
Immunogenicity and Reactogenicity of mRNA BNT162b2 COVID-19 Vaccine among Thai Adolescents with Chronic Diseases

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Study Procedures
2.3. Immunogenicity Measurement
2.4. Reactogenicity
2.5. Statistical Methods
3. Results
3.1. Study Populations
3.2. Immunogenicity
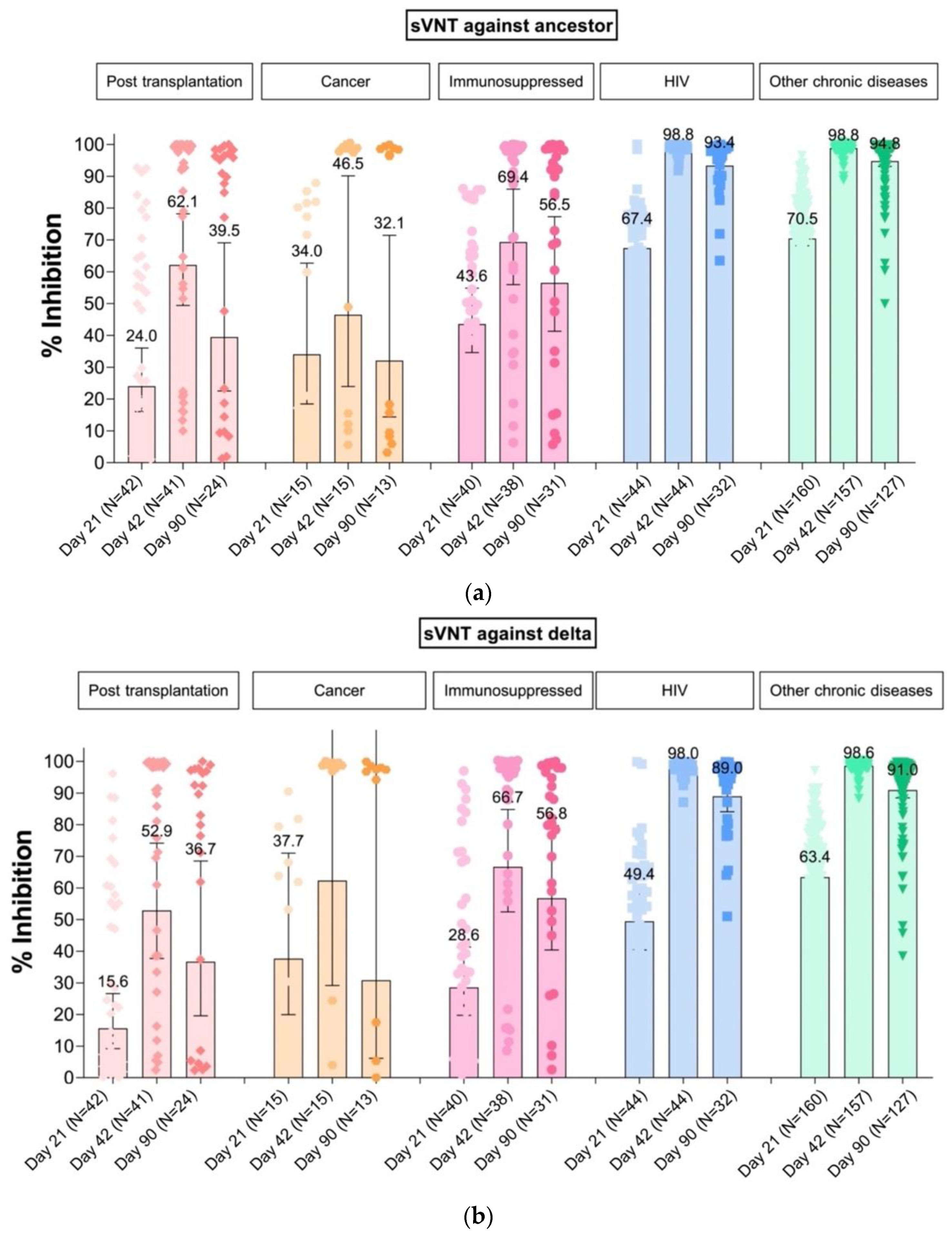
3.2.1. SARS-CoV-2 Surrogate Virus Neutralization Test (sVNT)
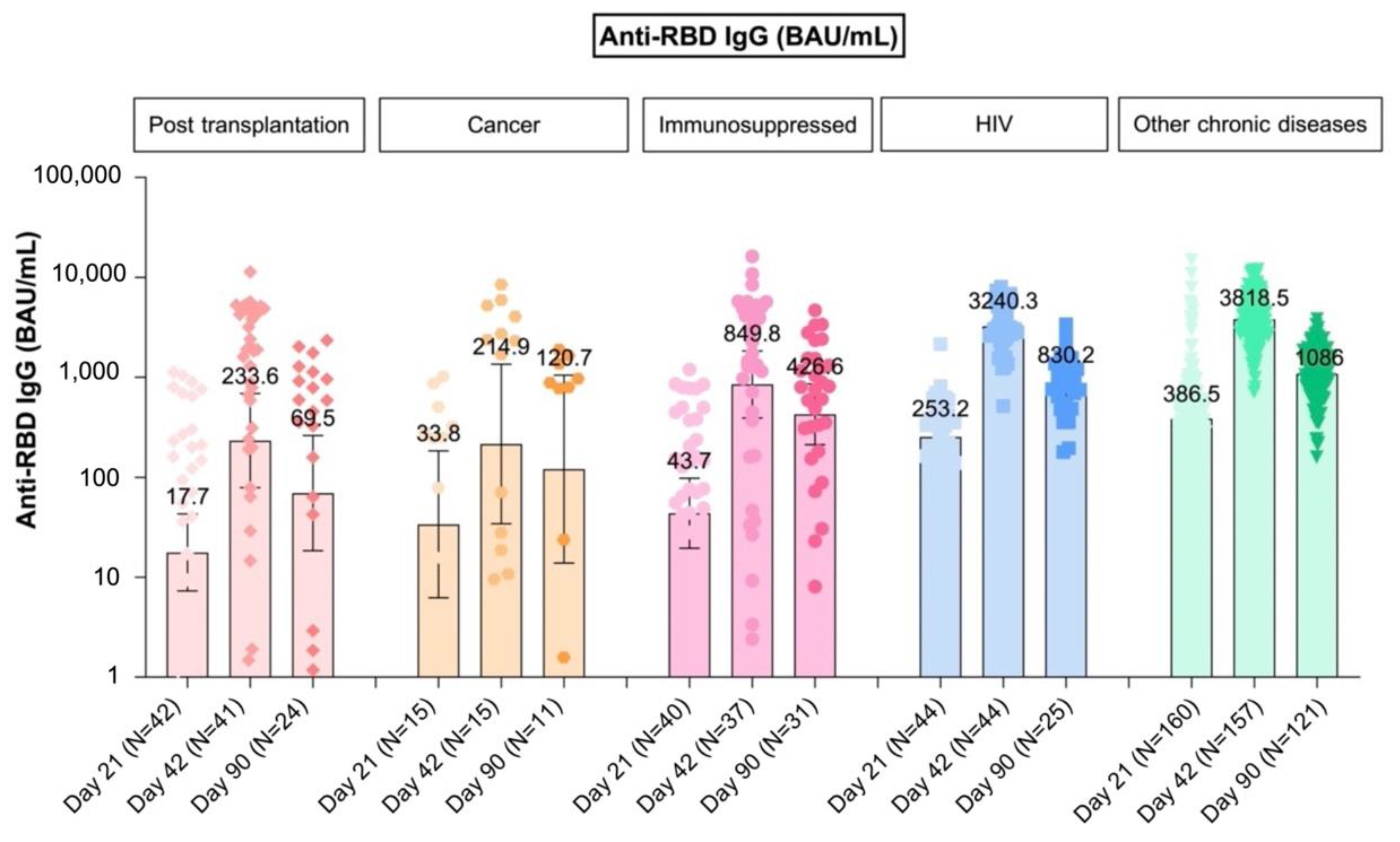
3.2.2. Quantitative IgG against Receptor-Binding Domain (Anti-RBD IgG)
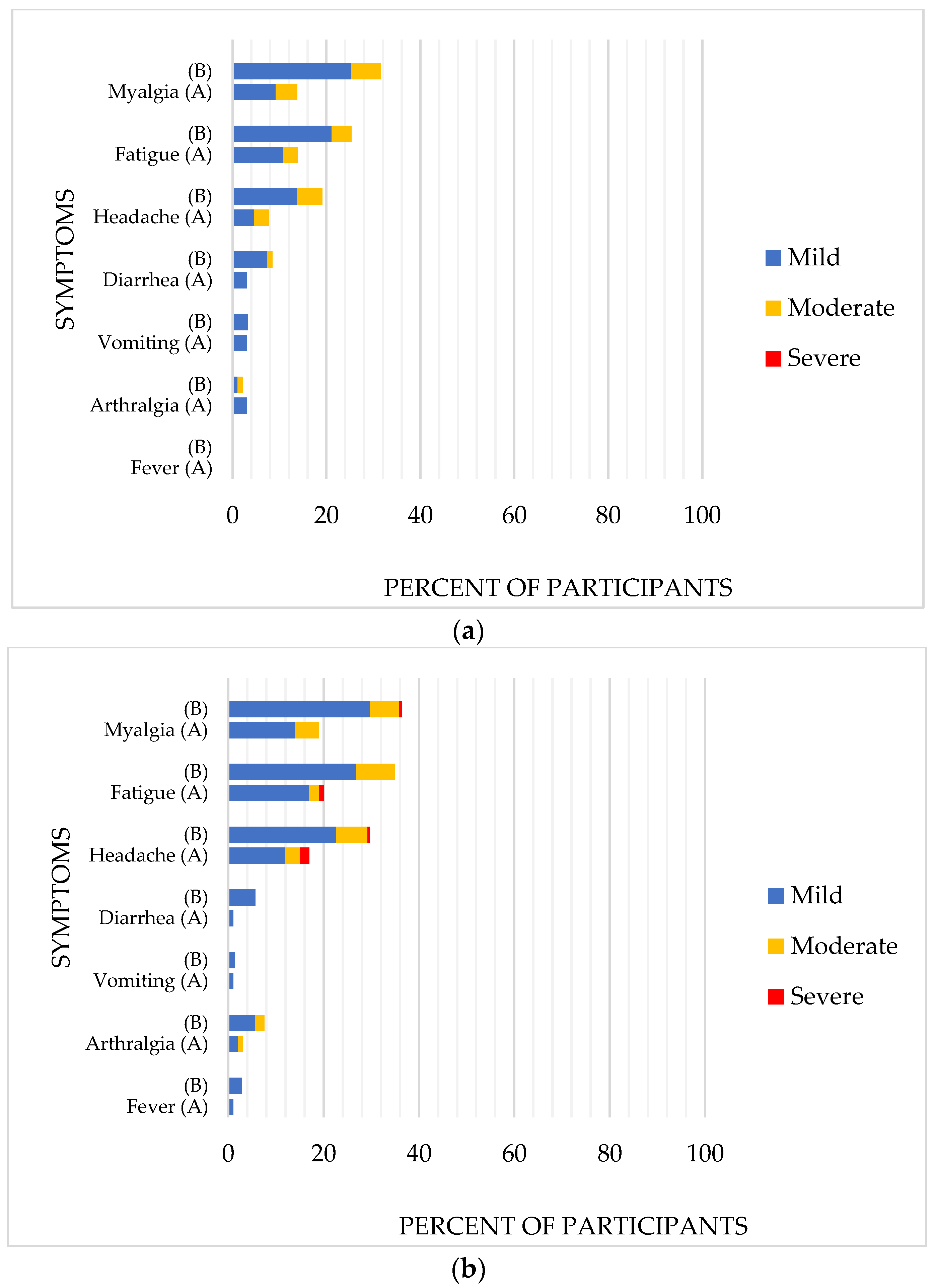
3.3. Reactogenicity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. 2022. Available online: https://covid19.who.int/ (accessed on 27 February 2022).
- COVID-19 Confirmed Cases and Deaths. Available online: https://data.unicef.org/resources/covid-19-confirmed-cases-and-deaths-dashboard/ (accessed on 5 February 2022).
- American Academy of Pediatrics. Children and COVID-19: State-Level Data Report. 2022. Available online: https://www.aap.org/en/pages/2019-novel-coronavirus-covid-19-infections/children-and-covid-19-state-level-data-report/ (accessed on 27 February 2022).
- Hoang, A.; Chorath, K.; Moreira, A.; Evans, M.; Burmeister-Morton, F.; Burmeister, F.; Naqvi, R.; Petershack, M.; Moreira, A. COVID-19 in 7780 pediatric patients: A systematic review. EClinicalMedicine 2020, 24, 100433. [Google Scholar] [CrossRef] [PubMed]
- Anugulruengkitt, S.; Teeraananchai, S.; Chantasrisawad, N.; Promsena, P.; Jantarabenjakul, W.; Puthanakit, T. Clinical outcomes of pediatric COVID-19 in a tertiary care center in Bangkok, Thailand. IJID Reg. 2020, 1, 159–162. [Google Scholar] [CrossRef]
- Payne, A.B.; Gilani, Z.; Godfred-Cato, S.; Belay, E.D.; Feldstein, L.R.; Patel, M.M.; Randolph, A.G.; Newhams, M.; Thomas, D.; Magleby, R.; et al. Incidence of multisystem inflammatory syndrome in children among US persons infected with SARS-CoV-2. JAMA Netw. Open 2021, 4, e2116420. [Google Scholar] [CrossRef] [PubMed]
- Samji, H.; Wu, J.; Ladak, A.; Vossen, C.; Stewart, E.; Dove, N.; Long, D.; Snell, G. Review: Mental health impacts of the COVID-19 pandemic on children and youth-a systematic review. Child Adolesc. Ment. Health 2021, 27, 173–189. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Roy, D.; Sinha, K.; Parveen, S.; Sharma, G.; Joshi, G. Impact of COVID-19 and lockdown on mental health of children and adolescents: A narrative review with recommendations. Psychiatry Res. 2020, 293, 113429. [Google Scholar] [CrossRef]
- US Food and Drug Administration (FDA). Coronavirus (COVID-19) Update: FDA Authorizes Pfizer-BioNTech COVID-19 Vaccine for Emergency Use in Adolescents in Another Important Action in Fight against Pandemic; US Food and Drug Administration: Silver Spring, MD, USA, 2021. [Google Scholar]
- Frenck, R.W., Jr.; Klein, N.P.; Kitchin, N.; Gurtman, A.; Absalon, J.; Lockhart, S.; Perez, J.L.; Walter, E.B.; Senders, S.; Bailey, R.; et al. Safety, immunogenicity, and efficacy of the BNT162b2 COVID-19 vaccine in adolescents. N. Engl. J. Med. 2021, 385, 239–250. [Google Scholar] [CrossRef]
- Deepak, P.; Kim, W.; Paley, M.A.; Yang, M.; Carvidi, A.B.; Demissie, E.G.; El-Qunni, A.A.; Haile, A.; Huang, K.; Kinnett, B.; et al. Effect of immunosuppression on the immunogenicity of mRNA vaccines to SARS-CoV-2: A prospective cohort study. Ann. Intern. Med. 2021, 174, 1572–1585. [Google Scholar] [CrossRef]
- Furer, V.; Eviatar, T.; Zisman, D.; Peleg, H.; Paran, D.; Levartovsky, D.; Zisapel, M.; Elalouf, O.; Kaufman, I.; Meidan, R.; et al. Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in adult patients with autoimmune inflammatory rheumatic diseases and in the general population: A multicentre study. Ann. Rheum. Dis. 2021, 80, 1330–1338. [Google Scholar] [CrossRef]
- Rozen-Zvi, B.; Yahav, D.; Agur, T.; Zingerman, B.; Ben-Zvi, H.; Atamna, A.; Tau, N.; Mashraki, T.; Nesher, E.; Rahamimov, R. Antibody response to SARS-CoV-2 mRNA vaccine among kidney transplant recipients: A prospective cohort study. Clin. Microbiol. Infect. 2021, 27, 1173.e1–1173.e4. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Antibody response to 2-dose SARS-CoV-2 mRNA vaccine series in solid organ transplant recipients. JAMA 2021, 325, 2204–2206. [Google Scholar] [CrossRef]
- Mbaeyi, S.; Oliver, S.E.; Collins, J.; Godfrey, M.; Goswami, N.D.; Hadler, S.C.; Jones, J.; Moline, H.; Moulia, D.; Reddy, S.; et al. The advisory committee on immunization practices’ interim recommendations for additional primary and booster doses of COVID-19 vaccines—United States, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- Graff, K.; Smith, C.; Silveira, L.; Jung, S.; Curran-Hays, S.; Jarjour, J.; Carpenter, L.; Pickard, K.; Mattiucci, M.; Fresia, J.; et al. Risk factors for severe COVID-19 in children. Pediatric Infect. Dis. J. 2021, 40, e137–e145. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. COVID-19: The Green Book, Chapter 14a. 2021. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/984310/Greenbook_chapter_14a_7May2021.pdf (accessed on 22 March 2022).
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I.; et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 2032–2040. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.W.; Chia, W.N.; Qin, X. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2–spike protein–protein interaction. Nat. Biotechnol. 2020, 38, 1073–1078. [Google Scholar] [CrossRef]
- Psichogiou, M.; Karabinis, A.; Poulakou, G.; Antoniadou, A.; Kotanidou, A.; Degiannis, D.; Pavlopoulou, I.D.; Chaidaroglou, A.; Roussos, S.; Mastrogianni, E. Comparative immunogenicity of BNT162b2 mRNA vaccine with natural SARS-CoV-2 infection. Vaccines 2021, 9, 1017. [Google Scholar] [CrossRef]
- Guidance for Industry. Toxicity Grading Scale for Healthy Adult and Adolescent Volunteers Enrolled in Preventive Vaccine Clinical Trials. 2007. Available online: https://www.fda.gov/media/73679/download (accessed on 17 December 2021).
- Ruddy, J.A.; Connolly, C.M.; Boyarsky, B.J.; Werbel, W.A.; Christopher-Stine, L.; Garonzik-Wang, J.; Segev, D.L.; Paik, J.J. High antibody response to two-dose SARS-CoV-2 messenger RNA vaccination in patients with rheumatic and musculoskeletal diseases. Ann. Rheum. Dis. 2021, 80, 1351–1352. [Google Scholar] [CrossRef]
- Grupper, A.; Rabinowich, L.; Schwartz, D.; Schwartz, I.F.; Ben-Yehoyada, M.; Shashar, M.; Katchman, E.; Halperin, T.; Turner, D.; Goykhman, Y.; et al. Reduced humoral response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients without prior exposure to the virus. Am. J. Transplant. 2021, 21, 2719–2726. [Google Scholar] [CrossRef]
- Collier, A.Y.; Yu, J.; McMahan, K.; Liu, J.; Atyeo, C.; Ansel, J.L.; Fricker, Z.P.; Pavlakis, M.; Curry, M.P.; Jacob-Dolan, C.; et al. Coronavirus disease 2019 messenger RNA vaccine immunogenicity in immunosuppressed individuals. J. Infect. Dis. 2022, 225, 1124–1128. [Google Scholar] [CrossRef]
- Redjoul, R.; Le Bouter, A.; Beckerich, F.; Fourati, S.; Maury, S. Antibody response after second BNT162b2 dose in allogeneic HSCT recipients. Lancet 2021, 398, 298–299. [Google Scholar] [CrossRef]
- Embi, P.J.; Levy, M.E.; Naleway, A.L.; Patel, P.; Gaglani, M.; Natarajan, K.; Dascomb, K.; Ong, T.C.; Klein, N.P.; Liao, I.C.; et al. Effectiveness of 2-dose vaccination with mRNA COVID-19 vaccines against COVID-19-associated hospitalizations among immunocompromised adults—Nine states, January-September 2021. MMWR 2021, 70, 1553–1559. [Google Scholar] [CrossRef]
- Crane, C.; Phebus, E.; Ingulli, E. Immunologic response of mRNA SARS-CoV-2 vaccination in adolescent kidney transplant recipients. Pediatric Nephrol. 2022, 37, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Fendler, A.; Shepherd, S.T.C.; Au, L.; Wilkinson, K.A.; Wu, M.; Byrne, F.; Cerrone, M.; Schmitt, A.M.; Joharatnam-Hogan, N.; Shum, B.; et al. Adaptive immunity and neutralizing antibodies against SARS-CoV-2 variants of concern following vaccination in patients with cancer: The CAPTURE study. Nat. Cancer 2021, 2, 1305–1320. [Google Scholar] [CrossRef] [PubMed]
- Levy, I.; Wieder-Finesod, A.; Litchevsky, V.; Biber, A.; Indenbaum, V.; Olmer, L.; Huppert, A.; Mor, O.; Goldstein, M.; Levin, E.G.; et al. Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in people living with HIV-1. Clin. Microbiol. Infect. 2021, 27, 1851–1855. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning immune humoral response to BNT162b2 Covid-19 vaccine over 6 months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Sahin, U.; Muik, A.; Derhovanessian, E.; Vogler, I.; Kranz, L.M.; Vormehr, M.; Baum, A.; Pascal, K.; Quandt, J.; Türeci, Ö.; et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T cell responses. Nature 2020, 586, 594–599. [Google Scholar] [CrossRef]
- Burns, M.D.; Boribong, B.P.; Bartsch, Y.C.; Loiselle, M.; Denis, K.J.; Sheehan, M.L.; Chen, J.W.; Davis, J.P.; Lima, R.; Edlow, A.G.; et al. Durability and cross-reactivity of SARS-CoV-2 mRNA vaccine in adolescent children. Vaccines 2022, 10, 492. [Google Scholar] [CrossRef]
- Bauernfeind, S.; Salzberger, B.; Hitzenbichler, F.; Scigala, K.; Einhauser, S.; Wagner, R.; Gessner, A.; Koestler, J.; Peterhoff, D. Association between reactogenicity and immunogenicity after vaccination with BNT162b2. Vaccines 2021, 9, 1089. [Google Scholar] [CrossRef]
- Coggins, S.A.; Laing, E.D.; Olsen, C.H.; Goguet, E.; Moser, M.; Jackson-Thompson, B.M.; Samuels, E.C.; Pollett, S.D.; Tribble, D.R.; Davies, J.; et al. Adverse effects and antibody titers in response to the BNT162b2 mRNA COVID-19 vaccine in a prospective study of healthcare workers. Open Forum Infect. Dis. 2021, 9, ofab575. [Google Scholar] [CrossRef]
- Müller, L.; Andrée, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J.; Hillebrandt, J.; Ritchie, A.; Rabl, D.; et al. Age-dependent immune response to the Biontech/Pfizer BNT162b2 Coronavirus Disease 2019 vaccination. Clin. Infect. Dis. 2021, 73, 2065–2072. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 312) | Immunocompromised (n = 100) | Chronic Diseases a (n = 212) | p-Value | |
|---|---|---|---|---|
| Age (y), | 15 | 15.5 | 14.9 | 0.13 |
| median (IQR) | (13.7–16.5) | (13.9–16.9) | (13.7–16.4) | |
| Female, N (%) | 161 (51.6) | 59 (58) | 102 (48.6) | 0.12 |
| BMI (kg/m2), median (IQR) | 21.7 (18.1–27.8) | 19.7 (17.1–24.2) | 22.4 (18.6–30.6) | <0.001 |
| Transplantation, N (%) | 42 (42) | |||
| Immunosuppressed, N (%) | 43 (43) | |||
| Cancer, N (%) | 15 (15) | |||
| HIV, N (%) | 46 (21.7) | |||
| Chronic diseases, N (%) | 166 (78.3) |
| Post Dose 1 | Post Dose 2 | Day 90 Post Dose 1 | ||||
|---|---|---|---|---|---|---|
| Day 21 (n = 292) a | Day 42 (n = 291) b | (n = 227) | ||||
| GMs (95% CI), % inh | Ancestor | Delta | Ancestor | Delta | Ancestor | Delta |
| Overall | 55.4 | 45.0 | 85.7 | 85.0 | 75.5 | 74.1 |
| (51.1–60.0) | (40.4–50.1) | (81.2–90.5) | (79.8–90.5) | (68.8–82.9) | (66.6–82.4) | |
| Immunocompromised | 32.4 | 22.7 | 62.4 | 59.7 | 44.7 | 43.9 |
| (26.0–40.3) | (16.9–30.4) | (53.3–73.1) | (49.2–72.6) | (33.9–58.9) | (30.8–62.4) | |
| - Transplantation (N = 42) | 24.0 | 15.6 | 62.1 | 52.9 | 39.5 | 36.7 |
| (16.0–36.0) | (9.2–26.6) | (49.4–78.2) | (37.7–74.2) | (22.5–69.1) | (19.6–68.5) | |
| - Immunosuppressed (N = 40) | 43.6 | 28.6 | 69.4 | 66.7 | 56.5 | 56.8 |
| (34.6–54.9) | (19.8–41.3) | (56.0–86.0) | (52.4–84.8) | (41.3–77.3) | (40.4–79.7) | |
| - Cancer (N = 15) | 34.0 | 37.7 | 46.5 | 62.3 | 32.1 | 30.8 |
| (18.5–62.7) | (20.0–71.0) | (24.0–90.1) | (29.2–133.1) | (14.4–71.5) | (6.2–154.1) | |
| Chronic diseases | 69.8 | 60.1 | 98.8 | 98.5 | 94.5 | 90.6 |
| (67.7–72.0) | (56.9–63.5) | (98.6–99.1) | (98.2–98.8) | (93.0–96.0) | (88.4–92.8) | |
| - HIV (N = 44) | 67.4 | 49.4 | 98.8 | 98.0 | 93.4 | 89.0 |
| (62.4–72.8) | (40.4–60.6) | (98.2–99.3) | (97.3–98.8) | (90.0–96.8) | (84.1–94.1) | |
| - Others chronic diseases (N = 160) | 70.5 | 63.4 | 98.8 | 98.6 | 94.8 | 91.0 |
| (68.2–72.8) | (60.9–66.0) | (98.6–99.1) | (98.3–98.9) | (93.1–96.5) | (88.5–93.5) | |
| GMR (95% CI) immocompromised vs. chronic diseases | 0.46 | 0.38 | 0.63 | 0.61 | 0.47 | 0.48 |
| (0.40–0.54) | (0.31–0.46) | (0.57–0.70) | (0.54–0.69) | (0.40–0.57) | (0.39–0.60) | |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Post Dose 1 | Post Dose 2 | Day 90 after Dose 1 | |
|---|---|---|---|
| Day 21 (n = 299) a | Day 42 (n = 294) b | (n = 212) | |
| GMs (95% CI), BAU/mL | |||
| Overall | 158.6 | 1803.5 | 599.9 |
| (125.0–201.3) | (1423.1–2285.5) | (469.8–765.9) | |
| Immunocompromised | 28.5 | 385.2 | 178.7 |
| (16.4–49.5) | (205.5–722.2) | (91.2–350.1) | |
| - Transplantation (N = 42) | 17.7 | 233.6 | 69.5 |
| (7.3–42.9) | (79.0–690.6) | (18.4–262.1) | |
| - Immunosuppressed (N = 40) | 43.7 | 849.8 | 426.6 |
| (19.6–97.8) | (393.4–1835.8) | (211.9–858.7) | |
| - Cancer (N = 15) | 33.8 | 214.9 | 120.7 |
| (6.2–183.6) | (34.2–1348.6) | (13.9–1050.1) | |
| Chronic diseases | 352.8 | 3683.7 | 1037.1 |
| (307.0–405.6) | (3398.5–3992.8) | (933.3–1152.5) | |
| - HIV (N = 44) | 253.2 | 3240.3 | 830.2 |
| (197.1–325.3) | (2699.0–3890.2) | (617.5–1116.1) | |
| - Others chronic diseases (N = 160) | 386.5 | 3818.5 | 1086.0 |
| (328.7–454.5) | (3490.4–4177.4) | (970.9–1214.6) | |
| GMR (95% CI) immocompromised vs. chronic diseases | 0.08 (0.05–0.12) | 0.10 (0.07–0.16) | 0.17 (0.11–0.28) |
| p-value | <0.001 | <0.001 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chantasrisawad, N.; Puthanakit, T.; Tangsathapornpong, A.; Techasaensiri, C.; Phongsamart, W.; Suwanpakdee, D.; Jaruampornpan, P.; Sophonphan, J.; Suntarattiwong, P.; Chotpitayasunondh, T., on behalf of the Study Team. Immunogenicity and Reactogenicity of mRNA BNT162b2 COVID-19 Vaccine among Thai Adolescents with Chronic Diseases. Vaccines 2022, 10, 871. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10060871
Chantasrisawad N, Puthanakit T, Tangsathapornpong A, Techasaensiri C, Phongsamart W, Suwanpakdee D, Jaruampornpan P, Sophonphan J, Suntarattiwong P, Chotpitayasunondh T on behalf of the Study Team. Immunogenicity and Reactogenicity of mRNA BNT162b2 COVID-19 Vaccine among Thai Adolescents with Chronic Diseases. Vaccines. 2022; 10(6):871. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10060871
Chicago/Turabian StyleChantasrisawad, Napaporn, Thanyawee Puthanakit, Auchara Tangsathapornpong, Chonnamet Techasaensiri, Wanatpreeya Phongsamart, Detchvijitr Suwanpakdee, Peera Jaruampornpan, Jiratchaya Sophonphan, Piyarat Suntarattiwong, and Tawee Chotpitayasunondh on behalf of the Study Team. 2022. "Immunogenicity and Reactogenicity of mRNA BNT162b2 COVID-19 Vaccine among Thai Adolescents with Chronic Diseases" Vaccines 10, no. 6: 871. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10060871