
Vaccination Attitudes and Experiences of Medical Doctors in Croatia amid the COVID-19 Pandemic: A Social Roles Conflict?

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
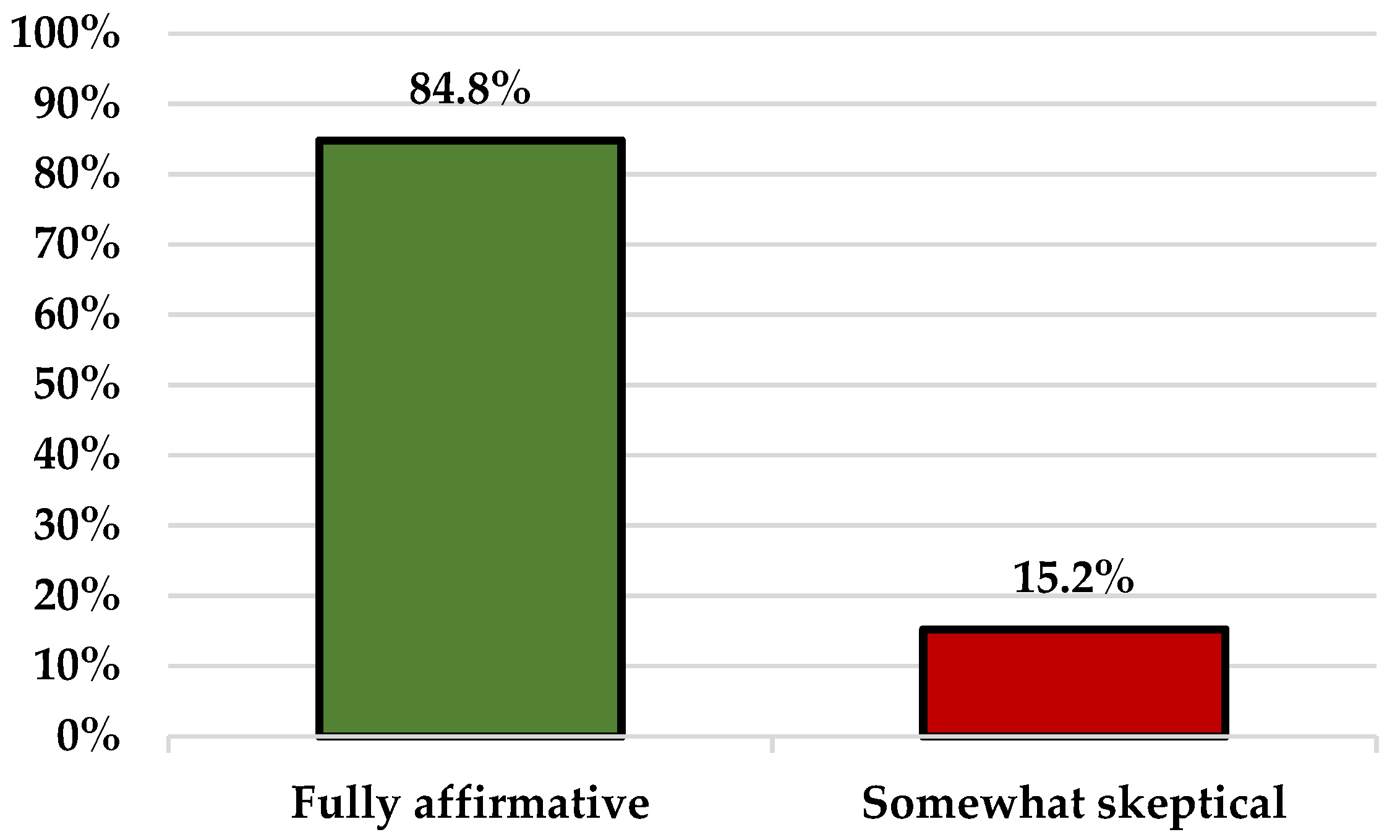
3.1. Overall Attitudes towards Vaccination
3.2. Mandatory Immunization Program
3.3. Vaccination Side-Effects
3.4. Communication with Vaccine-Hesitant Patients
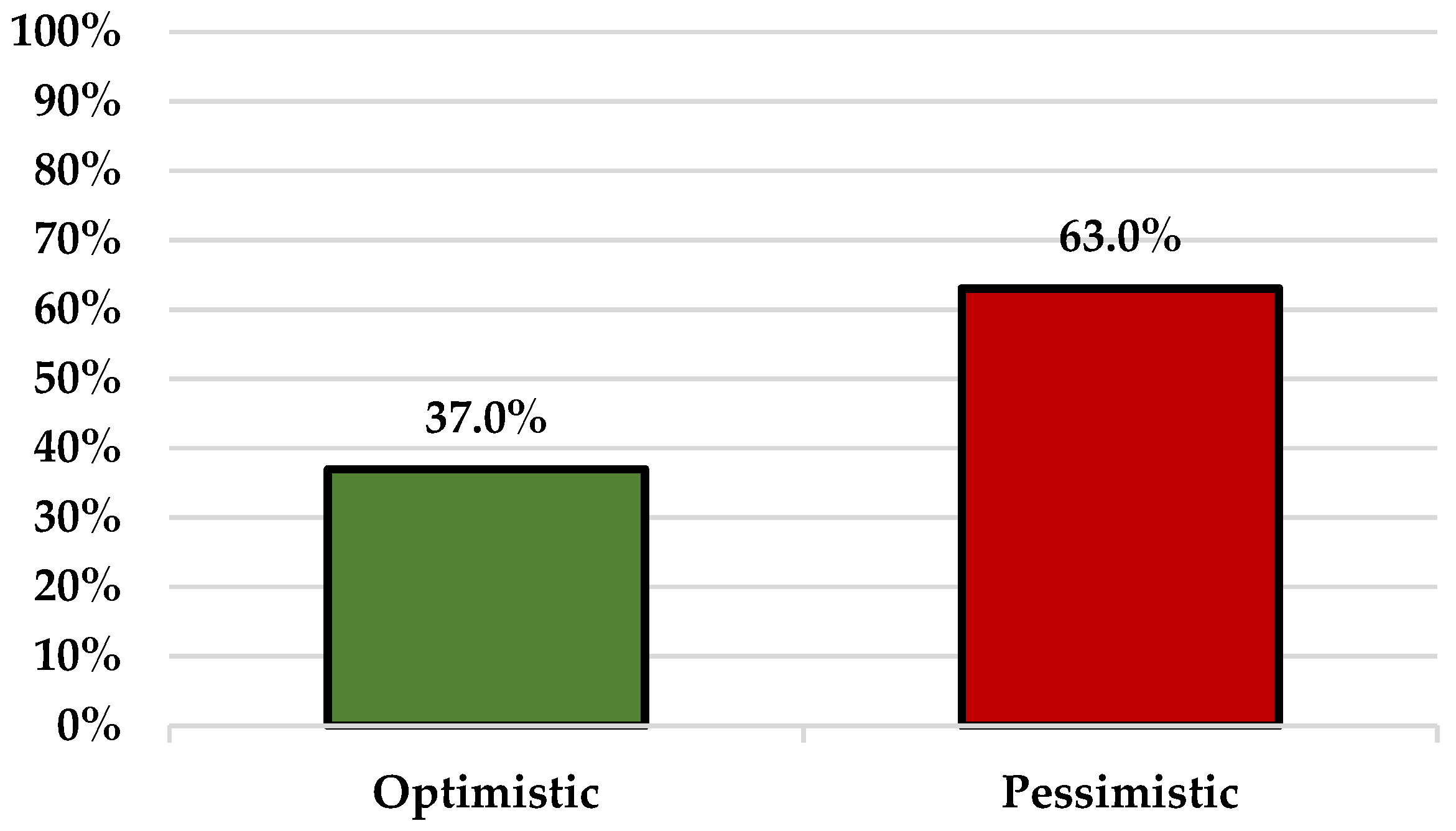
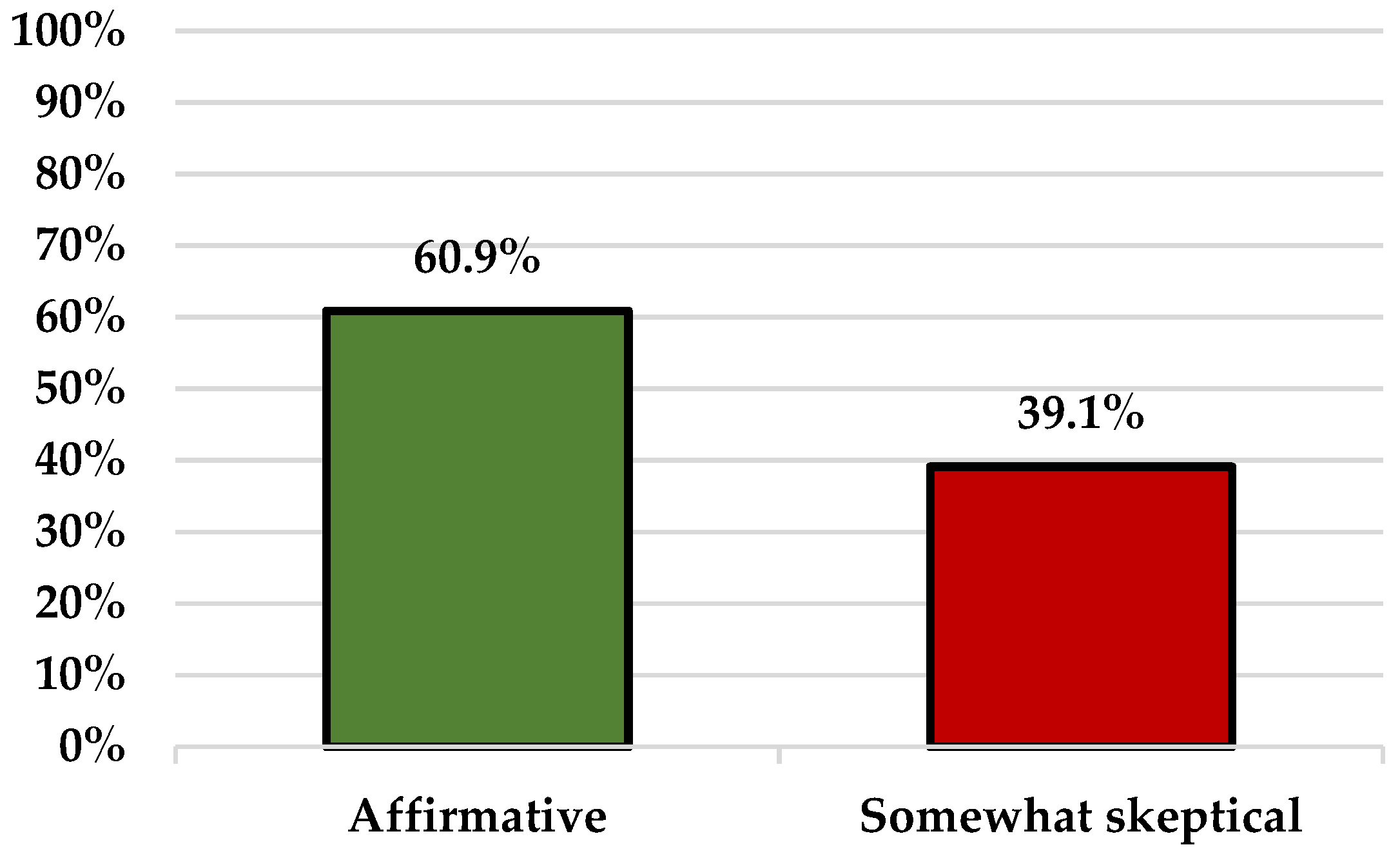
3.5. COVID-19 Vaccination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Vaccine Action Plan. Decade of vaccine collaboration. Vaccine 2013, 31, B5–B31. [Google Scholar] [CrossRef] [PubMed]
- Tešović, G. Childhood vaccinations in Croatia. Period. Biol. 2012, 114, 149–166. [Google Scholar]
- Kaić, B.; Gjenero-Margan, I.; Brzović, M.; Lakošeljac, D.; Aleraj, B.; Nemeth-Blažić, T.; Kolarić, B.; Macolić-Šarinić, V.; Šimunović, A.; Pavlić, J. Vaccine regulations in Croatia. Coll. Antropol. 2007, 31, 117–120. [Google Scholar]
- Lovrić Makarić, Z.; Kolarić, B.; Tomljenović, M.; Posavec, M. Attitudes and beliefs related to childhood vaccinations among parents of 6 years old children in Zagreb, Croatia. Vaccine 2018, 36, 7530–7535. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Implementation Program of Mandatory Vaccination in the Republic of Croatia in 2021; Ministry of Health: Zagreb, Croatia, 2020.
- Ministry of Health. Ordinance on the manner of immunization, seroprophylaxis, chemoprophylaxis against infectious diseases and persons who must be subjected to this obligation. In Official Gazette of the Republic of Croatia 103/2013; Narodne Novine Plc.: Zagreb, Croatia, 2013; p. 2322. [Google Scholar]
- Ministry of Health. Ordinance of amendment of ordinance on the manner of immunization, seroprophylaxis, chemoprophylaxis against infectious diseases and persons who must be subjected to this obligation. In Official Gazette of the Republic of Croatia 144/2020; Narodne Novine Plc.: Zagreb, Croatia, 2020; p. 2777. [Google Scholar]
- Ministry of Health. The law on protection of the population from infectious diseases. In Official Gazettes of the Republic of Croatia 79/2007, 113/2008, 43/2009, 130/2017, 114/2018, 47/2020, 134/2020, 143/2021; Narodne Novine Plc.: Zagreb, Croatia, 2021; p. 2436. [Google Scholar]
- Croatian Institute for Public Health. Croatian Health Statistics Yearbook 2019. Available online: http://ghdx.healthdata.org/record/croatia-health-statistics-yearbook-2019 (accessed on 28 February 2022).
- Vaccination Report of the Croatian Institute of Public Health (In Croatian). Available online: https://www.koronavirus.hr/uploads/Izvjestaj_o_cijepljenju_2602_docx_3f9b5fe63a.pdf (accessed on 28 February 2022).
- Dubé, E. Addressing vaccine hesitancy: The crucial role of healthcare providers. Clin. Microbiol. Infect. 2017, 23, 279–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Kang, J.; Mao, Y.; Zheng, P.; Abdullah, A.S.; Wu, G.; Wang, F. Investigating HPV- and HPV Vaccine-Related Knowledge, Perceptions, and Information Sources among Health Care Providers in Three Big Cities in China. Vaccines 2020, 8, 499. [Google Scholar] [CrossRef]
- Karafillakis, E.; Dinca, I.; Apfel, F.; Cecconi, S.; Wűrz, A.; Takacs, J.; Suk, J.; Celentano, L.P.; Kramarz, P.; Larson, H.J. Vaccine hesitancy among healthcare workers in Europe: A qualitative study. Vaccine 2016, 34, 5013–5020. [Google Scholar] [CrossRef]
- Verger, P.; Fressard, L.; Collange, F.; Gautier, A.; Jestin, C.; Launay, O.; Raude, J.; Pulcini, C.; Peretti-Watel, P. Vaccine Hesitancy Among General Practitioners and Its Determinants during Controversies: A National Cross-sectional Survey in France. EBioMedicine 2015, 2, 891–897. [Google Scholar] [CrossRef] [Green Version]
- Paterson, P.; Meurice, F.; Stanberry, L.R.; Glismann, S.; Rosenthal, S.L.; Larson, H.J. Vaccine hesitancy and healthcare providers. Vaccine 2016, 34, 6700–6706. [Google Scholar] [CrossRef] [Green Version]
- Barrière, J.; Vanjak, D.; Kriegel, I.; Otto, J.; Peyrade, F.; Estève, M.; Chamorey, E. Acceptance of the 2009 A(H1N1) influenza vaccine among hospital workers in two French cancer centers. Vaccine 2010, 28, 7030–7034. [Google Scholar] [CrossRef]
- Torun, S.D.; Torun, F. Vaccination against pandemic influenza A/H1N1 among healthcare workers and reasons for refusing vaccination in Istanbul in last pandemic alert phase. Vaccine 2010, 28, 5703–5710. [Google Scholar] [CrossRef] [PubMed]
- Omoleke, S.A.; Ajibola, O.; Omisakin, O.A.; Umeh, G.C. Vaccine hesitancy among medical practitioners. Sahel Med. J. 2020, 23, 126–131. [Google Scholar] [CrossRef]
- Paoli, S.; Lorini, C.; Puggelli, F.; Sala, A.; Grazzini, M.; Paolini, D.; Bonanni, P.; Bonaccorsi, G. Assessing vaccine hesitancy among healthcare workers: A cross-sectional study at an Italian paediatric hospital and the development of a healthcare worker’s vaccination compliance index. Vaccines 2019, 7, 201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Awaidy, S.T.; Al Mayahi, Z.K.; Kaddoura, M.; Mahomed, O.; Lahoud, N.; Abubakar, A.; Zaraket, H. Influenza vaccination hesitancy among healthcare workers in south al batinah governorate in Oman: A cross-sectional study. Vaccines 2020, 8, 661. [Google Scholar] [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 Vaccine in Southeast Asia: A Cross-Sectional Study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef]
- Marcu, A.; Rubinstein, H.; Michie, S.; Yardley, L. Accounting for personal and professional choices for pandemic influenza vaccination amongst English healthcare workers. Vaccine 2015, 3, 2267–2272. [Google Scholar] [CrossRef]
- McCarthy, E.M.; Azeez, M.A.; Fitzpatrick, F.M.; Donnelly, S. Knowledge, attitudes, and clinical practice of rheumatologists in vaccination of the at-risk rheumatology patient population. J. Clin. Rheumatol. 2012, 18, 237–241. [Google Scholar] [CrossRef]
- Austvoll-Dahlgren, A.; Helseth, S. Public health nurses’ barriers and facilitators to the use of research in consultations about childhood vaccinations. Scand. J. Caring. Sci. 2012, 26, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Poland, G.A. The 2009–2010 influenza pandemic: Effects on pandemic and seasonal vaccine uptake and lessons learned for seasonal vaccination campaigns. Vaccine 2010, 28, D3–D13. [Google Scholar] [CrossRef]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.L. Barriers of influenza vaccination intention and behavior—A systematic review of influenza vaccine hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.A.; Roma, P.; Da Molin, G.; Diella, G.; Montagna, M.T.; Ferracuti, S.; Liguori, G.; Orsi, G.B.; Napoli, C. Acceptance of COVID-19 Vaccination in the Elderly: A Cross-Sectional Study in Southern Italy. Vaccines 2021, 9, 1222. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. COVID-19 vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Dror, A.; Eisenbach, N.; Taiber, S.; Morozov, N.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine Hesitancy: The Next Challenge in the Fight Against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Kose, S.; Mandiracioglu, A.; Sahin, S.; Kaynar, T.; Karbus, O.; Ozbel, Y. Vaccine hesitancy of the COVID-19 by health care personnel. Int. J. Clin. Pract. 2021, 75, e13917. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Chan, E.Y.Y.; Yeoh, E.K.; Wong, S.Y.S. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine 2020, 38, 7049–7056. [Google Scholar] [CrossRef]
- Ledda, C.; Costantino, C.; Cuccia, M.; Maltezou, H.C.; Rapisarda, V. Attitudes of Healthcare Personnel towards Vaccinations before and during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 2703. [Google Scholar] [CrossRef]
- Abrams, K.M.; Wang, Z.; Song, Y.J.; Galindo-Gonzalez, S. Data Richness Trade-Offs between Face-to-Face, Online Audiovisual, and Online Text-Only Focus Groups. Soc. Sci. Comput. Rev. 2015, 33, 80–96. [Google Scholar] [CrossRef]
- Boydell, N.; Fergie, G.; McDaid, L.; Hilton, S. Avoiding pitfalls and realising opportunities: Reflecting on issues of sampling and recruitment for online focus groups. Int. J. Qual. Methods 2014, 13, 206–223. [Google Scholar] [CrossRef] [Green Version]
- Flynn, R.; Albrecht, L.; Scott, S.D. Two approaches to focus group data collection for qualitative health research: Maximizing resources and data quality. Int. J. Qual. Methods 2018, 17, 1609406917750781. [Google Scholar] [CrossRef]
- Rupert, D.J.; Poehlman, J.A.; Hayes, J.J.; Ray, S.E.; Moultrie, R.R. Virtual versus in-person focus groups: Comparison of costs, recruitment, and participant logistics. J. Med. Internet Res. 2017, 19, e6980. [Google Scholar] [CrossRef]
- Brüggen, E.; Willems, P. A Critical Comparison of Offline Focus Groups, Online Focus Groups and E-Delphi. Int. J. Mark. Res. 2009, 51, 1–15. [Google Scholar] [CrossRef]
- Vasileiou, K.; Barnett, J.; Thorpe, S.; Young, T. Characterising and justifying sample size sufficiency in interview-based studies: Systematic analysis of qualitative health research over a 15-year period. BMC Med. Res. Methodol. 2018, 18, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guest, G.; Namey, E.; McKenna, K. How Many Focus Groups Are Enough? Building an Evidence Base for Nonprobability Sample Sizes. Field Methods 2017, 29, 3–22. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Tracy, S.J. Qualitative quality: Eight a ”big-tent” criteria for excellent qualitative research. Qual. Inq. 2010, 16, 837–851. [Google Scholar] [CrossRef] [Green Version]
- Musa, S.; Skrijelj, V.; Kulo, A.; Habersaat, K.B.; Smjecanin, M.; Primorac, E.; Becirovic, D.; Jackson, C. Identifying barriers and drivers to vaccination: A qualitative interview study with health workers in the Federation of Bosnia and Herzegovina. Vaccine 2020, 38, 1906–1914. [Google Scholar] [CrossRef]
- Hollmeyer, H.G.; Hayden, F.; Poland, G.; Buchholz, U. Influenza vaccination of health care workers in hospitals—A review of studies on attitudes and predictors. Vaccine 2009, 27, 3935–3944. [Google Scholar] [CrossRef]
- Karlsson, L.C.; Lewandowsky, S.; Antfolk, J.; Salo, P.; Lindfelt, M.; Oksanen, T.; Kivimäki, M.; Soveri, A. The association between vaccination confidence, vaccination behavior, and willingness to recommend vaccines among Finnish healthcare workers. PLoS ONE 2019, 14, e0224330. [Google Scholar] [CrossRef]
- Napolitano, F.; D’Alessandro, A.; Angelillo, I.F. Investigating Italian parents’ vaccine hesitancy: A cross-sectional survey. Hum. Vaccines Immunother. 2018, 14, 1558–1565. [Google Scholar] [CrossRef] [Green Version]
- Collange, F.; Zaytseva, A.; Pulcini, C.; Bocquier, A.; Verger, P. Unexplained variations in general practitioners’ perceptions and practices regarding vaccination in France. Eur. J. Public Health 2019, 29, 2–8. [Google Scholar] [CrossRef]
- Lutringer-Magnin, D.; Kalecinski, J.; Barone, G.; Leocmach, Y.; Regnier, V.; Jacquard, A.C.; Soubeyrand, B.; Vanhems, P.; Chauvin, F.; Lasset, C. Human papillomavirus (HPV) vaccination: Perception and practice among French general practitioners in the year since licensing. Vaccine 2011, 29, 5322–5328. [Google Scholar] [CrossRef] [PubMed]
- Valour, F.; Bénet, T.; Chidiac, C. Pandemic A(H1N1)2009 influenza vaccination in Lyon University Hospitals, France: Perception and attitudes of hospital workers. Vaccine 2013, 31, 592–595. [Google Scholar] [CrossRef] [PubMed]
- Ciardi, F.; Menon, V.; Jensen, J.L.; Shariff, M.A.; Pillai, A.; Venugopal, U.; Kasubhai, M.; Dimitrov, V.; Kanna, B.; Poole, B.D. Knowledge, Attitudes and Perceptions of COVID-19 Vaccination among Healthcare Workers of an Inner-City Hospital in New York. Vaccines 2021, 9, 516. [Google Scholar] [CrossRef] [PubMed]
- Fotiadis, K.; Dadouli, K.; Avakian, I.; Bogogiannidou, Z.; Mouchtouri, V.A.; Gogosis, K.; Speletas, M.; Koureas, M.; Lagoudaki, E.; Kokkini, S.; et al. Factors Associated with Healthcare Workers’ (HCWs) Acceptance of COVID-19 Vaccinations and Indications of a Role Model towards Population Vaccinations from a Cross-Sectional Survey in Greece, May 2021. Int. J. Environ. Res. Public Health 2021, 18, 10558. [Google Scholar] [CrossRef] [PubMed]
- Fakonti, G.; Kyprianidou, M.; Toumbis, G.; Giannakou, K. Attitudes and Acceptance of COVID-19 Vaccination among Nurses and Midwives in Cyprus: A Cross-Sectional Survey. Front. Public Health 2021, 9, 656138. [Google Scholar] [CrossRef]
- Healy, C.M.; Pickering, L.K. How to communicate with vaccine-hesitant parents. Pediatrics 2011, 127, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Emanuel, E.J.; Emanuel, L.L. Four models of the physician-patient relationship. JAMA 1992, 267, 2221–2226. [Google Scholar] [CrossRef]
- Hough-Telford, C.; Kimberlin, D.W.; Aban, I.; Hitchcock, W.P.; Almquist, J.; Kratz, R.; O’Connor, K.G. Vaccine Delays, Refusals, and Patient Dismissals: A Survey of Pediatricians. Pediatrics 2016, 138, e20162127. [Google Scholar] [CrossRef] [Green Version]
- Levinson, W.; Lesser, C.S.; Epstein, R.M. Developing physician communication skills for patient-centered care. Health Aff. 2010, 29, 1310–1318. [Google Scholar] [CrossRef]
- Leask, J.; Kinnersley, P.; Jackson, C.; Cheater, F.; Bedford, H.; Rowles, G. Communicating with parents about vaccination: A framework for health professionals. BMC Pediatr. 2012, 12, 154. [Google Scholar] [CrossRef]
- Shon, E.J.; Wells, A. Effects of Patient-Centered Communication on Influenza Vaccination and Self-Reported General Health Status among Asian Americans: A Comparison Model for Young/Middle-Aged and Older Adults. J. Aging Health 2020, 32, 1409–1418. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.C.; Jones, A.L.; Feemster, K.A.; Fiks, A.G. HPV vaccine decision making in pediatric primary care: A semi-structured interview study. BMC Pediatr. 2011, 11, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Opel, D.J.; Heritage, J.; Taylor, J.A.; Mangione-Smith, R.; Salas, H.S.; Devere, V.; Zhou, C.; Robinson, J.D. The architecture of provider-parent vaccine discussions at health supervision visits. Pediatrics 2013, 132, 1037–1046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moss, J.L.; Reiter, P.L.; Rimer, B.K.; Brewer, N.T. Collaborative patient-provider communication and uptake of adolescent vaccines. Soc. Sci. Med. 2016, 159, 100–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Napolitano, F.; Navaro, M.; Vezzosi, L.; Santagati, G.; Angelillo, I.F. Primary care pediatricians’ attitudes and practice towards hpv vaccination: A nationwide survey in Italy. PLoS ONE 2018, 13, e0194920. [Google Scholar] [CrossRef]
- Smith, L.E.; Amlôt, R.; Weinman, J.; Yiend, J.; Rubin, G.J. A systematic review of factors affecting vaccine uptake in young children. Vaccine 2017, 35, 6059–6069. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.; Zhang, T.; Chen, L.; Yi, B.; Hao, X.; Zhou, S.; Zhang, R.; Greene, C. Increasing seasonal influenza vaccination among high risk groups in China: Do community healthcare workers have a role to play? Vaccine 2017, 35, 4060–4063. [Google Scholar] [CrossRef]
- Napolitano, F.; Napolitano, P.; Angelillo, I.F. Seasonal influenza vaccination in pregnant women: Knowledge, attitudes, and behaviors in Italy. BMC Infect. Dis. 2017, 17, 48. [Google Scholar] [CrossRef] [Green Version]
- Berry, N.J.; Henry, A.; Danchin, M.; Trevena, L.J.; Willaby, H.W.; Leask, J. When parents won’t vaccinate their children: A qualitative investigation of australian primary care providers’ experiences. BMC Pediatr. 2017, 17, 19. [Google Scholar] [CrossRef] [Green Version]
- Deml, M.J.; Buhl, A.; Notter, J.; Kliem, P.; Huber, B.M.; Pfeiffer, C.; Burton-Jeangros, C.; Tarr, P.E. ‘Problem patients and physicians’ failures’: What it means for doctors to counsel vaccine hesitant patients in Switzerland. Soc. Sci. Med. 2020, 255. [Google Scholar] [CrossRef]
- Zandbelt, L.C.; Smets, E.M.; Oort, F.J.; Godfried, M.H.; de Haes, H.C. Determinants of physicians’ patient-centred behaviour in the medical specialist encounter. Soc. Sci. Med. 2006, 63, 899–910. [Google Scholar] [CrossRef] [PubMed]
- Reich, J.A. Calling the Shots: Why Parents Reject Vaccines; New York University Press: New York, NY, USA, 2018. [Google Scholar]
- Jagosh, J.; Donald Boudreau, J.; Steinert, Y.; Macdonald, M.E.; Ingram, L. The importance of physician listening from the patients’ perspective: Enhancing diagnosis, healing, and the doctor-patient relationship. Patient Educ. Couns. 2011, 85, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Wanzer, M.B.; Booth-Butterfield, M.; Gruber, K. Perceptions of health care providers’ communication: Relationships between patient-centered communication and satisfaction. Health Commun. 2004, 16, 363–383. [Google Scholar] [CrossRef]
- Clark, N.M.; Cabana, M.D.; Nan, B.; Gong, Z.M.; Slish, K.K.; Birk, N.A.; Kaciroti, N. The clinician-patient partnership paradigm: Outcomes associated with physician communication behavior. Clin. Pediatr. 2008, 47, 49–57. [Google Scholar] [CrossRef]
- Henrikson, N.B.; Opel, D.J.; Grothaus, L.; Nelson, J.; Scrol, A.; Dunn, J.; Faubion, T.; Roberts, M.; Marcuse, E.K.; Grossman, D.C. Physician communication training and parental vaccine hesitancy: A randomized trial. Pediatrics 2015, 136, 70–79. [Google Scholar] [CrossRef] [Green Version]
- Wolfensberger, M.; Wrigley, A. Trust in Medicine. Its Nature, Justification, Significance, and Decline; Cambridge University Press: Cambridge, UK, 2019. [Google Scholar]
- Giddens, A. Consequences of Modernity; Polity Press: Cambridge, UK, 1990. [Google Scholar]
- Giddens, A. Runaway World: How Globalization Is Reshaping Our Lives, 2nd ed.; Profile Books: London, UK, 2002. [Google Scholar]
- Beck, U. Risk Society: Towards a New Modernity; Sage Publications: London, UK, 1992. [Google Scholar]
- Beck, U. World Risk Society; Polity Press: Cambridge, UK, 2000. [Google Scholar]
- Luhmann, N. Trust: Making and Breaking Cooperative Relations’. In Familiarity, Confidence, Trust: Problems and Alternatives; Gambetta, D., Ed.; Basil Blackwell: New York, NY, USA, 1988; pp. 94–107. [Google Scholar]
- Calnan, M.; Douglass, T. Hopes, hesitancy and the risky business of vaccine development. Health Risk Soc. 2020, 22, 291–304. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Focus Group Characteristics | Focus Group 1 (FG1) N = 18 | Focus Group 2 (FG2) N = 17 | Focus Group 3 (FG3) N = 11 |
|---|---|---|---|
| Age (years) Mean ± SD * | 44.3 ± 7.7 | 45.9 ± 5.5 | 42.8 ± 9.7 |
| Gender Male:Female | 5:13 | 8:9 | 5:6 |
| Participants job description | primary care pediatricians, general practitioners | secondary care pediatricians, other medical specialists | epidemiologists, other public health specialists |
| Participants institution | healthcare centers | general and county hospitals, clinical hospitals, and clinical hospital centers | county public health institutes and Croatian Institute of Public Health |
| Topic Number | Topic Content |
|---|---|
| 1 | Overall attitudes towards vaccination |
| 2 | Mandatory immunization program |
| 3 | Vaccination side-effects |
| 4 | Communication with vaccine-hesitant patients |
| 5 | COVID-19 vaccination |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miskulin, M.; Mujkic, A.; Miskulin, I.; Makaric, Z.L.; Kovacevic, E.; Pintaric, L.; Pavic, Z. Vaccination Attitudes and Experiences of Medical Doctors in Croatia amid the COVID-19 Pandemic: A Social Roles Conflict? Vaccines 2022, 10, 399. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10030399
Miskulin M, Mujkic A, Miskulin I, Makaric ZL, Kovacevic E, Pintaric L, Pavic Z. Vaccination Attitudes and Experiences of Medical Doctors in Croatia amid the COVID-19 Pandemic: A Social Roles Conflict? Vaccines. 2022; 10(3):399. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10030399
Chicago/Turabian StyleMiskulin, Maja, Aida Mujkic, Ivan Miskulin, Zvjezdana Lovric Makaric, Emma Kovacevic, Ljiljana Pintaric, and Zeljko Pavic. 2022. "Vaccination Attitudes and Experiences of Medical Doctors in Croatia amid the COVID-19 Pandemic: A Social Roles Conflict?" Vaccines 10, no. 3: 399. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10030399