
Higher Antibody Concentrations in U.S. Health Care Workers Associated with Greater Reactogenicity Post-Vaccination

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
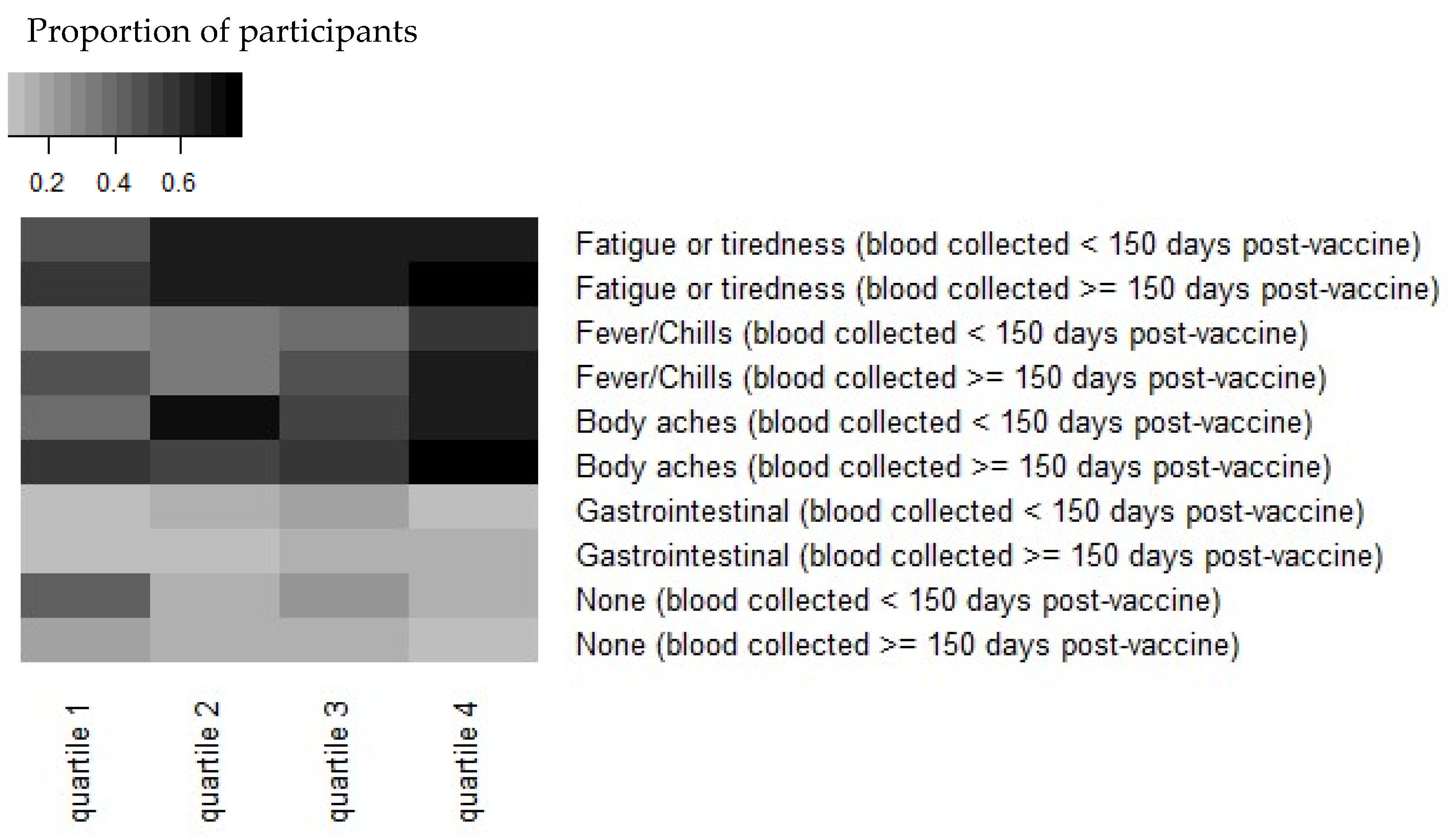
3.1. Post-Vaccine Reactogenicity
3.2. Antibody Levels over Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The New York Times. COVID Vaccinations Tracker. 2021. Available online: https://www.nytimes.com/interactive/2021/world/covid-vaccinations-tracker.html (accessed on 30 March 2022).
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Jackson, L.A.; Anderson, E.J.; Rouphael, N.G.; Roberts, P.C.; Makhene, M.; Coler, R.N.; McCullough, M.P.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; et al. An mRNA Vaccine against SARS-CoV-2—Preliminary Report. N. Engl. J. Med. 2020, 383, 1920–1931. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Prince, H.E.; Givens, T.S.; Lapé-Nixon, M.; Clarke, N.J.; Schwab, D.A.; Batterman, H.J.; Jones, R.S.; Meyer, W.A., III; Kapoor, H.; Rowland, C.M.; et al. Detection of SARS-CoV-2 IgG Targeting Nucleocapsid or Spike Protein by Four High-Throughput Immunoassays Authorized for Emergency Use. J. Clin. Microbiol. 2020, 58, e01742-20. [Google Scholar] [CrossRef] [PubMed]
- Theel, E.S.; Johnson, P.W.; Kunze, K.L.; Wu, L.; Gorsh, A.P.; Granger, D.; Roforth, M.M.; Jerde, C.R.; Lasho, M.; Andersen, K.J.; et al. SARS-CoV-2 Serologic Assays Dependent on Dual-Binding Demonstrate Diverging Kinetics Relative to Other Antibody Detection Methods. J. Clin. Microbiol. 2021, 59, e0123121. [Google Scholar] [CrossRef] [PubMed]
- Favresse, J.; Eucher, C.; Elsen, M.; Gillot, C.; Van Eeckhoudt, S.; Dogné, J.M.; Douxfils, J. Persistence of anti-SARS-CoV-2 antibodies depends on the analytical kit: A report for up to 10 months after infection. Microorganisms 2021, 9, 556. [Google Scholar] [CrossRef]
- Bradley, B.T.; Bryan, A.; Fink, S.L.; Goecker, E.A.; Roychoudhury, P.; Huang, M.L.; Zhu, H.; Chaudhary, A.; Madarampalli, B.; Lu, J.Y.; et al. Anti-SARS-CoV-2 Antibody Levels Measured by AdviseDx SARS-CoV-2 Assay Are Concordant with Previously Available Serologic Assays but Are Not Fully Predictive of Sterilizing Immunity. J. Clin. Microbiol. 2021, 59, e00989-21. [Google Scholar] [CrossRef]
- Perkmann, T.; Perkmann-Nagele, N.; Koller, T.; Mucher, P.; Radakovics, A.; Marculescu, R.; Wolzt, M.; Wagner, O.F.; Binder, C.J.; Haslacher, H. Anti-Spike Protein Assays to Determine SARS-CoV-2 Antibody Levels: A Head-to-Head Comparison of Five Quantitative Assays. Microbiol. Spectr. 2021, 9, e0024721. [Google Scholar] [CrossRef]
- Di Meo, A.; Miller, J.J.; Fabros, A.; Brinc, D.; Hall, V.; Pinzon, N.; Ierullo, M.; Ku, T.; Ferreira, V.H.; Kumar, D.; et al. Evaluation of Three anti-SARS-CoV-2 Serologic Immunoassays for Post-Vaccine Response. J. Appl. Lab. Med. 2021, 7, 57–65. [Google Scholar] [CrossRef]
- Lustig, Y.; Sapir, E.; Regev-Yochay, G.; Cohen, C.; Fluss, R.; Olmer, L.; Indenbaum, V.; Mandelboim, M.; Doolman, R.; Amit, S.; et al. BNT162b2 COVID-19 vaccine and correlates of humoral immune responses and dynamics: A prospective, single-centre, longitudinal cohort study in health-care workers. Lancet Respir. Med. 2021, 9, 999–1009. [Google Scholar] [CrossRef]
- Pellini, R.; Venuti, A.; Pimpinelli, F.; Abril, E.; Blandino, G.; Campo, F.; Conti, L.; De Virgilio, A.; De Marco, F.; Di Domenico, E.G.; et al. Initial observations on age, gender, BMI and hypertension in antibody responses to SARS-CoV-2 BNT162b2 vaccine. EClinicalMedicine 2021, 36, 100928. [Google Scholar] [CrossRef] [PubMed]
- Salvagno, G.L.; Henry, B.M.; Pighi, L.; De Nitto, S.; Gianfilippi, G.L.; Lippi, G. Three-month analysis of total humoral response to Pfizer BNT162b2 mRNA COVID-19 vaccination in healthcare workers. J. Infect. 2021, 83, e4–e5. [Google Scholar] [CrossRef] [PubMed]
- Tre-Hardy, M.; Cupaiolo, R.; Wilmet, A.; Beukinga, I.; Blairon, L. Waning antibodies in SARS-CoV-2 naïve vaccinees: Results of a three-month interim analysis of ongoing immunogenicity and efficacy surveillance of the mRNA-1273 vaccine in healthcare workers. J. Infect. 2021, 83, 381–412. [Google Scholar] [CrossRef]
- Widge, A.T.; Rouphael, N.G.; Jackson, L.A.; Anderson, E.J.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J.; et al. Durability of Responses after SARS-CoV-2 mRNA-1273 Vaccination. N. Engl. J. Med. 2021, 384, 80–82. [Google Scholar] [CrossRef]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 Covid-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Tokareva, Y.; Englund, J.A.; Dickerson, J.A.; Brown, J.C.; Zerr, D.M.; Walter, E.; Tsogoo, A.; Cappetto, K.; Valdez Gonzalez, J.; Strelitz, B.; et al. Prevalence of Health Care and Hospital Worker SARS-CoV-2 IgG Antibody in a Pediatric Hospital. Hosp. Pediatrics 2021, 11, e48–e53. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. V-Safe after Vaccination Health Checker. 2021. Available online: https://www.cdc.gov/vaccinesafety/ (accessed on 7 March 2022).
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. Covid-19 breakthrough infections in vaccinated health care workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef]
- Tré-Hardy, M.; Cupaiolo, R.; Wilmet, A.; Antoine-Moussiaux, T.; Della Vecchia, A.; Horeanga, A.; Papleux, E.; Vekemans, M.; Beukinga, I.; Blairon, L. Six-month interim analysis of ongoing immunogenicity surveillance of the mRNA-1273 vaccine in healthcare workers: A third dose is expected. J. Infect. 2021, 83, 559–564. [Google Scholar] [CrossRef]
- Collier, A.Y.; Barouch, D.H. Differential Kinetics of Immune Responses Elicited by Covid-19 Vaccines. N. Engl. J. Med. 2021, 385, 2010–2012. [Google Scholar] [CrossRef]
- Keehner, J.; Horton, L.E.; Binkin, N.J.; Laurent, L.C.; Pride, D.; Longhurst, C.A.; Abeles, S.R.; Torriani, F.J. Resurgence of SARS-CoV-2 Infection in a Highly Vaccinated Health System Workforce. N. Engl. J. Med. 2021, 385, 1330–1332. [Google Scholar] [CrossRef] [PubMed]
- Van Elslande, J.; Oyaert, M.; Ailliet, S.; Van Ranst, M.; Lorent, N.; Weygaerde, Y.V.; André, E.; Lagrou, K.; Vandendriessche, S.; Vermeersch, P. Longitudinal follow-up of IgG anti-nucleocapsid antibodies in SARS-CoV-2 infected patients up to eight months after infection. J. Clin. Virol. 2021, 136, 104765. [Google Scholar] [CrossRef] [PubMed]
- Shrock, E.; Fujimura, E.; Kula, T.; Timms, R.T.; Lee, I.-H.; Leng, Y.; Robinson, M.L.; Sie, B.M.; Li, M.Z.; Chen, Y.; et al. Viral epitope profiling of COVID-19 patients reveals cross-reactivity and correlates of severity. Science 2020, 370, eabd4250. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef]
- Rechavi, Y.; Shashar, M.; Lellouche, J.; Yana, M.; Yakubovich, D.; Sharon, N. Occurrence of BNT162b2 Vaccine Adverse Reactions Is Associated with Enhanced SARS-CoV-2 Antibody Response. Vaccines 2021, 9, 977. [Google Scholar] [CrossRef]
- Zhong, D.; Xiao, S.; Debes, A.K.; Egbert, E.R.; Caturegli, P.; Colantuoni, E.; Milstone, A.M. Durability of Antibody Levels After Vaccination with mRNA SARS-CoV-2 Vaccine in Individuals with or Without Prior Infection. JAMA 2021, 326, 2524–2526. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Number (%) | SARS-CoV-2 IgG Spike (AU/mL) (Median [IQR]) |
|---|---|---|
| Vaccine | ||
| Pfizer BNT | 363 (96) | 2130.2 [1264.7, 3475.8] |
| Moderna mRNA-1273 | 13 (3.4) | 7189.5 [4017.8, 9850.3] |
| I don’t recall | 2 (0.5) | 8450.45 [4637.7, 12263.2] |
| Sex | ||
| Female | 335 (86.6) | 2173 [1243.45, 3712.1] |
| Male | 52 (13.4) | 2003.35 [1334.9, 3363.9] |
| Age (years) | ||
| <35 | 164 (42.4%) | 2418.4 [1355.65, 3721.45] |
| 35–44 | 143 (37%) | 1882.6 [1184.6, 3261.35] |
| 45–55 | 52 (13.4%) | 1852.65 [1225, 4370.3] |
| >55 | 28 (7.2%) | 2045.35 [1349.3, 4018.25] |
| Race | ||
| American Indian or Alaska Native | 2 (0.5) | 1240.7 [986.75, 1494.65] |
| Asian American | 57 (14.7) | 1940.7 [1429.4, 2740.8] |
| Native Hawaiian or other Pacific Islander | 2 (0.5) | 2287.25 [1759.7, 2814.8] |
| Black or African American | 7 (1.8) | 2838.8 [1406.9, 3859.65] |
| White | 321 (82.9) | 2247.5 [1242.6, 3789.6] |
| Other | 5 (1.3) | 1578.6 [4.5, 6662.6] |
| >1 race | 10 (2.6) | 2697.65 [1946.55, 3389.2] |
| Ethnicity | ||
| Hispanic | 25 (6.5) | 1386.55 [882.8, 3484] |
| Not Hispanic | 360 (93) | 2173 [1272.8, 3586.1] |
| Prefer not to say | 2 (0.5) | 8942.1 [5375.15, 12,509] |
| Symptom | Number (%) |
|---|---|
| None | 76 (19.6) |
| Fever | 130 (33.6) |
| Chills | 137 (35.4) |
| Headache | 169 (43.7) |
| Joint Pains | 72 (18.6) |
| Muscle or body aches | 214 (55.3) |
| Fatigue or tiredness | 242 (62.5) |
| Nausea | 44 (11.4) |
| Vomiting | 5 (1.3) |
| Diarrhea | 3 (0.8) |
| Abdominal pain | 6 (1.6) |
| Rash (other than at the injection site) | 3 (0.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dickerson, J.A.; Englund, J.A.; Wang, X.; Brown, J.C.; Zerr, D.M.; Strelitz, B.; Klein, E.J. Higher Antibody Concentrations in U.S. Health Care Workers Associated with Greater Reactogenicity Post-Vaccination. Vaccines 2022, 10, 601. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10040601
Dickerson JA, Englund JA, Wang X, Brown JC, Zerr DM, Strelitz B, Klein EJ. Higher Antibody Concentrations in U.S. Health Care Workers Associated with Greater Reactogenicity Post-Vaccination. Vaccines. 2022; 10(4):601. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10040601
Chicago/Turabian StyleDickerson, Jane A., Janet A. Englund, Xing Wang, Julie C. Brown, Danielle M. Zerr, Bonnie Strelitz, and Eileen J. Klein. 2022. "Higher Antibody Concentrations in U.S. Health Care Workers Associated with Greater Reactogenicity Post-Vaccination" Vaccines 10, no. 4: 601. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10040601