
IgG Antibodies Generation and Side Effects Caused by Ad5-nCoV Vaccine (CanSino Biologics) and BNT162b2 Vaccine (Pfizer/BioNTech) among Mexican Population

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. S1 IgG Antibodiesdetection
2.3. Statistical Analysis
3. Results
3.1. Study Population
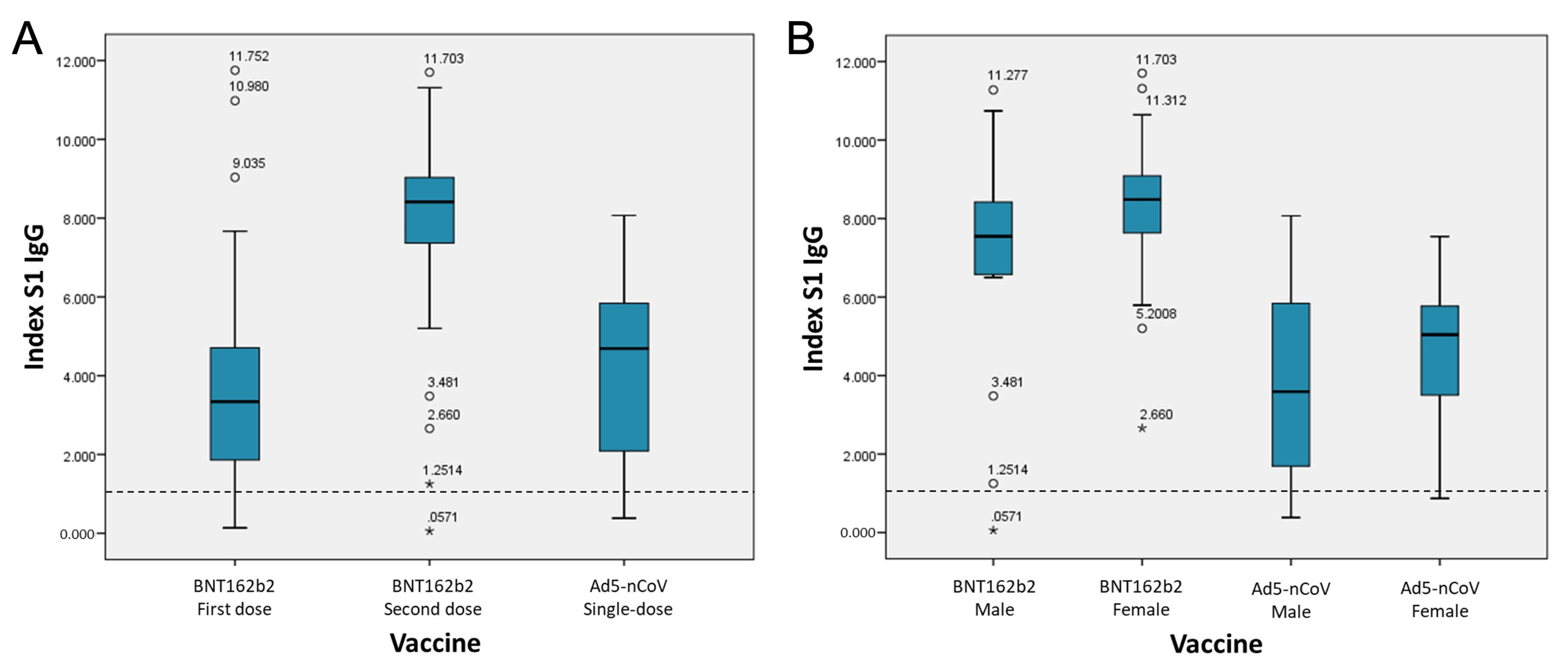
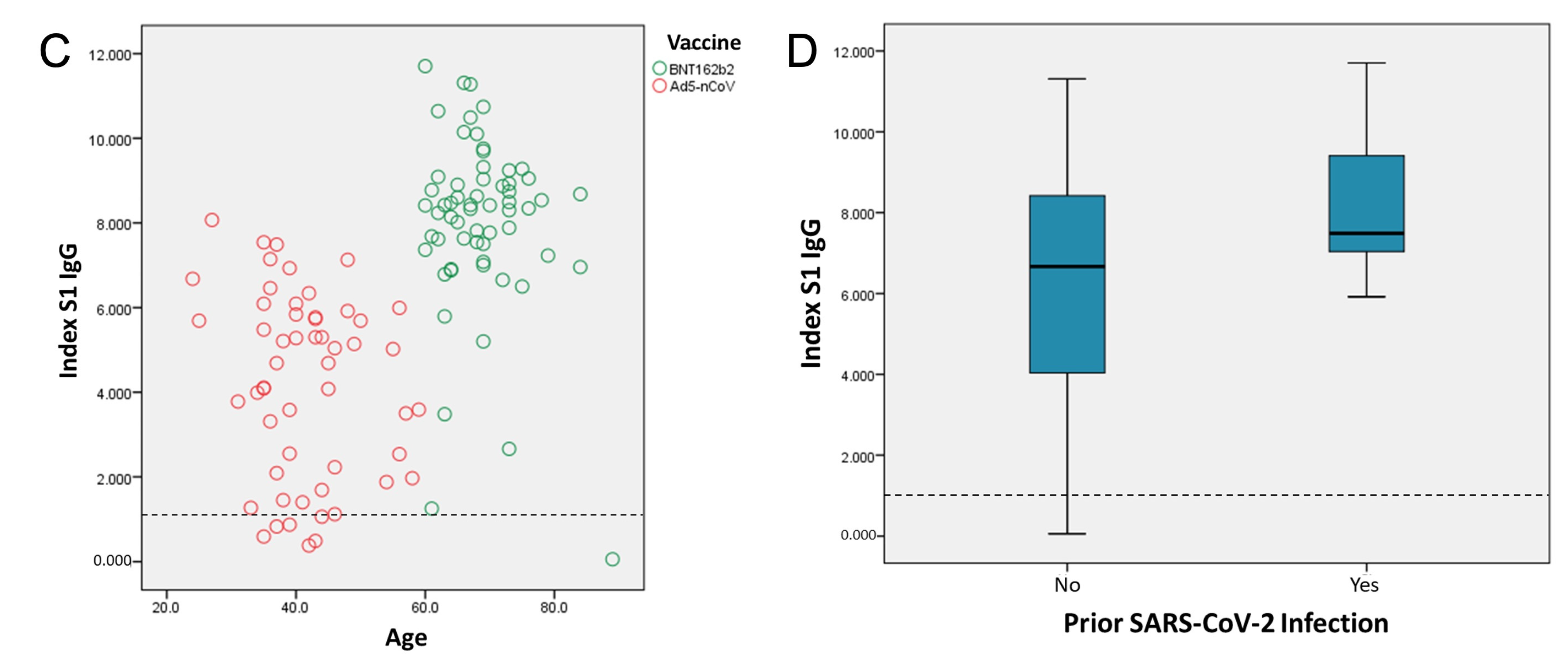
3.2. Detection of S1 IgG Antibodies
3.3. Side Effects of Vaccination
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garcia, L.F. Immune Response, Inflammation, and the Clinical Spectrum of COVID-19. Front. Immunol. 2020, 11, 1441. [Google Scholar] [CrossRef]
- WHO. WHO Coronavirus (COVID-19) Dashboard 2021. Available online: https://covid19.who.int/ (accessed on 25 June 2021).
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Gostin, L.O.; Hodge, J.G., Jr.; Bloom, B.R.; El-Mohandes, A.; Fielding, J.; Hotez, P.; Kurth, A.; Larson, H.J.; Orenstein, W.A.; Rabin, K.; et al. The public health crisis of underimmunisation: A global plan of action. Lancet Infect. Dis. 2020, 20, e11–e16. [Google Scholar] [CrossRef]
- Grigoryan, L.; Pulendran, B. The immunology of SARS-CoV-2 infections and vaccines. Semin. Immunol. 2020, 50, 101422. [Google Scholar] [CrossRef]
- Mulligan, M.J.; Lyke, K.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Raabe, V.; Bailey, R.; Swanson, K.A.; et al. Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults. Nature 2020, 586, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Sahin, U.; Muik, A.; Derhovanessian, E.; Vogler, I.; Kranz, L.M.; Vormehr, M.; Baum, A.; Pascal, K.; Quandt, J.; Maurus, D.; et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T cell responses. Nature 2020, 586, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based Covid-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef]
- Zhu, F.C.; Guan, X.H.; Li, Y.H.; Huang, J.Y.; Jiang, T.; Hou, L.H.; Li, J.X.; Yang, B.F.; Wang, L.; Wang, W.J.; et al. Immunogenicity and safety of a recombinant adenovirus type-5-vectored COVID-19 vaccine in healthy adults aged 18 years or older: A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet 2020, 396, 479–488. [Google Scholar] [CrossRef]
- Zhu, F.C.; Li, Y.H.; Guan, X.H.; Hou, L.H.; Wang, W.J.; Li, J.X.; Wu, S.P.; Wang, B.S.; Wang, Z.; Wang, L.; et al. Safety, tolerability, and immunogenicity of a recombinant adenovirus type-5 vectored COVID-19 vaccine: A dose-escalation, open-label, non-randomised, first-in-human trial. Lancet 2020, 395, 1845–1854. [Google Scholar] [CrossRef]
- Abu-Raddad, L.J.; Chemaitelly, H.; Butt, A.A.; National Study Group for COVID-19 Vaccination. Effectiveness of the BNT162b2 Covid-19 Vaccine against the B.1.1.7 and B.1.351 Variants. N. Engl. J. Med. 2021, 385, 187–189. [Google Scholar] [CrossRef]
- Chen, J.; Lu, H. New challenges to fighting COVID-19: Virus variants, potential vaccines, and development of antivirals. Biosci. Trends 2021, 15, 126–128. [Google Scholar] [CrossRef]
- Hall, V.J.; Foulkes, S.; Saei, A.; Andrews, N.; Oguti, B.; Charlett, A.; Wellington, E.; Stowe, J.; Gillson, N.; Atti, A.; et al. COVID-19 vaccine coverage in health-care workers in England and effectiveness of BNT162b2 mRNA vaccine against infection (SIREN): A prospective, multicentre, cohort study. Lancet 2021, 397, 1725–1735. [Google Scholar] [CrossRef]
- Keehner, J.; Horton, L.E.; Pfeffer, M.A.; Longhurst, C.A.; Schooley, R.T.; Currier, J.S.; Abeles, S.R.; Torriani, F.J. SARS-CoV-2 Infection after Vaccination in Health Care Workers in California. N. Engl. J. Med. 2021, 384, 1774–1775. [Google Scholar] [CrossRef]
- Salud, S.D. Estatus Regulatorio de las Vacunas Contra el virus SARS-CoV-2 en México 2021. Available online: http://vacunacovid.gob.mx/wordpress/informacion-de-la-vacuna/ (accessed on 26 June 2021).
- Salud, S.D. Calendario de Vacunación 2021. Available online: http://vacunacovid.gob.mx/wordpress/calendario-vacunacion/ (accessed on 26 June 2021).
- FDA. EUROIMMUN Anti-SARS-CoV-2 ELISA (IgG) EUA Letter of Authorization. Available online: https://www.fda.gov/media/137606/download (accessed on 27 January 2021).
- Elezkurtaj, S.; Greuel, S.; Ihlow, J.; Michaelis, E.G.; Bischoff, P.; Kunze, C.A.; Sinn, B.V.; Gerhold, M.; Hauptmann, K.; Ingold-Heppner, B.; et al. Causes of death and comorbidities in hospitalized patients with COVID-19. Sci. Rep. 2021, 11, 4263. [Google Scholar] [CrossRef]
- Salud, O.M.D.L. La OMS Incluye otra Vacuna Contra la COVID-19 en su Lista de uso en Emergencias y Publica Recomendaciones Provisionales en Materia de Políticas 2021. Available online: https://www.who.int/es/news/item/07-05-2021-who-lists-additional-covid-19-vaccine-for-emergency-use-and-issues-interim-policy-recommendations?fbclid=IwAR1adwWoRGoC83BU2oY5xVCCJiHYaBi89MbKtYGZKXLaKlgYMx7oxPNcIgA (accessed on 26 June 2021).
- Bradley, T.; Grundberg, E.; Selvarangan, R.; LeMaster, C.; Fraley, E.; Banerjee, D.; Belden, B.; Louiselle, D.; Nolte, N.; Biswell, R.; et al. Antibody Responses after a Single Dose of SARS-CoV-2 mRNA Vaccine. N. Engl. J. Med. 2021, 384, 1959–1961. [Google Scholar] [CrossRef]
- (CDC), Centros para el Control y la Prevencóin de Enfermedades. Visión General y Seguridad de la Vacuna Contra el COVID-19 de Pfizer-BioNTech 2021. Available online: https://espanol.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/Pfizer-BioNTech.html (accessed on 26 June 2021).
- Chandrashekar, A.; Liu, J.; Martinot, A.J.; McMahan, K.; Mercado, N.B.; Peter, L.; Tostanoski, L.H.; Yu, J.; Maliga, Z.; Nekorchuk, M.; et al. SARS-CoV-2 infection protects against rechallenge in rhesus macaques. Science 2020, 369, 812–817. [Google Scholar] [CrossRef]
- Deng, W.; Bao, L.; Liu, J.; Xiao, C.; Liu, J.; Xue, J.; Lv, Q.; Qi, F.; Gao, H.; Yu, P.; et al. Primary exposure to SARS-CoV-2 protects against reinfection in rhesus macaques. Science 2020, 369, 818–823. [Google Scholar] [CrossRef]
- Ángeles, C.M. Han Muerto 1183 Personas por Covid ya Vacunadas: Ssa: La Jornada. Available online: https://www.jornada.com.mx/notas/2021/06/24/politica/han-muerto-1-183-personas-por-covid-ya-vacunadas-ssa/ (accessed on 25 June 2021).
- CDC COVID-19 Vaccine Breakthrough Case Investigations Team. COVID-19 Vaccine Breakthrough Infections Reported to CDC-United States, January 1–April 30, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 792–793. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Harvala, H.; Mehew, J.; Robb, M.L.; Ijaz, S.; Dicks, S.; Patel, M.; Watkins, N.; Simmonds, P.; Brooks, T.; Johnson, R.; et al. Convalescent plasma treatment for SARS-CoV-2 infection: Analysis of the first 436 donors in England, 22 April to 12 May 2020. Euro Surveill. 2020, 25, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Valdivia, A.; Torres, I.; Latorre, V.; Frances-Gomez, C.; Albert, E.; Gozalbo-Rovira, R.; Alcaraz, M.J.; Buesa, J.; Rodriguez-Diaz, J.; Geller, R.; et al. Inference of SARS-CoV-2 spike-binding neutralizing antibody titers in sera from hospitalized COVID-19 patients by using commercial enzyme and chemiluminescent immunoassays. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 485–494. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Pan, Z.; Yue, S.; Yu, F.; Zhang, J.; Yang, Y.; Li, R.; Liu, B.; Yang, X.; Gao, L.; et al. Disease severity dictates SARS-CoV-2-specific neutralizing antibody responses in COVID-19. Signal Transduct. Target Ther. 2020, 5, 180. [Google Scholar] [CrossRef]
- Planas, D.; Veyer, D.; Baidaliuk, A.; Staropoli, I.; Guivel-Benhassine, F.; Rajah, M.M.; Planchais, C.; Porrot, F.; Robillard, N.; Puech, J.; et al. Reduced sensitivity of SARS-CoV-2 variant Delta to antibody neutralization. Nature 2021, 596, 276–280. [Google Scholar] [CrossRef]
- Figueiredo-Campos, P.; Blankenhaus, B.; Mota, C.; Gomes, A.; Serrano, M.; Ariotti, S.; Costa, C.; Nunes-Cabaco, H.; Mendes, A.M.; Gaspar, P.; et al. Seroprevalence of anti-SARS-CoV-2 antibodies in COVID-19 patients and healthy volunteers up to 6 months post disease onset. Eur. J. Immunol. 2020, 50, 2025–2040. [Google Scholar] [CrossRef]
- Mehew, J.; Johnson, R.; Roberts, D.; Harvala, H. Convalescent plasma for COVID-19: Male gender, older age and hospitalisation associated with high neutralising antibody levels, England, 22 April to 12 May 2020. Euro Surveill. 2020, 25, 2001754. [Google Scholar] [CrossRef]
- Bajaj, V.; Gadi, N.; Spihlman, A.P.; Wu, S.C.; Choi, C.H.; Moulton, V.R. Aging, Immunity, and COVID-19: How Age Influences the Host Immune Response to Coronavirus Infections? Front. Physiol. 2020, 11, 571416. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Vaccine | Total | ||||
|---|---|---|---|---|---|---|
| BNT162b2 | Ad5-nCoV | n = 115 | % | |||
| n | % | n | % | |||
| Sex | ||||||
| Male | 15 | 24.6 | 25 | 46.3 | 40 | 34.8 |
| Female | 46 | 75.4 | 29 | 53.7 | 75 | 65.2 |
| Comorbidities | ||||||
| Diabetes | 11 | 18.0 | 3 | 5.6 | 14 | 12.2 |
| Arterial hypertension | 24 | 39.3 | 2 | 3.7 | 26 | 22.6 |
| Cancer | 3 | 4.9 | 0 | 0 | 3 | 2.6 |
| Allergies | 13 | 21.3 | 11 | 20.4 | 24 | 20.9 |
| Chronic kidney disease | 1 | 1.6 | 0 | 0 | 1 | 0.9 |
| Chronic liver disease | 1 | 1.6 | 0 | 0 | 1 | 0.9 |
| Immunosuppression | 2 | 3.3 | 2 | 3.7 | 4 | 3.5 |
| Obesity and overweight | 15 | 24.6 | 12 | 22.2 | 27 | 23.5 |
| Other chronic disease | 11 | 18.0 | 3 | 5.6 | 14 | 12.2 |
| Characteristic | Vaccine | |||||||
|---|---|---|---|---|---|---|---|---|
| BNT162b2 (Second Dose) | Ad5-nCoV | |||||||
| Mean | SD | n = 61 | P | Mean | SD | n = 54 | P | |
| Comorbidities | ||||||||
| Diabetes | ||||||||
| Yes | 6.93 | 3.00 | 11 | 0.095 | 2.86 | 2.31 | 3 | 0.883 |
| No | 8.25 | 1.82 | 50 | 4.26 | 2.16 | 51 | ||
| Arterial hypertension | ||||||||
| Yes | 7.99 | 2.02 | 24 | 0.391 | 1.5 | 0.54 | 2 | 0.072 |
| No | 8.02 | 2.20 | 37 | 4.49 | 2.15 | 52 | ||
| Cancer | ||||||||
| Yes | 8.55 | 1.05 | 3 | 0.463 | 0 | 0 | 0 | - |
| No | 7.98 | 2.16 | 58 | 4.19 | 2.18 | 54 | ||
| Allergies | ||||||||
| Yes | 7.99 | 1.02 | 13 | 0.102 | 3.21 | 2.24 | 11 | 0.915 |
| No | 8.01 | 2.34 | 48 | 4.44 | 2.12 | 43 | ||
| Immunosuppression | ||||||||
| Yes | 5.06 | 5.38 | 2 | 0.018 | 3.1 | 2.89 | 2 | 0.819 |
| No | 8.11 | 1.96 | 59 | 4.23 | 2.17 | 52 | ||
| Obesity and overweight | ||||||||
| Yes | 8.36 | 1.31 | 15 | 0.169 | 3.85 | 2.38 | 12 | 0.44 |
| No | 7.89 | 2.32 | 46 | 4.29 | 2.14 | 42 | ||
| Sex | ||||||||
| Female | 8.37 | 1.55 | 46 | 0.010 | 4.53 | 1.84 | 29 | 0.027 |
| Male | 6.90 | 3.11 | 15 | 3.79 | 2.49 | 25 | ||
| Side Effect | Vaccine | |||||
|---|---|---|---|---|---|---|
| BNT162b2 | Ad5-nCoV | |||||
| First Dose | Second Dose | Single-Dose | ||||
| n | % | n | % | n | % | |
| Injection site pain | 39 | 63.9 | 36 | 59.0 | 26 | 48.1 |
| Redness | 1 | 1.6 | 5 | 8.2 | 2 | 3.7 |
| Swelling | 0 | 0 | 2 | 3.3 | 2 | 3.7 |
| Fatigue | 15 | 24.6 | 20 | 32.8 | 27 | 50.0 |
| Fever | 0 | 0 | 2 | 3.3 | 9 | 16.7 |
| Nausea | 0 | 0 | 3 | 4.9 | 4 | 7.4 |
| Chills | 1 | 1.6 | 2 | 3.3 | 7 | 13.0 |
| Headache | 5 | 8.2 | 4 | 6.5 | 14 | 25.9 |
| Myalgia | 5 | 8.2 | 11 | 18.0 | 19 | 35.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guzmán-Martínez, O.; Guardado, K.; de Guevara, E.L.; Navarro, S.; Hernández, C.; Zenteno-Cuevas, R.; Montero, H. IgG Antibodies Generation and Side Effects Caused by Ad5-nCoV Vaccine (CanSino Biologics) and BNT162b2 Vaccine (Pfizer/BioNTech) among Mexican Population. Vaccines 2021, 9, 999. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9090999
Guzmán-Martínez O, Guardado K, de Guevara EL, Navarro S, Hernández C, Zenteno-Cuevas R, Montero H. IgG Antibodies Generation and Side Effects Caused by Ad5-nCoV Vaccine (CanSino Biologics) and BNT162b2 Vaccine (Pfizer/BioNTech) among Mexican Population. Vaccines. 2021; 9(9):999. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9090999
Chicago/Turabian StyleGuzmán-Martínez, Oscar, Kathia Guardado, Elsa Ladrón de Guevara, Saturnino Navarro, Crescencio Hernández, Roberto Zenteno-Cuevas, and Hilda Montero. 2021. "IgG Antibodies Generation and Side Effects Caused by Ad5-nCoV Vaccine (CanSino Biologics) and BNT162b2 Vaccine (Pfizer/BioNTech) among Mexican Population" Vaccines 9, no. 9: 999. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9090999