
The Impact of COVID-19 Pandemic on Inequity in Routine Childhood Vaccination Coverage: A Systematic Review

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
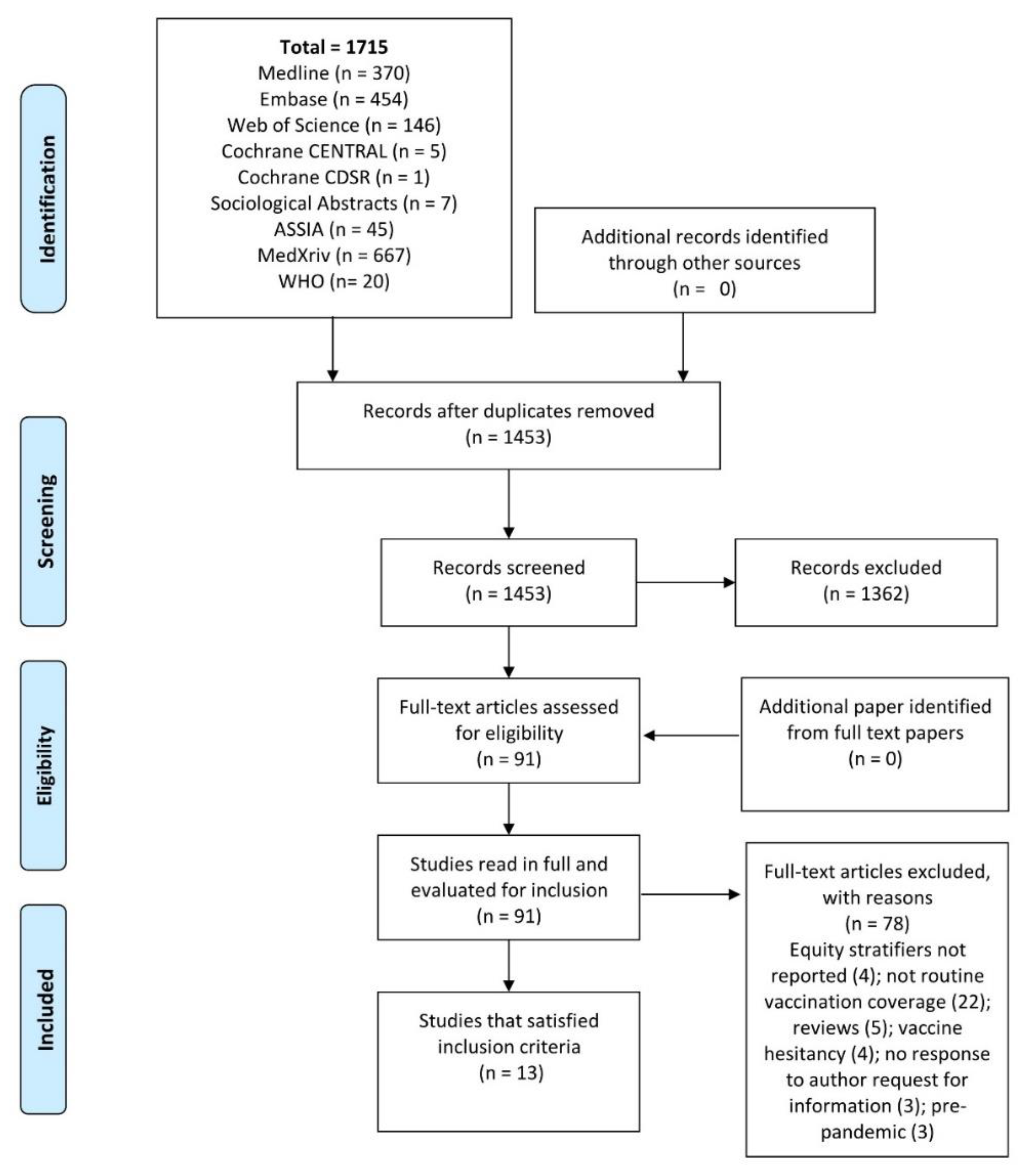
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction and Synthesis
2.4. Risk of Bias Assessment
3. Results
3.1. Characteristics of Included Studies

{kind=link}
{kind=link}
| Study | Year | Country | Study Design | Data Collection Months | Total Number of Children Studied | Age of Children | Sex: Males No. (%) |
|---|---|---|---|---|---|---|---|
| Ackerson et al. [23] | 2021 | Southern California, USA | Retrospective cohort study using electronic health records (EHR) of the Kaiser Permanente Southern California integrated health care system | January to August 2020 compared with January to August 2019 2020 data sub-divided into: Pre-pandemic: 1 January–12 March Stay-at-home: 413 March–May 6 Reopening: 7 May to 31 August | 987,544 eligible for vaccination on 1 January 2019 992,971 eligible for vaccination on 1 January 2020 | 0–18 years | 504,456 (51.1%) 2019 507,361 (51.1%) 2020 |
| Bell et al. [15] | 2021 | UK | Mixed methods study with an online cross-sectional survey and semi-structured telephone interviews | 19 April and 11 May 2020 | 1252 parents or guardians of eligible children | 18 months or less | Not stated |
| Bramer et al. [24] | 2020 | Michigan State, USA | Secondary analysis of routinely collected Michigan State-level data on children eligible for vaccination | May 2020 (pandemic months) compared to May 2019 (pre-pandemic month) | 9539 children from the pandemic month and 9269 children from the pre-pandemic month) | 1–24 months | Not stated |
| Chandir et al. [14] | 2020 | Sindh Province, Pakistan | Secondary analysis of regional electronic data from the Government of Sindh’s Zindagi Mehfooz (Safe Life) Electronic Immunization Registry (ZM EIR) | 23 September 2019–22 March 2020 (pre-lockdown period) and 23 March–9 May 2020 (COVID-19 lockdown period) | 786,325 children enrolled in pre-lockdown period and 83,360 during lockdown period | 0–24 months | 407,410 (51.8%) pre-pandemic; 43,728 (52.5%) in lockdown |
| DeSilva et al. [22] | 2021 | California, Oregon, Washington, Colorado, Minnesota, and Wisconsin, USA | Surveillance study using a pre-pandemic, post-pandemic control design | February 2020 (Pre-Pandemic); May 2020 (Pandemic restrictions); September 2020 (Post-Pandemic) Same months in 2019 used as controls | 39,113 children in 2019 and 40,373 in 2020 | Children reaching specified ages (7 months, 18 months, 6 years, 13 years, and 18 years) in February, May, or September 2019 and 2020 | 1429,979 (51.0%) |
| Hou Z et al. [28] | 2020 | Wuhan and Shanghai, China | Cross-sectional online survey | 12–17 March 2020 | 1655 children and young people enrolled in the survey–626 had scheduled vaccinations during the study period | 3 to 17 years | 830 (50.2%) |
| Jain et al. [20] | 2021 | Rajasthan, India | Retrospective observational study based on phone survey– | March 2020 (pre-lockdown);March-May2020 (Lockdown period) and June-July 2020 (post-lockdown period) | 2114 children: 443 > 12 months of age before March 2020 (unexposed to lockdown); 722 turned 12 months between March and May 2020 (partially exposed); 796 aged 9 months March to May (heavily exposed); 183 aged 9 months in June-July (post-exposed)) | Children born in or after January 2019 and at least 12 months of age at the time of the survey | 1122 (52%) |
| Miretu et al. [25] | 2021 | Dessie Town, Northeast Ethiopia | A community-based cross-sectional survey using multistage cluster sampling | 22 July to 7 August 2020 | 610 mothers with children aged 15–23 months enrolled. | 15–23 months | 300 (49.2%) |
| Moreno-Montoya et al. [21] | 2021 | Colombia | An ecological study of monthly vaccination data from the Expanded Program of Immunization (EPI) | March to October 2020 (lockdown period March to 1 September) compared with March to October 2019 | 2,128,642 children in 2019 2,110,767 children in 2020 | Three age cohorts: <12 months 12–24 months 5 years | Not stated |
| Rizwan et al. [16] | 2021 | Pakistan | Cross-sectional survey | 25 July to 7 August 2020 | 345 children whose parents completed the questionnaire and had up-to-date vaccination cards | <2 years | 181 (52.4%) |
| Shapiro et al. [29] | 2021 | 9 middle- and 16 high-income countries | National panel survey data | 14 May to 9 June 2020 | 9359 children in 9 middle-income countries and 14,886 in 16 high-income countries/ | 0–17 years | Not stated |
| Silveira MF et al. [27] | 2021 | Brazil | Cross-sectional survey | 24–27 August 2020 | 2530 children (vaccination data collected by questionnaire for 2439 children and from vaccination cards for 1547 children) | <2 years | 1305 (51.6%) |
| Tegegne W et al. [26] | 2020 | Southwest Ethiopia | Cross-sectional mixed-methods survey | 2 September to 21 October 2020 | 1300 children | 10–23 months | Not stated |
| Study | Routine Childhood Vaccine Studied | Equity Stratifiers Measured | Analysis | Main Results |
|---|---|---|---|---|
| Ackerson et al. [23] | HepB, ROTA, DTaP, Hib, PCV13, IPV, MMR, VAR, HepA, Tdap, MenACWY, 9vHPV | Race or ethnicity: Hispanic; Non-Hispanic white; Non-Hispanic Black; Non-Hispanic Asian American | Outcome: Total of all routine vaccine doses administered for ages 0–18 years during pre-pandemic (1 January to 12 March), stay-at-home (13 March to 6 May) periods. Analysis by race or ethnicity: Difference-in-Difference (DID) analyses and estimated adjusted percentage differences and 95% CIs using Poisson regression models, adjusting for the percentage difference in vaccine doses administered during the pre-pandemic period | Adjusted % Difference (95% CI) (Stay-at-Home period v. Pre-pandemic): Hispanic: −46.4 (−47.2,−45.7) Non-Hispanic White: −49.1 (−50.1,−48.2) Non-Hispanic Black: −53.4 (−55.1,−51.7) Non-Hispanic Asian American: −41.7 (−43.3,−40.0) |
| Bell et al. [15] | Recommended vaccines according to the UK schedule [details of schedule not given in paper] | Race or ethnicity: White; Black and Minority Ethnicity (BAME) Annual Household Income: Low (<£35,000); Medium (£35,000–84,999): High (>£85,000) Employment: Working full-time; Working part-time; Homemaker; Student; Unemployed | AOR with 95% CI for overdue vaccinations by race/ethnicity, household income and employment adjusted for each other and the number of children | Overdue vaccinations by 4: Race/ethnicity (White = reference): BAME: AOR 2.15 (95% CI 0.72,6.40) Income (Medium = reference): Low: AOR 1.24 (0.63,2.46) High: AOR 0.93 (0.43,1.97) Employment (Full-time = reference): Part-time: AOR 0.93 (0.47,1.85) Homemaker: AOR 2.23(0.97,5.22) [Student and Unemployed–insufficient numbers for analysis] |
| Bramer et al. [24] | Pentavalent (HepB+Hib+DTaP), Hexavalent (HepB+Hib+DTaP+IPV), MMR/MR/measles, HepB (separate shot), ROTA | Medicaid enrolment v. non-Medicaid enrolment | Frequencies: up-to-date with vaccinations in May 2020 cf. 2016–19 No probability or analysis of statistical significance for equity stratifiers | Reductions in all age cohorts apart from those aged under one month. Up-to-date series coverage for each age cohort assessed in May 2020 is lower for Medicaid enrolled children than non-Medicaid enrolled children. The largest difference in the 7-month cohort–34.6% Medicaid v. 55.0% non-Medicaid up to date |
| Chandir et al. [14] | Pentavalent (HepB+Hib+DTaP), Measles, ROTA, PCV, BCG, IPV/OPV | Individual level: Rural/Urban dweller; Maternal Education in years–0,1–8,9–10,11–12,13+. Area level (Union Councils–smallest admin areas): Rural v. Urban; Slum v. Non-slum; Super High-Risk Union Councils (SHRUC) | Analysis 1: age-appropriate Penta 3 vaccination completion during lockdown: ARRs calculated by rural v. urban dweller and maternal education level adjusted for child’s sex, birth in a hospital, Penta 2 vaccination by outreach, outreach vaccination history, age at Penta 2 and BCG. Both rural/urban dweller and maternal education were included in the regression model Analysis 2: area-based decline in average daily vaccine visits lockdown v. baseline Analysis 3: Percentage difference in enrolment COVID-19 lockdown v. baseline by maternal education (95% CI) | Analysis 1: by years of maternal education (no years as ref*): 1–5 years ARR 1.19 (95% CI 1.13,1.25); 6–10 years ARR 1.38 (1.27,1.50); 11–12 years ARR 1.50 (1.35,1.65); 12+ years ARR 1.38 (1.23,1.55). By rural v. urban (rural as ref): ARR 1.03 (0.98,1.08) Analysis 2: [no measure of probability–only frequencies]: % reduction in vaccination visits–Rural–54.9% v. Urban −53.8%; Slum–53.8% v. Non-Slum–51.3%; SHRUC −68.1% v. Non-SHRUC −50.6% Analysis 3: % difference in enrolment by maternal education: none–3.1% (−3.45,−2.74); 1–8 years–0.5% (−0.86,−0.14); 9–10 years–1.3% (1.14,1.45); 11–12 years −1.12% (1.08,1.32); >12 yrs–1.2% (1.01,1.32). |
| DeSilva et al. [22] | HepB, ROTA, DTaP, Hib, PCV13, IPV, MMR, VAR, HPV, MCV4 | Race or ethnicity: Asian; Black; Hispanic; White; Other | Outcome: Up-to-date (UTD) with scheduled vaccines Unadjusted proportions (95% CIs) UTD in May 2020 compared with February 2020 by race/ethnicity stratified by age group | February/May 7 months Asian 0.88 (0.87,0.90)/0.81(0.79,0.83) Black 0.68 (0.63,0.73)/0.54(0.49,0.60) H’panic0.82 (0.80,0.84)/0.71(0.69,0.74) Other 0.80 (0.77,0.82)/0.70(0.67,0.72) White 0.81 (0.79,0.82)/0.72(0.70,0.74) 18 months: Asian 0.78 (0.76,0.80)/0.76 (0.74,0.79) Black 0.49 (0.45,0.53)/0.41 (0.36,0.45) H’panic0.59 (0.58,0.61)/0.56 (0.54,0.58) Other 0.59 (0.57,0.62)/0.54 (0.51,0.57) White 0.59 (0.57,0.61)/0.52 (0.50,0.54) 6 years: Asian 0.81 (0.79,0.83)/0.80 (0.78,0.82) Black 0.74 (0.70,0.77)/0.76 (0.73,0.80) H’panic0.81 (0.79,0.82)/0.80 (0.79,0.82) Other 0.74 (0.72,0.77)/0.72 (0.69,0.74) White 0.79 (0.78,0.81)/0.80 (0.79,0.82) 13 years: Asian 0.71 (0.68,0.74)/0.72 (0.69,0.74) Black 0.54 (0.50,0.58)/0.52 (0.49,0.56) H’panic0.64 (0.63,0.66)/0.64 (0.62,0.66) Other 0.55 (0.52,0.58)/0.50 (0.47,0.53) White 0.53 (0.51,0.55)/0.55 (0.53,0.56) 18 years: Asian 0.63 (0.60,0.67)/0.65 (0.62,0.68) Black 0.60 (0.56,0.64)/0.62 (0.58,0.65) H’panic0.68 (0.66,0.70)/0.67 (0.65,0.69) Other 0.51 (0.48,0.54)/0.49 (0.47,0.52) White 0.56 (0.54,0.58)/0.54 (0.52,0.56) |
| Hou Z et al. [28] | Scheduled childhood vaccination (excluding COVID vaccine). in children aged 3 to 17 years [details of schedule not given in paper] | Education level of responding parent: High school or below; Some college; Bachelor’s degree or above | OR with 95% CI of delay in vaccination schedule by parent educational level adjusted for city, child’s age and gender, household size, father respondent, COVID−19 cases in the neighbourhood | Delayed scheduled vaccination by educational status (Bachelor’s degree or above as a reference): Some college: AOR 0.75 (95% CI 0.46,1.21); High school or below: AOR 0.30 (0.15,0.59) |
| Jain et al. [20] | Pentavalent (HepB+Hib+DTaP), Measles, BCG | Low assets, low caste, and low parent education | Analyses of interest: To study changes in the percentage of children fully immunised during lockdown compared with prior to lockdown (data only for the heavily exposed group (796) and unexposed group (443)): Analysis 1: Percentage point (PP) differences in fully immunised rates between exposed groups by equity stratifiers (95% CIs) Analysis 2: PP differences in equity stratifier difference (95% CI) | Assets: Analysis 1: High (77.1–70.4) PP = −6.5 (95% CI −13.03,−0.30); Low (71.5–59.3) PP = −12.4 (−19.9,−4·8) Analysis 2: PP difference between exposed groups by asset level difference = −5.6 (−15.8,4.6) Caste: Analysis 1: High (74.8–66.8) PP = −8.4(−13.9,−2.2); Low (72.6–52.9) PP = −13.5 (−23.5,−3.0) Analysis 2: PP difference between exposed groups by caste difference = −5.6 (−17.7,6.4). Parent education: Analysis 1: High (79.0–73.2) PP = −5.8(−12.6,1.1); Low (70.1–57.1) PP = −13.0 (−20.3, −5.7) Analysis 2: PP difference between exposed groups by education difference = −7.2 (−17.3,2.8) |
| Miretu et al. [25] | Pentavalent (HepB+Hib+DTaP), PCV, Measles, ROTA, BCG, OPV | Education status of mother/caregiver: Cannot read or write No schooling but can read or write School grades 1–8 School grade 9–12 College/University or above | Outcome: Fully vaccinated Logistic regression: Odds ratio (OR) of being fully vaccinated in different educational statuses compared to mothers/caregivers who cannot read or write (reference group) by education status adjusted for marital status, father as the main caregiver, and distance to a health facility | Can read or write: AOR 7.82 (95% CI 1.24,49.2); Grade 1–8: AOR 5.23 (1.23,20.22); Grade 9–12: AOR 2.71 (0.65,11.25); College/University: AOR 3.91(0.92,16.60) |
| Moreno-Montoya et al.[21] | BCG, HepB, IPV, OPV, ROTA, PCV, Pentavalent (HepB+Hib+DTaP), Hib, MMR, VAR, HepA, YF. | Rural v. urban areas | Two-level multilevel linear regression model to assess the effect of rural residence on absolute differences in individual vaccine coverage at different ages between 2019 and 2020; the geographical area was considered a level 2 variable, and rural residence a level 1 variable. The effect size of rural residence expressed as Beta coefficients (95% CI) | Beta coefficients by rural residence: <12 months: BCG 0.45 (0.22,0.69); Hep B 0.49 (0.25,0.73); IPV 0.36 (0.16,0.57); OPV+IPV 0.26 (0.06,0.48); Penta 1 0.39 (0.19,0.58); Rota 2 0.37 (0.18,0.56); Pneumococcal 3 0.39 (0.19,0.59) 12–23 months: MMR 0.14 (−0.05,0.33); Varicella 0.21 (−0.01,0.41); Pneumococcal 0.17 (−0.03,0.37); Hep A 0.16 (−0.04,0.37); Yellow Fever 0.12 (−0.08,0.33); OPV 0.10 (−0.08,0.29); DPT 0.13 (−0.06,0.31) 5 years: MMR 0.25 (0.06,0.45); OPV 0.22 (0.02,0.43); DPT 0.28 (0.08,0.49) |
| Rizwan et al. [16] | Pentavalent (HepB+Hib+DTaP), MMR, BCG, OPV | The educational level of mother and father Illiterate; Primary; Secondary; Graduate; Masters; Professional degree Monthly income in rupees (<20,000; 20,000–50,000; 50,000–100,000; >100,000) | Outcome: any missed vaccination during the pandemic Univariate analysis with chi-square and p value | Frequencies 4 with p value Father’s education: Illiterate 40.7%; Primary 51.2%; Secondary 32.7%; Graduate 40.3%; Masters 0%; Professional degrees 38.5% p = 0.006 Mother’s education: Illiterate 42.7%; Primary 76.3%; Secondary 31.2%; Graduate 25.5%; Masters 0%; Professional degrees 71.4% p = 0.082 Monthly income 5: low (not specified) p = 0.023 |
| Shapiro et al. [29] | Routine childhood vaccinations in country vaccination schedules | Individual respondent (not stated if head of household): Employment status (unemployed, retired, student v. employed full or part-time) Transnational level: Income level of a country defined by World Bank: Middle- v. High-income | Outcome: Any missed or delayed vaccinations during the pandemic. Individual level: OR by employment status adjusted for COVID-19 risk factors, respondent’s sex, age, psychological distress, household size, and the number of children. Transnational level: Frequencies by middle-and high-income countries compared by t-tests (p values) | Missed childhood vaccinations: By employment status (not working reference) stratified by country income group: Working (Middle-income countries) AOR 1.38 (95% CI 1.14,1.67). Working (High-income countries) AOR 1.75 (1.36,2.25) Transnational level: Middle income countries 7.6% v. High-income countries 3.0% (p value < 0.05) |
| Silveira MF et al. [27] | Pentavalent (HepB+Hib+DTaP), MMR, HepB, BCG, OPV | Household wealth quintiles (based on household assets and characteristics of the building) | The proportion (95% CI) of children with any missed dose of scheduled vaccines under 3 years of age (schedule of vaccinations in 2nd year not specified) was analysed from questionnaire responses and vaccination card records by wealth quintiles | Missed vaccination–questionnaire responses: Wealth quintile: Q1(poorest) 22.5%(95% CI 19.3,26.2); Q2 21.0%(17.7,24.7); Q3 17.0%(13.9,20.6); Q4 17.5%(14.0,21.6); Q5 (wealthiest) 15.0%(11.6,19.1) p for linear trend = 0.03. Vaccination card record: Wealth quintile: Q1 24.5%(20.6,28.8); Q2 24.5%(20.2,29.4); Q3 19.0%(15.0,23.7); Q4 17.8%(13.6,23.0); Q5 15.6%(11.3,21.1) p for linear trend = 0.01. |
| Tegegne W et al. [26] | Pentavalent (HepB+Hib+DTaP), Measles, ROTA, PCV, BCG, IPV/OPV | Maternal Education: Cannot read or write Able to read or write Primary and Secondary SchoolDiploma, Degree and above | OR with 95% CI for incomplete vaccination (defined as a child who missed at least one dose of the included vaccines) by maternal education adjusted for marital status, place of delivery, waiting time at a health facility, means of transportation to a health facility | Incomplete vaccination by maternal education (Diploma, degree or above as a reference): Can not read or write: AOR 5.08 (95% CI 2.31,11.14); Can read or write: AOR 3.46 (1.31,12.86); Primary and Secondary school: AOR 3.54(1.59,7.89) |
3.2. Risk of Bias Assessment
A Narrative Synthesis of Outcomes
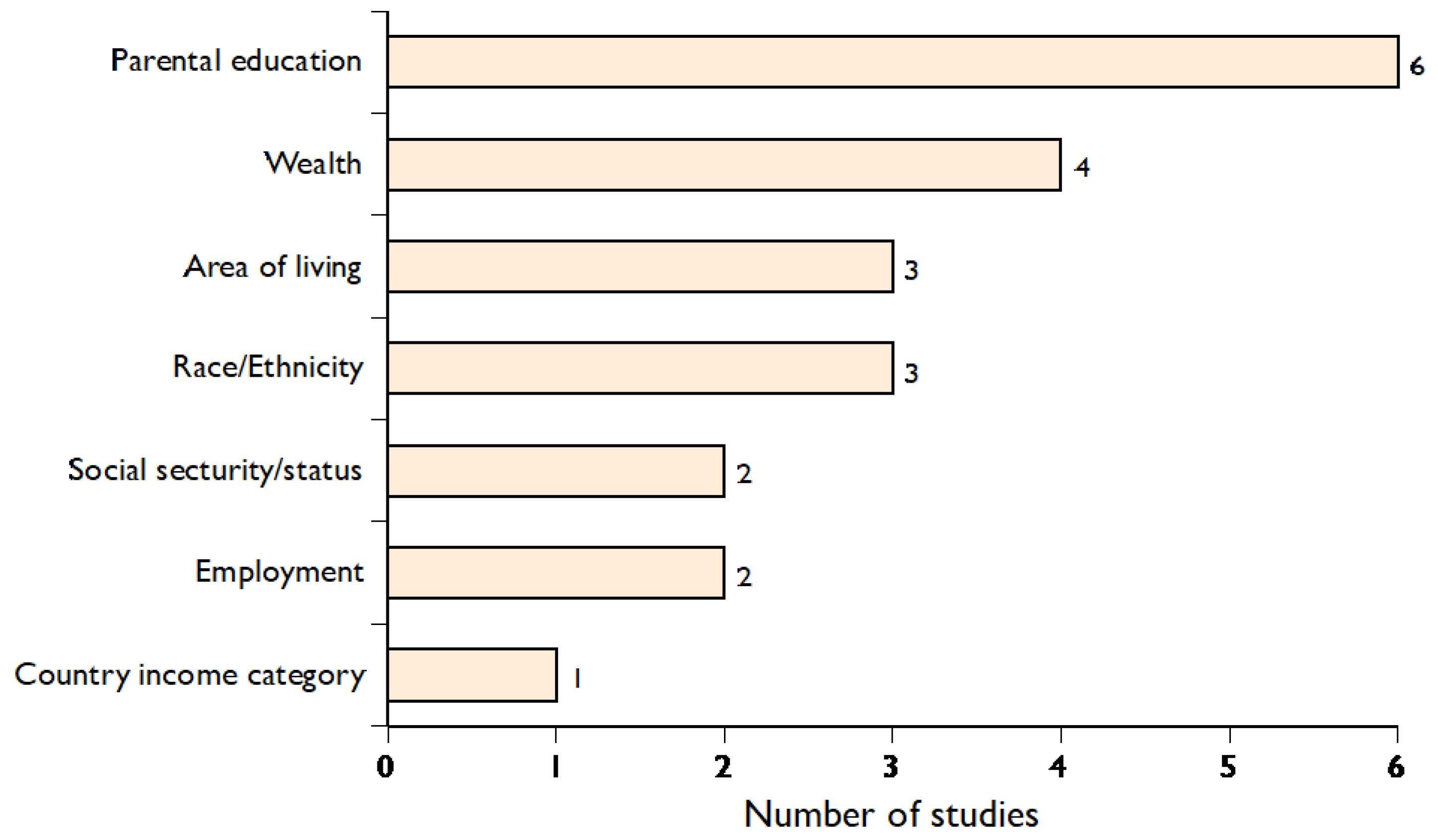
3.3. Narrative Synthesis of Outcome 1: Change in Routine Childhood Vaccination during the COVID-19 Pandemic by Equity Stratifiers
3.3.1. Parental Education
3.3.2. Other Equity Stratifiers
3.4. Narrative Synthesis of Outcome 2: Change in Inequity in Routine Childhood Vaccination Coverage during the COVID-19 Pandemic Compared with Baseline
3.5. Narrative Synthesis of Outcome 3: Differential Coverage for Specific Vaccines during the COVID-19 Pandemic by Equity Stratifiers
3.6. Narrative Synthesis of Outcome 4: Differential Coverage in Age Groups during the COVID-19 Pandemic by Equity Stratifiers
3.7. Narrative Synthesis of Outcome 5: Inequity in Coverage between HICs and LMICs during the Pandemic
3.8. Outcome 1: Change in Routine Childhood Vaccination Coverage during the COVID-19 Pandemic by Equity Stratifiers
3.9. Outcome 2: Change in Inequity in Routine Childhood Vaccination Coverage during the COVID-19 Pandemic Compared with Baseline
3.10. Outcome 3: Differential Coverage for Individual Vaccines during the COVID-19 Pandemic by Equity Stratifiers
3.11. Outcome 4: Differential Coverage in Age Groups during the COVID-19 Pandemic by Equity Stratifiers
3.12. Outcome 5: Inequity in Coverage between HICs and LMICs during the Pandemic
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Causey, K.; Fullman, N.; Sorensen, R.J.D.; Galles, N.C.; Zheng, P.; Aravkin, A.; Danovaro-Holliday, M.C.; Martinez-Piedra, R.; Sodha, S.V.; Velandia-González, M.P.; et al. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020: A modelling study. Lancet 2021, 398, 522–534. [Google Scholar] [CrossRef]
- Roberts, L. Pandemic brings mass vaccinations to a halt. Science 2020, 368, 116–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO/UNICEF. Immunisation Coverage: Are We Losing Ground? WHO/UNICEF: Geneva, Switzerland, 2009. Available online: https://data.unicef.org/resources/immunization-coverage-are-we-losing-ground/ (accessed on 21 October 2021).
- WHO. State of Inequality: Childhood Immunisation; World Health Organization: Geneva, Switzerland, 2016. Available online: https://www.who.int/docs/default-source/gho-documents/health-equity/16-dec-final-for-web-16147-state-of-inequality-in-childhood-immunization.pdf?Sfvrsn=ac6c954c_2 (accessed on 21 October 2021).
- Josephson, A.; Kilic, T.; Michler, J.D. Socioeconomic impacts of COVID-19 in low-income countries. Nat. Hum. Behav. 2021, 5, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Bambra, C.; Riordan, R.; Ford, J.; Mathews, F. The COVID-19 pandemic and health inequalities. J. Epidemiol. Community Health 2020, 74, 964–968. [Google Scholar] [CrossRef]
- UNICEF. Narrowing the Gaps: The Power of Investing in the Poorest Children; UNICEF: New York, NY, USA, 2017. Available online: https://www.unicef.org/publications/index_96534.html (accessed on 21 October 2021).
- Goldhagen, J.L.; Shenoda, S.; Oberg, C.; Mercer, R.; Kadir, A.; Raman, S.; Waterston, T.; Spencer, N.J. Rights, justice, and equity: A global agenda for child health and wellbeing. Lancet Child Adolesc. Health 2020, 4, 80–90. [Google Scholar] [CrossRef]
- Spencer, N.; Nathawad, R.; Arpin, E.; Johnson, S. Pandemics, epidemics and inequities in routine childhood vaccination coverage: A rapid review. BMJ Paediatr. Open 2020, 4, e000842. [Google Scholar] [CrossRef] [PubMed]
- Chandir, S.; Siddiqui, D.A.; Setayesh, H.; Khan, A.J. Impact of COVID-19 lockdown on uptake of routine immunisation in Karachi, Pakistan. Lancet 2020, 8, e1118-9. [Google Scholar] [CrossRef]
- O’Neill, J.; Tabish, H.; Welsh, V.; Petticrew, M.; Pottie, K.; Clarke, M.; Evans, T.; Pardo, J.P.; Waters, E.; White, H.; et al. Applying an equity lens to interventions: Using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J. Clin. Epidemiol. 2014, 67, 56–64. [Google Scholar] [CrossRef]
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ 2020, 368, 16890. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Pereson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 26 October 2021).
- Chandir, S.; Siddiqui, D.A.; Mehmood, M.; Setayesh, H.; Siddique, M.; Mirza, A.; Soundardjee, R.; Dharma, V.K.; Shah, M.T.; Abdullah, S.; et al. Impact of COVID-19 pandemic response on uptake of routine immunisations in Sindh, Pakistan: An analysis of provincial electronic immunisation registry data. Vaccine 2020, 38, 7146–7155. [Google Scholar] [CrossRef]
- Bell, S.; Clarke, R.; Paterson, P.; Mounier-Jack, S. Parents’ and guardians’ views and experiences of accessing routine childhood vaccinations during the coronavirus (COVID-19) pandemic: A mixed methods study in England. PLoS ONE 2020, 15, e0244049. [Google Scholar] [CrossRef] [PubMed]
- Rizwan, W.; Duggal, M.N.; Rana, M.N.; Rafique, M.; Ghaffar, J.; Sadiq, M. Effect of COVID-19 Pandemic on Vaccination of Children. Under Two Years of Age. Pak. Pediatr. J. 2021, 45, 161–168. [Google Scholar]
- Zhong, Y.; Clapham, E.; Aishworiya, R.; Chua, Y.X.; Mathews, J.; Ong, M.; Wang, J.; Murugasu, B.; Chiang, W.C.; Lee, B.W.; et al. Childhood vaccinations: Hidden impact of COVID-19 on children in Singapore. Vaccine 2021, 39, 780–785. [Google Scholar] [CrossRef]
- Dabo, M.; Samah, Y.; Kande, M.; Sompare, D.; Camara, A.; Dian, B.M.; Solano, S.; Baldé, I.; Fabrice, L.A.T.O.U.; Sylla, Y.; et al. Early effect of the Covid-19 epidemic on vaccine coverage of major antigens in Guinea: An analysis of the interrupted time series of national immunisation coverage. MedRxiv, 2020; preprint. [Google Scholar] [CrossRef]
- Bode, S.M.; Gowda, C.; Mangini, M.; Kemper, A.R. COVID-19 and Primary Measles Vaccination Rates in a Large Primary Care Network. Pediatrics 2021, 147, e2020035576. [Google Scholar] [CrossRef]
- Jain, R.; Chopra, A.; Falézan, C.; Patel, M.; Dupas, P. COVID-19 related immunisation disruptions in Rajasthan, India: A retrospective observational study. Vaccine 2021, 39, 4343–4350. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Montoya, J.; Ballesteros, S.M.; Sotelo, J.C.R.; Cervera, C.L.B.; Barrera-López, P.; De la Hoz-Valle, J.A. Impact of the COVID-19 pandemic on routine childhood immunisation in Colombia. Arch. Dis. Child. 2021, 107, e4. [Google Scholar] [CrossRef]
- DeSilva, M.B.; Haalapa, J.; Vasquez-Benitez, G.; Daley, M.F.; Nordin, J.D.; Klein, N.P.; Henninger, M.L.; Williams, J.T.B.; Hambidge, S.J.; Jackson, M.L.; et al. Association of the COVID-19 Pandemic with Routine Childhood Vaccination Rates and Proportion Up to Date with Vaccinations Across 8 US Health Systems in the Vaccine Safety Datalink. JAMA Pediatr. 2022, 176, 68–77. [Google Scholar] [CrossRef]
- Ackerson, B.K.; Sy, L.S.; Glenn, S.C.; Qian, L.; Park, C.H.; Riewerts, R.J.; Jacobsen, S.J. Pediatric Vaccination During the COVID-19 Pandemic. Pediatrics 2021, 148, e2020047092. [Google Scholar] [CrossRef]
- Bramer, C.A.; Kimmins, L.M.; Swanson, R.; Kuo, J.; Vranesich, P.; Jacques-Carroll, L.A.; Shen, A.K. Decline in Child Vaccination Coverage During the COVID-19 Pandemic—Michigan Care Improvement Registry, May 2016–May 2020. Am. J. Transplant. 2020, 20, 1930. [Google Scholar] [CrossRef]
- Miretu, D.G.; Asfaw, Z.A.; Addis, S.G. Impact of COVID-19 pandemic on vaccination coverage among children aged 15 to 23 months at Dessie town, Northeast Ethiopia, 2020. Hum. Vaccin. Immunother. 2021, 17, 2427–2436. [Google Scholar] [CrossRef]
- Tegegne, A.W.; Gidafie, A.; Mamo, D.G.; Wassie, S.T.; Mengie, Z.A. Immunisation Status and Challenges During COVID-19 and Associated Factors Among Children Aged 10–23 Months in South Region, Ethiopia 2020. Pediatr. Health Med. Ther. 2021, 12, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Silveira, M.F.; Tonial, C.T.; Maranhão, A.G.K.; Teixeira, A.M.; Hallal, P.C.; Menezes, A.M.B.; Horta, B.L.; Hartwig, F.P.; Barros, A.J.; Victora, C.G. Missed childhood immunisations during the COVID-19 pandemic in Brazil: Analyses of routine statistics and of a national household survey. Vaccine 2021, 39, 3404–3409. [Google Scholar] [CrossRef] [PubMed]
- Hou, Z.; Song, S.; Du, F.; Shi, L.; Zhang, D.; Lin, L.; Yu, H. The Influence of the COVID-19 Epidemic on Prevention and Vaccination Behaviors Among Chinese Children and Adolescents: Cross-sectional Online Survey Study. JMIR Public Health Surveill 2021, 7, e26372. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, G.K.; Gottfredson, N.; Leask, J.; Wiley, K.; Ganter-Restrepo, F.E.; Jones, S.P.; Menning, L.; Brewer, N.T. COVID-19 and missed or delayed vaccination in 26 middle- and high-income countries: An observational survey. Vaccine 2022, 40, 945–952. [Google Scholar] [CrossRef] [PubMed]
- Restrepo-Méndez, M.; Barros, A.; Wong, K.; Johnson, H.L.; Pariyo, G.; França, G.V.; Wehrmeister, F.C.; Victora, C. Inequalities in full immunisation coverage: Trends in low-and middle-income countries. Bull. World Health Organ. 2016, 94, 794–805. [Google Scholar] [CrossRef]
- Roser, R.; Ortiz-Ospina, M. “Measuring progress towards the Sustainable Development Goals”. SDG-Tracker.org, 2018. Available online: https://sdg-tracker.org/good-health (accessed on 27 December 2021).
- Vaccine Coverage Collaborators. Measuring routine childhood vaccination coverage in 204 countries and territories, 1980–2019: A systematic analysis for the Global Burden of Disease Study 2020, Release 1. Lancet 2021, 398, 503–521. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n7. [Google Scholar] [CrossRef]
- Hill, H.A.; Yankey, D.; Elam-Evans, L.D.; Singleton, J.A.; Sterrett, N. Vaccination Coverage by Age 24 Months Among Children Born in 2017 and 2018—National Immunization Survey-Child, United States, 2018–2020. MMWR 2021, 70, 1435–1440. [Google Scholar] [CrossRef]
- The Lancet Child Adolescent Health. Childhood vaccinations: Playing catch-up. Lancet Child Adolesc. Health 2021, 5, 605. [Google Scholar] [CrossRef]
- WHO. Pulse Survey on Continuity of Essential Health Services during the COVID-19 Pandemic. Interim Report; World Health Organization: Genva, Switzerland, 2020.
- UN Development Programme. Impact of COVID-19 on the Sustainable Development Goals: Pursuing the Sustainable Development Goals (SDGs) in a World Reshaped by COVID-19. 2 December 2020. Available online: https://sdgintegration.undp.org/sites/default/files/Impact_of_COVID-19_on_the_SDGs.pdf (accessed on 7 December 2021).
- Demographic and Health Surveys. Available online: https://dhsprogram.com/ (accessed on 12 December 2021).
- UNICEF. Multiple Indicator Cluster Surveys; UNICEF: New York, NY, USA. Available online: https://mics.unicef.org/ (accessed on 12 December 2021).


| Selection | Comparability | Outcome | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Author | Representative of Exposed Children (Low Social Group) in the Population: Yes */Partly */No/Not Stated | Non-Exposed Children (Higher Social Group) from the Same Population: Yes */No/Not Stated | Ascertainment of Exposure (Social Group): Administrative Records */Structured Interview */Self-Report/Not Stated | Change in Coverage Data Collected during the Period of the Pandemic Not Before: Yes */No | Study Controls for Potential Confounding Variables: Yes */No | Ascertainment of Vaccine Coverage: Data Linkage */Self-Report/Not Stated | Was the Period of Ascertainment Adequate to Identify a Difference in Coverage: Yes */No/Not Stated | Adequacy of Follow-Up: All Children Accounted For */>70% Accounted For */<70% Acoounted For/Not Stated | No. of Stars |
| Ackerson et al. [23] | Partly * | Yes * | Administrative records * | Yes * | Yes * | Data Linkage * | Yes * | All * | 8 |
| Bell et al. [15] | No | Yes * | Structured interview * | Yes * | Yes * | Self-Report | Yes * | >70% * | 6 |
| Bramer et al. [24] | Not Stated | Yes * | Administrative records * | Yes * | No | Data Linkage * | Yes * | All * | 6 |
| Chandir et al. [14] | Yes * | Yes * | Administrative records * | Yes * | Yes * | Data Linkage * | Yes * | All * | 8 |
| DeSilva et al. [22] | Yes * | Yes * | Administrative records * | Yes * | No | Data Linkage * | Yes * | All * | 7 |
| Hou et al. [28] | Partly * | Yes * | Structured interview * | Yes * | Yes * | Self-Report | Yes * | >70% * | 7 |
| Jain et al. [20] | Partly * | Yes * | Structured interview * | Yes * | Yes * | Self-Report | Yes * | >70% * | 7 |
| Miretu et al. [25] | Partly * | Yes * | Structured interview * | Yes * | Yes * | Self-Report & Vacc Cards | Yes * | All * | 7 |
| Moreno-Montoya et al. [21] | Yes * | Yes * | Administrative records * | Yes * | Yes * | Data Linkage * | Yes * | All * | 8 |
| Rizwan et al. [16] | No | Yes * | Structured interview * | Yes * | No | Self-Report & Vacc Cards | Yes * | Not Stated | 4 |
| Shapiro et al. [29] | Partly * | Yes * | Structured interview * | Yes * | Yes * | Self-Report | Yes * | Not Stated | 6 |
| Silveira et al. [27] | Partly * | Yes * | Structured interview* | Yes * | No | Self-Report and Vacc Card | Yes * | <70% | 5 |
| Tegegne et al. [26] | Partly * | Yes * | Structured interview * | Yes * | Yes * | Self-Report | Yes * | Not Stated | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spencer, N.; Markham, W.; Johnson, S.; Arpin, E.; Nathawad, R.; Gunnlaugsson, G.; Homaira, N.; Rubio, M.L.M.; Trujillo, C.J. The Impact of COVID-19 Pandemic on Inequity in Routine Childhood Vaccination Coverage: A Systematic Review. Vaccines 2022, 10, 1013. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10071013
Spencer N, Markham W, Johnson S, Arpin E, Nathawad R, Gunnlaugsson G, Homaira N, Rubio MLM, Trujillo CJ. The Impact of COVID-19 Pandemic on Inequity in Routine Childhood Vaccination Coverage: A Systematic Review. Vaccines. 2022; 10(7):1013. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10071013
Chicago/Turabian StyleSpencer, Nicholas, Wolfgang Markham, Samantha Johnson, Emmanuelle Arpin, Rita Nathawad, Geir Gunnlaugsson, Nusrat Homaira, Maria Lucia Mesa Rubio, and Catalina Jaime Trujillo. 2022. "The Impact of COVID-19 Pandemic on Inequity in Routine Childhood Vaccination Coverage: A Systematic Review" Vaccines 10, no. 7: 1013. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10071013