
A Systematic Review on the Emergence of Omicron Variant and Recent Advancement in Therapies
 , ,
, ,  and
and
Abstract
:1. Introduction
2. The Emergence of the Omicron (B.1.1.529) Variant and Its Sub-Lineage
3. Mechanism of Omicron Variant
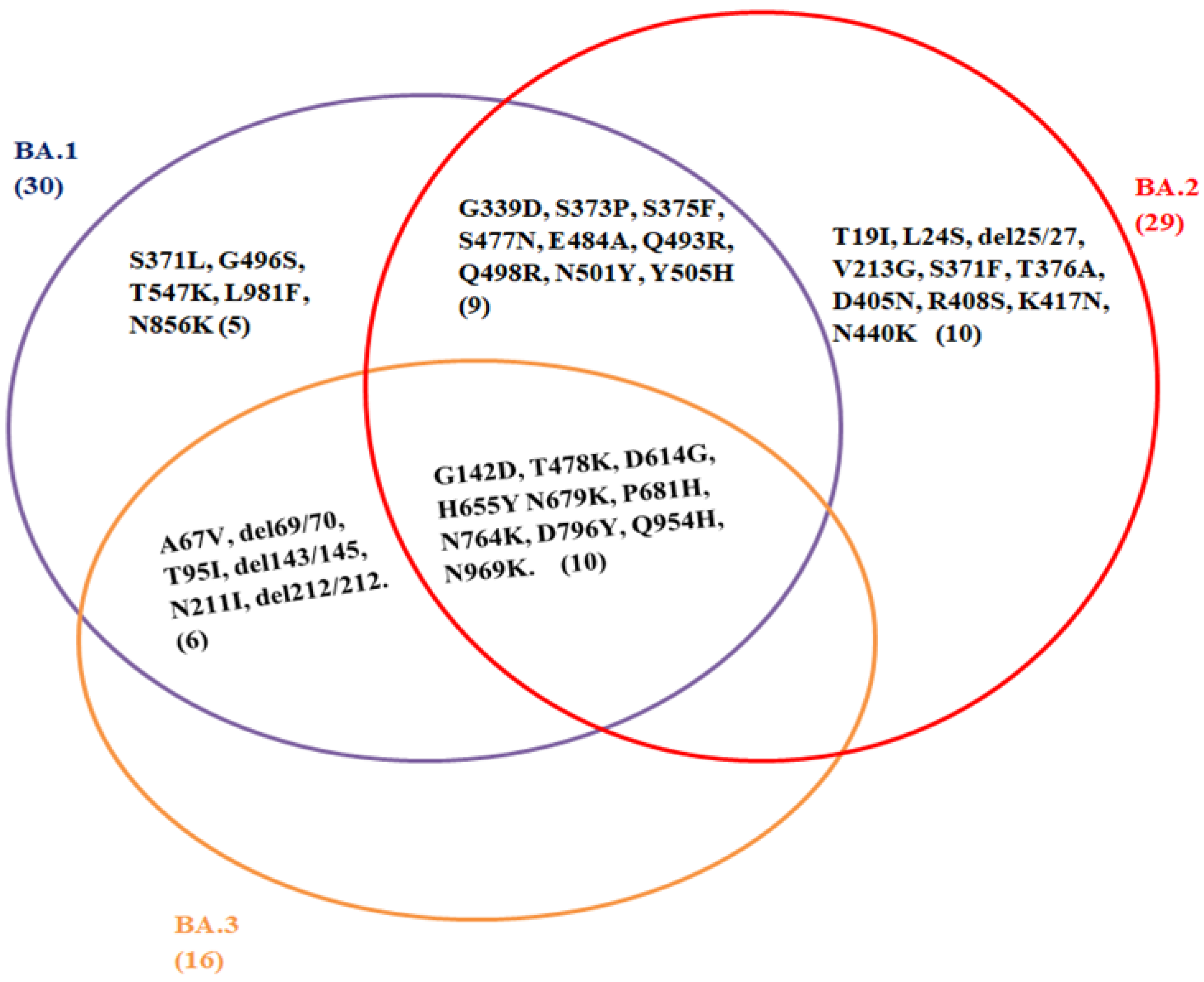
4. Mutations in Omicron Variant
5. Impact of Diagnosis on the Omicron Variant
6. Advancement in Therapeutics Drugs
6.1. Immunomodulatory Drugs
6.2. Antivirals Therapy
6.3. Monoclonal Antibodies
6.3.1. Bamlanivimab and Etesevimab
6.3.2. Casirivimab and Imdevimab mAb
6.3.3. Sotrovimab
6.3.4. Tixagevimab Plus Cilgavimab
6.3.5. Bebtelovimab (LY-CoV1404)

{kind=link}
| Drugs | Dosage | Method of Administration | Duration | Side Effect | Mode of Action | Efficacy of Monoclonal Antibodies/ Drugs against SARS-CoV-2 Variants | Reference |
|---|---|---|---|---|---|---|---|
| Sarilumab | Single dose of sarilumab 400 mg | Intravenous infusion | Sarilumab infusion should be used within 4 h of preparation | Neutropenia, thrombocytopenia and GI perforation | Suppress cytokine storm | Effective against COVID-19 | [61,63,65] |
| Tocilizumab (Actemra) | 12 mg/kg in patients weighing <30 kg and 8 mg/kg in those weighing ≥30 kg (max dose 800 mg) | Intravenous infusion | Administered as a single IV infusion over 60 min | Neutropenia, thrombocytopenia, serum hepatic transaminase elevations, gastrointestinal perforations, and anaphylaxis | Inhibits binding of the proinflammatory cytokine IL-6 to its receptors | Effective against COVID-19 | [61,65] |
| Dexamethasone (DEX) | DEX 6 mg | Orally or Intravenous infusion | Once daily for up to 10 days or until hospital discharge, whichever comes first | Avascular necrosis, Adrenal insufficiency, Increased BP, Peripheral edema, and Myopathy | Suppress inflammation | Effective against COVID-19 | [65] |
| Baricitinib (Olumiant) | 4 mg | Orally | Once daily while hospitalized for up to 14 days | Lymphoma and other malignancies, Thrombosis, GI perforation and serious cardiac-related events (e.g., MI, stroke) | Inhibits viral endocytosis | Effective against COVID-19 | [65] |
| Remdesivir (Veklury) | 200 mg IV on day 1, followed by 100 mg once daily | Intravenous infusion | Treatment duration is 5–10 days | Nausea, Hypersensitivity reactions | Inhibits viral RNA-dependent RNA polymerase | Active against Omicron and all other variants: Alpha, Beta, Gamma and Delta | [70,71] |
| Molnupiravir | 800 mg every 12 h | Orally | Treatment should be started within 5 days of symptom onset | Diarrhea, nausea, and dizziness | Targets viral RNA polymerase, inducing mutagenesis and inhibiting SARS-CoV-2 replication | Active against the entire variants: Alpha, Beta, Gamma, Delta and Omicron | [69,71] |
| Paxlovid (Ritonavir-Boosted Nirmatrelvir) | 300/100 mg (2 nirmatrelvir tablets and 1 ritonavir tablet taken together) twice daily | Orally | Treatment should be started within 5 days of symptom onset | Dysgeusia, diarrhea, hypertension, and myalgia | Inhibits the SARS-CoV-2 main protease (Mpro), preventing viral replication. | Active against entire SARS-CoV-2 variant including, omicron | [71] |
| Bamlanivimab Plus etesevimab | 700 mg (one vial) of Bamlanivimab and 1400 mg (two vials) of etesevimab | single Intravenous infusion | One-time dose right after COVID-positive test and within 10 days after the onset of infection symptoms | Bleeding, bruising, pain, soreness, or swelling at injection sit | Binds to spike protein RBD of SARS-CoV-2 | Active against two SARS-CoV-2 variant: Alpha and Delta | [76,77,81] |
| Casirivimab plus imdevimab (REGEN-COV) | 600 mg of casirivimab and 600 mg of imdevimabis diluted together in 50, 100, 150, or 250 mL of normal saline at a maximum rate of 310 mL/hr (180 mL/hr if diluted in 50 mL) | Intravenous infusion or Subcutaneous injection | After a positive SARS-CoV-2 test result and within 10 days of COVID-19 symptom onset | Pain, bleeding, bruising of the skin, soreness, swelling, or infection at injection site | Bind at different sites on the RBD of the spike protein of SARS-CoV-2. | Active against all SARS-CoV-2 variant: Alpha, Beta, Gamma, Delta, Omicron | [77,79,82] |
| Sotrovimab | 500 mg of sotrovimab diluted in 50 or 100 mL of normal saline | Intravenous infusion | After a positive viral test for SARS-CoV-2 and within 10 days of symptom onset | Rash (2%) and diarrhea (1%). Hypersensitivity reactions, including anaphylaxis | Binds at the epitope sites on the spike protein and prevent membrane fusion after the virus binds to the human ACE2 receptor | Active against the entire variants: Alpha, Beta, Gamma, Delta and Omicron | [75,78,84] |
| Tixagevimab plus cilgavimab | 150 mg of each antibody is administered. | Intramuscular injection | one time as two shots (one after another) | Headache (6%) and fatigue (4%). | Binds to non-overlapping region of the SARS-CoV-2 spike protein. | Active against the entire variants: Alpha, Beta, Gamma, Delta and Omicron | [75,78,85] |
| Bebtelovimab | 175 mg/2 mL vials | Intravenous infusion | Treatment should be started within 7 days of symptom onset | Rash, pruritus, and infusion-related reactions | Binds to the spike protein and prevents its attachment to the human receptor | Active against the Omicron variant of SARS-CoV-2 (Neutralize BA.1 and BA.2omicron variant) | [76] |
7. Discussion
8. Conclusions and Prospect
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. 2022. Available online: https://covid19.who.int/ (accessed on 14 February 2022).
- Rahmani, S.; Rezaei, N. Omicron (B.1.1.529) variant: Development, dissemination, and dominance. J. Med. Virol. 2021, 94, 1787–1788. [Google Scholar] [CrossRef] [PubMed]
- Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/activities/tracking-SARS-CoV-2-variants/ (accessed on 20 February 2022).
- World Health Organization (WHO). Classification of Omicron (B.1.1.529): SARSCoV-2 Variant of Concern. 2021. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 5 January 2022).
- UNICEF. What We Know about the Omicron Variant. Available online: https://www.unicef.org/coronavirus/what-we-know-about-omicron-variant (accessed on 16 February 2022).
- CDC. Science Brief: Omicron (B.1.1.529) Variant (Updated 2 December 2021). Available online: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/scientific-brief-omicron-variant.html (accessed on 16 February 2022).
- UK Health Security Agency. SARS-CoV-2 Variants of Concern and Variants under Investigation. 26 November 2021. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1036501/Technical_Briefing_29_published_26_November_2021.pdf (accessed on 14 February 2022).
- Harvard Medical School. Coronavirus Resource Center—Harvard Health. Harvard Health Publishing. Lab Studies, Animal Studies, and Epidemiological Data All Indicate That Omicron May Cause Less Severe Disease Than Previous Variants. Available online: https://www.health.harvard.edu/diseases-and-conditions/coronavirus-resource-center (accessed on 11 January 2022).
- Leonhardt, D. Omicron Is Milder. The New York Times, 5 January 2022. Available online: https://www.nytimes.com/2022/01/05/briefing/omicron-risk-milder-pandemic.html(accessed on 7 January 2022).
- Petersen, E.; Ntoumi, F.; Hui, D.S.; Abubakar, A.; Kramer, L.D.; Obiero, C.; Tambyah, P.A.; Blumberg, L.; Yapi, R.; Al-Abri, S.; et al. Emergence of new SARS-CoV-2 Variant of Concern Omicron (B.1.1.529)—Highlights Africa’s research capabilities, but exposes major knowledge gaps, inequities of vaccine distribution, inadequacies in global COVID-19 response and control efforts. Int. J. Infect. Dis. 2022, 114, 268–272. [Google Scholar] [CrossRef] [PubMed]
- Mohapatra, R.K.; Sarangi, A.K.; Kandi, V.; Azam, M.; Tiwari, R.; Dhama, K. Omicron (B.1.1.529 variant of SARS-CoV-2); An emerging threat: Current global scenario. J. Med. Virol. 2021, 94, 1780–1783. [Google Scholar] [CrossRef]
- WHO. Less than 10% of African Countries to Hit Key COVID-19 Vaccination Goal. 2021. Available online: https://www.afro.who.int/news/less-10-african-countries-hit-key-covid-19-vaccination-goal (accessed on 28 November 2021).
- Maruki, T.; Iwamoto, N.; Kanda, K.; Okumura, N.; Yamada, G.; Ishikane, M.; Ujiie, M.; Saito, M.; Fujimoto, T.; Kageyama, T.; et al. Two cases of breakthrough SARS-CoV-2 infections caused by the Omicron variant (B.1.1.529 lineage) in international travelers to Japan. Clin. Infect. Dis. 2022, 75, e354–e356. [Google Scholar] [CrossRef] [PubMed]
- First Omicron Cases Detected in India. Available online: https://thehill.com/policy/international/583965-first-omicron-cases-detected-in-india (accessed on 6 January 2022).
- Germany Reports First Two Cases of Omicron Variant. Available online: https://www.thejournal.ie/germany-omicron-coronavirus-covid-19-bavaria-5613843-Nov2021/ (accessed on 6 January 2022).
- GISAID. Tracking of Variants. 2021. Available online: https://www.gisaid.org/hcov19-variants/ (accessed on 30 November 2021).
- Jansen, L.; Tegomoh, B.; Lange, K.; Showalter, K.; Figliomeni, J.; Abdalhamid, B.; Iwen, P.C.; Fauver, J.; Buss, B.; Donahue, M. Investigation of a SARS-CoV-2 B.1.1.529 (omicron) variant cluster—Nebraska, november-december 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1782–1784. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Infectious Diseases, Japan. Active Epidemiological Investigation on SARS-CoV-2 Infection Caused by Omicron Variant (Pango Lineage B.1.1.529 in Japan: Preliminary Report on Infectious Period. 2022. Available online: https://www.niid.go.jp/niid/en/2019-ncov-e/10884-covid19-66-en.html (accessed on 22 January 2022).
- UK Health Security Agency. SARS-CoV-2 Variants of Concern and Variants under Investigation in England. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1050999/Technical-Briefing-35-28January2022.pdf (accessed on 6 February 2022).
- Washington Post. There’s a New Version of Omicron but So Far It Doesn’t Appear to Be More Dangerous. Available online: https://www.stripes.com/covid/2022-01-25/new-omicron-version-mutation-BA-2-4405690.html (accessed on 25 January 2022).
- Outbreak.Info. BA.2 Lineage Report. Available online: https://outbreak.info/situation-reports?pango=BA.2 (accessed on 11 February 2022).
- Lyngse, F.P.; Kirkeby, C.; Denwood, M.; Christiansen, L.E.; Mølbak, K.; Møller, C.H.; Skov, R.; Krause, T.; Rasmussen, M.; Sieber, R.; et al. Transmission of SARS-CoV-2 Omicron VOC subvariants BA.1 and BA.2: Evidence from Danish Households. medRxiv 2022. [Google Scholar] [CrossRef]
- Omicron BA.2: What We Know about the Covid Sub-Variant. Available online: https://www.bbc.com/news/health-60233899 (accessed on 7 February 2022).
- GISAID. hCoV-19 Tracking of Variants. Available online: https://www.epicov.org/epi3/frontend#58aca (accessed on 10 February 2022).
- Kupferschmidt, K.; Vogel, G. How bad is Omicron? Some clues are emerging. Science 2021, 374, 1304–1305. [Google Scholar] [CrossRef]
- Wahid, M.; Jawed, A.; Mandal, R.K.; Dailah, H.G.; Janahi, E.M.; Dhama, K.; Somvanshi, P.; Haque, S. Variants of SARS-CoV-2, their effects on infection, transmission and neutralization by vaccine-induced antibodies. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 5857–5864. [Google Scholar] [CrossRef]
- Lupala, C.S.; Ye, Y.; Chen, H.; Su, X.-D.; Liu, H. Mutations on RBD of SARS-CoV-2 Omicron variant result in stronger binding to human ACE2 receptor. Biochem. Biophys. Res. Commun. 2022, 590, 34–41. [Google Scholar] [CrossRef]
- Jackson, C.B.; Farzan, M.; Chen, B.; Choe, H. Mechanisms of SARS-CoV-2 entry into cells. Nat. Rev. Mol. Cell Biol. 2022, 23, 3–20. [Google Scholar] [CrossRef]
- Willett, B.J.; Grove, J.; MacLean, O.A.; Wilkie, C.; Logan, N.; De Lorenzo, G.; Furnon, W.; Scott, S.; Manali, M.; Szemiel, A.; et al. The hyper-transmissible SARS-CoV-2 Omicron variant exhibits significant antigenic change, vaccine escape and a switch in cell entry mechanism. medRxiv 2022, 23, 3–20. [Google Scholar] [CrossRef]
- Saxena, S.K.; Kumar, S.; Ansari, S.; Paweska, J.T.; Maurya, V.K.; Tripathi, A.K.; Abdel-Moneim, A.S. Characterization of the novel SARS-CoV-2 omicron (B.1.1.529) variant of concern and its global perspective. J. Med. Virol. 2021, 94, 1738–1744. [Google Scholar] [CrossRef]
- Wu, L.; Zhou, L.; Mo, M.; Liu, T.; Wu, C.; Gong, C.; Lu, K.; Gong, L.; Zhu, W.; Xu, Z. SARS-CoV-2 Omicron RBD shows weaker binding affinity than the currently dominant Delta variant to human ACE2. Signal Transduct. Target. Ther. 2022, 7, 8. [Google Scholar] [CrossRef]
- Korber, B.; Fischer, W.M.; Gnanakaran, S.; Yoon, H.; Theiler, J.; Abfalterer, W.; Hengartner, N.; Giorgi, E.E.; Bhattacharya, T.; Foley, B.; et al. Tracking Changes in SARS-CoV-2 Spike: Evidence that D614G Increases Infectivity of the COVID-19 Virus. Cell 2020, 182, 812–827.e19. [Google Scholar] [CrossRef]
- Corum, J.; Zimmer, C. Tracking Omicron and Other Coronavirus Variants. 2021. Available online: https://www.nytimes.com/interactive/2021/health/coronavirus-variant-tracker.html (accessed on 7 January 2022).
- Poudel, S.; Ishak, A.; Perez-Fernandez, J.; Garcia, E.; León-Figueroa, D.A.; Romaní, L.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Highly mutated SARS-CoV-2 Omicron variant sparks significant concern among global experts—What is known so far? Travel Med. Infect. Dis. 2022, 45, 102234. [Google Scholar] [CrossRef]
- Science the Wire. A ‘Stealth’ Version of Omicron Could Challenge Surveillance Efforts. Available online: https://science.thewire.in/external-affairs/world/ba-2-sublineage-omicron-s-gene-target-failure-surveillance/ (accessed on 7 January 2022).
- Kazybay, B.; Ahmad, A.; Mu, C.; Mengdesh, D.; Xie, Y. Omicron N501Y mutation among SARS-CoV-2 lineages: Insilico analysis of potent binding to tyrosine kinase and hypothetical repurposed medicine. Travel Med. Infect. Dis. 2022, 45, 102242. [Google Scholar] [CrossRef]
- Mannar, D.; Saville, J.W.; Zhu, X.; Srivastava, S.S.; Berezuk, A.M.; Tuttle, K.S.; Marquez, A.C.; Sekirov, I.; Subramaniam, S. SARS-CoV-2 Omicron variant: Antibody evasion and cryo-EM structure of spike protein-ACE2 complex. Science 2022, 375, 760–764. [Google Scholar] [CrossRef]
- McCallum, M.; Czudnochowski, N.; Rosen, L.E.; Zepeda, S.K.; Bowen, J.E.; Walls, A.C.; Hauser, K.; Joshi, A.; Stewart, C.; Dillen, J.R.; et al. Structural basis of SARS-CoV-2 Omicron immune evasion and receptor engagement. Science 2022, 375, 846–868. [Google Scholar] [CrossRef]
- Liu, Z.; VanBlargan, L.A.; Bloyet, L.-M.; Rothlauf, P.W.; Chen, R.E.; Stumpf, S.; Zhao, H.; Errico, J.M.; Theel, E.S.; Liebeskind, M.J.; et al. Identification of SARS-CoV-2 spike mutations that attenuate monoclonal and serum antibody neutralization. Cell Host Microbe 2021, 29, 477–488.e4. [Google Scholar] [CrossRef]
- Quarleri, J.; Galvan, V.; Delpino, M.V. Omicron variant of the SARS-CoV-2: A quest to define the consequences of its high mutational load. Geroscience 2022, 44, 53–56. [Google Scholar] [CrossRef]
- Negi, S.S.; Schein, C.H.; Braun, W. Regional and temporal coordinated mutation patterns in SARS-CoV-2 spike protein revealed by a clustering and network analysis. Sci. Rep. 2022, 12, 1128. [Google Scholar] [CrossRef]
- Leary, S.; Gaudieri, S.; Parker, M.D.; Chopra, A.; James, I.; Pakala, S.; Alves, E.; John, M.; Lindsey, B.B.; Keeley, A.J.; et al. Generation of a novel SARS-CoV-2 sub-genomic RNA due to the R203K/G204R variant in nucleocapsid: Homologous recombination has potential to change SARS-CoV-2 at both protein and RNA level. Pathog. Immun. 2021, 6, 27–49. [Google Scholar] [CrossRef]
- Mourier, T.; Shuaib, M.; Hala, S.; Mfarrej, S.; Alofi, F.; Naeem, R.; Alsomali, A.; Jorgensen, D.; Subudhi, A.K.; Ben, R.F.; et al. SARS-CoV-2 genomes from Saudi Arabia implicate nucleocapsid mutations in host response and increased viral load. Nat. Commun. 2022, 13, 601. [Google Scholar] [CrossRef]
- Kannan, S.R.; Spratt, A.N.; Sharma, K.; Chand, H.S.; Byrareddy, S.N.; Singh, K. Omicron SARS-CoV-2 variant: Unique features and their impact on pre-existing antibodies. J. Autoimmun. 2022, 126, 102779. [Google Scholar] [CrossRef]
- Karim, S.S.A.; Karim, Q.A. Omicron SARS-CoV-2 variant: A new chapter in the COVID-19 pandemic. Lancet 2021, 398, 2126–2128. [Google Scholar] [CrossRef]
- World Health Organization. Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2020-DON305 (accessed on 22 June 2021).
- Therapeutic Goods Administration (TGA). COVID-19 Rapid Antigen Self-Tests That Are Approved in Australia. Available online: https://www.tga.gov.au/covid-19-rapid-antigen-self-tests-are-approved-australia (accessed on 15 December 2021).
- Nordgren, J.; Sharma, S.; Olsson, H.; Jämtberg, M.; Falkeborn, T.; Svensson, L.; Hagbom, M. SARS-CoV-2 rapid antigen test: High sensitivity to detect infectious virus. J. Clin. Virol. 2021, 140, 104846. [Google Scholar] [CrossRef]
- Deerain, J.; Druce, J.; Tran, T.; Batty, M.; Yoga, Y.; Fennell, M.; Dwyer, D.E.; Kok, J.; Williamson, D.A. Assessment of the Analytical Sensitivity of 10 Lateral Flow Devices against the SARS-CoV-2 Omicron Variant. J. Clin. Microbiol. 2022, 60, e0247921. [Google Scholar] [CrossRef]
- Bekliz, M.; Perez-Rodriguez, F.; Puhach, O.; Adea, K.; Melancia, S.M.; Baggio, S.; Corvaglia, A.; Jacquerioz-Bausch, F.; Alvarez, C.; Essaidi-Laziosi, M.; et al. Sensitivity of SARS-CoV-2 antigen-detecting rapid tests for Omicron variant. medRxiv 2021. [Google Scholar] [CrossRef]
- U.S. Food & Drug Administration. SARS-CoV-2 Viral Mutations: Impact on COVID-19 Tests. Available online: https://www.fda.gov/medical-devices/coronavirus-covid-19-and-medical-devices/sars-cov-2-viral-mutations-impact-covid-19-tests.ccessed (accessed on 6 January 2022).
- Comparative Evaluation of the Sensitivity of SARS-CoV-2 Rapid Antigen Tests (Self-Tests + Rapid Tests). Available online: https://www.pei.de/DE/newsroom/dossier/coronavirus/testsysteme.html (accessed on 6 January 2022).
- Adamson, B.; Sikka, R.; Wyllie, A.L.; Premsrirut, P. Discordant SARS-CoV-2 PCR and Rapid Antigen Test Results When Infectious: A December 2021 Occupational Case Series. medRxiv 2021. [Google Scholar] [CrossRef]
- Schrom, J.; Marquez, C.; Pilarowski, G.; Wang, G.; Mitchell, A.; Puccinelli, R.; Black, D.; Rojas, S.; Ribeiro, S.; Martinez, J.; et al. Direct Comparison of SARS Co-V-2 Nasal RT- PCR and Rapid Antigen Test (BinaxNOW™) at a Community Testing Site During an Omicron Surge. medRxiv 2022, 22268954. [Google Scholar] [CrossRef]
- Surasi, K.; Cummings, K.J.; Hanson, C.; Morris, M.K.; Salas, M.; Seftel, D.; Ortiz, L.; Thilakaratne, R.; Stainken, C.; Wadford, D.A. Effectiveness of Abbott BinaxNOW Rapid Antigen Test for Detection of SARS-CoV-2 Infections in Outbreak among Horse Racetrack Workers, California, USA. Emerg. Infect. Dis. 2021, 27, 2761–2767. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Adeli, K.; Plebani, M. Commercial immunoassays for detection of anti-SARS-CoV-2 spike and RBD antibodies: Urgent call for validation against new and highly mutated variants. Clin. Chem. Lab. Med. 2022, 60, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Metzger, C.M.J.A.; Lienhard, R.; Seth-Smith, H.M.B.; Roloff, T.; Wegner, F.; Sieber, J.; Bel, M.; Greub, G.; Egli, A. PCR performance in the SARS-CoV-2 Omicron variant of concern? Swiss Med. Wkly. 2021, 151, w30120. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.Y.L.; Chong, Y.M.; Sam, I.C.; Chan, Y.F. SARS-CoV-2 multiplex RT-PCR to detect variants of concern (VOCs) in Malaysia, between January to May 2021. J. Virol. Methods 2022, 301, 114462. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Science Brief: Emerging SARSCoV-2 Variants. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/scientific-brief-emerging-variants.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F201,%209-ncov%2Fmore%2Fscience-and-research%2Fscientific-brief-emerging-variants.html (accessed on 5 January 2022).
- IGM Biosciences Advances Novel Antibody IGM-6268 into Clinical Trials for the Treatment and Prevention of COVID-19. Available online: https://www.biospace.com/article/releases/igm-biosciences-advances-novel-antibody-igm-6268-into-clinical-trials-for-the-treatment-and-prevention-of-covid-19-/ (accessed on 20 February 2022).
- Chamlagain, R.; Shah, S.; Paudel, B.S.; Dhital, R.; Kandel, B. Efficacy and Safety of Sarilumab in COVID-19: A Systematic Review. Interdiscip. Perspect. Infect. Dis. 2021, 2021, 8903435. [Google Scholar] [CrossRef]
- CORIMUNO-19 Collaborative Group. Sarilumab in adults hospitalised with moderate-to-severe COVID-19 pneumonia (CORIMUNO-SARI-1): An open-label randomised controlled trial. Lancet Rheumatol. 2022, 4, E24–E32. [Google Scholar] [CrossRef]
- WHO Approves 2 New COVID-19 Treatments Amid Omicron. Available online: https://www.thevibes.com/articles/world/52032/who-approves-2-new-covid-19-treatments-amid-omicron (accessed on 19 February 2022).
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Therapeutic Management of Hospitalized Adults with COVID-19. Available online: https://www.covid19treatmentguidelines.nih.gov/management/clinical-management/hospitalized-adults--therapeutic-management/ (accessed on 19 February 2022).
- Fahnøe, U.; Ronit, A.; Berg, R.M.G.; Jørgensen, S.E.; Mogensen, T.H.; Underwood, A.P.; Scheel, T.K.H.; Bukh, J.; Plovsing, R.R. A distinct dexamethasone- dependent gene expression profile in the lungs of COVID-19 patients. J. Infect. Dis. 2022, jiac218. [Google Scholar] [CrossRef]
- Coronavirus (COVID-19) Update: FDA Authorizes First Oral Antiviral for Treatment of COVID-19. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-first-oral-antiviral-treatment-covid-19 (accessed on 19 February 2022).
- Paxlovid for Treatment of COVID-19. Available online: https://secure.medicalletter.org/w1642a (accessed on 19 February 2022).
- FDA. Fact Sheet for Health Care Providers: Emergency Use Authorization for Molnupiravir. Available online: https://www.fda.gov/media/155054/download?utm_medium=email&utm_source=govdelivery (accessed on 19 February 2022).
- FDA Approves First Treatment for COVID-19. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-treatment-covid-19 (accessed on 19 February 2022).
- Vangeel, L.; Chiu, W.; De Jonghe, S.; Maes, P.; Slechten, B.; Raymenants, J.; André, E.; Leyssen, P.; Neyts, J.; Jochmans, D. Remdesivir, Molnupiravir and Nirmatrelvir remain active against SARS-CoV-2 Omicron and other variants of concern. Antivir. Res. 2022, 198, 105252. [Google Scholar] [CrossRef]
- Taylor, P.C.; Adams, A.C.; Hufford, M.M.; de la Torre, I.; Winthrop, K.; Gottlieb, R.L. Neutralizing monoclonal antibodies for treatment of COVID-19. Nat. Rev. Immunol. 2021, 21, 382–393. [Google Scholar] [CrossRef]
- Ferré, V.M.; Peiffer-Smadja, N.; Visseaux, B.; Descamps, D.; Ghosn, J.; Charpentier, C. Omicron SARS-CoV-2 variant: What we know and what we don’t. Anaesth. Crit. Care Pain Med. 2022, 4, 100998. [Google Scholar] [CrossRef] [PubMed]
- Dual mAb Therapy Reduces Viral Load in Patients with Mild to Moderate COVID-19. Available online: https://hospitalpharmacyeurope.com/covid-19/dual-mab-therapy-reduces-viral-load-in-patients-with-mild-to-moderate-covid-19/ (accessed on 18 February 2022).
- NIH. COVID-19 Treatment Guidelines; Anti-SARS-CoV-2 Monoclonal Antibodies. Available online: https://www.covid19treatmentguidelines.nih.gov/therapies/anti-sars-cov-2-antibody-products/anti-sars-cov-2-monoclonal-antibodies/ (accessed on 18 February 2022).
- Bebtelovimab (LY-CoV1404) Monoclonal Antibody. Available online: https://www.precisionvaccinations.com/vaccines/bebtelovimab-ly-cov1404-monoclonal-antibody (accessed on 19 February 2022).
- Falcone, M.; Tiseo, G.; Valoriani, B.; Barbieri, C.; Occhineri, S.; Mazzetti, P.; Vatteroni, M.L.; Suardi, L.R.; Riccardi, N.; Pistello, M.; et al. Efficacy of Bamlanivimab/Etesevimab and Casirivimab/Imdevimab in Preventing Progression to Severe COVID-19 and Role of Variants of Concern. Infect. Dis. Ther. 2021, 10, 2479–2488. [Google Scholar] [CrossRef] [PubMed]
- Takashita, E.; Kinoshita, N.; Yamayoshi, S.; Sakai-Tagawa, Y.; Fujisaki, S.; Ito, M.; Iwatsuki-Horimoto, K.; Chiba, S.; Halfmann, P.; Nagai, H.; et al. Efficacy of Antibodies and Antiviral Drugs against Covid-19 Omicron Variant. N. Engl. J. Med. 2022, 386, 995–998. [Google Scholar] [CrossRef] [PubMed]
- Aleem, A.; Akbar Samad, A.B.; Slenker, A.K. Emerging Variants of SARS-CoV-2 and Novel Therapeutics Against Coronavirus (COVID-19); StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK570580 (accessed on 20 May 2022).
- Bamlanivimab and Etesevimab Authorized States, Territories, and U.S. Jurisdictions. Available online: https://www.fda.gov/media/151719/download (accessed on 19 February 2022).
- Medlineplus: Bamlanivimab and Etesevimab Injection. Available online: https://medlineplus.gov/druginfo/meds/a621008.html (accessed on 19 February 2022).
- Therapeutic Antibodies for COVID-19. Available online: https://evidentic.com/therapeutic-antibodies-for-covid-19/ (accessed on 19 February 2022).
- UPDATE—Allocation of Bamlanivimab/Etesevimab and REGEN-COV Therapeutics Paused. Available online: https://www.phe.gov/emergency/events/COVID19/investigation-MCM/Bamlanivimab-etesevimab/Pages/important-update-24Jan2022.aspx (accessed on 19 February 2022).
- Food and Drug Administration. Fact Sheet for Healthcare Providers: Emergency Use Authorization (EUA) of Sotrovimab. 2021. Available online: https://www.fda.gov/media/149534/download (accessed on 19 February 2022).
- Tixagevimab and Cilgavimab (Evusheld) for Pre-Exposure Prophylaxis of COVID-19. Available online: https://secure.medicalletter.org/w1641a (accessed on 19 February 2022).

| WHO Designation | Country First Origin | Pango Lineages | Variant Prevalence Countries as of 11 February 2022 | GISAID | Next Strain | Mutation | Additional Amino Acid Changes Monitored |
|---|---|---|---|---|---|---|---|
| Alpha (18 December 2020) | United Kingdom, September-2020 | 9 Sub-lineages: B.1.1.7, Q.1, Q.4Q.5, Q.8, Q.7, Q.2, Q.6, Q.3. | United Kingdom (262,616) | GRY, GR/501Y.V1 | 20I/501Y.V1, 20B/501Y.V1 | 22 mutations (9 mutation spike protein, with deletion:del69/70, del144/144) | +S:484K +S:452R |
| Beta (18 December 2020) | South Africa, May-2020 | B.1.351, B.1.351.3, B.1.351.2, B.1.351.5, B.1.351.1 | South Africa (6885) | GH/501Y.V2 | 20H/501Y.V2 | 18 mutations (8 mutation at spike protein, with deletion:del241/243) | +S:L18F |
| Gamma (11 January 2021) | Brazil, November 2020. | 23 Pango lineages currently associated with the Gamma variant. | Brazil (47,475) | GR/501Y.V3 | 20J/501Y.V3 | 23 mutations (12 mutation at spike protein) | +S:681H |
| Delta (11 May 2021) | India, Oct-2020 | 216 Pango lineages currently associated with the Delta variant | India (69,457) | G/452R.V3 | 21A/S:478K | 29 mutations (8 mutation at spike protein, with deletion:del157/158) | +S:417N +S:484K |
| Omicron (26 November 2021) | South Africa, November 2021 | BA.1, BA.1.1, BA.2BA.3 | South Africa (4930) | GR/484A | 21K, 21L, 21M. | ∼50 mutations (30 mutations at spike protein, with deletion: del69/70, del143/145, and del212/212.) | +S:R346K |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Konyak, B.M.; Sharma, M.; Kharia, S.; Pandey, R.P.; Chang, C.-M. A Systematic Review on the Emergence of Omicron Variant and Recent Advancement in Therapies. Vaccines 2022, 10, 1468. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10091468
Konyak BM, Sharma M, Kharia S, Pandey RP, Chang C-M. A Systematic Review on the Emergence of Omicron Variant and Recent Advancement in Therapies. Vaccines. 2022; 10(9):1468. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10091468
Chicago/Turabian StyleKonyak, Beyau M., Mohan Sharma, Shabnam Kharia, Ramendra Pati Pandey, and Chung-Ming Chang. 2022. "A Systematic Review on the Emergence of Omicron Variant and Recent Advancement in Therapies" Vaccines 10, no. 9: 1468. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10091468