
A Scoping Review to Find Out Worldwide COVID-19 Vaccine Hesitancy and Its Underlying Determinants


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.1.1. Search Sources
2.1.2. Search Terms
2.2. Study Eligibility Criteria
2.3. Study Selection
2.4. Data Extraction and Data Synthesis
3. Results
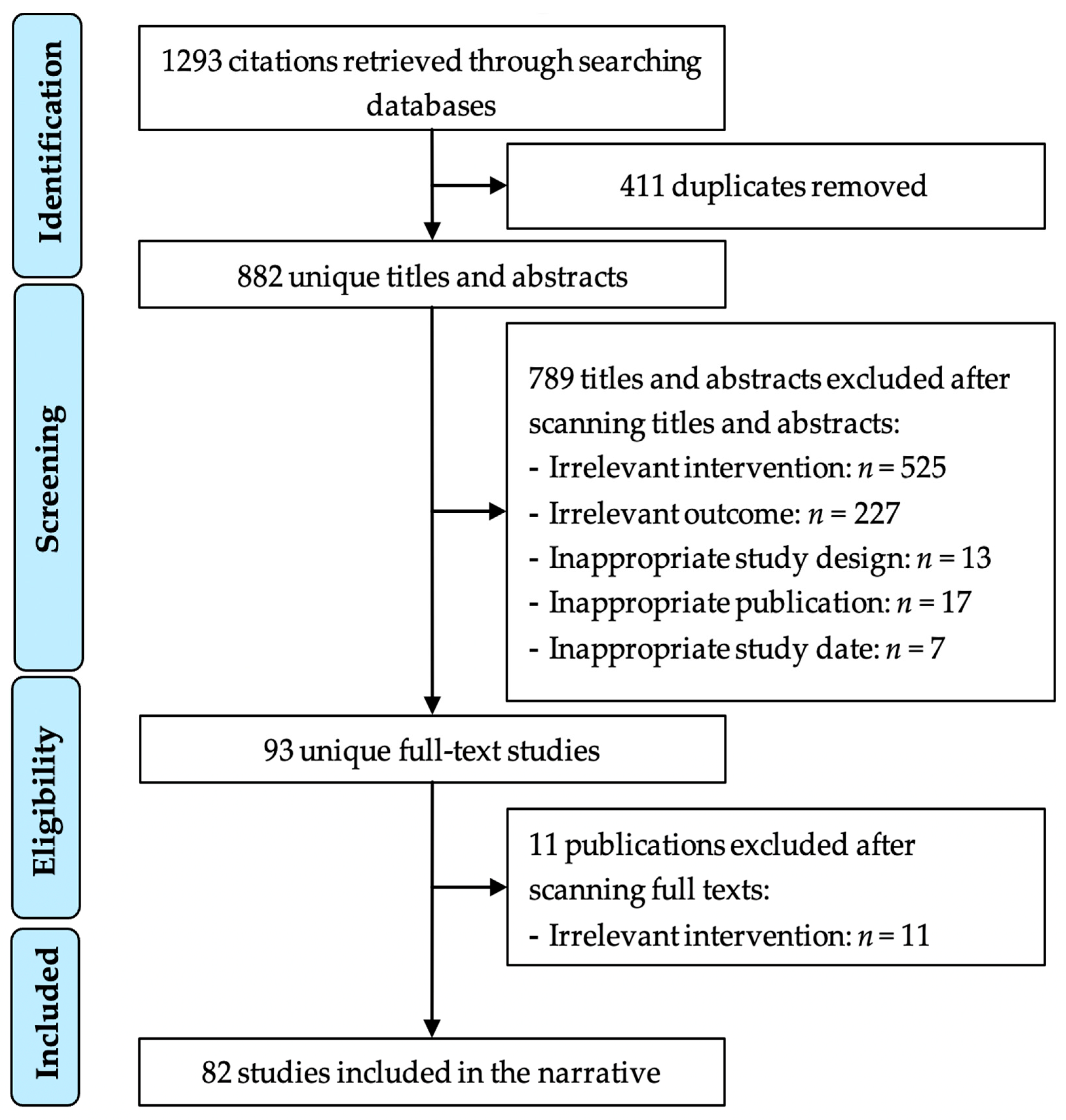
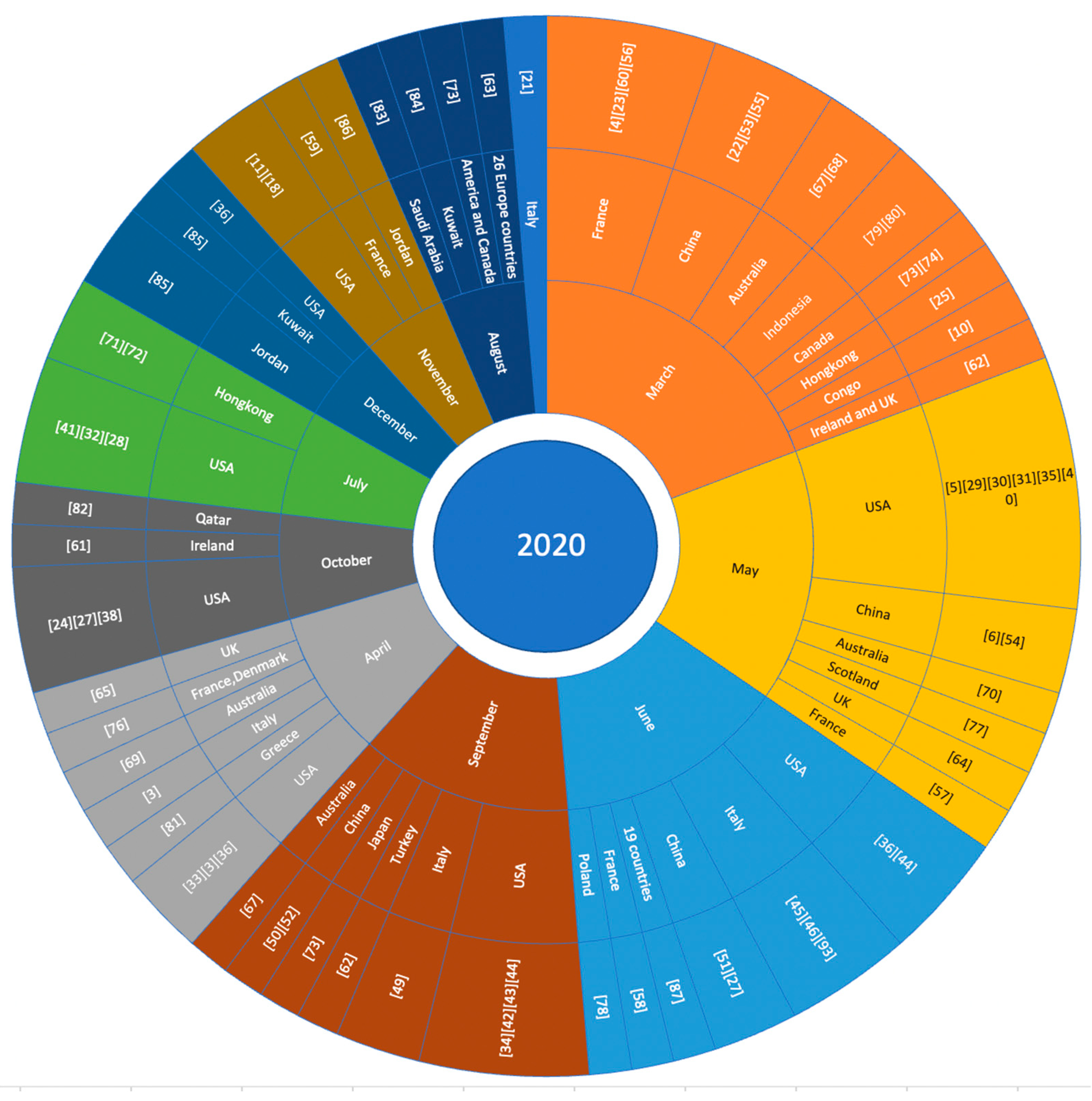
3.1. Search Results
3.2. Characteristics of Included Studies
3.2.1. Summary of Included Studies
3.2.2. Measurement Tools
3.3. Worldwide COVID-19 Vaccine Acceptance and Hesitancy Rate
3.4. Determinants of COVID-19 Vaccine Hesitancy
3.5. Vaccine Hesitancy among Ethnic Minorities
4. Discussion
4.1. Principal Findings
4.2. Strengths and Limitations
4.2.1. Strengths
4.2.2. Limitations
4.3. Practical and Research Implications
4.3.1. Practical Implications
4.3.2. Research Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Report of the Sage Working Group. October 2014, p. 64. Available online: https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf (accessed on 22 February 2021).
- Randolph, H.E.; Barreiro, L.B. Herd immunity: Understanding COVID-19. Immunity 2020, 52, 737–741. [Google Scholar] [CrossRef]
- Biasio, L.R.; Bonaccorsi, G.; Lorini, C.; Pecorelli, S. Assessing COVID-19 vaccine literacy: A preliminary online survey. Hum. Vaccines Immunother. 2021, 17, 1304–1312. [Google Scholar] [CrossRef] [PubMed]
- Hacquin, A.-S.; Altay, S.; de Araujo, E.; Chevallier, C.; Mercier, H. Sharp Rise in Vaccine Hesitancy in a Large and Representative Sample of the French Population: Reasons for Vaccine Hesitancy. 2020. Available online: http://0-dx-doi-org.brum.beds.ac.uk/10.31234/osf.io/r8h6z (accessed on 22 February 2021).
- Callaghan, T.; Moghtaderi, A.; Lueck, J.A.; Hotez, P.; Strych, U.; Dor, A.; Fowler, E.F.; Motta, M. Correlates and disparities of intention to vaccinate against COVID-19. Soc. Sci. Med. 2021, 272, 113638. [Google Scholar] [CrossRef] [PubMed]
- Dong, D.; Xu, R.H.; Wong, E.L.; Hung, C.; Feng, D.; Feng, Z.; Yeoh, E.; Wong, S.Y. Public preference for COVID-19 vaccines in China: A discrete choice experiment. Health Expect 2020, 23, 1543–1578. [Google Scholar] [CrossRef]
- Chevallier, C.; Hacquin, A.-S.; Mercier, H. COVID-19 vaccine hesitancy: Shortening the last mile. Trends Cogn. Sci. 2021, 25, 331–333. [Google Scholar] [CrossRef]
- Daley, M.F.; Narwaney, K.J.; Shoup, J.A.; Wagner, N.M.; Glanz, J.M. Addressing parents’ vaccine concerns: A randomized trial of a social media intervention. Am. J. Prev. Med. 2018, 55, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Vivion, M.; MacDonald, N.E. Vaccine hesitancy, vaccine refusal and the anti-vaccine movement: Influence, impact and implications. Expert Rev. Vaccines 2015, 14, 99–117. [Google Scholar] [CrossRef] [PubMed]
- Kabamba Nzaji, M.; Kabamba Ngombe, L.; Ngoie Mwamba, G.; Banza Ndala, D.B.; Mbidi Miema, J.; Lungoyo, C.L.; Mwimba, B.L.; Bene, A.C.M.; Musenga, E.M. Acceptability of vaccination against COVID-19 among healthcare workers in the democratic republic of the Congo. Pragmatic Obs. Res. 2020, 11, 103–109. [Google Scholar] [CrossRef]
- Unroe, K.T.; Evans, R.; Weaver, L.; Rusyniak, D.; Blackburn, J. Willingness of long-term care staff to receive a COVID-19 vaccine: A single state survey. J. Am. Geriatr. Soc. 2021, 69, 593–599. [Google Scholar] [CrossRef]
- Webster, J.; Watson, R.T. Analyzing the Past to Prepare for the Future: Writing a Literature Review. MIS Q. 2002, 26, xiii–xxiii. [Google Scholar]
- Sucharew, H.; Macaluso, M. Methods for research evidence synthesis: The scoping review approach. J. Hosp. Med. 2019, 14, 416–418. [Google Scholar] [CrossRef] [Green Version]
- Rowley, J.; Slack, F. Conducting a literature review. Manag. Res. News 2004, 27, 31–39. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abd-Alrazaq, A.A.; Alajlani, M.; Alalwan, A.; Bewick, B.M.; Gardner, P.; Househ, M. An overview of the features of chatbots in mental health: A scoping review. Int. J. Med. Inform. 2019, 132, 103978. [Google Scholar] [CrossRef] [PubMed]
- Abd-Alrazaq, A.A.; Alajlani, M.; Ali, N.; Denecke, K.; Bewick, B.M.; Househ, M. Perceptions and opinions of patients about mental health chatbots: Scoping review. J. Med. Internet Res. 2021, 23, e17828. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Shahrabani, S.; Benzion, U.; Yom Din, G. Factors affecting nurses’ decision to get the flu vaccine. Eur. J. Health Econ. 2009, 10, 227–231. [Google Scholar] [CrossRef]
- Barello, S.; Palamenghi, L.; Graffigna, G. Looking inside the ‘black box’ of vaccine hesitancy: Unlocking the effect of psychological attitudes and beliefs on COVID-19 vaccine acceptance and implications for public health communication. Psychol. Med. 2021, 1–2. [Google Scholar] [CrossRef]
- Barello, S.; Nania, T.; Dellafiore, F.; Graffigna, G.; Caruso, R. ‘Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur. J. Epidemiol. 2020, 35, 781–783. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Barrière, J.; Gal, J.; Hoch, B.; Cassuto, O.; Leysalle, A.; Chamorey, E.; Borchiellini, D. Acceptance of SARS-CoV-2 vaccination among French patients with cancer: A cross-sectional survey. Ann. Oncol. 2021, 32, 673–674. [Google Scholar] [CrossRef]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef]
- Wong, M.C.; Wong, E.L.; Huang, J.; Cheung, A.W.; Law, K.; Chong, M.K.; Ng, R.W.; Lai, C.K.; Boon, S.S.; Lau, J.T.; et al. Acceptance of the COVID-19 vaccine based on the health belief model: A population-based survey in Hong Kong. Vaccine 2021, 39, 1148–1156. [Google Scholar] [CrossRef]
- Qiao, S.; Tam, C.C.; Li, X. Risk exposures, risk perceptions, negative attitudes toward general vaccination, and COVID-19 vaccine acceptance among college students in South Carolina. Am. J. Health Promot. 2021, 1–25. [Google Scholar] [CrossRef]
- Ruiz, J.B.; Bell, R.A. Predictors of intention to vaccinate against COVID-19: Results of a nationwide survey. Vaccine 2021, 39, 1080–1086. [Google Scholar] [CrossRef] [PubMed]
- Kreps, S.; Prasad, S.; Brownstein, J.S.; Hswen, Y.; Garibaldi, B.T.; Zhang, B.; Kriner, D.L. Factors associated with US adults’ likelihood of accepting COVID-19 vaccination. JAMA Netw. Open 2020, 3, e2025594. [Google Scholar] [CrossRef] [PubMed]
- Caban-Martinez, A.J.; Silvera, C.A.; Santiago, K.M.; Louzado-Feliciano, P.; Burgess, J.L.; Smith, D.L.; Jahnke, S.; Horn, G.P.; Graber, J.M. COVID-19 vaccine acceptability among us firefighters and emergency medical services workers. J. Occup. Environ. Med. 2021, 63, 369–373. [Google Scholar] [CrossRef] [PubMed]
- Shekhar, R.; Sheikh, A.; Upadhyay, S.; Singh, M.; Kottewar, S.; Mir, H.; Barrett, E.; Pal, S. COVID-19 vaccine acceptance among health care workers in the United States. Vaccines 2021, 9, 119. [Google Scholar] [CrossRef] [PubMed]
- Latkin, C.A.; Dayton, L.; Yi, G.; Colon, B.; Kong, X. Mask usage, social distancing, racial, and gender correlates of COVID-19 vaccine intentions among adults in the US. PLoS ONE 2021, 16, e0246970. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes toward a potential SARS-CoV-2 vaccine: A survey of US adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Bogart, L.M.; Ojikutu, B.O.; Tyagi, K.; Klein, D.J.; Mutchler, M.G.; Dong, L.; Lawrence, S.J.; Thomas, D.R.; Kellman, S. COVID-19 related medical mistrust, health impacts, and potential vaccine hesitancy among black americans living with HIV. JAIDS J. Acquir. Immune Defic. Syndr. 2021, 86, 200–207. [Google Scholar] [CrossRef]
- Ehde, D.M.; Roberts, M.K.; Herring, T.E.; Alschuler, K.N. Willingness to obtain COVID-19 vaccination in adults with multiple sclerosis in the United States. Mult. Scler. Relat. Disord. 2021, 49, 102788. [Google Scholar] [CrossRef]
- Gadoth, M.A.; Halbrook, M.M.; Martin-Blais, R.; Gray, A.; Tobin, N.H.; Ferbas, K.G.; Aldrovandi, M.G.M.; Rimoin, M.A.W. Cross-sectional assessment of COVID-19 vaccine acceptance among health care workers in Los Angeles. Ann. Intern. Med. 2021. [Google Scholar] [CrossRef]
- Thunstrom, L.; Ashworth, M.; Finnoff, D.; Newbold, S. Hesitancy towards a COVID-19 Vaccine and Prospects for Herd Immunity. SSRN Electron. Available online: https://ssrn.com/abstract=3593098 or http://0-dx-doi-org.brum.beds.ac.uk/10.2139/ssrn.3593098 (accessed on 30 June 2020).
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 Vaccination hesitancy in the United States: A rapid national assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef]
- Mercadante, A.R.; Law, A.V. Since January 2020 Elsevier has created a COVID-19 resource centre with free information in English and Mandarin on the novel coronavirus COVID- 19 The COVID-19 resource centre is hosted on Elsevier Connect the company’s public news and information. Diabetes Metab. Syndr. 2020, 14, 337–339. [Google Scholar]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef] [PubMed]
- Guidry, J.P.; Laestadius, L.I.; Vraga, E.K.; Miller, C.A.; Perrin, P.B.; Burton, C.W.; Ryan, M.; Fuemmeler, B.F.; Carlyle, K.E. Willingness to get the COVID-19 vaccine with and without emergency use authorization. Am. J. Infect. Control. 2021, 49, 137–142. [Google Scholar] [CrossRef]
- Pogue, K.; Jensen, J.L.; Stancil, C.K.; Ferguson, D.G.; Hughes, S.J.; Mello, E.J.; Burgess, R.; Berges, B.K.; Quaye, A.; Poole, B.D. Influences on attitudes regarding potential COVID-19 vaccination in the United States. Vaccines 2020, 8, 582. [Google Scholar] [CrossRef] [PubMed]
- Largent, E.A.; Persad, G.; Sangenito, S.; Glickman, A.; Boyle, C.; Emanuel, E.J. US public attitudes toward COVID-19 vaccine mandates. JAMA Netw. Open 2020, 3, e2033324. [Google Scholar] [CrossRef]
- Karlsson, L.C.; Soveri, A.; Lewandowsky, S.; Karlsson, L.; Karlsson, H.; Nolvi, S.; Karukivi, M.; Lindfelt, M.; Antfolk, J. Fearing the disease or the vaccine: The case of COVID-19. Personal. Individ. Differ. 2021, 172, 110590. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Thomas, K.; Shah, M.D.; Vizueta, N.; Cui, Y.; Vangala, S.; Kapteyn, A. National trends in the US public’s likelihood of getting a COVID-19 vaccine—April 1 to December 8, 2020. JAMA 2021, 325, 396. [Google Scholar] [CrossRef]
- Graffigna, G.; Palamenghi, L.; Boccia, S.; Barello, S. Relationship between citizens’ health engagement and intention to take the COVID-19 vaccine in Italy: A mediation analysis. Vaccines 2020, 8, 576. [Google Scholar] [CrossRef]
- Caserotti, M.; Girardi, P.; Rubaltelli, E.; Tasso, A.; Lotto, L.; Gavaruzzi, T. Associations of COVID-19 risk perception with vaccine hesitancy over time for Italian residents. Soc. Sci. Med. 2021, 272, 113688. [Google Scholar] [CrossRef]
- Palamenghi, L.; Barello, S.; Boccia, S.; Graffigna, G. Mistrust in biomedical research and vaccine hesitancy: The forefront challenge in the battle against COVID-19 in Italy. Eur. J. Epidemiol. 2020, 35, 785–788. [Google Scholar] [CrossRef]
- La Vecchia, C.; Negri, E.; Alicandro, G.; Scarpino, V. Attitudes towards influenza vaccine and a potential COVID-19 vaccine in Italy and differences across occupational groups, September 2020. Med. Lav 2020, 111, 445–448. [Google Scholar] [PubMed]
- Prati, G. Intention to receive a vaccine against SARS-CoV-2 in Italy and its association with trust, worry and beliefs about the origin of the virus. Health Educ. Res. 2020, 35, 505–511. [Google Scholar] [CrossRef]
- Fu, C.; Wei, Z.; Pei, S.; Li, S.; Sun, X.; Liu, P. Acceptance and preference for COVID-19 vaccination in healthcare workers (HCWs). Medrxiv 2020, 2962, 548. [Google Scholar] [CrossRef] [Green Version]
- Zhang, K.C.; Fang, Y.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.Q.; Zhou, X.; Wang, Z. Parental acceptability of COVID-19 vaccination for children under the age of 18 years: Cross-sectional online survey. JMIR Pediatr. Parent. 2020, 3, e24827. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Luo, X.; Ma, Z.F. Willingness of the general population to accept and pay for COVID-19 vaccination during the early stages of COVID-19 pandemic: A nationally representative survey in mainland China. Hum. Vaccines Immunother. 2021, 17, 1622–1627. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Li, Y.; Chen, J.; Wen, Z.; Feng, F.; Zou, H.; Fu, C.; Chen, L.; Shu, Y.; Sun, C. An online survey of the attitude and willingness of Chinese adults to receive COVID-19 vaccination. Hum. Vaccines Immunother. 2021, 17, 2279–2288. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Li, X.; Su, X.; Xiao, T.; Wang, Y.; Hu, P.; Li, H.; Guan, J.; Tian, H.; Wang, P.; et al. A study on willingness and influencing factors to receive COVID-19 vaccination among Qingdao residents. Hum. Vaccines Immunother. 2021, 17, 408–413. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Chan, E.Y.Y.; Yeoh, E.K.; Wong, S.Y.S. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine 2020, 38, 7049–7056. [Google Scholar] [CrossRef]
- Bertin, P.; Nera, K.; Delouvée, S. Conspiracy beliefs, rejection of vaccination, and support for hydroxychloroquine: A conceptual replication-extension in the COVID-19 pandemic context. Front. Psychol. 2020, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Schwarzinger, M.; Watson, V.; Arwidson, P.; Alla, F.; Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Health 2021, 6, e210–e221. [Google Scholar] [CrossRef]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef]
- Gagneux-Brunon, A.; Detoc, M.; Bruel, S.; Tardy, B.; Rozaire, O.; Frappe, P.; Botelho-Nevers, E. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J. Hosp. Infect. 2021, 108, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Verger, P.; Scronias, D.; Dauby, N.; Adedzi, K.A.; Gobert, C.; Bergeat, M.; Gagneur, A.; Dubé, E. Attitudes of healthcare workers towards COVID-19 vaccination: A survey in France and French-speaking parts of Belgium and Canada, 2020. Eurosurveillance 2021, 26, 2002047. [Google Scholar] [CrossRef]
- Murphy, J.J.; Vallieres, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hatman, T.K.; McKay, R.; Bennett, K.M.; Mason, L.; Miller, J.G.; et al. Preparing for a COVID-19 Vaccine: Identifying and Psychologically Profiling Those Who Are Vaccine Hesitant or Resistant in Two General Population Samples. 2020. Available online: http://0-dx-doi-org.brum.beds.ac.uk/10.31234/osf.io/8dtnq (accessed on 21 February 2021).
- Salali, G.D.; Uysal, M.S. COVID-19 vaccine hesitancy is associated with beliefs on the origin of the novel coronavirus in the UK and Turkey. Psychol. Med. 2020, 1–3, online ahead of print. [Google Scholar] [CrossRef]
- Marcec, R.; Majta, M.; Likic, R. Will vaccination refusal prolong the war on SARS-CoV-2? Postgrad. Med. J. 2020, 97, 143–149. [Google Scholar] [CrossRef]
- Williams, L.; Gallant, A.J.; Rasmussen, S.; Nicholls, L.A.B.; Cogan, N.; Deakin, K.; Young, D.; Flowers, P. Towards intervention development to increase the uptake of COVID-19 vaccination among those at high risk: Outlining evidence-based and theoretically informed future intervention content. Br. J. Health Psychol. 2020, 25, 1039–1054. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: A multi-methods study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S.; et al. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2020, 1–15. [Google Scholar] [CrossRef]
- Borriello, A.; Master, D.; Pellegrini, A.; Rose, J.M. Preferences for a COVID-19 vaccine in Australia. Vaccine 2021, 39, 473–479. [Google Scholar] [CrossRef]
- Attwell, K.; Lake, J.; Sneddon, J.; Gerrans, P.; Blyth, C.; Lee, J. Converting the maybes: Crucial for a successful COVID-19 vaccination strategy. PLoS ONE 2021, 16, e0245907. [Google Scholar] [CrossRef]
- Alley, S.J.; Stanton, R.; Browne, M.; To, Q.G.; Khalesi, S.; Williams, S.L.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. As the pandemic progresses, how does willingness to vaccinate against COVID-19 evolve? Int. J. Environ. Res. Public Health 2021, 18, 797. [Google Scholar] [CrossRef]
- Seale, H.; Heywood, A.E.; Leask, J.; Sheel, M.; Durrheim, D.N.; Bolsewicz, K.; Kaur, R. Examining Australian public perceptions and behaviors towards a future COVID-19 vaccine. BMC Infect. Dis. 2021, 21, 1–9. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.-K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 vaccination during the COVID-19 pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Groenewoud, R.; Rachor, G.S.; Asmundson, G.J.G. A proactive approach for managing COVID-19: The importance of understanding the motivational roots of vaccination hesitancy for SARS-CoV2. Front. Psychol. 2020, 11, 575950. [Google Scholar] [CrossRef] [PubMed]
- Kumar, D.; Chandra, R.; Mathur, M.; Samdariya, S.; Kapoor, N. Vaccine hesitancy: Understanding better to address better. Isr. J. Health Policy Res. 2016, 5, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kose, S.; Mandiracioglu, A.; Sahin, S.; Kaynar, T.; Karbus, O.; Ozbel, Y. Vaccine hesitancy of the COVID-19 by health care personnel. Int. J. Clin. Pr. 2021, 75, 17–20. [Google Scholar] [CrossRef]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; Van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef]
- Williams, L.; Flowers, P.; McLeod, J.; Young, D.; Rollins, L.; The CATALYST Project Team. Social patterning and stability of intention to accept a COVID-19 vaccine in Scotland: Will those most at risk accept a vaccine? Vaccines 2021, 9, 17. [Google Scholar] [CrossRef] [PubMed]
- Feleszko, W.; Lewulis, P.; Czarnecki, A.; Waszkiewicz, P. Flattening the curve of COVID-19 vaccine rejection—An international overview. Vaccines 2021, 9, 44. [Google Scholar] [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 Vaccine in Southeast Asia: A cross-sectional study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Vo, T.Q.; et al. Willingness-to-pay for a COVID-19 vaccine and its associated determinants in Indonesia. Hum. Vaccines Immunother. 2020, 16, 3074–3080. [Google Scholar] [CrossRef]
- Kourlaba, G.; Kourkouni, E.; Maistreli, S.; Tsopela, C.-G.; Molocha, N.-M.; Triantafyllou, C.; Koniordou, M.; Kopsidas, I.; Chorianopoulou, E.; Maroudi-Manta, S.; et al. Willingness of Greek general population to get a COVID-19 vaccine. Glob. Health Res. Policy 2021, 6, 1–10. [Google Scholar] [CrossRef]
- Alabdulla, M.; Reagu, S.M.; Al-Khal, A.; Elzain, M.; Jones, R.M. COVID-19 vaccine hesitancy and attitudes in Qatar: A national cross-sectional survey of a migrant-majority population. Influenza Other Respir. Viruses 2021, 15, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Al-Mohaithef, M.; Padhi, B.K. Determinants of COVID-19 vaccine acceptance in Saudi Arabia: A web-based national survey. J. Multidiscotlandip. Health 2020, 13, 1657–1663. [Google Scholar] [CrossRef] [PubMed]
- Alqudeimat, Y.; Alenezi, D.; AlHajri, B.; Alfouzan, H.; Almokhaizeem, Z.; Altamimi, S.; Almansouri, W.; Alzalzalah, S.; Ziyab, A. Acceptance of a COVID-19 Vaccine and its related determinants among the general adult population in Kuwait. Med. Princ. Pr. 2021, 10, 2052–2061. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High rates of COVID-19 vaccine hesitancy and its association with conspiracy beliefs: A study in Jordan and Kuwait among other Arab countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- El-Elimat, T.; AbuAlSamen, M.M.; Almomani, B.A.; Al-Sawalha, N.A.; Alali, F.Q. Acceptance and attitudes toward COVID-19 vaccines: A cross-sectional study from Jordan. PLoS ONE 2021, 16, e0250555. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Scotlandott, C.R.; Adam, P.; Lawrence, O.G.; Heidi, J.L.; Kenneth, R.; Spencer, K.; El-Mohandes, A. Author Correction: A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021. [Google Scholar] [CrossRef]
- Kane, M. Discotlandussion. Vaccine 1998, 16, S73–S75. [Google Scholar] [CrossRef]
- Peretti-Watel, P.; Seror, V.; Cortaredona, S.; Launay, O.; Raude, J.; Verger, P.; Fressard, L.; Beck, F.; Legleye, S.; L’Haridon, O.; et al. A future vaccination campaign against COVID-19 at risk of vaccine hesitancy and politicisation. Lancet Infect. Dis. 2020, 20, 769–770. [Google Scholar] [CrossRef]
- Kochhar, S.; Salmon, D.A. Planning for COVID-19 vaccines safety surveillance. Vaccine 2020, 38, 6194–6198. [Google Scholar] [CrossRef]
- Goldman, R.D.; Yan, T.D.; Seiler, M.; Cotanda, C.P.; Brown, J.C.; Klein, E.J.; Hoeffe, J.; Gelernter, R.; Hall, J.E.; Davis, A.L.; et al. Caregiver willingness to vaccinate their children against COVID-19: Cross sectional survey. Vaccine 2020, 38, 7668–7673. [Google Scholar] [CrossRef]
- Olagoke, A.A.; Olagoke, O.; Hughes, A.M. Intention to vaccinate against the novel 2019 Coronavirus disease: The role of health locus of control and religiosity. J. Relig. Health 2021, 60, 65–80. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. COVID-19 vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Razai, M.S.; Osama, T.; McKechnie, D.G.J.; Majeed, A. Covid-19 vaccine hesitancy among ethnic minority groups. BMJ 2021, 372, n513. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Dobalian, A.; Ward, K.D. COVID-19 Vaccine hesitancy and its determinants among adults with a history of tobacco or marijuana use. J. Community Health 2021, 1–9. [Google Scholar] [CrossRef]
- Hotez, P.J. Anti-science extremism in America: Escalating and globalizing. Microbes Infect. 2020, 22, 505–507. [Google Scholar] [CrossRef] [PubMed]
- Sherman, S.M.; Smith, L.E.; Sim, J.; Amlôt, R.; Cutts, M.; Dasch, H.; Rubin, G.J.; Sevdalis, N. COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum. Vaccines Immunother. 2021, 17, 1612–1621. [Google Scholar] [CrossRef]
- Joshi, M.A.; Kaur, R.; Kaur, A.; Grover, D.N.; El-Mohandes, A. Predictors of COVID-19 Vaccine Acceptance, Intention, and Hesitancy: A Scoping Review. Front. Public Health 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Armand, A.; et al. COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Aw, J.; Seng, J.J.; Seah, S.S.; Low, L.L. COVID-19 Vaccine Hesitancy—A Scoping Review of Literature in High-Income Countries. Vaccines 2021, 9, 900. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, C.; Langley, J.; Steenbeek, A.; Taylor, B.; Kennie-Kaulbach, N.; Grantmyre, H.; Isenor, J. A Behavioral analysis of nurses’ and pharmacists’ role in addressing vaccine hesitancy: Scoping review. Nat. Med. 2021, 9, 1385–1394. [Google Scholar] [CrossRef]
- Roghani, A. The Influence of Covid-19 Vaccine on Daily Cases, Hospitalization, and Death Rate in Tennessee: A Case Study in the United States. Available online: https://www.medrxiv.org/content/10.1101/2021.03.16.21253767v1 (accessed on 22 February 2021).
- Khuroo, M.S.; Khuroo, M.S.; Sofi, A.A.; Khuroo, N.S. COVID-19 vaccines: A race against time in the middle of death and devastation! J. Clin. Exp. Hepatol. 2020, 10, 610–621. [Google Scholar] [CrossRef]
- Haghpanah, F.; Lin, G.; Levin, S.A.; Klein, E. Analysis of the potential impact of durability, timing, and transmission blocking of COVID-19 vaccine on morbidity and mortality. EClinicalMedicine 2021, 35, 100863. [Google Scholar] [CrossRef]
- Riad, A.; Pokorná, A.; Attia, S.; Klugarová, J.; Koščík, M.; Klugar, M. Prevalence of COVID-19 vaccine side effects among healthcare workers in the Czech Republic. J. Clin. Med. 2021, 10, 1428. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Criteria | Specified Criteria |
|---|---|
| Inclusion |
|
| Exclusion |
|
| Country | No. of Studies | Target Population | ||||
|---|---|---|---|---|---|---|
| BV (79) | AV (2) | General Population | Students | Health Workers | People at High Risk | |
| United States | 23 | 0 | 16 | 2 | 3 | 2 |
| Italy | 10 | 0 | 7 | 1 | 1 | 1 |
| China | 8 | 0 | 7 | 0 | 1 | 0 |
| France | 6 | 1 | 5 | 0 | 2 | 1 |
| United Kingdom | 6 | 0 | 5 | 0 | 0 | 1 |
| Australia | 4 | 0 | 4 | 0 | 0 | 0 |
| Hong Kong | 3 | 0 | 1 | 1 | 1 | 0 |
| Canada | 2 | 0 | 1 | 0 | 1 | 0 |
| Turkey | 2 | 0 | 0 | 1 | 1 | 0 |
| Ireland | 1 | 0 | 0 | 0 | 0 | 1 |
| Poland | 1 | 0 | 1 | 0 | 0 | 0 |
| Japan | 1 | 0 | 1 | 0 | 0 | 0 |
| Saudi Arabia | 1 | 0 | 1 | 0 | 0 | 0 |
| Qatar | 1 | 0 | 1 | 0 | 0 | 0 |
| Oman | 1 | 0 | 1 | 0 | 0 | 0 |
| Jordan | 1 | 1 | 1 | 0 | 0 | 0 |
| Kuwait | 1 | 0 | 1 | 0 | 0 | 0 |
| Congo | 1 | 0 | 1 | 0 | 0 | 0 |
| Greece | 1 | 0 | 1 | 0 | 0 | 0 |
| Europe (26 Countries) | 1 | 0 | 1 | 0 | 0 | 0 |
| World (19 Countries) | 1 | 0 | 1 | 0 | 0 | 0 |
| Country | Type of Population | Population Size | Vaccine Uptake (%) | Vaccine Hesitancy (%) | Vaccine Refusal (%) |
|---|---|---|---|---|---|
| USA | GP [28] | N = 1971, F = 51% | 79 | 21 | N/S |
| HCW [11] | N = 8243, F = 87% | 45 | 24 | N/S | |
| Student [26] | N = 1062, F = 79.8% | 60.6 | 15.1 | 24.3 | |
| CRC [33] | N = 101, M = 77% | N/S | 34 | N/S | |
| Italy | GP [3] | N = 1004, M = 49.1% | 58.6 | 26 | 15 |
| HCW [47] | N = 968 | 83.2 | 16.3 | N/S | |
| Student [21] | N = 735, F = 79.6% | 86.1 | 13.9 | N/S | |
| CRC [46] | N = 2267, F = 69% | 86 | 13 | N/S | |
| China | GP [6] | N = 1236, F = 51.1% | 80 | 10.9 | 8.1 |
| HCW [50] | N = 541, F = 60% | 76.4 | 20 | 3.6 | |
| France | GP [56] | N = 4027 | 48.8 | 47.9 | N/S |
| HCW [59] | N = 2047, F = 75% | 48.6 | 23 | N/S | |
| CRC [23] | N = 999, F = 56.1% | 53.7 | N/S | N/S | |
| UK | GP [65] | N = 3667, M = 50.1 | 71.7 | 16.6 | 11.7 |
| CRC [63] | N = 527, F = 57% | 86 | N/S | N/S | |
| Australia | GP [69] | N = 1420 | 69 | 10 | N/S |
| Hong Kong | Student [72] | N = 1200, F = 71.4 | N/S | 40.4 | 17.4 |
| GP [25] | N = 1200, M = 28.7% | 42.2 | 57.8 | N/S | |
| HCW [71] | N = 1205, F = 90% | 63 | N/S | N/S | |
| Canada | GP [73] | N = 3674, F = 43% | N/S | N/S | 20 |
| HCW [74] | N = 1541 | 65 | N/S | N/S | |
| Turkey | GP [62] | N = 3936 | 54 | 31 | N/S |
| HCW [75] | N = 1138, F = 72.5 | N/S | 43 | N/S | |
| Ireland | GP [61] | N = 1041 | 65 | N/S | N/S |
| Denmark and Portugal | GP [76] | N = 7664 | 73.9 | N/S | N/S |
| Scotland | GP [77] | N = 3436 | 74 | N/S | N/S |
| Poland | GP [78] | N = 1066 | 37 | N/S | N/S |
| Congo | HCW [10] | N = 613, F = 49.1 | 28 | N/S | N/S |
| Greece | GP [81] | N = 1004, F = 49% | 57.7 | 16.3 | 26 |
| Indonesia | GP [80] | N = 1359, F = 65.7 | 78.3 | N/S | N/S |
| Qatar | GP [82] | N = 7821, M = 59.4% | N/S | 19.8 | 20.2 |
| Saudi Arabia | GP [83] | N = 992, M = 34% | N/S | 35 | N/S |
| Jordan | GP [87] | N = 2173, M = 30.6% | 29.1 | N/S | N/S |
| Kuwait | GP [85] | N = 2368, F = 67.4% | 53.1 | N/S | N/S |
| Determinants | No. of Paper | Place of Study | Education | Occupation |
|---|---|---|---|---|
| Vaccine safety and efficacy | 15 | USA, China, Hong Kong, Australia, England, France, Qatar | Undergrad | HCW, full-time employee |
| Vaccine side effects | 12 | USA, China, Canada, Turkey, Kuwait | High school, secondary | Workers, employee, nurse |
| Individuals believe that they are at less risk to get infected by COVID-19 | 9 | USA, Saudi Arabia, UK, Italy | High school to university | Employee |
| Religious beliefs | 5 | France, Denmark, Portugal, Germany | High school | Not specified |
| Price of vaccine and lack of insurance | 5 | China, Indonesia, USA | Primary school and high school | Private sector employee |
| Mistrust in healthcare | 7 | USA | College education | Student, employed |
| Mistrust in government | 6 | France, Ireland, Italy, USA | All level | All profession |
| The rapid development of a vaccine | 5 | Jordan, USA, UK | University level | Doctors, nurse, employed |
| Widespread misinformation in the social media | 7 | Greece, European countries, Jordan, Kuwait | High school | Student, employed, unemployed, retired |
| Past vaccine experience | 3 | Australia, France | Diploma | Health workers |
| Demographic influence | 4 | Turkey, USA, Italy | High school, bachelor | All profession |
| Political instability | 3 | USA | All level | HCWs, all profession |
| Racist and ethnic minority | 3 | USA | High school, bachelor | All profession |
| Trust in the vaccine manufacturer | 5 | China, Hong Kong | Primary to bachelor’s degree | HCWs, employee, student |
| Lockdown periods decrease the number of cases | 1 | Italy | High school | All level |
| Trust in natural remedies | 1 | America and Canada | All level | Full-time and part-time employee |
| Lack of information about vaccine | 4 | Saudi Arabia, Qatar, Kuwait, Jordan | High school to graduate | Employed |
| Inconsistent risk message from public health organization | 4 | USA, Canada, UK | All level | All level |
| Anti-vaccination movement | 4 | USA, Jordan, Europe | High school to undergrad | Employed |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biswas, M.R.; Alzubaidi, M.S.; Shah, U.; Abd-Alrazaq, A.A.; Shah, Z. A Scoping Review to Find Out Worldwide COVID-19 Vaccine Hesitancy and Its Underlying Determinants. Vaccines 2021, 9, 1243. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9111243
Biswas MR, Alzubaidi MS, Shah U, Abd-Alrazaq AA, Shah Z. A Scoping Review to Find Out Worldwide COVID-19 Vaccine Hesitancy and Its Underlying Determinants. Vaccines. 2021; 9(11):1243. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9111243
Chicago/Turabian StyleBiswas, Md. Rafiul, Mahmood Saleh Alzubaidi, Uzair Shah, Alaa A. Abd-Alrazaq, and Zubair Shah. 2021. "A Scoping Review to Find Out Worldwide COVID-19 Vaccine Hesitancy and Its Underlying Determinants" Vaccines 9, no. 11: 1243. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9111243