
Global Trends and Correlates of COVID-19 Vaccination Hesitancy: Findings from the iCARE Study

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants and Recruitment
2.3. iCARE Survey Questionnaire
2.4. Data Analysis
3. Results
3.1. Sample Description
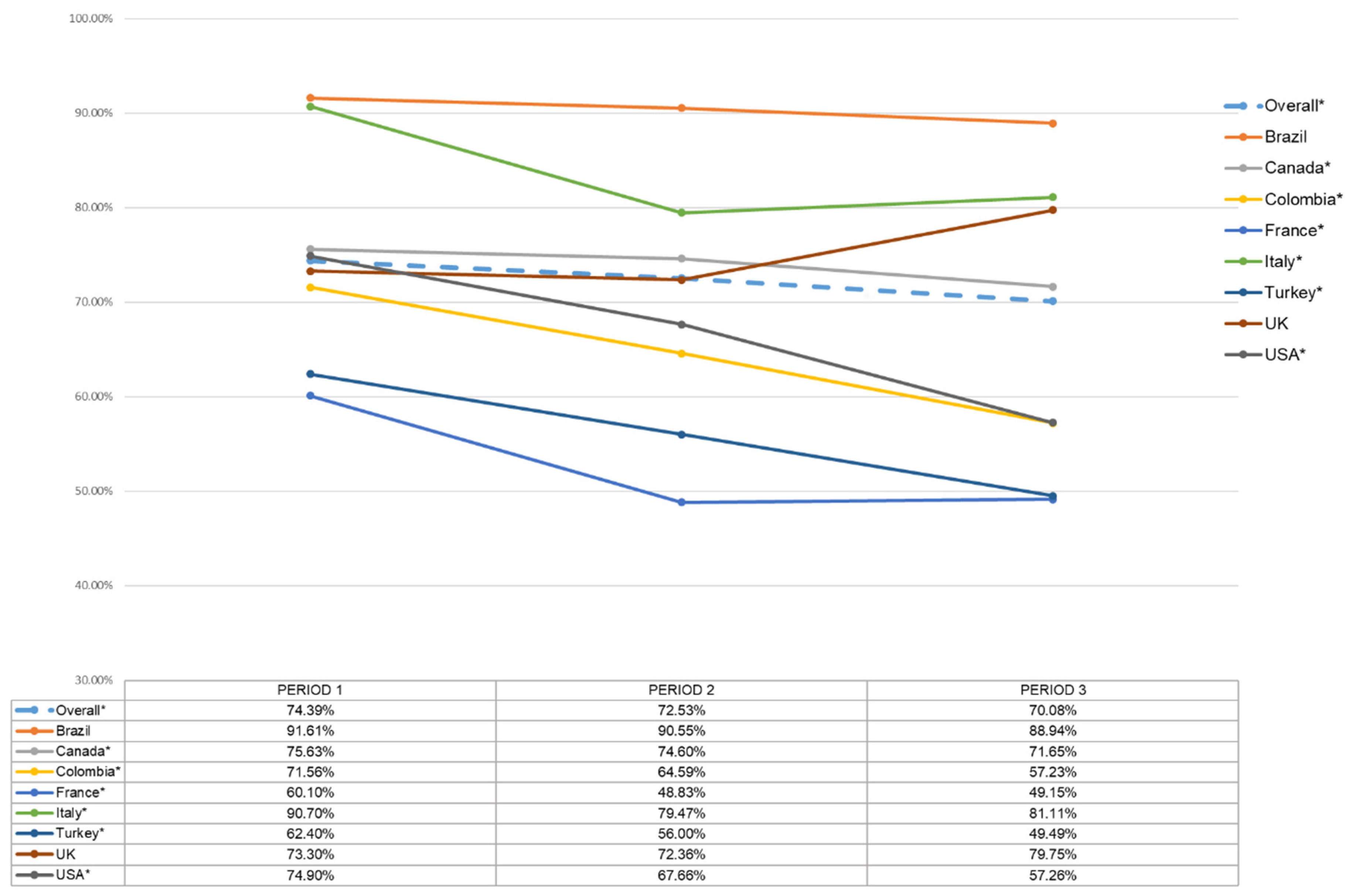
3.2. Estimates of Vaccine Hesitancy and Changes over Time
3.3. Predictors of Vaccine Hesitancy
3.4. Association between COVID-19-Related Concerns and Vaccine Hesitancy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 20 April 2021).
- de Figueiredo, A.; Simas, C.; Karafillakis, E.; Paterson, P.; Larson, H.J. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: A large-scale retrospective temporal modelling study. Lancet 2020, 396, 898–908. [Google Scholar] [CrossRef]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.D.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Covid World Vaccination Tracker—The New York Times. Available online: https://www.nytimes.com/interactive/2021/world/covid-vaccinations-tracker.html (accessed on 20 April 2021).
- Covid-19 Vaccine Tracker. Available online: https://vac-lshtm.shinyapps.io/ncov_vaccine_landscape/ (accessed on 20 April 2021).
- Shrotri, M.; Swinnen, T.; Kampmann, B.; Parker, E.P.K. An interactive website tracking COVID-19 vaccine development. Lancet Glob. Heal. 2021, 9, e590–e592. [Google Scholar] [CrossRef]
- Wouters, O.J.; Shadlen, K.C.; Salcher-Konrad, M.; Pollard, A.J.; Larson, H.J.; Teerawattananon, Y.; Jit, M. Challenges in ensuring global access to COVID-19 vaccines: Production, affordability, allocation, and deployment. Lancet 2021, 397, 1023–1034. [Google Scholar] [CrossRef]
- Wang, W.; Wu, Q.; Yang, J.; Dong, K.; Chen, X.; Bai, X.; Chen, X.; Chen, Z.; Viboud, C.; Ajelli, M.; et al. Global, regional, and national estimates of target population sizes for COVID-19 vaccination. medRxiv 2020. [Google Scholar] [CrossRef]
- Global.Health. A Data Science Initiative. Available online: https://global.health/ (accessed on 20 April 2021).
- Abu-Raddad, L.J.; Chemaitelly, H.; Butt, A.A. Effectiveness of the BNT162b2 Covid-19 Vaccine against the B.1.1.7 and B.1.351 Variants. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Adam, D. What scientists know about new, fast-spreading coronavirus variants. Nature 2021. [Google Scholar] [CrossRef] [PubMed]
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccines Immunother. 2020, 16, 1–8. [Google Scholar] [CrossRef]
- Limaye, R.J.; Sauer, M.; Truelove, S.A. Politicizing public health: The powder keg of rushing COVID-19 vaccines. Hum. Vaccines Immunother. 2020. [Google Scholar] [CrossRef]
- Sallam, M. Covid-19 vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Wyka, K.; Rauh, L.; Rabin, K.; Ratzan, S.; Gostin, L.O.; Larson, H.J.; El-Mohandes, A. Hesitant or Not? The Association of Age, Gender, and Education with Potential Acceptance of a COVID-19 Vaccine: A Country-level Analysis. J. Health Commun. 2020, 25, 799–807. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and receptivity for covid-19 vaccines: A rapid systematic review. Vaccines 2021, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Bacon, S.L.; Lavoie, K.L.; Boyle, J.; Stojanovic, J.; Joyal-Desmarais, K. International assessment of the link between COVID-19 related attitudes, concerns and behaviours in relation to public health policies: Optimising policy strategies to improve health, economic and quality of life outcomes (the iCARE Study). BMJ Open 2021, 11, 46127. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6. [Google Scholar] [CrossRef] [Green Version]
- Rosenstock, I.M. The Health Belief Model and Preventive Health Behavior. Health Educ. Monogr. 1974, 2, 354–386. [Google Scholar] [CrossRef]
- Kaiser, H.F. The Application of Electronic Computers to Factor Analysis. Educ. Psychol. Meas. 1960, 20, 141–151. [Google Scholar] [CrossRef]
- Salali, G.D.; Uysal, M.S. COVID-19 vaccine hesitancy is associated with beliefs on the origin of the novel coronavirus in the UK and Turkey. Psychol. Med. 2020, 1, 1–3. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Byrne, T.; Patel, P.; Shrotri, M.; Beale, S.; Michie, S.; Butt, J.; Hawkins, N.; Hardelid, P.; Rodger, A.; Aryee, A.; et al. Trends, patterns and psychological influences on COVID-19 vaccination intention: Findings from a large prospective community cohort study in England and Wales (Virus Watch). medRxiv 2021. [Google Scholar] [CrossRef]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Heal. Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef]
- Bish, A.; Yardley, L.; Nicoll, A.; Michie, S. Factors associated with uptake of vaccination against pandemic influenza: A systematic review. Vaccine 2011, 29, 6472–6484. [Google Scholar] [CrossRef]
- Brien, S.; Kwong, J.C.; Buckeridge, D.L. The determinants of 2009 pandemic A/H1N1 influenza vaccination: A systematic review. Vaccine 2012, 30, 1255–1264. [Google Scholar] [CrossRef]
- Latkin, C.A.; Dayton, L.; Yi, G.; Colon, B.; Kong, X. Mask usage, social distancing, racial, and gender correlates of COVID-19 vaccine intentions among adults in the US. PLoS ONE 2021, 16, e0246970. [Google Scholar] [CrossRef]
- Green, M.S.; Abdullah, R.; Vered, S.; Nitzan, D. A study of ethnic, gender and educational differences in attitudes toward COVID-19 vaccines in Israel—Implications for vaccination implementation policies. Isr. J. Health Policy Res. 2021, 10, 26. [Google Scholar] [CrossRef]
- Gustafson, P.E. Gender differences in risk perception: Theoretical and methodological perspectives. Risk Anal. 1998, 18, 805–811. [Google Scholar] [CrossRef] [PubMed]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; van der Bles, A.M.; Spiegelhalter, D.; van der Linden, S. Risk perceptions of COVID-19 around the world. J. Risk Res. 2020, 23, 994–1006. [Google Scholar] [CrossRef]
- COVID-19 and Its Economic Toll on Women: The Story behind the Numbers; UN Women: New York, NY, USA, 2020; Available online: https://www.unwomen.org/en/news/stories/2020/9/feature-covid-19-economic-impacts-on-women (accessed on 20 April 2021).
- Lavoie, K.L.; Gosselin-Boucher, V.; Stojanovic, J.; Voisard, B.; Szczepanik, G.; Boyle, J.A.; Belanger-Gravel, A.; Bacon, S.L. Determinants of adherence to COVID-19 preventive behaviours in Canada: Results from the iCARE Study. medRxiv 2021. [Google Scholar] [CrossRef]
- Flanagan, K.L.; Fink, A.L.; Plebanski, M.; Klein, S.L. Sex and gender differences in the outcomes of vaccination over the life course. Annu. Rev. Cell Dev. Biol. 2017, 33, 577–599. [Google Scholar] [CrossRef] [PubMed]
- Kleina, S.L.; Marriott, I.; Fish, E.N. Sex-based differences in immune function and responses to vaccination. Trans. R. Soc. Trop. Med. Hyg. 2014, 109, 9–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galasso, V.; Pons, V.; Profeta, P.; Becher, M.; Brouard, S.; Foucault, M. Gender differences in COVID-19 attitudes and behavior: Panel evidence from eight countries. Proc. Natl. Acad. Sci. USA 2020, 117, 27285–27291. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Vaccine Janssen: EMA Finds Possible Link to Very Rare Cases of Unusual Blood Clots with Low Blood Platelets; European Medicines Agency: Amsterdam, The Netherlands, 2021. Available online: https://www.ema.europa.eu/en/news/covid-19-vaccine-janssen-ema-finds-possible-link-very-rare-cases-unusual-blood-clots-low-blood (accessed on 3 May 2021).
- AstraZeneca’s COVID-19 Vaccine: EMA Finds Possible Link to Very Rare Cases of Unusual Blood Clots with Low Blood Platelets; European Medicines Agency: Amsterdam, The Netherlands, 2021. Available online: https://www.ema.europa.eu/en/news/astrazenecas-covid-19-vaccine-ema-finds-possible-link-very-rare-cases-unusual-blood-clots-low-blood (accessed on 3 May 2021).
- Booth, A.; Reed, A.B.; Ponzo, S.; Yassaee, A.; Aral, M.; Plans, D.; Labrique, A.; Mohan, D. Population risk factors for severe disease and mortality in COVID-19: A global systematic review and meta-analysis. PLoS ONE 2021, 16, e0247461. [Google Scholar] [CrossRef]
- Whitehead, M.; Taylor-Robinson, D.; Barr, B. Poverty, health, and covid-19. BMJ 2021, 372, n376. [Google Scholar] [CrossRef]
- Caserotti, M.; Girardi, P.; Rubaltelli, E.; Tasso, A.; Lotto, L.; Gavaruzzi, T. Associations of COVID-19 risk perception with vaccine hesitancy over time for Italian residents. Soc. Sci. Med. 2021, 272, 113688. [Google Scholar] [CrossRef]
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications. Lancet Reg. Heal. Eur. 2021, 1, 100012. [Google Scholar] [CrossRef]
- Schwarzinger, M.; Watson, V.; Arwidson, P.; Alla, F.; Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Heal. 2021, 6, e210–e221. [Google Scholar] [CrossRef]
- Fridman, A.; Gershon, R.; Gneezy, A. COVID-19 and vaccine hesitancy: A longitudinal study. PLoS ONE 2021, 16, e0250123. [Google Scholar] [CrossRef]
- Szmyd, B.; Karuga, F.F.; Bartoszek, A.; Staniecka, K.; Siwecka, N.; Bartoszek, A.; Błaszczyk, M.; Radek, M. Attitude and behaviors towards sars-cov-2 vaccination among healthcareworkers: A cross-sectional study from Poland. Vaccines 2021, 9, 218. [Google Scholar] [CrossRef]
- Szmyd, B.; Bartoszek, A.; Karuga, F.F.; Staniecka, K.; Błaszczyk, M.; Radek, M. Medical students and sars-cov-2 vaccination: Attitude and behaviors. Vaccines 2021, 9, 128. [Google Scholar] [CrossRef]
- Brewer, N.T.; Chapman, G.B.; Gibbons, F.X.; Gerrard, M.; McCaul, K.D.; Weinstein, N.D. Meta-analysis of the relationship between risk perception and health behavior: The example of vaccination. Heal. Psychol. 2007, 26, 136–145. [Google Scholar] [CrossRef] [Green Version]
- Faasse, K.; Newby, J. Public Perceptions of COVID-19 in Australia: Perceived Risk, Knowledge, Health-Protective Behaviors, and Vaccine Intentions. Front. Psychol. 2020, 11, 551004. [Google Scholar] [CrossRef] [PubMed]
- Loomba, S.; de Figueiredo, A.; Piatek, S.J.; de Graaf, K.; Larson, H.J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat. Hum. Behav. 2021, 5, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Böhm, R.; Korn, L. Inviting free-riders or appealing to prosocial behavior? Game-theoretical reflections on communicating herd immunity in vaccine advocacy. Health Psychol. 2013, 32, 978–985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, C.M.C.; Plotkin, S.A. Impact of Vaccines; Health, Economic and Social Perspectives. Front. Microbiol. 2020, 11, 1526. [Google Scholar] [CrossRef] [PubMed]
- iCARE Study. Infographics—MBMC. Available online: https://mbmc-cmcm.ca/covid19/research/infog/ (accessed on 4 May 2021).
- McEachan, R.; Taylor, N.; Harrison, R.; Lawton, R.; Gardner, P.; Conner, M. Meta-Analysis of the Reasoned Action Approach (RAA) to Understanding Health Behaviors. Ann. Behav. Med. 2016, 50, 592–612. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Sociodemographic and Health Variables | Vaccine Hesitancy | ||||
|---|---|---|---|---|---|
| Somewhat Likely, Unlikely, Very Unlikely | Extremely Likely | p-Value a | |||
| N | % | N | % | ||
| Overall | 7074 | 26.61 | 19,508 | 73.39 | |
| Missing values | 5446 | ||||
| Period b | |||||
| 3 | 1064 | 29.92 | 2492 | 70.08 | <0.0001 |
| 2 | 1678 | 27.47 | 4431 | 72.53 | |
| 1 | 4332 | 25.61 | 12,585 | 74.39 | |
| Continent | |||||
| North America | 4022 | 25.66 | 11,653 | 74.34 | <0.0001 |
| Europe | 2249 | 32.19 | 4738 | 67.81 | |
| South America | 803 | 20.48 | 3117 | 79.52 | |
| Sex | |||||
| Women | 5272 | 27.66 | 13,788 | 72.34 | <0.0001 |
| Men | 1724 | 23.6 | 5581 | 76.4 | |
| Age | |||||
| Less than or equal to 29 | 1898 | 28.32 | 4803 | 71.68 | <0.0001 |
| 30–64 years | 4510 | 28.18 | 11,495 | 71.82 | |
| 65 years or more | 633 | 16.74 | 3148 | 83.26 | |
| Education level | |||||
| High school or lower | 1477 | 25.83 | 4242 | 74.17 | 0.3451 |
| Graduate or postgraduate degree | 5177 | 26.45 | 14,395 | 73.55 | |
| Current employment status | |||||
| Unemployed | 1095 | 21.26 | 4056 | 78.74 | <0.0001 |
| Employed | 4135 | 27.72 | 10,784 | 72.28 | |
| Student | 550 | 32.05 | 1166 | 67.95 | |
| Residential area | |||||
| Rural or country area | 987 | 29.79 | 2326 | 70.21 | <0.0001 |
| Suburban or regional | 1922 | 27.88 | 4972 | 72.12 | |
| Urban or city | 3753 | 24.79 | 11,385 | 75.21 | |
| Perceived average annual household income | |||||
| Bottom third | 1027 | 33.56 | 2033 | 66.44 | <0.0001 |
| Middle third | 3433 | 27.82 | 8907 | 72.18 | |
| Top third | 1497 | 19.97 | 6001 | 80.03 | |
| Health condition at risk | |||||
| No | 4650 | 27.94 | 11,991 | 72.06 | <0.0001 |
| Yes | 2071 | 23.23 | 6844 | 76.77 | |
| History of seasonal influenza vaccination | |||||
| Never or once or twice in the last 5 years | 5365 | 34.89 | 10,010 | 65.11 | <0.0001 |
| Every year and 3 times in the last 5 years | 1188 | 12.41 | 8387 | 87.59 | |
| Sociodemographic and Health Variables | Univariate Analysis a | Multivariate Analysis b | ||||||
|---|---|---|---|---|---|---|---|---|
| OR c | 95% Confidence Interval | p-Value | OR c | 95% Confidence Interval | p-Value | |||
| Lower | Upper | Lower | Upper | |||||
| Period d | ||||||||
| 3 | 1 | 1 | ||||||
| 2 | 0.89 | 0.81 | 0.97 | 0.0099 | 0.77 | 0.69 | 0.86 | <0.0001 |
| 1 | 0.81 | 0.74 | 0.87 | <0.0001 | 0.63 | 0.57 | 0.7 | <0.0001 |
| Continent | ||||||||
| North America | 1 | 1 | ||||||
| Europe | 1.38 | 1.29 | 1.46 | <0.0001 | 1.37 | 1.27 | 1.49 | <0.0001 |
| South America | 0.75 | 0.69 | 0.81 | <0.0001 | 0.66 | 0.58 | 0.74 | <0.0001 |
| Sex | ||||||||
| Women | 1 | 1 | ||||||
| Men | 0.81 | 0.76 | 0.86 | <0.0001 | 0.84 | 0.78 | 0.91 | <0.0001 |
| Age | ||||||||
| Less than or equal to 29 | 1 | 1 | ||||||
| 30–64 years | 0.99 | 0.93 | 1.06 | 0.8243 | 1.04 | 0.93 | 1.15 | 0.5273 |
| 65 years or more | 0.51 | 0.46 | 0.56 | <0.0001 | 0.75 | 0.64 | 0.88 | 0.0004 |
| Education level | ||||||||
| High school or lower | 1 | 1 | ||||||
| Graduate or postgraduate degree | 1.03 | 0.97 | 1.11 | 0.3472 | 1.07 | 0.98 | 1.18 | 0.1306 |
| Current employment status | ||||||||
| Unemployed | 1 | 1 | ||||||
| Employed | 1.42 | 1.32 | 1.53 | <0.0001 | 1.03 | 0.93 | 1.15 | 0.5495 |
| Student | 1.75 | 1.55 | 1.97 | <0.0001 | 1.08 | 0.92 | 1.27 | 0.3643 |
| Residential area | ||||||||
| Rural or country area | 1 | 1 | ||||||
| Suburban or regional | 0.91 | 0.83 | 0.99 | 0.045 | 0.98 | 0.87 | 1.09 | 0.6787 |
| Urban or city | 0.78 | 0.72 | 0.84 | <0.0001 | 0.83 | 0.74 | 0.92 | 0.0003 |
| Perceived average annual household income | ||||||||
| Bottom third | 1 | 1 | ||||||
| Middle third | 0.76 | 0.70 | 0.83 | <0.0001 | 0.81 | 0.73 | 0.90 | <0.0001 |
| Top third | 0.49 | 0.45 | 0.54 | <0.0001 | 0.53 | 0.47 | 0.59 | <0.0001 |
| Health condition at risk e | ||||||||
| No | 1 | 1 | ||||||
| Yes | 0.78 | 0.74 | 0.83 | <0.0001 | 0.97 | 0.90 | 1.05 | 0.4244 |
| History of seasonal influenza vaccination | ||||||||
| Never or once or twice in the last 5 years | 1 | 1 | ||||||
| Every year and 3 times in the last 5 years | 0.26 | 0.25 | 0.28 | <0.0001 | 0.26 | 0.24 | 0.29 | <0.0001 |
| OR d | 95% CI e | |||||
|---|---|---|---|---|---|---|
| Variable | Estimate a | SE b | p-Value c | Lower | Upper | |
| Intercept | 1.101 | 0.108 | <0.0001 | |||
| Health concerns (others) (continuous) | −0.309 | 0.025 | <0.0001 | 0.73 | 0.70 | 0.77 |
| Health concerns (self) (continuous) | −0.374 | 0.022 | <0.0001 | 0.69 | 0.66 | 0.72 |
| Personal financial concerns (continuous) | 0.369 | 0.020 | <0.0001 | 1.45 | 1.39 | 1.50 |
| Social/economic concerns (continuous) | −0.199 | 0.022 | <0.0001 | 0.82 | 0.79 | 0.86 |
| Goodness-of-Fit Test f (p = 0.06) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stojanovic, J.; Boucher, V.G.; Gagne, M.; Gupta, S.; Joyal-Desmarais, K.; Paduano, S.; Aburub, A.S.; Sheinfeld Gorin, S.N.; Kassianos, A.P.; Ribeiro, P.A.B.; et al. Global Trends and Correlates of COVID-19 Vaccination Hesitancy: Findings from the iCARE Study. Vaccines 2021, 9, 661. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9060661
Stojanovic J, Boucher VG, Gagne M, Gupta S, Joyal-Desmarais K, Paduano S, Aburub AS, Sheinfeld Gorin SN, Kassianos AP, Ribeiro PAB, et al. Global Trends and Correlates of COVID-19 Vaccination Hesitancy: Findings from the iCARE Study. Vaccines. 2021; 9(6):661. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9060661
Chicago/Turabian StyleStojanovic, Jovana, Vincent G. Boucher, Myriam Gagne, Samir Gupta, Keven Joyal-Desmarais, Stefania Paduano, Ala’ S. Aburub, Sherri N. Sheinfeld Gorin, Angelos P. Kassianos, Paula A. B. Ribeiro, and et al. 2021. "Global Trends and Correlates of COVID-19 Vaccination Hesitancy: Findings from the iCARE Study" Vaccines 9, no. 6: 661. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9060661