Vaccination Attitude and Communication in Early Settings: An Exploratory Study


 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Context of the Study
2.2. Design of the Study
2.3. Recruitment of Participants
2.4. Questionnaire
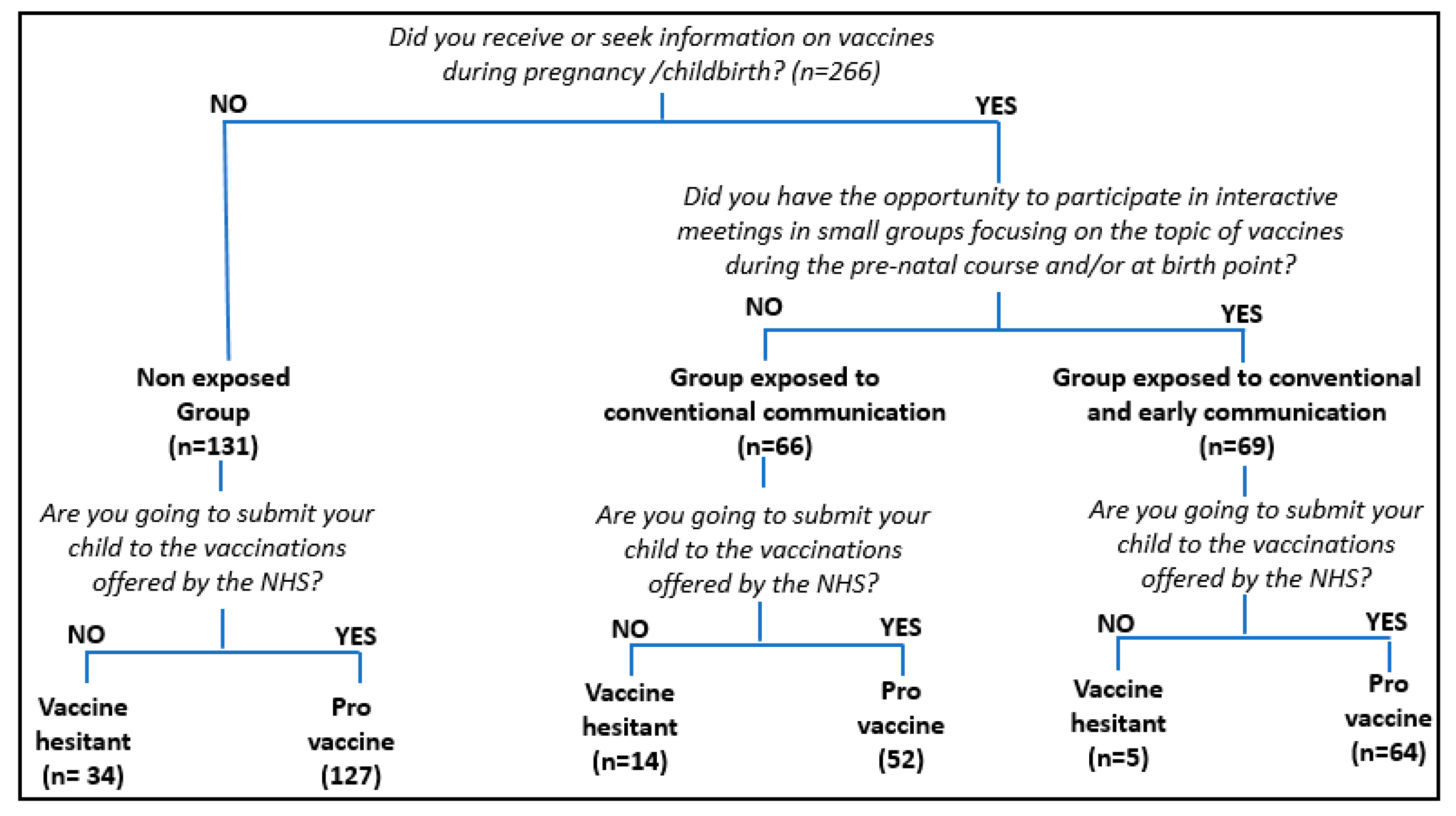
Did you receive or seek information on vaccines during pregnancy /childbirth? Consider both health and non-health sources.(yes or no)
During the pre-natal course and/or at birth point did you have the opportunity to participate in small group meetings (about 8–10 people), conducted in a participatory way (not frontal lessons, but interactive meetings where you could express yourselves freely), and focused on the topic of vaccines (vaccination schedule, benefits and risks)?(yes or no)
- If you had the opportunity to participate in these meetings, was it useful?(yes or no)
- If you did not attend these meetings, would you have been glad to have this opportunity?(yes or no)
- Are you going to submit your child to the free vaccinations offered by the National Health System, within the proposed timetable?(open ended question)
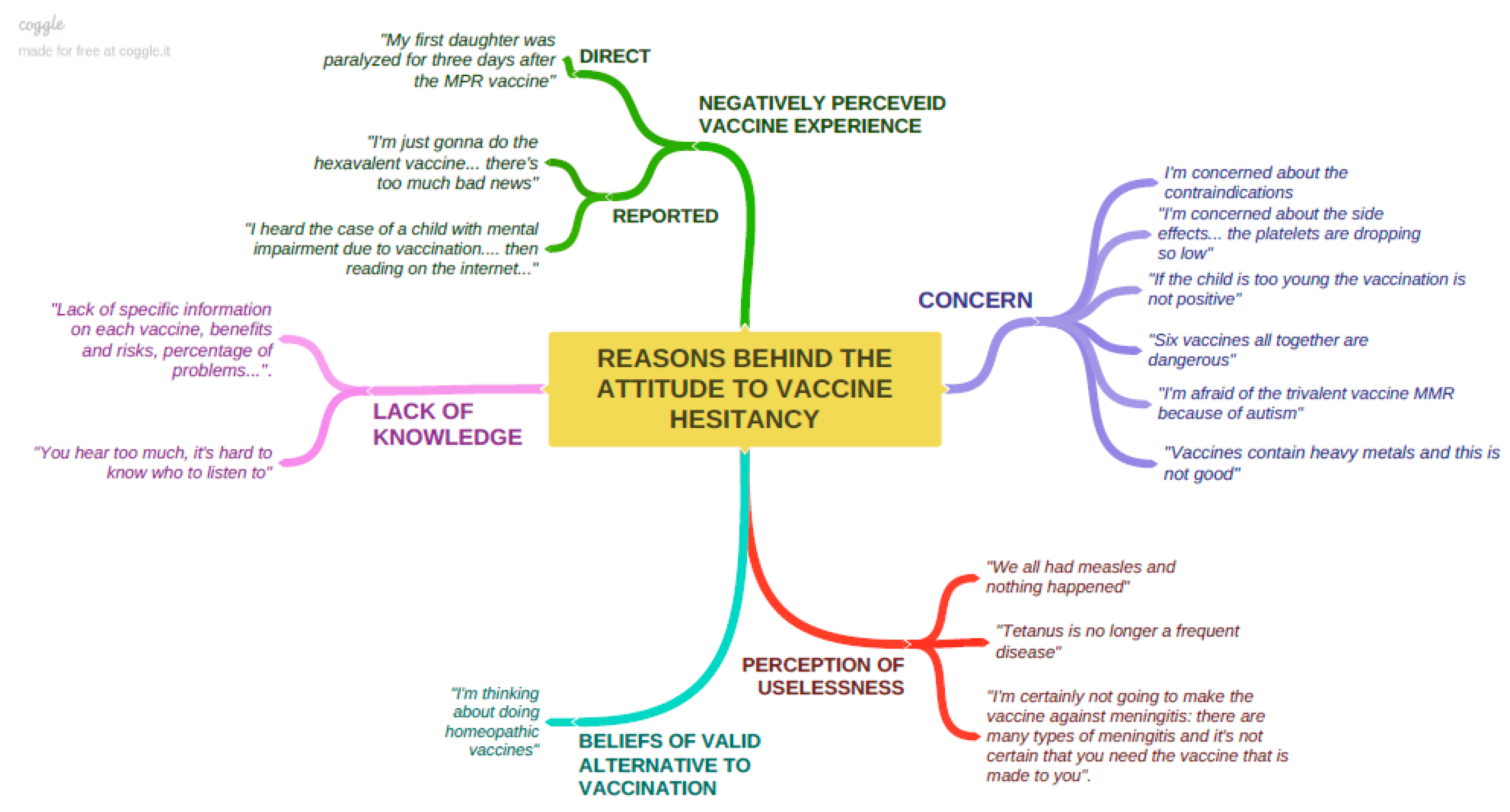
- If you are not going to submit your child to all the free vaccinations offered by the National Health System, which vaccines are you more hesitant about and why?(open ended question)
- (1)
- “Non-exposed group”, i.e., mothers who declare that they have not received or looked for any specific information on vaccines during pregnancy/childbirth and who have not attended meetings on this topic.
- (2)
- “Group exposed to conventional communication”, i.e., mothers who declare that, during pregnancy/childbirth, they have received and/or looked for information about vaccines by means of healthcare and non-healthcare sources, but who have not attended meetings on this topic.
- (3)
- “Group exposed to conventional and early communication”, i.e., mothers who declare that they have received or looked for information about vaccines by means of healthcare and non-healthcare sources, and who have attended meetings about vaccines during the prenatal course and/or at birth point.
- (1)
- Pro-vaccine attitude, i.e., mothers who steadily declare that they would follow the vaccination schedule offered by the NHS (both compulsory and recommended) without any doubt or concern.
- (2)
- Vaccine hesitancy attitude, i.e., mothers who express strong perplexity and reluctancy and/or declare that they would not entirely follow the vaccination schedule proposed by the NHS.
2.5. Data Analysis
3. Results
3.1. Sample Description
3.2. Attitude to Vaccination
3.3. Exposure to Information on Vaccines
3.4. Association between Attitude to Vaccination and Different Exposures to Communication Regarding Vaccines
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Ethics and Consent to Participate
Data Availability
Abbreviations
| WHO | World Health Organization |
| NHS | National Health System |
| OR | odds ratio |
| CI | confidence interval |
References
- Smith, T.C. Vaccine Rejection and Hesitancy: A Review and Call to Action. Open Forum Infect. Dis. 2017, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Europe. European Vaccine Action Plan 2015–2020. Available online: https://www.euro.who.int/__data/assets/pdf_file/0020/253730/64wd15e_EVAP_140459.pdf (accessed on 22 October 2020).
- Cherry, J.D. Epidemic pertussis in 2012 the resurgence of a vaccine preventable disease. N. Engl. J. Med. 2012, 367, 785–787. [Google Scholar] [CrossRef] [PubMed]
- Orenstein, W.A.; Ahmed, R. Simply put: Vaccination saves lives. Proc. Natl. Acad. Sci. USA 2017, 114, 4031–4033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giubilini, A.; Savulescu, J. Vaccination, Risks, and Freedom: The Seat Belt Analogy. Public Health Eth. 2019, 12, 237–249. [Google Scholar] [CrossRef] [PubMed]
- Omer, S.B.; Salmon, D.A.; Orenstein, W.A.; de Hart, M.P.; Halsey, N. Vaccine refusal, mandatory immunization, and the risks of vaccine-preventable diseases. N. Engl. J. Med. 2009, 360, 1981–1988. [Google Scholar] [CrossRef]
- Vaz, O.M.; Ellinǵson, M.K.; Weiss, P.; Jenness, S.M.; Bardají, A.; Bednarczyk, R.A.; Omer, S.B. Mandatory Vaccination in Europe. Pediatrics 2020, 145. [Google Scholar] [CrossRef] [Green Version]
- Bozzola, E.; Spina, G.; Russo, R.; Bozzola, M.; Corsello, G.; Villani, A. Mandatory vaccinations in European countries, undocumented information, false news and the impact on vaccination uptake: The position of the Italian pediatric society. Ital. J. Pediatr. 2018, 44, 67. [Google Scholar] [CrossRef]
- Bonanni, P. Enlarged free childhood vaccination offer in Italy proposed to curb the rise in the growing anti-vaccine message. Expert Rev. Vaccines 2018, 17, 1–3. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, N.E. The SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Ève, D.; MacDonald, N.E. Managing the risks of vaccine hesitancy and refusals. Lancet Infect. Dis. 2016, 16, 518–519. [Google Scholar]
- Kata, A. Anti-vaccine activists, Web 2.0, and the postmodern paradigm- An overview of tactics and tropes used online by the anti-vaccination movement. Vaccine 2012, 30, 3778–3789. [Google Scholar] [CrossRef] [PubMed]
- Vrdelja, M.; Kraigher, A.; Vercic, D.; Kropivnik, S. The growing vaccine hesitancy: Exploring the influence of the internet. Eur. J. Public Health 2018, 28, 934–939. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Gagnon, D.; MacDonald, N.E. SAGE Working Group on Vaccine Hesitancy. Strategies intended to address vaccine hesitancy: Review of published reviews. Vaccine 2015, 33, 4191–4203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorini, C.; Santomauro, F.; Donzellini, M.; Capecchi, L.; Bechini, A.; Boccalini, S.; Bonanni, P.; Bonaccorsi, G. Health literacy and vaccination: A systematic review. Hum. Vaccines Immunother. 2018, 14, 478–488. [Google Scholar] [CrossRef] [Green Version]
- Thomson, A.; Vallée-Tourangeau, G.; Suggs, L.S. Strategies to increase vaccine acceptance and uptake: From behavioral insights to context-specific, culturally-appropriate, evidence-based communications and interventions. Vaccine 2018, 36, 6457–6458. [Google Scholar] [CrossRef]
- Parrish-Sprowl, J. Vaccine hesitancy communication: What counts as evidence. Vaccine 2018, 36, 6529–6530. [Google Scholar] [CrossRef] [Green Version]
- Betsch, C. Innovations in communication: The Internet and the psychology of vaccination decisions. Eurosurveillance 2011, 16. [Google Scholar] [CrossRef]
- Fitzsimons, G.J.; Hutchinson, J.W.; Williams, P. Non-Conscious Influences on Consumer Choice. Mark. Lett. 2002, 13, 269–279. [Google Scholar] [CrossRef]
- Germinario, C.; Gallone, M.S.; Tafuri, S. How to fight anti-vaccinists prejudices: The viewpoint of public health. Epidemiol. Prev. 2014, 38, 120–123. [Google Scholar]
- Greenberg, J.; Dubé, E.; Driedger, M. Vaccine Hesitancy: In Search of the Risk Communication Comfort Zone. PLoS Curr. 2017. [Google Scholar] [CrossRef]
- World Health Organization. Health Promotion Glossary. Available online: http://www.who.int/healthpromotion/about/HPR%20Glossary%201998.pdf (accessed on 22 October 2020).
- Italian Ministry of Health. Piano Nazionale Prevenzione Vaccinale 2017–2019. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2571_allegato.pdf (accessed on 22 October 2020).
- Ames, H.M.; Glenton, C.; Lewin, S. Parents’ and informal caregivers’ views and experiences of communication about routine childhood vaccination: A synthesis of qualitative evidence. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, N.J.; Danchin, M.; Trevena, L.; Witteman, H.O.; Kinnersley, P.; Snelling, T.; Robinson, P.; Leask, J. Sharing knowledge about immunisation (SKAI): An exploration of parents’ communication needs to inform development of a clinical communication support intervention. Vaccine 2018, 36, 6480–6490. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Vaccine Hesitancy: A Growing Challenge for Immunization Programmes. Available online: http://www.who.int/mediacentre/news/releases/2015/vaccine-hesitancy/en/ (accessed on 22 October 2020).
- Corben, P.; Leask, J. To close the childhood immunization gap, we need a richer understanding of parents’ decision-making. Hum. Vaccines Immunother. 2016, 12, 3168–3176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giambi, C.; Fabiani, M.; D’Ancona, F.; Ferrara, L.; Fiacchini, D.; Gallo, T.; Martinelli, D.; Pascucci, M.G.; Prato, R.; Filia, A.; et al. Parental vaccine hesitancy in Italy—Results from a national survey. Vaccine 2018, 36, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Gagnon, D.; Zhou, Z.; Deceuninck, G. Parental Vaccine Hesitancy in Quebec (Canada). PLoS Curr. 2016, 8. [Google Scholar] [CrossRef] [Green Version]
- WHO Risk Scales: Benefits of Vaccines Far Outweigh the Risks. 2017. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/vaccines-and-immunization/publications/2017/risk-scales-benefits-of-vaccines-far-outweigh-the-risks-2017 (accessed on 13 November 2020).
- Kaufman, J.; Ryan, R.; Walsh, L.; Horey, D.; Leask, J.; Robinson, P.; Hill, S. Face-to-face interventions for informing or educating parents about early childhood vaccination. Cochrane Database Syst. Rev. 2018, 5. [Google Scholar] [CrossRef]
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J. SAGE Working Group on Vaccine Hesitancy. Strategies for addressing vaccine hesitancy—A systematic review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [Green Version]
- Danchin, M.H.; Costa-Pinto, J.; Attwell, K.; Willaby, H.; Wiley, K.; Hoq, M.; Leask, J.; Perrett, K.P.; O’Keefe, J.; Giles, M.L.; et al. Vaccine decision-making begins in pregnancy: Correlation between vaccine concerns, intentions and maternal vaccination with subsequent childhood vaccine uptake. Vaccine 2018, 36, 6473–6479. [Google Scholar] [CrossRef]
- Corben, P.; Leask, J. Vaccination hesitancy in the antenatal period: A cross-sectional survey. BMC Public Health 2018, 18, 566. [Google Scholar] [CrossRef] [Green Version]
- Sadaf, A.; Richards, J.L.; Glanz, J.; Salmon, D.A.; Omer, S.B. A systematic review of interventions for reducing parental vaccine refusal and vaccine hesitancy. Vaccine 2013, 31, 4293–4304. [Google Scholar] [CrossRef]
- Gagneur, A.; Battista, M.C.; Boucher, F.D.; Quach, C.; DeWals, P.; Lemaitre, T.; Anne Farrands, A.; Boulianne, N.; Sauvageau, C.; Ouakki, M.; et al. Promoting vaccination in maternity wards—Motivational interview technique reduces hesitancy and enhances intention to vaccinate, results from a multicentre non-controlled pre- and post-intervention RCT-nested study, Quebec, March 2014 to February 2015. Eurosurveillance 2019, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosso, A.; Massimi, A.; De Vito, C.; Adamo, G.; Baccolini, V.; Marzuillo, C.; Vacchio, M.R.; Villari, P. Factors affecting the vaccination choices of pregnant women for their children: A systematic review of the literature. Hum. Vaccines Immunother. 2020, 16, 1969–1980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosso, A.; Massimi, A.; De Vito, C.; Adamo, G.; Baccolini, V.; Marzuillo, C.; Vacchio, M.R.; Villari, P. Knowledge and attitudes on pediatric vaccinations and intention to vaccinate in a sample of pregnant women from the City of Rome. Vaccine 2019, 37, 1954–1963. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameters | n | Estimates (95% CI) |
|---|---|---|
| Mothers’ mean age | 266 | 33 (32–33) |
| Mothers living in Cagliari metropolitan area | 203 | 76% (71–81%) |
| Mothers having a diploma or being graduated | 216 | 81% (77–86%) |
| Mothers working in the healthcare sector | 6 | 4% (2–7%) |
| Primigravidae | 164 | 62% (57–67%) |
| Mothers having attended prenatal classes | 106 | 39% (34–45%) |
| Exposure to Communication Regarding Vaccines | Prevalence (95% CI) |
|---|---|
| Non-exposed group Mothers who declare that they have not received or looked for any specific information on vaccines during pregnancy/childbirth and who have not attended meetings on this topic (n = 131). | 49% (41–58%) |
| Group exposed to conventional communication Mothers who declare that they have received and/or looked for information about vaccines by means of healthcare and non-healthcare sources, and who have not attended meetings on this topic (n = 66). | 25% (14–35%) |
| Group exposed to conventional and early communication Mothers who declare that they have received or looked for information about vaccines by means of healthcare and non-healthcare sources, and who to have attended meetings about vaccines during prenatal course and/or at birth point (n = 69). | 26% (16–36%) |
| Exposure to Communication Regarding Vaccines | Prevalence of Vaccine Hesitancy % (95% CI) | p Value |
|---|---|---|
| Non-exposed group Mothers who declare that they have not received or looked for any specific information on vaccines during pregnancy/childbirth and who have not attended meetings on this topic (n = 131). | 26% (18–33%) n = 34 | 0.002 |
| Group exposed to conventional communication Mothers who declare that they have received and/or looked for information about vaccines by means of healthcare and non-healthcare sources, but who have not attended meetings on this topic (n = 66). | 21% (11–31%) n = 14 | |
| Group exposed to conventional and early communicationMothers who declare that they have received and/or looked for information about vaccines by means of healthcare and non-healthcare sources, and who have attended meetings on this topic (n = 69). | 7% (1–13%) n = 5 |
| Independent Variables | OR (CI 95%) | p Value |
|---|---|---|
| Non-exposed mothers (n = 131) | 4.5 (1.7–12.1) | <0.001 |
| Mothers exposed to conventional communication (66) | 3.4 (1.2–10.2) | 0.03 |
| Mothers exposed to conventional & early communication (n = 69) | 1 (reference) | 0.012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mereu, N.; Mereu, A.; Murgia, A.; Liori, A.; Piga, M.; Argiolas, F.; Salis, G.; Santus, S.; Porcu, C.; Contu, P.; et al. Vaccination Attitude and Communication in Early Settings: An Exploratory Study. Vaccines 2020, 8, 701. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8040701
Mereu N, Mereu A, Murgia A, Liori A, Piga M, Argiolas F, Salis G, Santus S, Porcu C, Contu P, et al. Vaccination Attitude and Communication in Early Settings: An Exploratory Study. Vaccines. 2020; 8(4):701. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8040701
Chicago/Turabian StyleMereu, Noemi, Alessandra Mereu, Alessandra Murgia, Arianna Liori, Michela Piga, Federico Argiolas, Graziella Salis, Simonetta Santus, Carmela Porcu, Paolo Contu, and et al. 2020. "Vaccination Attitude and Communication in Early Settings: An Exploratory Study" Vaccines 8, no. 4: 701. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8040701