c, p = 0.16 | |||
| Over all anti-SARS-CoV-2 spike protein antibody seroconversion | Yes (n = 145; 90.06%) | No (n = 16; 9.93%) | Yes (n = 29; 70.73%) | No (n = 12; 29.26%) | Yes (n = 19; 95.0%) | No (n = 1; 5%) | 0.002 |
| Characteristics | Seroconversion | |||
|---|---|---|---|---|
| Yes | No | p Value | ||
| Post-transplant interval (months) associated seroconversion | 2–60 | 73 (87.95%) | 10 (12.04%) | 0.71 |
| 60–120 | 72 (84.7%) | 13 (15.3%) | ||
| 120–180 | 31 (86.1%) | 5 (13.8%) | ||
| >180 | 17 (94.4%) | 1 (5.5%) | ||
| BMI (kg/m2) associated seroconversion | <18.4 | n = 37 (90.2%) | n = 4 (9.7%) | 0.23 |
| 18.4–24.99 | n = 72 (82.75%) | n = 15 (17.24%) | ||
| 25.29–29.99 | n = 62 (92.5%) | n = 5 (7.4%) | ||
| >30 | n = 22 (81.5%) | n = 5 (18.51%) | ||
| Age-wise (Year) seroconversion $ | 18–45 | n = 130 (90.27%) | n = 14 (9.72%) | 0.074 |
| 46–60 | n= 56 (82.35%) | n = 12 (17.46%) | ||
| >60 | n = 7 (70%) | n = 3 (30%) | ||
| Vaccine brand associated seroconversion | Covishield™ | n= 32 (76.19%) | n = 10 (23.80%) | 0.003 |
| Titer: 1831.10 (81.26–7522.56) AU/mL | ||||
| Covaxin™ | n = 16 (84.21%) | n = 3 (15.78%) | 0.016 | |
| Titer: 1373.90 (IQR: 507.80–3765.10) AU/mL | ||||
| Blood group associated seroconversion | A+ | n = 47 (87.03%) | n = 7 (12.96%) | 0.488 |
| B+ | n = 62 (82.66%) | n = 13 (17.33%) | ||
| AB+ | n = 27 (93.10%) | n = 2 (6.89%) | ||
| O+ | n = 57 (89.06%) | n = 7 (10.93%) | ||
| Immunosuppression associated seroconversion | Tacrolimus + MMF + Steroid | n = 184 (86.79%) | n = 28 (13.20%) | 1.00 |
| Cyclosporin + MMF + Steroid | n = 9 (90%) | n = 1 (10%) | ||
| Serum creatinine | <1.4 | 120 (87.59%) | 17 (12.40%) | 0.83 |
| >1.4 | 73 (85.88%) | 12 (14.11%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prasad, N.; Yadav, B.; Singh, M.; Gautam, S.; Bhadauria, D.; Patel, M.; Kushwaha, R.; Yadav, D.; Singh, A.; Yachha, M.; et al. Humoral Immune Response of SARS-CoV-2 Infection and Anti-SARS-CoV-2 Vaccination in Renal Transplant Recipients. Vaccines 2022, 10, 385. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10030385
Prasad N, Yadav B, Singh M, Gautam S, Bhadauria D, Patel M, Kushwaha R, Yadav D, Singh A, Yachha M, et al. Humoral Immune Response of SARS-CoV-2 Infection and Anti-SARS-CoV-2 Vaccination in Renal Transplant Recipients. Vaccines. 2022; 10(3):385. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10030385
Chicago/Turabian StylePrasad, Narayan, Brijesh Yadav, Mantabya Singh, Sonam Gautam, Dharmendra Bhadauria, Manas Patel, Ravi Kushwaha, Deependra Yadav, Ankita Singh, Monika Yachha, and et al. 2022. "Humoral Immune Response of SARS-CoV-2 Infection and Anti-SARS-CoV-2 Vaccination in Renal Transplant Recipients" Vaccines 10, no. 3: 385. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10030385