Parental Vaccine Preferences for Their Children in China: A Discrete Choice Experiment

 ,
,
Abstract: Background
1. Introduction
2. Method
2.1. Discrete Choice Experiment
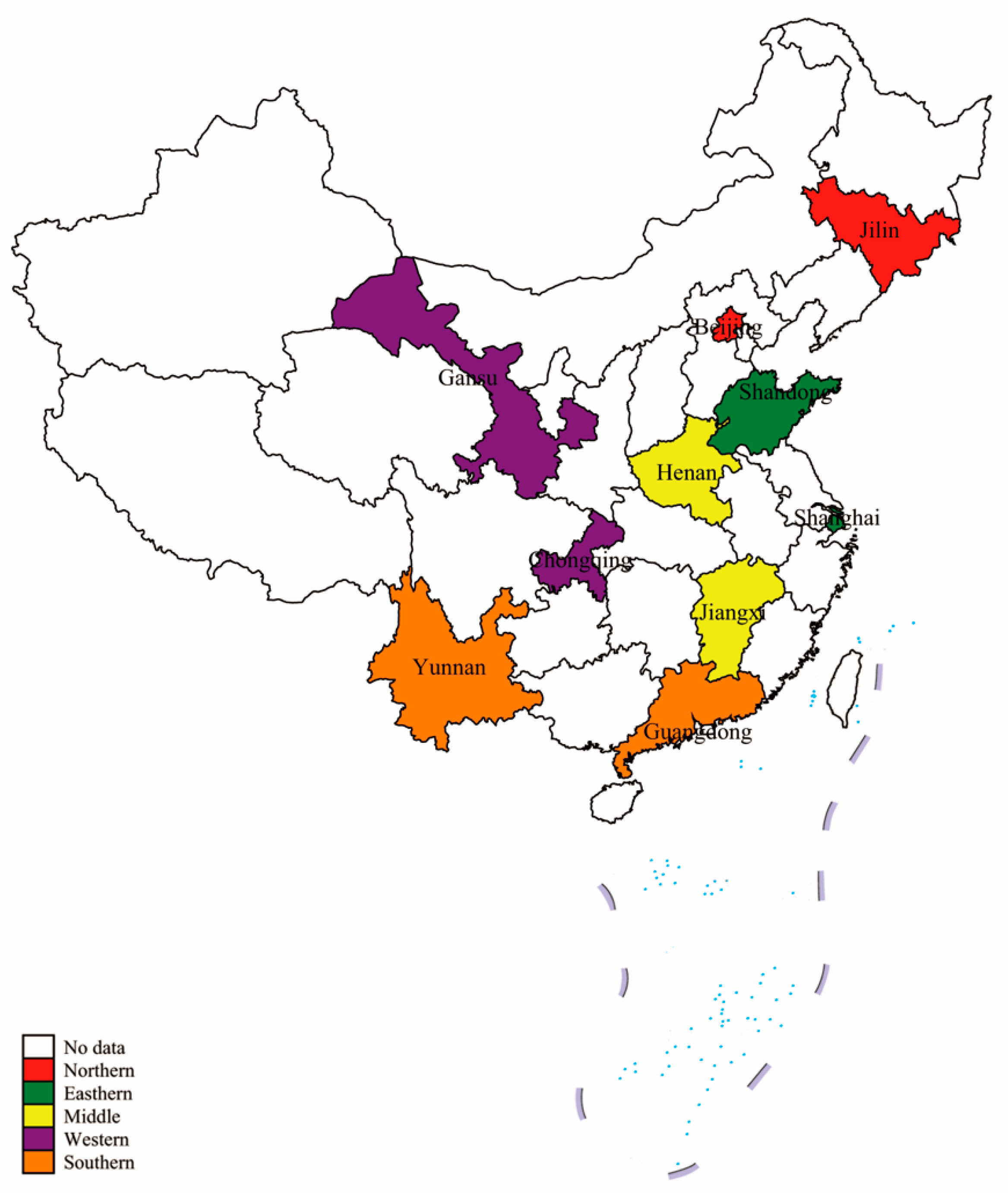
2.2. Study Population and Sample Size
2.3. Survey Development
2.4. Data Collection and Analysis
3. Result
3.1. Study Population
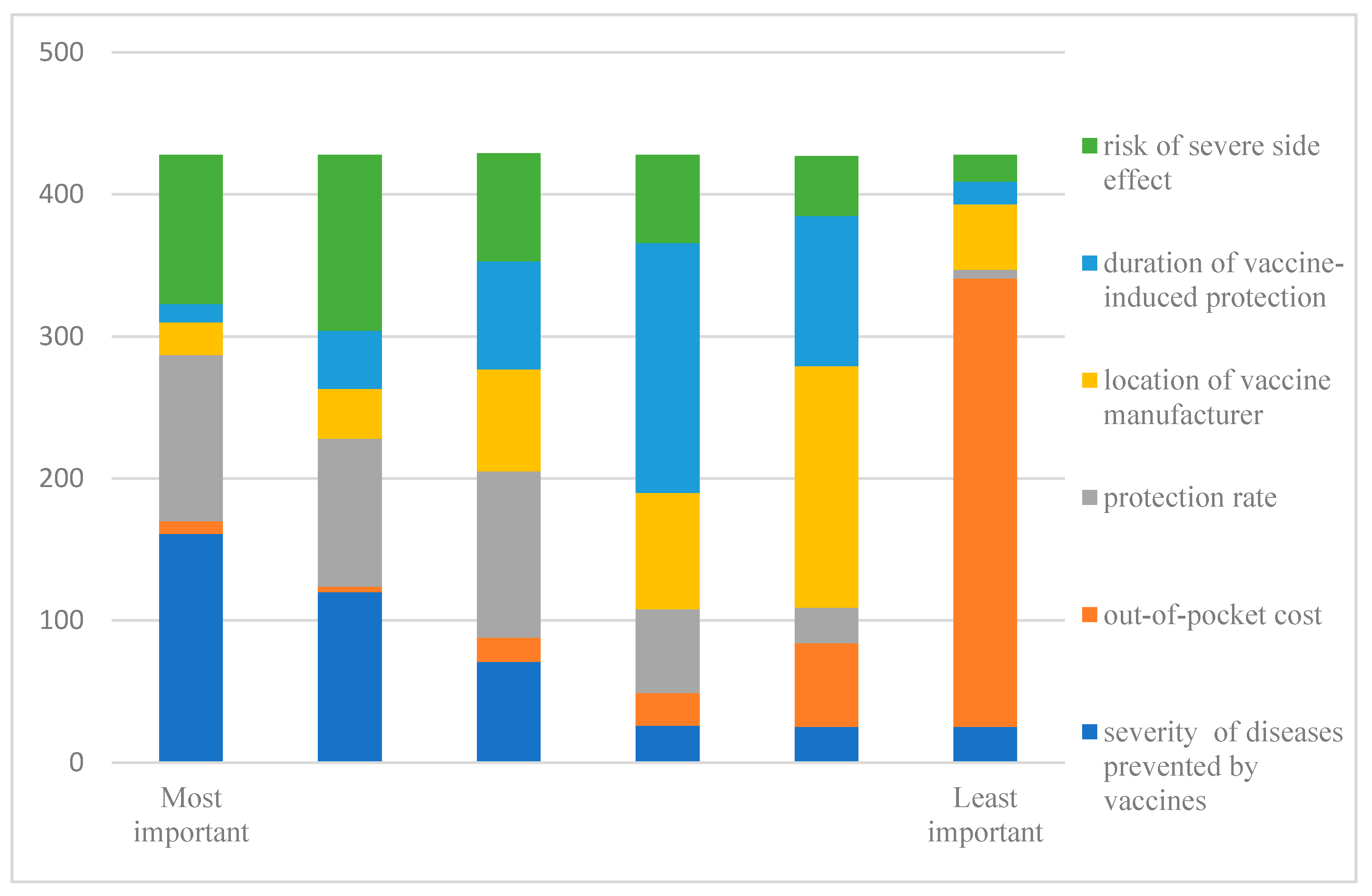
3.2. Importance Rating
3.3. Results of DCE Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/feature-stories/ten-threats-to-global-health-in-2019 (accessed on 26 March 2020).
- Chabot, I.; Goetghebeur, M.M.; Grégoire, J.-P. The societal value of universal childhood vaccination. Vaccine 2004, 22, 1992–2005. [Google Scholar] [CrossRef] [PubMed]
- Peck, M.; Gacic-Dobo, M.; Diallo, M.S.; Nedelec, Y.; Sodha, S.S.; Wallace, A.S. Global Routine Vaccination Coverage, 2018. MMWR. Morb. Mortal. Wkly. Rep. 2019, 68, 937–942. [Google Scholar] [CrossRef]
- Ye, L.; Fang, T.; Ma, R.; Dong, H.; Xu, G. Coverage of seasonal influenza vaccine among 6–35 month old children in Ningbo city of Zhejiang province, 2010–2018. Chin. J. Vaccines Immun. 2019, 25, 88–95. [Google Scholar]
- Wang, J. Status quo analysis on non-immunization programe vaccination among 600 preschool children. Henan Med. Res. 2020, 29, 1044–1046. [Google Scholar]
- Macdonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, R.M.; Sauver, J.L.S.; Rutten, L.J.F. Vaccine Hesitancy. In Proceedings of the Mayo Clinic Proceedings; Elsevier BV: Amsterdam, The Netherlands, 2015; Volume 90, pp. 1562–1568. [Google Scholar]
- McClure, C.C.; Cataldi, J.R.; O’Leary, S.T. Vaccine Hesitancy: Where We Are and Where We Are Going. Clin. Ther. 2017, 39, 1550–1562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SteelFisher, G.K.; Blendon, R.J.; Bekheit, M.M.; Lubell, K. The Public’s Response to the 2009 H1N1 Influenza Pandemic. N. Engl. J. Med. 2010, 362, e65. [Google Scholar] [CrossRef] [Green Version]
- Larson, H.J.; Cooper, L.Z.; Eskola, J.; Katz, S.L.; Ratzan, S. Addressing the vaccine confidence gap. Lancet 2011, 378, 526–535. [Google Scholar] [CrossRef]
- Han, B.; Wang, S.; Wan, Y.; Liu, J.; Zhao, T.; Cui, J.; Zhuang, H.; Cui, F. Has the public lost confidence in vaccines because of a vaccine scandal in China. Vaccine 2019, 37, 5270–5275. [Google Scholar] [CrossRef]
- Cao, L.; Zheng, J.; Cao, L.; Cui, J.; Xiao, Q. Evaluation of the impact of Shandong illegal vaccine sales incident on immunizations in China. Hum. Vaccines Immunother. 2018, 14, 1672–1678. [Google Scholar] [CrossRef]
- Liu, B.; Chen, R.; Zhao, M.; Zhang, X.; Wang, J.; Gao, L.; Xu, J.; Wu, Q.; Ning, N. Vaccine confidence in China after the Changsheng vaccine incident: A cross-sectional study. BMC Public Heal. 2019, 19, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Michaels-Igbokwe, C.; Macdonald, S.; Currie, G.R. Individual Preferences for Child and Adolescent Vaccine Attributes: A Systematic Review of the Stated Preference Literature. Patient Patient-Cent. Outcomes Res. 2017, 10, 687–700. [Google Scholar] [CrossRef] [PubMed]
- Poulos, C.; Standaert, B.; Sloesen, B.; Stryjewska, I.; Janitsary, A.; Hauber, B. Preferences for vaccines against children’s diarrheal illness among mothers in Poland and Hungary. Vaccine 2018, 36, 6022–6029. [Google Scholar] [CrossRef] [PubMed]
- Verelst, F.; Willem, L.; Kessels, R.; Beutels, P. Individual decisions to vaccinate one’s child or oneself: A discrete choice experiment rejecting free-riding motives. Soc. Sci. Med. 2018, 207, 106–116. [Google Scholar] [CrossRef] [PubMed]
- De Bekker-Grob, E.; Veldwijk, J.; Jonker, M.; Donkers, B.; Huisman, J.; Buis, S.; Swait, J.; Lancsar, E.; Witteman, C.L.; Bonsel, G.; et al. The impact of vaccination and patient characteristics on influenza vaccination uptake of elderly people: A discrete choice experiment. Vaccine 2018, 36, 1467–1476. [Google Scholar] [CrossRef]
- Wagner, A.L.; Boulton, M.L.; Sun, X.; Huang, Z.; Harmsen, I.A.; Ren, J.; Zikmund-Fisher, B.J. Parents’ concerns about vaccine scheduling in Shanghai, China. Vaccine 2017, 35, 4362–4367. [Google Scholar] [CrossRef]
- Guo, N.; Zhang, G.; Zhu, D.; Wang, J.; Shi, L. The effects of convenience and quality on the demand for vaccination: Results from a discrete choice experiment. Vaccine 2017, 35, 2848–2854. [Google Scholar] [CrossRef]
- Sun, X.; Wagner, A.L.; Ji, J.; Huang, Z.; Zikmund-Fisher, B.J.; Boulton, M.L.; Ren, J.; Prosser, L.A. A conjoint analysis of stated vaccine preferences in Shanghai, China. Vaccine 2020, 38, 1520–1525. [Google Scholar] [CrossRef]
- De Bekker-Grob, E.W.; Ryan, M.; Gerard, K. Discrete choice experiments in health economics: A review of the literature. Heal. Econ. 2012, 21, 145–172. [Google Scholar] [CrossRef]
- Lancsar, E.; Louviere, J. Conducting Discrete Choice Experiments to Inform Healthcare Decision Making. Pharmacoeconomics 2008, 26, 661–677. [Google Scholar] [CrossRef]
- Clark, M.D.; Determann, D.; Petrou, S.; Moro, D.; De Bekker-Grob, E.W. Discrete Choice Experiments in Health Economics: A Review of the Literature. Pharmacoeconomics 2014, 32, 883–902. [Google Scholar] [CrossRef] [PubMed]
- Bridges, J.F.; Hauber, A.B.; Marshall, D.; Lloyd, A.; Prosser, L.A.; Regier, D.A.; Johnson, F.R.; Mauskopf, J. Conjoint Analysis Applications in Health—A Checklist: A Report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Heal. 2011, 14, 403–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, F.R.; Lancsar, E.; Marshall, D.; Kilambi, V.; Mühlbacher, A.; Regier, D.A.; Bresnahan, B.W.; Kanninen, B.; Bridges, J.F. Constructing Experimental Designs for Discrete-Choice Experiments: Report of the ISPOR Conjoint Analysis Experimental Design Good Research Practices Task Force. Value Heal. 2013, 16, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauber, A.B.; González, J.M.; Oudshoorn-Groothuis, C.; Prior, T.; Marshall, D.A.; Cunningham, C.; Ijzerman, M.J.; Bridges, J.F. Statistical Methods for the Analysis of Discrete Choice Experiments: A Report of the ISPOR Conjoint Analysis Good Research Practices Task Force. Value Heal. 2016, 19, 300–315. [Google Scholar] [CrossRef] [Green Version]
- Orme, B. Sample Size Issues for Conjoint Analysis Studies; Sawtooth Software Technical Paper: Sequim, WA, USA, 1998. [Google Scholar]
- De Bekker-Grob, E.W.; Donkers, B.; Jonker, M.F.; Stolk, E.A. Sample Size Requirements for Discrete-Choice Experiments in Healthcare: A Practical Guide. Patient Patient-Cent. Outcomes Res. 2015, 8, 373–384. [Google Scholar] [CrossRef] [Green Version]
- Seanehia, J.; Treibich, C.; Holmberg, C.; Müller-Nordhorn, J.; Casin, V.; Raude, J.; Mueller, J.E. Quantifying population preferences around vaccination against severe but rare diseases: A conjoint analysis among French university students, 2016. Vaccine 2017, 35, 2676–2684. [Google Scholar] [CrossRef]
- Wang, B.; Chen, G.; Ratcliffe, J.; Afzali, H.H.A.; Giles, L.; Marshall, H. Adolescent values for immunisation programs in Australia: A discrete choice experiment. PLoS ONE 2017, 12, e0181073. [Google Scholar] [CrossRef] [Green Version]
- Cheng, J.; Pullenayegum, E.M.; Marshall, D.A.; Marshall, J.K.; Thabane, L. An empirical comparison of methods for analyzing correlated data from a discrete choice survey to elicit patient preference for colorectal cancer screening. BMC Med. Res. Methodol. 2012, 12, 15. [Google Scholar] [CrossRef] [Green Version]
- Cui, J.; Cao, L.; Zheng, J.; Cao, L.; Duo, M.; Xiao, Q. Reported coverage of vaccines in the national immunization program of China, 2015. Chin. J. Vaccines Immun. 2017, 23, 601–607. [Google Scholar]
- Hensher, D.A. Accounting for scale heterogeneity within and between pooled data sources. Transp. Res. Part A Policy Pr. 2012, 46, 480–486. [Google Scholar] [CrossRef]
- CSY. China Statistical Yearbook 2019; China Statistical Publishing House: Beijing, China, 2019. [Google Scholar]
- Ngorsuraches, S.; Nawanukool, K.; Petcharamanee, K.; Poopantrakool, U. Parents’ preferences and willingness-to-pay for human papilloma virus vaccines in Thailand. J. Pharm. Policy Pr. 2015, 8, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, C.K.H.; Man, K.K.; Ip, P.; Kwan, M.; McGhee, S.M. Mothers’ Preferences and Willingness to Pay for Human Papillomavirus Vaccination for Their Daughters: A Discrete Choice Experiment in Hong Kong. Value Heal. 2018, 21, 622–629. [Google Scholar] [CrossRef] [PubMed]
- Liao, Q.; Lam, W.W.T.; Wong, C.K.H.; Lam, C.; Chen, J.; Fielding, R. The relative effects of determinants on Chinese adults’ decision for influenza vaccination choice: What is the effect of priming? Vaccine 2019, 37, 4124–4132. [Google Scholar] [CrossRef] [PubMed]
- Marshall, H.; Chen, G.; Clarke, M.; Ratcliffe, J. Adolescent, parent and societal preferences and willingness to pay for meningococcal B vaccine: A Discrete Choice Experiment. Vaccine 2016, 34, 671–677. [Google Scholar] [CrossRef]
- Shono, A.; Kondo, M. Parents’ preferences for seasonal influenza vaccine for their children in Japan. Vaccine 2014, 32, 5071–5076. [Google Scholar] [CrossRef]
- Brown, D.S.; Johnson, F.R.; Poulos, C.; Messonnier, M.L. Mothers’ preferences and willingness to pay for vaccinating daughters against human papillomavirus. Vaccine 2010, 28, 1702–1708. [Google Scholar] [CrossRef]
- Hofman, R.; de Bekker-Grob, E.W.; Raat, H.; Helmerhorst, T.J.; van Ballegooijen, M.; Korfage, I.J. Parents’ preferences for vaccinating daughters against human papillomavirus in the Netherlands: A discrete choice experiment. BMC Public Heal. 2014, 14, 454. [Google Scholar] [CrossRef] [Green Version]
- Arbiol, J.; Yabe, M.; Nomura, H.; Borja, M.; Gloriani, N.; Yoshida, S.-I. Using discrete choice modeling to evaluate the preferences and willingness to pay for leptospirosis vaccine. Hum. Vaccines Immunother. 2015, 11, 1046–1056. [Google Scholar] [CrossRef] [Green Version]
- Flood, E.; Ryan, K.J.; Rousculp, M.D.; Beusterien, K.M.; Divino, V.M.; Block, S.L.; Hall, M.C.; Mahadevia, P.J. Parent Preferences for Pediatric Influenza Vaccine Attributes. Clin. Pediatr. 2010, 50, 338–347. [Google Scholar] [CrossRef]
- Dahlström, L.A.; Tran, T.N.; Lundholm, C.; Young, C.; Sundström, K.; Sparén, P. Attitudes to HPV vaccination among parents of children aged 12–15 years—A population-based survey in Sweden. Int. J. Cancer 2010, 126, 500–507. [Google Scholar] [CrossRef]
- The Standing Committee of the National People’s Congress. Vaccine Administration Act. Available online: https://www.nmpa.gov.cn/xxgk/fgwj/flxzhfg/20190702121701506.html (accessed on 22 August 2020).
- Veldwijk, J.; Lambooij, M.S.; Bruijning-Verhagen, P.C.; Smit, H.A.; De Wit, G.A. Parental preferences for rotavirus vaccination in young children: A discrete choice experiment. Vaccine 2014, 32, 6277–6283. [Google Scholar] [CrossRef] [PubMed]
- Poulos, C.; Johnson, F.R.; Krishnarajah, G.; Anonychuk, A.; Misurski, D. Pediatricians’ Preferences for Infant Meningococcal Vaccination. Value Heal. 2015, 18, 67–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eilers, R.; De Melker, H.; Veldwijk, J.; Krabbe, P. Vaccine preferences and acceptance of older adults. Vaccine 2017, 35, 2823–2830. [Google Scholar] [CrossRef] [PubMed]
- Poulos, C.; Curran, D.; Anastassopoulou, A.; De Moerlooze, L. German travelers’ preferences for travel vaccines assessed by a discrete choice experiment. Vaccine 2018, 36, 969–978. [Google Scholar] [CrossRef]
- Huang, Z.; Sun, X.; Wagner, A.L.; Ren, J.; Boulton, M.L.; Prosser, L.A.; Zikmund-Fisher, B.J. Parent and caregiver perceptions about the safety and effectiveness of foreign and domestic vaccines in Shanghai, China. PLoS ONE 2018, 13, e0197437. [Google Scholar] [CrossRef]
- Zhao, W. Public Consultation on Vaccine Administration Act Xinhua Net: Xinhua Net. 2018. Available online: http://www.xinhuanet.com/politics/2018-11/11/c_1123696553.htm (accessed on 22 August 2020).
- Veldwijk, J.; Van Der Heide, I.; Rademakers, J.; Schuit, A.; De Wit, G.A.; Uiters, E.; Lambooij, M.S. Preferences for Vaccination. Med. Decis. Mak. 2015, 35, 948–958. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Attributes | Attribute Levels |
|---|---|
| The severity of diseases prevented by vaccines (mortality) | 1% |
| 5% | |
| 10% | |
| 15% | |
| Protection rate prevented by vaccines | 65% |
| 80% | |
| 95% | |
| Duration of vaccine-induced protection | 1 year |
| 5 years | |
| 10 years | |
| The risk of severe side effects | Low risk |
| Moderate risk | |
| High risk | |
| Location of vaccine manufacturer | Domestic |
| Imported | |
| The out-of-pocket cost of a vaccine | 0 Yuan |
| 150 Yuan | |
| 300 Yuan |
| Vaccine Attributes | Vaccine A | Vaccine B |
|---|---|---|
| Severity of diseases prevented by a vaccine | 15% | 5% |
| Protection rate prevented by vaccines | 80% | 65% |
| Duration of vaccine-induced protection | 1 year | 5 year |
| Risk of severe side effects | Moderate risk | High risk |
| Location of vaccine manufacturer | Domestic | Imported |
| Out-of-pocket cost of the vaccine | 0 yuan | 150 yuan |
| Which vaccine would you prefer? | ☐ | ☐ |
| In reality, would you vaccinate your child with the option you chose above? | ☐ YES ☐ NO | |
| Characteristics | All (N = 580) | Parents Who Passed the Consistency Test (N = 428) | Parents Who Failed the Consistency Test (N = 152) | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Age (years) a | 31.22 | 0.21 | 31.27 | 0.24 | 31.04 | 0.44 |
| Household size a | 4.56 | 0.05 | 4.58 | 0.06 | 4.53 | 0.10 |
| Monthly income (RMB) a | 12539.2 | 530.68 | 12762.24 | 666.22 | 11911.18 | 763.45 |
| Monthly expenditure (RMB) a | 7215.10 | 223.37 | 7141.47 | 247.43 | 7422.41 | 492.06 |
| Child’ age a | 2.03 | 0.05 | 2.09 | 0.06 | 1.85 | 0.09 |
| N | % | N | % | N | % | |
| Relation to the childb | ||||||
| Mother | 474 | 81.72 | 351 | 82.01 | 123 | 80.92 |
| Father | 106 | 18.28 | 77 | 17.99 | 29 | 19.08 |
| Ethics | ||||||
| Han | 549 | 94.66 | 403 | 94.16 | 146 | 96.05 |
| Minority | 31 | 5.34 | 25 | 5.84 | 6 | 3.95 |
| Child’s genderb | ||||||
| Male | 302 | 52.07 * | 236 | 55.14 * | 66 | 43.42 * |
| Female | 278 | 47.93 * | 192 | 44.86 * | 86 | 56.58 * |
| One childb | ||||||
| Yes | 261 | 45.00 | 193 | 45.09 | 68 | 44.74 |
| No | 319 | 55.00 | 235 | 54.91 | 84 | 55.26 |
| Child healthc | ||||||
| Very good | 276 | 47.59 * | 195 | 45.56 * | 81 | 53.29 * |
| Good | 242 | 41.72 * | 180 | 42.06 * | 62 | 40.79 * |
| Fair or poor | 62 | 10.69 * | 53 | 12.38 * | 9 | 5.92 * |
| Jobb | ||||||
| Working | 387 | 66.72 | 292 | 68.22 | 95 | 62.50 |
| Non-working | 193 | 33.28 | 136 | 31.78 | 57 | 37.50 |
| Regionb | ||||||
| Urban | 355 | 61.21 | 256 | 59.81 | 99 | 65.13 |
| Rural | 225 | 38.79 | 172 | 40.19 | 53 | 34.87 |
| Education levelsc | ||||||
| Primary or below | 8 | 1.38 | 7 | 1.64 | 1 | 0.66 |
| Junior or senior | 247 | 42.59 | 188 | 43.93 | 59 | 38.82 |
| College and above | 325 | 56.03 | 233 | 54.43 | 92 | 60.52 |
| Attributes | β | SE † | SD | SE ‡ |
|---|---|---|---|---|
| Non-vaccination | −3.336 *** | 0.4464 | 4.361 *** | 0.3548 |
| Protection rate prevented by a vaccine (ref: 65%) | ||||
| 80% | 0.504 *** | 0.0757 | 0.044 | 0.1407 |
| 95% | 1.230 *** | 0.0882 | 0.696 *** | 0.1125 |
| Risk of severe side effect event (ref: high) | ||||
| moderate | 0.793 *** | 0.0782 | 0.243 | 0.1596 |
| low | 1.667 *** | 0.1131 | 1.407 *** | 0.1156 |
| Location of vaccine manufacturer (ref: domestic) | ||||
| Imported | −0.152 * | 0.0638 | 0.740 *** | 0.0904 |
| Duration of vaccine-induced protection (ref: 1 year) | ||||
| 5 years | 0.310 *** | 0.0732 | 0.017 | 0.1317 |
| 10 years | 0.642 *** | 0.0925 | 0.939 *** | 0.1133 |
| Out-of-pocket Cost | −0.001 ** | 0.0003 | 0.003 *** | 0.0004 |
| Severity of diseases prevented by vaccines (per 1%) | 0.003 | 0.0088 | 0.136 *** | 0.0108 |
| Log likelihood | −3030.5396 | |||
| AIC | 6101.079 | |||
| BIC | 6250.286 | |||
| Respondents, n | 428 | |||
| Observations, n | 12840 | |||
| Attributes | β | SE | p-Value | 95% CI | |
|---|---|---|---|---|---|
| Non-vaccination | −3.112 | 0.638 | <0.001 | −4.361 | −1.862 |
| Protection rate prevented by a vaccine (ref: 65%) | |||||
| 80% | 0.501 | 0.075 | <0.001 | 0.355 | 0.647 |
| 95% | 1.386 | 0.115 | <0.001 | 1.160 | 1.611 |
| Risk of severe side effect event (ref: high) | |||||
| moderate | 0.794 | 0.077 | <0.001 | 0.643 | 0.944 |
| low | 1.609 | 0.201 | <0.001 | 1.215 | 2.003 |
| Location of vaccine manufacturer (ref: domestic) | |||||
| Imported | −0.403 | 0.091 | <0.001 | −0.582 | −0.224 |
| Duration of vaccine-induced protection (ref: 1 year) | |||||
| 5 years | 0.315 | 0.072 | <0.001 | 0.174 | 0.457 |
| 10 years | 0.517 | 0.096 | <0.001 | 0.329 | 0.706 |
| Out-of-pocket Cost | −0.001 | 0.000 | <0.001 | −0.002 | −0.001 |
| Severity of diseases prevented by vaccines (per 1%) | 0.003 | 0.011 | 0.799 | −0.018 | 0.024 |
| Interaction terms | |||||
| Non-vaccination * working | 0.683 | 0.622 | 0.272 | −0.536 | 1.902 |
| Non-vaccination * age (>30 years old) | 0.584 | 0.458 | 0.203 | −0.315 | 1.482 |
| Non-vaccination * father | −1.576 | 0.585 | 0.007 | −2.723 | −0.428 |
| Non-vaccination * rural | −1.283 | 0.500 | 0.010 | −2.263 | −0.304 |
| Non-vaccination * education level (college and above) | 0.280 | 0.501 | 0.576 | −0.701 | 1.261 |
| Non-vaccination * health state (fair/poor) | −1.899 | 0.854 | 0.026 | −3.573 | −0.224 |
| Lowest risk of severe side effect * education level (college and above) | 0.445 | 0.193 | 0.021 | 0.068 | 0.823 |
| Lowest risk of severe side effect * rural | −0.299 | 0.190 | 0.116 | −0.671 | 0.074 |
| Lowest risk of severe side effect * age (>30 years old) | −0.155 | 0.187 | 0.406 | −0.521 | 0.211 |
| 90% protection rate * age (>30 years old) | −0.362 | 0.143 | 0.012 | −0.642 | −0.081 |
| Protection duration of 10 years * father | 0.433 | 0.204 | 0.034 | 0.033 | 0.833 |
| Imported vaccine * education level (college and above) | 0.468 | 0.124 | <0.001 | 0.225 | 0.712 |
| Log likelihood | −3234.7672 | ||||
| AIC | 6100.574 | ||||
| BIC | 6339.304 | ||||
| Respondents, n | 428 | ||||
| Observations, n | 12840 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gong, T.; Chen, G.; Liu, P.; Lai, X.; Rong, H.; Ma, X.; Hou, Z.; Fang, H.; Li, S. Parental Vaccine Preferences for Their Children in China: A Discrete Choice Experiment. Vaccines 2020, 8, 687. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8040687
Gong T, Chen G, Liu P, Lai X, Rong H, Ma X, Hou Z, Fang H, Li S. Parental Vaccine Preferences for Their Children in China: A Discrete Choice Experiment. Vaccines. 2020; 8(4):687. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8040687
Chicago/Turabian StyleGong, Tiantian, Gang Chen, Ping Liu, Xiaozhen Lai, Hongguo Rong, Xiaochen Ma, Zhiyuan Hou, Hai Fang, and Shunping Li. 2020. "Parental Vaccine Preferences for Their Children in China: A Discrete Choice Experiment" Vaccines 8, no. 4: 687. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8040687