
Impact of Introducing Hepatitis B Birth Dose Vaccines into the Infant Immunization Program in Burkina Faso: Study Protocol for a Stepped Wedge Cluster Randomized Trial (NéoVac Study)


 , , , , add
Show full author list
, , , , add
Show full author list
Abstract
:1. Introduction
2. Methods
2.1. NéoVac Research Program
2.2. Specific Objectives
- -
- To assess the effectiveness of introducing HepB-BD on the risk of MTCT, defined as positive HBsAg in infants aged 9 months;
- -
- To assess the impact of introducing HepB-BD on the risk of MTCT in subgroups of mother–child pairs defined by the maternal HBsAg;
- -
- To assess the impact of introducing HepB-BD on the risk of MTCT in subgroups of mother–child pairs defined by the maternal hepatitis B e antigen (HBeAg) and HBV DNA levels;
- -
- To explore the dose–response relationship between the number of hepatitis B vaccine doses administered (0–4) and the risk of HBsAg positivity in infants;
- -
- To examine the association between the timeliness of the first dose of the hepatitis B vaccine and the risk of HBsAg positivity in infants;
- -
- To compare the immunological response between those who received HepB-BD and those who did not by titration of the antibody to HBsAg (anti-HBs) in infants;
- -
- To describe the coverage and timeliness of HepB-BD, pentavalent vaccines, and other vaccines recommended by the national infant immunization program in Burkina Faso;
- -
- To estimate the prevalence of HBsAg in mothers of children aged 9 months;
- -
- To estimate the prevalence of HBeAg in HBsAg-positive mothers;
- -
- To estimate the prevalence of HBV DNA levels ≥200,000 IU/mL in HBsAg-positive mothers.
- -
- To evaluate the acceptability of adding HepB-BD into the infant immunization program among healthcare workers and community members.
- -
- To evaluate the public health benefits, the cost, and the cost-effectiveness of introducing HepB-BD into the infant immunization program in Burkina Faso versus the current situation.
2.3. Study Design
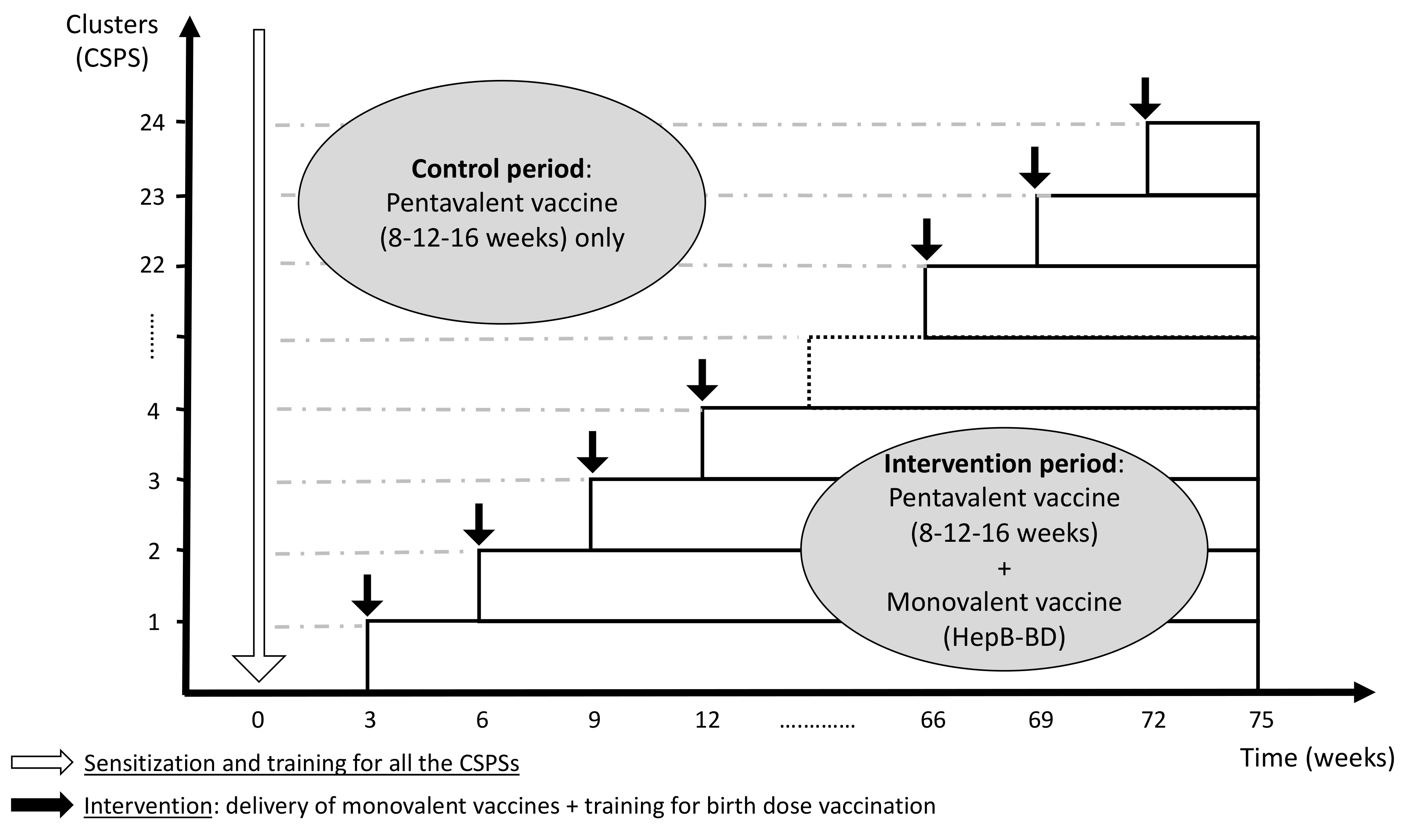
2.3.1. Stepped Wedge Cluster Randomized Trial
2.3.2. Why Cluster Randomized Trial Rather Than Individually Randomized Trial?
2.3.3. Why Stepped Wedge Rather Than Parallel Design?
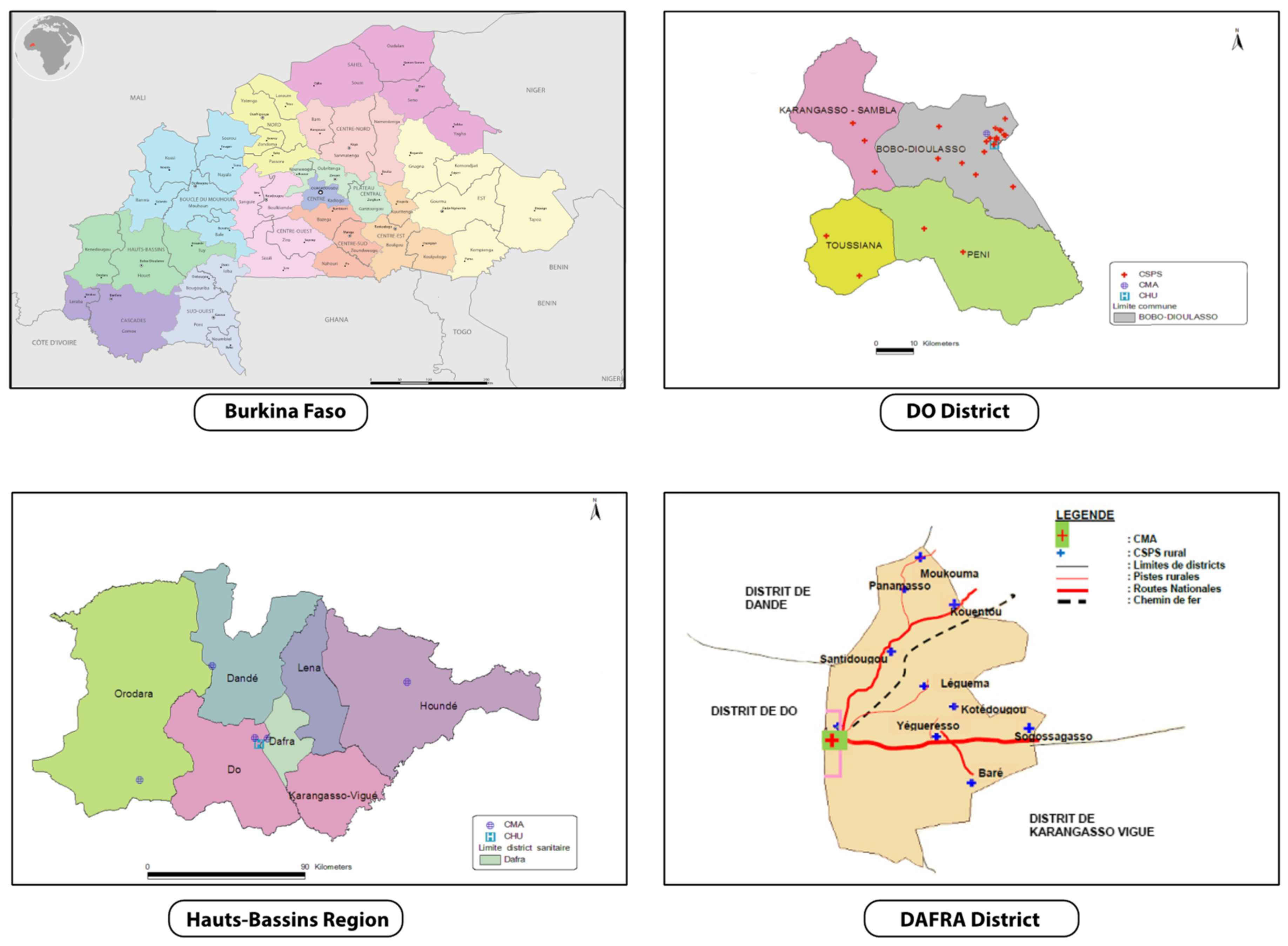
2.4. Study Setting
2.5. Eligibility Criteria
2.5.1. Clusters
2.5.2. Individuals
2.6. Interventions
2.6.1. Initial Training
2.6.2. Control Period
2.6.3. Interventional Period
2.6.4. Routine Care
2.7. Outcomes
2.7.1. Primary Outcome
- -
- The risk of MTCT, defined as a prevalence of positive HBsAg in infants aged 9 months.
2.7.2. Secondary Outcomes
- -
- The coverage and timeliness of HepB-BD, pentavalent vaccines, and other vaccines recommended by the national infant immunization program.
- -
- The prevalence of anti-HBs ≥10 IU/L (or ≥100 IU/L) in infants aged 9 months.
- -
- The prevalence of HBsAg in mothers of children aged 9 months.
- -
- The prevalence of HBeAg in HBsAg-positive mothers.
- -
- The prevalence of HBV DNA levels ≥200,000 IU/mL in HBsAg-positive mothers.
- -
- Anthropology: the acceptability of adding HepB-BD into the infant immunization program among healthcare workers and community members.
- -
- Health economics: the public health benefits, the cost, and the cost-effectiveness of introducing HepB-BD into the infant immunization program in Burkina Faso versus the current situation.
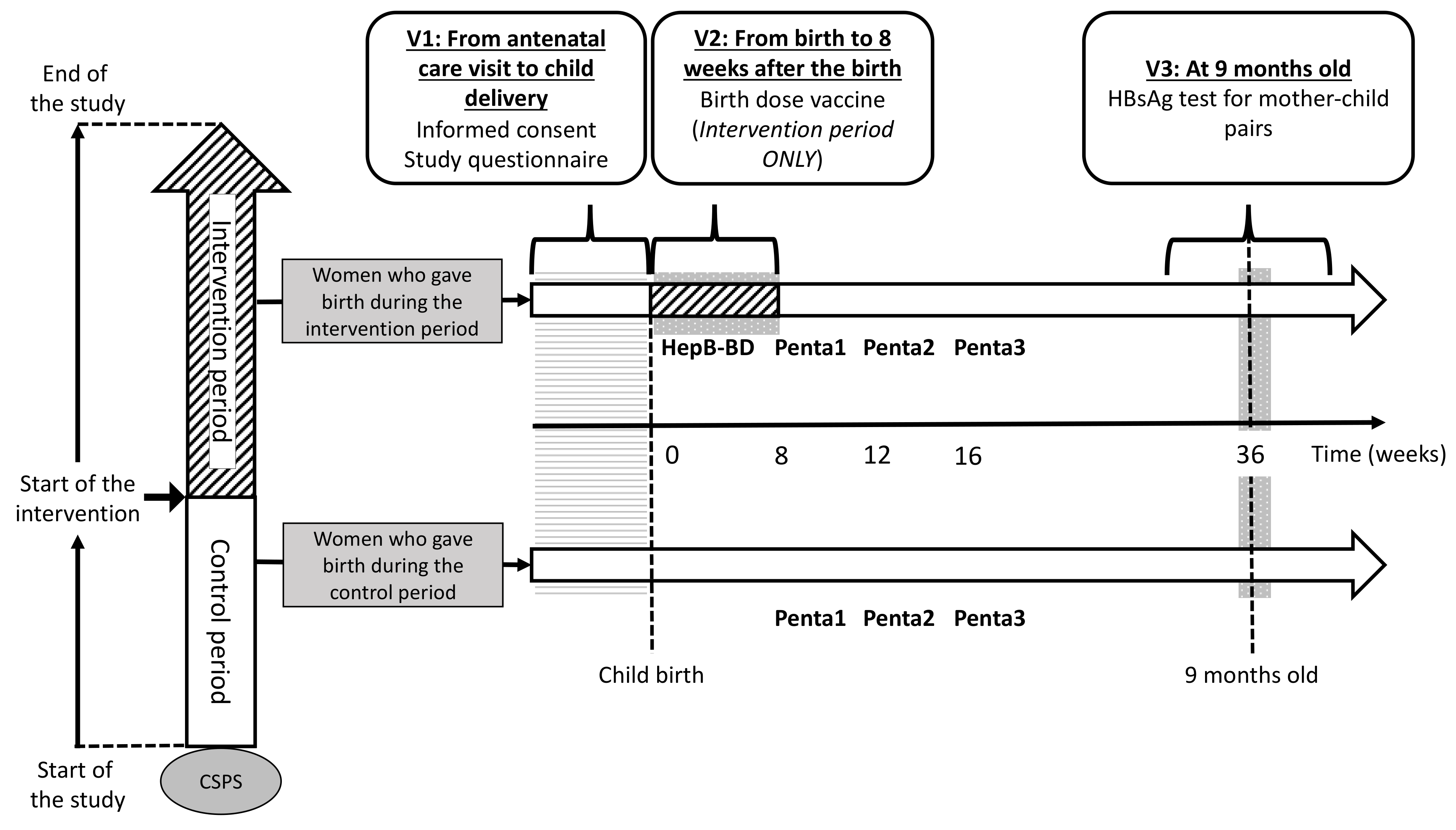
2.8. Participant Flow
2.8.1. First Visit (V1)
2.8.2. Second Visit (V2)
2.8.3. Third Visit (V3)
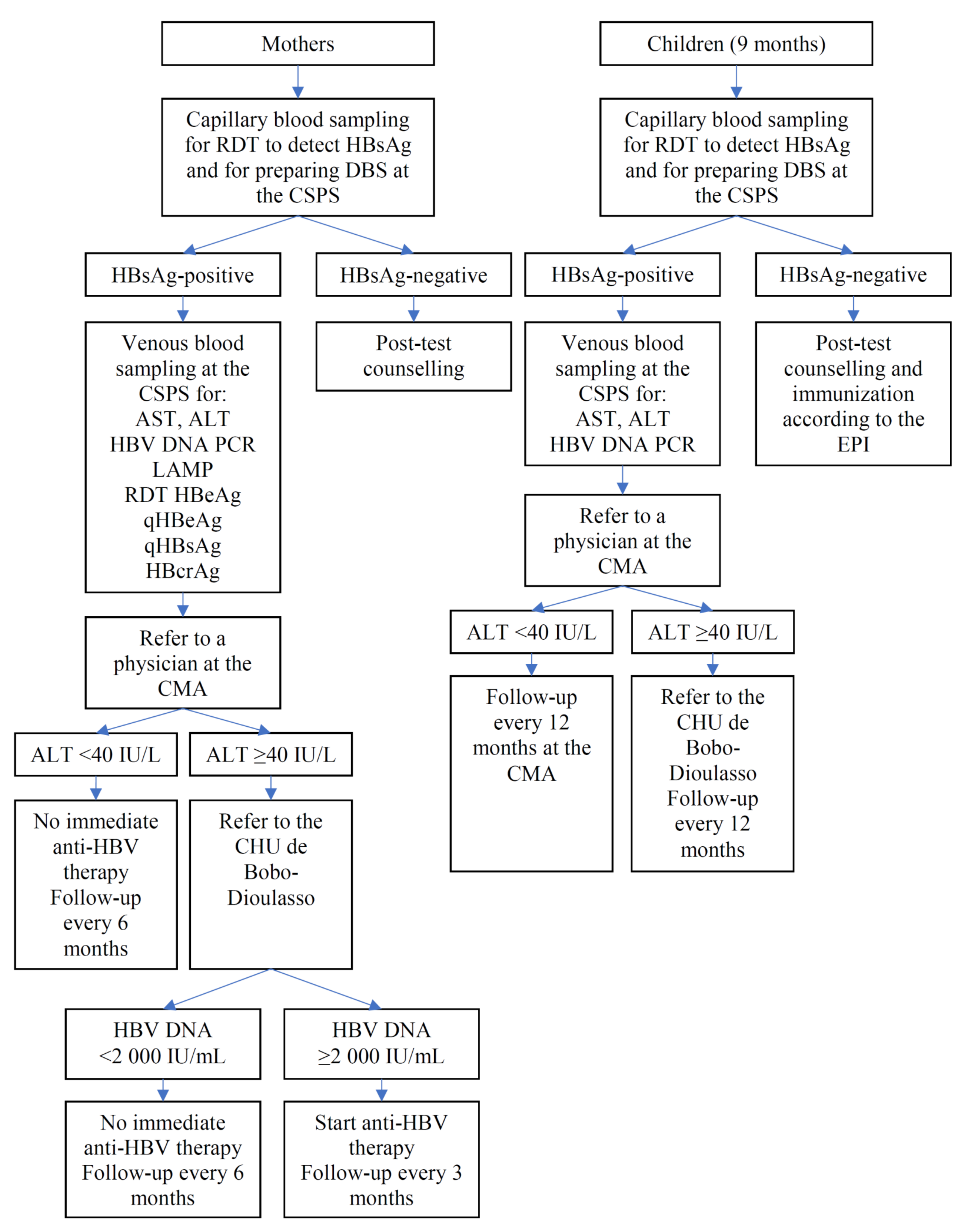
2.8.4. Participants Found to Carry HBsAg
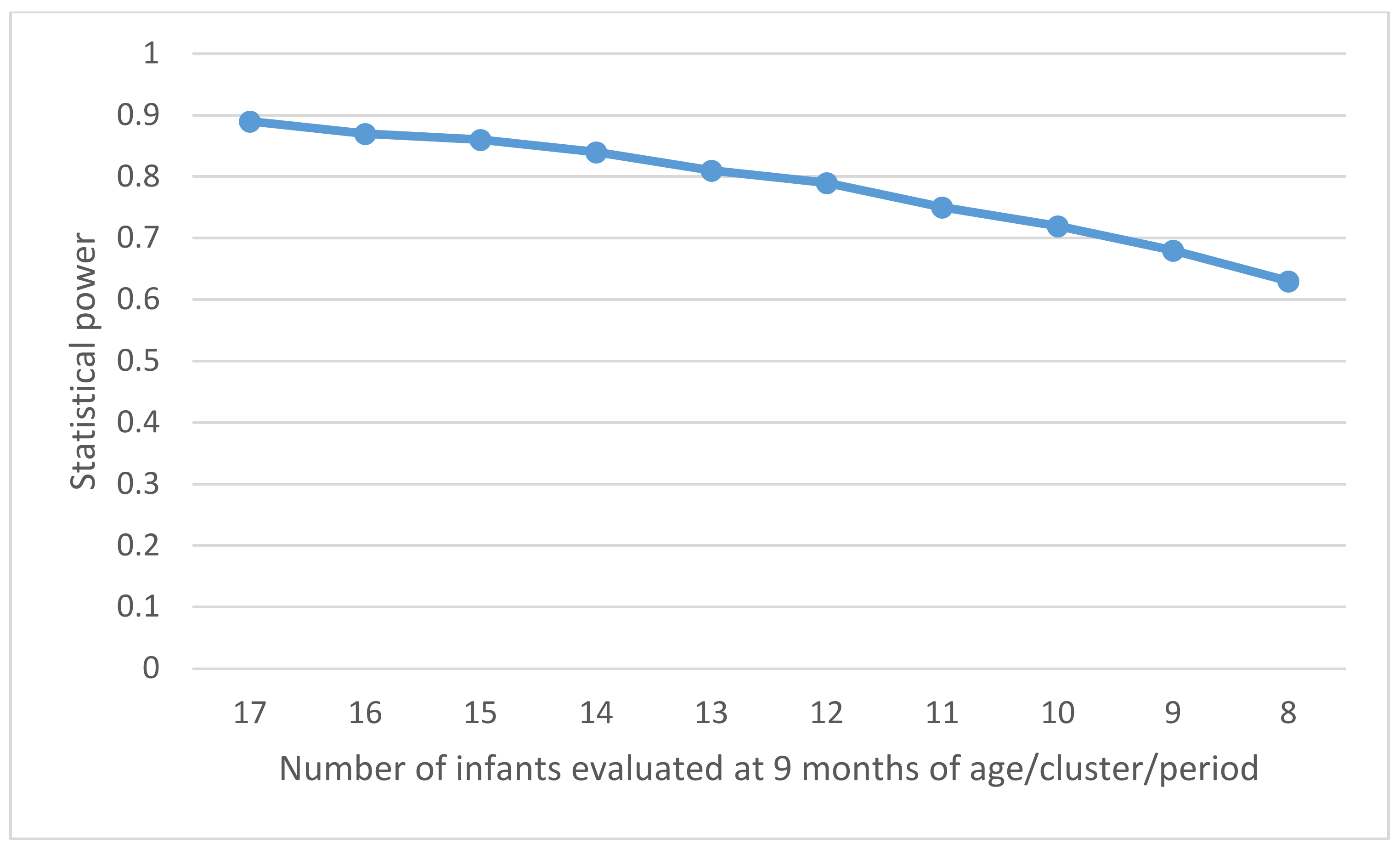
2.9. Power Calculation
- (a)
- The average number of live births in a catchment area covered by each CSPS is about 22 per month.
- (b)
- Infant death or lost to follow-up occurs in 10% of children by the age of 9 months.
- (c)
- The prevalence of HBsAg in pregnant women (PHBsAg) is estimated at 10%, but it can vary from 5% to 15% between the clusters [34].
- (d)
- The prevalence of HBeAg in HBsAg-positive pregnant women (PHBeAg) is estimated at 15%, but it can vary from 10% to 20% between the clusters [35].
- (e)
- (f)
2.10. Assignment of Intervention
2.11. Data Management
2.12. Statistical Methods
2.13. Monitoring
2.14. Research Ethics Approval
- -
- Comité de Recherche Clinique (CoRC), Institut Pasteur, Paris, France: approved on 25 October 2018.
- -
- IRB, Institut Pasteur, Paris, France: approved on 8 November 2018.
- -
- Comité d’éthique pour la recherche en santé (CERS), Ministère de la santé/Ministère de l’enseignement supérieur, de la recherche scientifique et de l’innovation, Burkina Faso: approved on 4 December 2018.
- -
- Comité d’éthique institutionnel du Centre MURAZ: approved on 4 April 2019.
- -
- Comité technique d’examen des demandes d’autorisation d’essais cliniques (CTEC): approved on 4 November 2019.
- -
- The project has also been registered in the ClinicalTrials.gov with the following ID (NCT04029454).
2.15. Dissemination Policy
2.16. Work Package 2: Anthropology
2.17. Work Package 3: Health Economics
2.18. Ancillary Study: PREDICT-B
- -
- To evaluate the performance of low-cost HBV markers to diagnose high-HBV DNA levels (≥200,000 UI/mL) quantified by real-time polymerase chain reaction (PCR) as a reference standard, in serum samples and dried blood spots (DBS) collected from HBsAg-positive mothers in Burkina Faso. The following alternative markers will be assessed:
- ◦
- ◦
- ◦
- ◦
- Semi-quantification of HBV DNA levels using hepatitis B loop-mediated isothermal amplification (HBV-LAMP) assay [63].
- -
- To evaluate the performance of the low-cost HBV markers in HBsAg-positive mothers to predict the risk of MTCT, defined as positive HBsAg in infants aged 9 months.
- -
- To compare the performance of the low-cost HBV markers to diagnose high HBV DNA levels (≥200,000 UI/mL) by the sample type (serum versus DBS).
- -
- To assess the effectiveness and cost-effectiveness of antenatal screening strategies using the low-cost HBV markers and subsequent antiviral treatment during pregnancy to prevent HBV MTCT in sub-Saharan Africa using modelling.
- In Burkina Faso, the vast majority of adults have been in contact with HBV during childhood, resulting in the prevalence of total hepatitis B core antibody (anti-HBc) exceeding 70–80% in adults [32]. Therefore, primo-infection during adulthood is very rare.
- HBV viral replication remains stable after pregnancy in HBsAg-positive women; a large observational study in Australia did not find any significant difference in HBV DNA levels between samples collected during pregnancy and those collected 12 months after delivery [64].
3. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Global Hepatitis Report, 2017; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Stanaway, J.D.; Flaxman, A.D.; Naghavi, M.; Fitzmaurice, C.; Vos, T.; Abubakar, I.; Abu-Raddad, L.J.; Assadi, R.; Bhala, N.; Cowie, B.; et al. The global burden of viral hepatitis from 1990 to 2013: Findings from the Global Burden of Disease Study 2013. Lancet 2016, 388, 1081–1088. [Google Scholar] [CrossRef] [Green Version]
- WHO. Global Health Sector Strategy on Viral Hepatitis 2016–2021; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Edmunds, W.J.; Medley, G.F.; Nokes, D.J.; Hall, A.J.; Whittle, H.C. The influence of age on the development of the hepatitis B carrier state. Proc. Biol. Sci. 1993, 253, 197–201. [Google Scholar] [CrossRef]
- Hyams, K.C. Risks of Chronicity Following Acute Hepatitis B Virus Infection: A Review. Clin. Infect. Dis. 1995, 20, 992–1000. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.-H. Natural history and clinical management of chronic hepatitis B virus infection in children. Hepatol. Int. 2008, 2, S28–S36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimakawa, Y.; Yan, H.-J.; Tsuchiya, N.; Bottomley, C.; Hall, A.J. Association of early age at establishment of chronic hepatitis b infection with persistent viral replication, liver cirrhosis and hepatocellular carcinoma: A systematic review. PLoS ONE 2013, 8, e69430. [Google Scholar] [CrossRef] [PubMed]
- Shimakawa, Y.; Lemoine, M.; Njai, H.F.; Bottomley, C.; Ndow, G.; Goldin, R.D.; Jatta, A.; Jeng-Barry, A.; Wegmuller, R.; E Moore, S.; et al. Natural history of chronic HBV infection in West Africa: A longitudinal population-based study from The Gambia. Gut 2016, 65, 2007–2016. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Huang, A.; Zhao, Y. Spontaneous loss of chronic HBV infection markers in treatment-naïve children: A systematic review and pooled meta-analyses. Expert Rev. Anti Infect. Ther. 2021, 19, 649–660. [Google Scholar] [CrossRef]
- WHO. Hepatitis B vaccines. WHO position paper. Wkly. Epidemiol. Rec. 2009, 84, 405–420. [Google Scholar]
- Spearman, C.W.; Afihene, M.; Ally, R.; Apica, B.; Awuku, Y.; Cunha, L.; Dusheiko, G.; Gogela, N.; Kassianides, C.; Kew, M.; et al. Hepatitis B in sub-Saharan Africa: Strategies to achieve the 2030 elimination targets. Lancet Gastroenterol. Hepatol. 2017, 2, 900–909. [Google Scholar] [CrossRef] [Green Version]
- WHO. WHO Vaccine-Preventable Diseases: Monitoring System. 2020 Global Summary (Data as of 12 October 2020). 2020. Available online: https://apps.who.int/immunization_monitoring/globalsummary/schedules (accessed on 7 January 2021).
- Sosler, S. Update on Gavi’s Support for HepB Birthdose. 2021, pp. 1–8. Available online: https://www.globalhep.org/sites/default/files/content/webinar/files/2021-04/Update_Gavi%20support%20for%20HepB%20BD_March%202021.pdf (accessed on 20 May 2021).
- GAVI the Vaccine Alliance. Gavi Board Starts Framing Alliance’s Approach to 2021–2025 Period 2018. Available online: https://www.gavi.org/news/media-room/gavi-board-starts-framing-alliances-approach-2021-2025-period (accessed on 5 February 2021).
- Bassoum, O.; Kimura, M.; Dia, A.T.; Lemoine, M.; Shimakawa, Y. Coverage and Timeliness of Birth Dose Vaccination in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. Vaccines 2020, 8, 301. [Google Scholar] [CrossRef]
- Moturi, E.; Tevi-Benissan, C.; Hagan, J.; Shendale, S.; Mayenga, D.; Murokora, D.; Patel, M.; Hennessey, K.; Mihigo, R. Implementing a Birth Dose of Hepatitis B Vaccine in Africa: Findings from Assessments in 5 Countries. J. Immunol. Sci. 2018, 2, 31–40. [Google Scholar] [CrossRef] [Green Version]
- WHO. Practices to Improve Coverage of the Hepatitis B Birth Dose Vaccine; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Lee, C.; Gong, Y.; Brok, J.; Boxall, E.H.; Gluud, C. Hepatitis B immunisation for newborn infants of hepatitis B surface antigen-positive mothers. Cochrane Database Syst. Rev. 2006, CD004790. [Google Scholar] [CrossRef]
- WHO. Systematic Review of Safety and Efficacy of Childhood Schedules Using Hepatitis B Containing Vaccines; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Ekra, D.; Herbinger, K.-H.; Konate, S.; Leblond, A.; Fretz, C.; Cilote, V.; Douai, C.; Da Silva, A.; Gessner, B.D.; Chauvin, P. A non-randomized vaccine effectiveness trial of accelerated infant hepatitis B immunization schedules with a first dose at birth or age 6 weeks in Côte d’Ivoire. Vaccine 2008, 26, 2753–2761. [Google Scholar] [CrossRef] [PubMed]
- WHO. Hepatitis B vaccines: WHO position paper—July 2017. Wkly. Epidemiol. Rec. 2017, 27, 369–392. [Google Scholar] [CrossRef]
- Marion, S.A.; Tomm Pastore, M.; Pi, D.W.; Mathias, R.G. Long-term follow-up of hepatitis b vaccine in infants of carrier mothers. Am. J. Epidemiol. 1994, 140, 734–746. [Google Scholar] [CrossRef]
- Diallo, M.Y.; Gosset, A.; Vray, M.; Ouédraogo, E.; Betsem, E.; Shimakawa, Y.; Boyer, S. Coût et efficacité de la vaccination à la naissance contre l’hépatite B au Burkina Faso, résultats préliminaires du projet Néovac. In Proceedings of the AfraVIH 2018, 9ème Conférence Internationale Francoph, VIH/Hépatites, Bordeaux, France, 4–7 April 2018; p. 115. [Google Scholar]
- Campbell, M.K.; Piaggio, G.; Elbourne, D.R.; Altman, D.G. Consort 2010 statement: Extension to cluster randomised trials. BMJ 2012, 345, e5661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemming, K.; Haines, T.; Chilton, P.J.; Girling, A.J.; Lilford, R.J. The stepped wedge cluster randomised trial: Rationale, design, analysis, and reporting. BMJ 2015, 350, h391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, A.W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Krleža-Jerić, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A.; et al. SPIRIT 2013 statement: Defining standard protocol items for clinical trials. Ann. Intern. Med. 2013, 158, 200–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, R.J.; Moulton, L.H. Cluster Randomised Trials; Chapman & Hall/CRC: Boca Raton, FL, USA, 2009. [Google Scholar]
- Ministère de la Santé du Burkina Faso. Plan d’Action 2015 du District Sanitaire de Dô; Bobo-Dioulasso, Burkina Faso, 2014.
- Ministère de la Santé du Burkina Faso. Plan d’Action 2016 du District Sanitaire de Dafra; Bobo-Dioulasso, Burkina Faso, 2015.
- Murayama, A.; Momose, H.; Yamada, N.; Hoshi, Y.; Muramatsu, M.; Wakita, T.; Ishimaru, K.; Hamaguchi, I.; Kato, T. Evaluation of in vitro screening and diagnostic kits for hepatitis B virus infection. J. Clin. Virol. 2019, 117, 37–42. [Google Scholar] [CrossRef]
- Avellon, A.; Ala, A.; Diaz, A.; Domingo, D.; Gonzalez, R.; Hidalgo, L.; Kooner, P.; Loganathan, S.; Martin, D.; McPherson, S.; et al. Clinical performance of Determine HBsAg 2 rapid test for Hepatitis B detection. J. Med Virol. 2020, 92, 3403–3411. [Google Scholar] [CrossRef] [Green Version]
- Collenberg, E.; Ouedraogo, T.; Ganamé, J.; Fickenscher, H.; Kynast-Wolf, G.; Becher, H.; Kouyaté, B.; Kräusslich, H.-G.; Sangaré, L.; Tebit, D.M. Seroprevalence of six different viruses among pregnant women and blood donors in rural and urban Burkina Faso: A comparative analysis. J. Med. Virol. 2006, 78, 683–692. [Google Scholar] [CrossRef] [PubMed]
- McNaughton, A.L.; Lourenço, J.; Bester, P.A.; Mokaya, J.; Lumley, S.F.; Obolski, U.; Forde, D.; Maponga, T.G.; Katumba, K.R.; Goedhals, D.; et al. Hepatitis B virus seroepidemiology data for Africa: Modelling intervention strategies based on a systematic review and meta-analysis. PLoS Med. 2020, 17, e1003068. [Google Scholar] [CrossRef] [Green Version]
- Lingani, M.; Akita, T.; Ouoba, S.; Sanou, A.M.; Sugiyama, A.; Tarnagda, Z.; Ohisa, M.; Tinto, H.; Mishiro, S.; Tanaka, J. High prevalence of hepatitis B infections in Burkina Faso (1996–2017): A systematic review with meta-analysis of epidemiological studies. BMC Public Health 2018, 18, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keane, E.; Funk, A.L.; Shimakawa, Y. Systematic review with meta-analysis: The risk of mother-to-child transmission of hepatitis B virus infection in sub-Saharan Africa. Aliment. Pharmacol. Ther. 2016, 44, 1005–1017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.D.; Lo, K.J.; Wu, J.C.; Tsai, Y.T.; Wang, J.Y.; Ting, L.P.; Tong, M.J. Prevention of maternal-infant hepatitis B virus transmission by immunization: The role of serum hepatitis B virus DNA. Hepatology 1986, 6, 369–373. [Google Scholar] [CrossRef] [PubMed]
- Machaira, M.; Papaevangelou, V.; Vouloumanou, E.K.; Tansarli, G.S.; Falagas, M.E. Hepatitis B vaccine alone or with hepatitis B immunoglobulin in neonates of HBsAg+/HBeAg− mothers: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2015, 70, 396–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemming, K.; Girling, A. A Menu-Driven Facility for Power and Detectable-Difference Calculations in Stepped-Wedge Cluster-Randomized Trials. Stata J. Promot. Commun. Stat. Stata 2014, 14, 363–380. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software partners. J Biomed. Inform 2019. [Google Scholar] [CrossRef]
- White, I.R.; Horton, N.J.; Carpenter, J.; Pocock, S.J. Strategy for intention to treat analysis in randomised trials with missing outcome data. BMJ 2011, 342, 910–912. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 Explanation and Elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c869. [Google Scholar] [CrossRef] [Green Version]
- Démolis, R.; Botão, C.; Heyerdahl, L.W.; Gessner, B.D.; Cavailler, P.; Sinai, C.; Magaço, A.; Le Gargasson, J.-B.; Mengel, M.; Guillermet, E. A rapid qualitative assessment of oral cholera vaccine anticipated acceptability in a context of resistance towards cholera intervention in Nampula, Mozambique. Vaccine 2018, 36, 6497–6505. [Google Scholar] [CrossRef]
- Giles-Vernick, T.; Traoré, A.; Bainilago, L. Incertitude, Hepatitis B, and Infant Vaccination in West and Central Africa. Med. Anthropol. Q. 2016, 30, 203–221. [Google Scholar] [CrossRef]
- Giles-Vernick, T.; Hejoaka, F.; Sanou, A.; Shimakawa, Y.; Bamba, I.; Traoré, A. Barriers to Linkage to Care for Hepatitis B Virus Infection: A Qualitative Analysis in Burkina Faso, West Africa. Am. J. Trop. Med. Hyg. 2016, 95, 1368–1375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimakawa, Y.; Pourette, D.; Bainilago, L.; Enel, C.; Sombié, R.; Rado, R.; Lemoine, M.; Giles-Vernick, T. Improving communication about viral hepatitis in Africa. Lancet Infect. Dis. 2017, 17, 688–689. [Google Scholar] [CrossRef]
- Boye, S.; Shimakawa, Y.; Vray, M.; Giles-Vernick, T. Limited awareness of hepatitis B but widespread recognition of its sequelae in rural senegal: A qualitative study. Am. J. Trop. Med. Hyg. 2020, 102, 637–643. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Guide for Standardization of Economic Evaluations of Immunization Programmes, 2nd ed.; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Nayagam, S.; Thursz, M.; Sicuri, E.; Conteh, L.; Wiktor, S.; Low-Beer, D.; Hallett, T.B. Requirements for global elimination of hepatitis B: A modelling study. Lancet Infect. Dis. 2016, 16, 1399–1408. [Google Scholar] [CrossRef] [Green Version]
- De Villiers, M.J.; Gamkrelidze, I.; Hallett, T.B.; Nayagam, S.; Razavi, H.; Razavi-Shearer, D. Modelling hepatitis B virus infection and impact of timely birth dose vaccine: A comparison of two simulation models. PLoS ONE 2020, 15, e0237525. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [Green Version]
- Maylin, S.; Boyd, A.; Martinot-Peignoux, M.; Delaugerre, C.; Bagnard, G.; Lapalus, M.; Zoulim, F.; Lavocat, F.; Marcellin, P.; Simon, F.; et al. Quantification of hepatitis B e antigen between Elecsys HBeAg and Architect HBeAg assays among patients infected with hepatitis B virus. J. Clin. Virol. 2013, 56, 306–311. [Google Scholar] [CrossRef]
- Seck, A.; Ndiaye, F.; Maylin, S.; Ndiaye, B.; Simon, F.; Funk, A.L.; Fontanet, A.; Takahashi, K.; Akbar, S.M.F.; Mishiro, S.; et al. Poor Sensitivity of Commercial Rapid Diagnostic Tests for Hepatitis B e Antigen in Senegal, West Africa. Am. J. Trop. Med. Hyg. 2018, 99, 428–434. [Google Scholar] [CrossRef]
- Clement, F.; Dewint, P.; Leroux-Roels, G. Evaluation of a New Rapid Test for the Combined Detection of Hepatitis B Virus Surface Antigen and Hepatitis B Virus e Antigen. J. Clin. Microbiol. 2002, 40, 4603–4606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, D.T.-Y.; Ma, H.; Lemon, S.M.; Doo, E.; Ghany, M.G.; Miskovsky, E.; Woods, G.L.; Park, Y.; Hoofnagle, J.H. A rapid immunochromatographic assay for hepatitis B virus screening. J. Viral Hepat. 2003, 10, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Akanmu, A.S.; A Esan, O.; O Adewuyi, J.; O Davies, A.; Okany, C.C.; O Olatunji, R.; Babalola, T. Evaluation of a rapid test kit for detection of HBsAg/eAg in whole blood: A possible method for pre-donation testing. Afr. J. Med. Med. Sci. 2006, 35, 5–8. [Google Scholar]
- Mainet-González, D.; Palenzuela-Gardon, D.O.; Aguilar Rubido, J.C. Comparison between an immunochromatographic test with an amplified ELISA for detecting e antigen and anti-e antigen antibodies in chronic Hepatitis B. Biotecnol. Apl. 2009, 26, 143–145. [Google Scholar]
- Boucheron, P.; Lu, Y.; Yoshida, K.; Zhao, T.; Funk, A.L.; Lunel-Fabiani, F.; Guingané, A.; Tuaillon, E.; van Holten, J.; Chou, R.; et al. Accuracy of HBeAg to identify pregnant women at risk of transmitting hepatitis B virus to their neonates: A systematic review and meta-analysis. Lancet Infect. Dis. 2021, 21, 85–96. [Google Scholar] [CrossRef]
- Ségéral, O.; N’Diaye, D.S.; Prak, S.; Nouhin, J.; Chhun, S.; Khamduang, W.; Chim, K.; Roque-Afonso, A.-M.; Piola, P.; Borand, L.; et al. Usefulness of a serial algorithm of HBsAg and HBeAg rapid diagnosis tests to detect pregnant women at risk of HBV mother-to-child transmission in Cambodia, the ANRS 12328 pilot study. J. Clin. Virol. 2018, 109, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Segeral, O.; Dim, B.; Durier, C.; Prak, S.; Chhim, K.; Vong, C.; Pech, S.; Tiv, S.; Nem, B.; Hout, K.; et al. Hepatitis B e Antigen (HBeAg) Rapid Test and Alanine Aminotransferase Level–Based Algorithm to Identify Pregnant Women at Risk of HBV Mother-to-Child Transmission: The ANRS 12345 TA PROHM Study. Clin. Infect. Dis. 2020, 71, E587–E593. [Google Scholar] [CrossRef] [Green Version]
- Shimakawa, Y.; Ndow, G.; Njie, R.; Njai, H.F.; Takahashi, K.; Akbar, S.M.F.; Cohen, D.; Nayagam, S.; Jeng, A.; Ceesay, A.; et al. Hepatitis B corerelated antigen: An alternative to hepatitis B Virus DNA to assess treatment eligibility in Africa. Clin. Infect. Dis. 2019, 70, 1442–1452. [Google Scholar] [CrossRef]
- Yoshida, K.; Desbiolles, A.; Feldman, S.F.; Ahn, S.H.; Alidjinou, E.K.; Atsukawa, M.; Bocket, L.; Brunetto, M.R.; Buti, M.; Carey, I.; et al. Hepatitis B Core-Related Antigen to Indicate High Viral Load: Systematic Review and Meta-Analysis of 10,397 Individual Participants. Clin. Gastroenterol. Hepatol. 2021, 19, 46–60.e8. [Google Scholar] [CrossRef]
- Shimakawa, Y.; Vernoux, L.; Gabassi, A.; Mercier-Delarue, S.; Vincent, J.P.; Simon, F.; Maylin, S. Analytical validation of hepatitis B core-related antigen (HBcrAg) using dried blood spots (DBS). J. Viral Hepat. 2021, 28, 837–843. [Google Scholar] [CrossRef]
- Vanhomwegen, J.; Kwasiborski, A.; Diop, A.; Boizeau, L.; Hoinard, D.; Vray, M.; Bercion, R.; Ndiaye, B.; Dublineau, A.; Michiyuki, S.; et al. Development and clinical validation of loop-mediated isothermal amplification (LAMP) assay to diagnose high HBV DNA levels in resource-limited settings. Clin. Microbiol. Infect. 2021. [Google Scholar] [CrossRef]
- Giles, M.; Visvanathan, K.; Lewin, S.; Bowden, S.; Locarnini, S.; Spelman, T.; Sasadeusz, J. Clinical and virological predictors of hepatic flares in pregnant women with chronic hepatitis B. Gut 2015, 64, 1810–1815. [Google Scholar] [CrossRef]
- Brown, R.S.; McMahon, B.J.; Lok, A.S.; Wong, J.B.; Ahmed, A.T.; Mouchli, M.A.; Wang, Z.; Prokop, L.J.; Murad, M.H.; Mohammed, K. Antiviral therapy in chronic hepatitis B viral infection during pregnancy: A systematic review and meta-analysis. Hepatology 2016, 63, 319–333. [Google Scholar] [CrossRef]
- Funk, A.L.; Lu, Y.; Yoshida, K.; Zhao, T.; Boucheron, P.; van Holten, J.; Chou, R.; Bulterys, M.; Shimakawa, Y. Efficacy and safety of antiviral prophylaxis during pregnancy to prevent mother-to-child transmission of hepatitis B virus: A systematic review and meta-analysis. Lancet Infect. Dis. 2021, 21, 70–84. [Google Scholar] [CrossRef]
- WHO. Prevention of Mother-to-Child Transmission of Hepatitis B Virus: Guidelines on Antiviral Prophylaxis in Pregnancy; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Terrault, N.A.; Lok, A.S.; McMahon, B.J.; Chang, K.-M.; Hwang, J.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef]
- Sarin, S.K.; Kumar, M.P.; Lau, G.K.; Abbas, Z.; Chan, H.L.Y.; Chen, C.J.; Chen, D.-S.; Chen, H.L.; Chien, R.N.; Dokmeci, A.; et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: A 2015 update. Hepatol. Int. 2016, 10, 1–98. [Google Scholar] [CrossRef] [PubMed]
- Shimakawa, Y.; Toure-Kane, C.; Mendy, M.; Thursz, M.; Lemoine, M. Mother-to-child transmission of hepatitis B in sub-Saharan Africa. Lancet Infect. Dis. 2016, 16, 19–20. [Google Scholar] [CrossRef]
- Hagan, J.E.; Carvalho, E.; Souza, V.; Dos Anjos, M.Q.; Abimbola, T.O.; Pallas, S.W.; Benissan, M.C.T.; Shendale, S.; Hennessey, K.; Patel, M.K. Selective Hepatitis B Birth-Dose Vaccination in São Tomé and Príncipe: A Program Assessment and Cost-Effectiveness Study. Am. J. Trop. Med. Hyg. 2019, 101, 891–898. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Strategies | Screening For Pregnant Women | Peripartum Antiviral Prophylaxis | HepB-BD | HepB3 (8-12-16 weeks) | |
|---|---|---|---|---|---|
| HBsAg RDT | Test for High Viral Replication * | ||||
| Current standard of care | - | - | - | - | Yes |
| Universal birth dose vaccination | - | - | - | Yes | Yes |
| Two-step diagnostic procedure (conventional approach in resource-rich context) | Yes | Yes (Only those tested positive for HBsAg) | Yes (Only those with high viral replication) | Yes | Yes |
| One-step diagnostic procedure | - | Yes (Test all women for high viral replication) | Yes (Only those with high viral replication) | Yes | Yes |
| Treat-all strategy | Yes | - | Yes (All HBsAg-positive women) | Yes | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tall, H.; Adam, P.; Tiendrebeogo, A.S.E.; Vincent, J.P.; Schaeffer, L.; von Platen, C.; Fernandes-Pellerin, S.; Sawadogo, F.; Bokoum, A.; Bouda, G.; et al. Impact of Introducing Hepatitis B Birth Dose Vaccines into the Infant Immunization Program in Burkina Faso: Study Protocol for a Stepped Wedge Cluster Randomized Trial (NéoVac Study). Vaccines 2021, 9, 583. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9060583
Tall H, Adam P, Tiendrebeogo ASE, Vincent JP, Schaeffer L, von Platen C, Fernandes-Pellerin S, Sawadogo F, Bokoum A, Bouda G, et al. Impact of Introducing Hepatitis B Birth Dose Vaccines into the Infant Immunization Program in Burkina Faso: Study Protocol for a Stepped Wedge Cluster Randomized Trial (NéoVac Study). Vaccines. 2021; 9(6):583. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9060583
Chicago/Turabian StyleTall, Haoua, Pierrick Adam, Abdoul Salam Eric Tiendrebeogo, Jeanne Perpétue Vincent, Laura Schaeffer, Cassandre von Platen, Sandrine Fernandes-Pellerin, François Sawadogo, Alkadri Bokoum, Ghislain Bouda, and et al. 2021. "Impact of Introducing Hepatitis B Birth Dose Vaccines into the Infant Immunization Program in Burkina Faso: Study Protocol for a Stepped Wedge Cluster Randomized Trial (NéoVac Study)" Vaccines 9, no. 6: 583. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9060583