
Use of Intravaginal Progesterone-Releasing Device Results in Similar Pregnancy Rates and Losses to Long-Acting Progesterone to Synchronize Acyclic Embryo Recipient Mares

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experiment 1
2.1.1. Animals and Husbandry
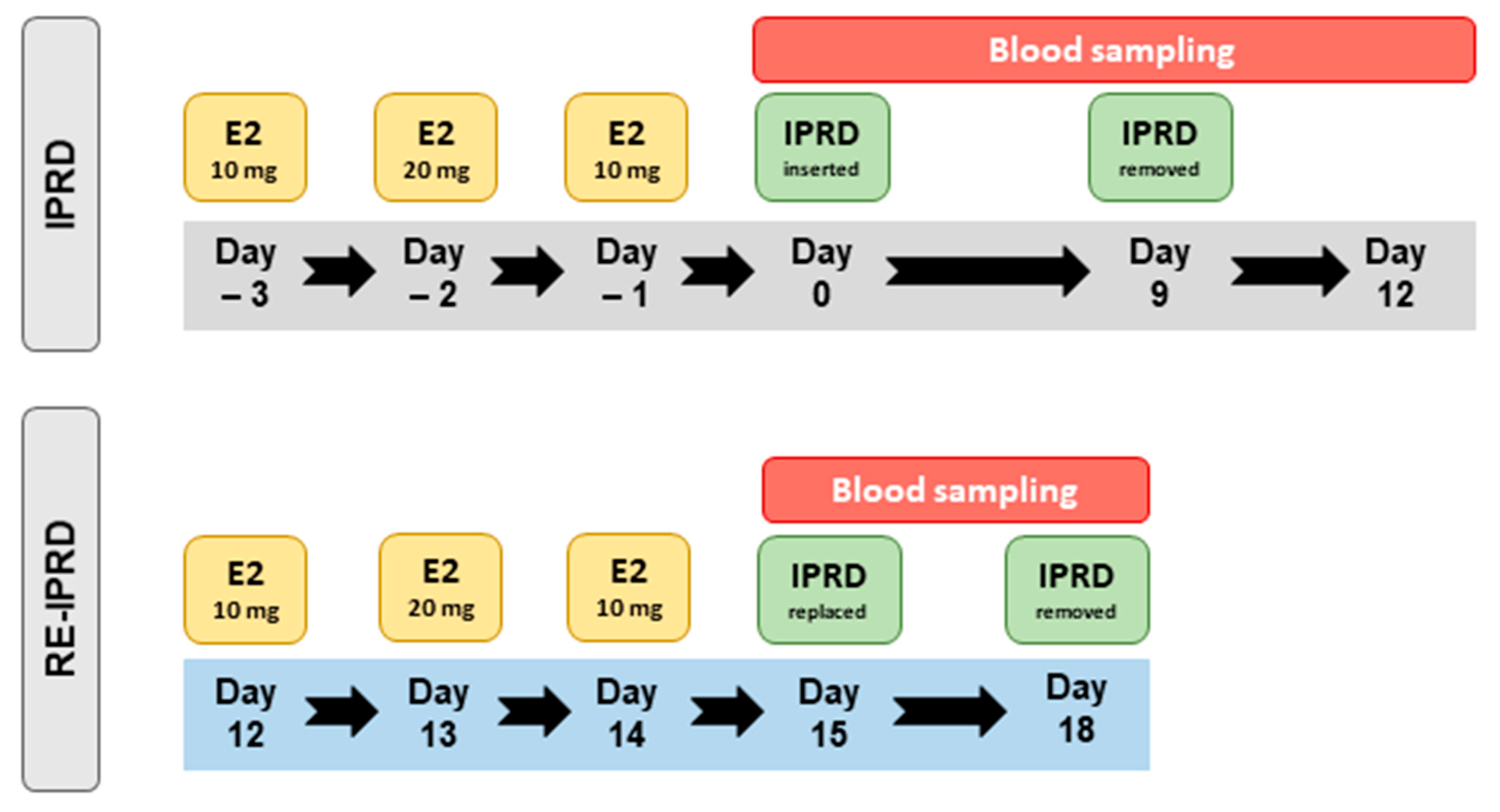
2.1.2. Design
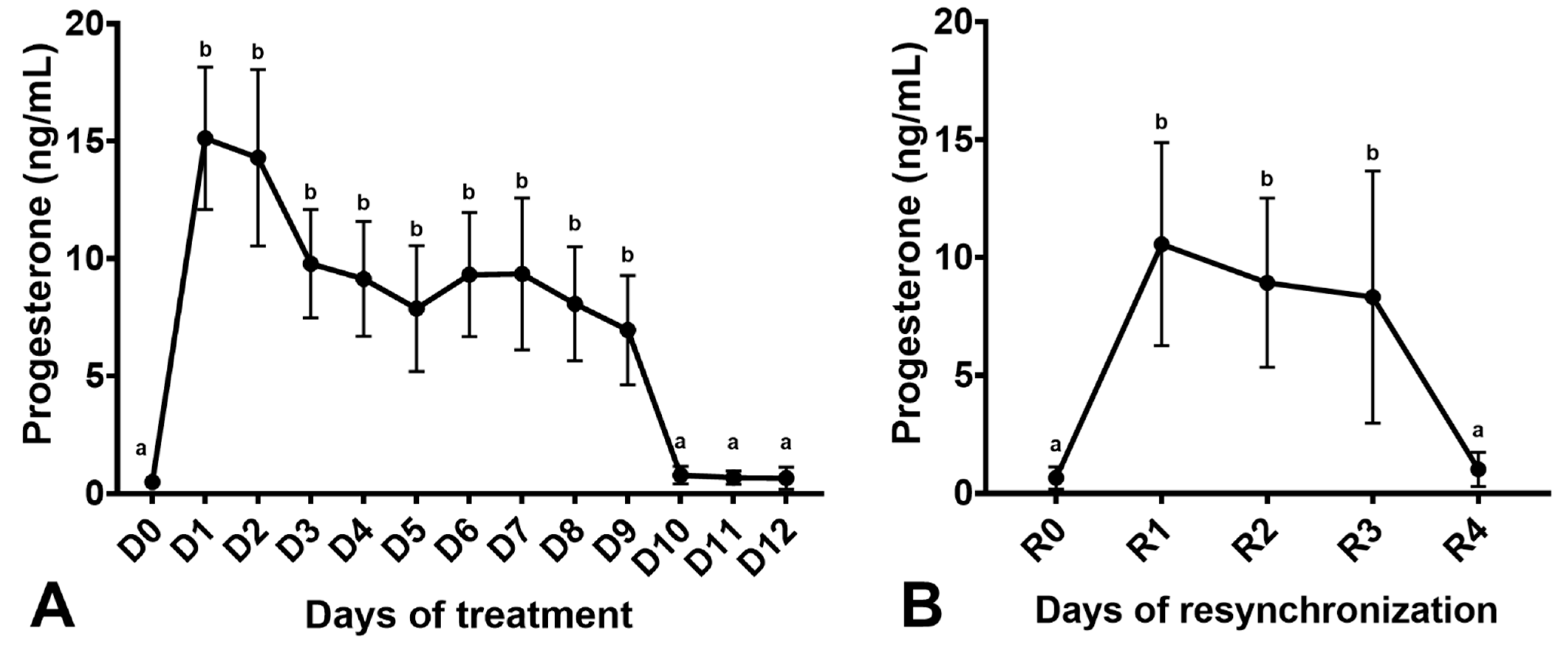
2.1.3. Progesterone Evaluation
2.2. Experiment 2
Breeding Management of Embryo Donor Mares, Embryo Flushing, and Transfer
2.3. Statistical Analyses
3. Results
3.1. Experiment 1
3.2. Experiment 2
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Squires, E.L.; McCue, P.M.; Vanderwall, D. The current status of equine embryo transfer. Theriogenology 1999, 51, 91–104. [Google Scholar] [CrossRef]
- Panzani, D.; Rota, A.; Pacini, M.; Vannozzi, I.; Camillo, F. One year old fillies can be successfully used as embryo donors. Theriogenology 2007, 67, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.L.H. Embryo transfer in competition horses: Managing mares and expectations. Equine Vet. Educ. 2014, 26, 322–327. [Google Scholar] [CrossRef]
- McCue, P.; Squires, E. Equine Embryo Transfer, 1st ed.; CRC Press: Boca Raton, FL, USA, 2015. [Google Scholar]
- Allen, W.R.; Rowson, L.E. Surgical and non-surgical egg transfer in horses. J. Reprod. Fertil. Suppl. 1975, 23, 525–530. [Google Scholar]
- Greco, G.M.; Fioratti, E.G.; Segabinazzi, L.G.; Dell’Aqua, J.A.; Crespilho, A.M.; Castro-Chaves, M.M.B.; Alvarenga, M.A. Novel long-acting progesterone protocols used to successfully synchronize donor and recipient mares with satisfactory pregnancy and pregnancy loss rates. J. Equine Vet. Sci. 2016, 39, 58–61. [Google Scholar] [CrossRef]
- Oliveira Neto, I.V.; Canisso, I.F.; Segabinazzi, L.G.; Dell’Aqua, C.P.F.; Alvarenga, M.A.; Papa, F.O.; Dell’Aqua, J.A. Synchronization of cyclic and acyclic embryo recipient mares with donor mares. Anim. Reprod. Sci. 2018, 190, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ginther, O.J. Reproductive Biology of the Mare-Basic and Applied Aspects, 2nd ed.; Equiservices Publishing: Cross Plains, WI, USA, 1992. [Google Scholar]
- Filho, A.N.R.; Pessôa, M.A.; Gioso, M.M.; Alvarenga, M.A. Transfer of equine embryos into anovulatory recipients supplemented with short or long acting progesterone. Anim. Reprod. 2004, 1, 91–95. [Google Scholar]
- Hinrichs, K.; Sertich, P.L.; Kenney, R.M. Use of altrenogest to prepare ovariectomized mares as embryo transfer recipients. Theriogenology 1986, 26, 455–460. [Google Scholar] [CrossRef]
- McKinnon, A.O.; Squires, E.L.; Carnevale, E.M.; Hermenet, M.J. Ovariectomized steroid-treated mares as embryo transfer recipients and as a model to study the role of progestins in pregnancy maintenance. Theriogenology 1988, 29, 1055–1063. [Google Scholar] [CrossRef]
- Silva, E.S.M.; Ignácio, F.S.; Fritsch, S.C.; Zanoni, D.S.; Pantoja, J.C.F.; Oliveira-Filho, J.P.; Meira, C. Administration of 2.5 mg of estradiol followed by 1500 mg of progesterone to anovulatory mares promote similar uterine morphology, hormone concentrations and molecular dynamics to those observed in cyclic mares. Theriogenology 2017, 97, 159–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, E.S.M.; Roser, J.F.; Gomes, A.R.C.; Fritsch, S.C.; Pantoja, J.C.F.; Oliveira-Filho, J.P.; Meira, C. Comparison of different regimens of estradiol benzoate treatments followed by long-acting progesterone to prepare noncycling mares as embryo recipients. Theriogenology 2016, 86, 1749–1756. [Google Scholar] [CrossRef] [Green Version]
- Silva, E.S.M.; Cuervo-Arango, J.; de Ruijter-Villani, M.; Klose, K.; Oquendo, P.S.; Stout, T.A.E. Effect of the duration of estradiol priming prior to progesterone administration on endometrial gene expression in anestrous mares. Theriogenology 2019, 131, 96–105. [Google Scholar] [CrossRef]
- Silva, E.S.M.; Vaz, I.S.; Rodrigues, T.S.; Brandão, F.Z.; Oquendo, P.S.; Oquendo, F.M.G.; Beletti, M.E.; Cuervo-Arango, J. Artificial long estrus protocols administered prior to progesterone increase endometrial uterocalin expression in anestrous mares. J. Equine Vet. Sci. 2021, 103, 103669. [Google Scholar] [CrossRef]
- Squires, E.L. Hormonal manipulation of the mare: A review. J. Equine Vet. Sci. 2008, 28, 627–634. [Google Scholar] [CrossRef]
- Vanderwall, D.K.; Marquardt, J.L.; Woods, G.L. Use of a compounded long-acting progesterone formulation for equine pregnancy maintenance. J. Equine Vet. Sci. 2007, 27, 62–66. [Google Scholar] [CrossRef]
- Martínez, M.F.; Kastelic, J.P.; Adams, G.P.; Cook, B.; Olson, W.O.; Mapletoft, R.J. The use of progestins in regimens for fixed-time artificial insemination in beef cattle. Theriogenology 2002, 57, 1049–1059. [Google Scholar] [CrossRef]
- Polo, G.; De Lima, L.G.F.; Kozicki, L.E.; Junior, J.A.D.A.; Camargo, C.E.; Segui, M.S.; Macan, R.; Alberini, V.; Ladewig, E.; Weiss, R.R.; et al. Two administrations of an intravaginal progesterone device on the induction of ovarian cyclicity in anestrous mares. Pferdeheilkunde 2016, 32, 217–222. [Google Scholar] [CrossRef] [Green Version]
- Hanlon, D.W.; Firth, E.C. The reproductive performance of Thoroughbred mares treated with intravaginal progesterone at the start of the breeding season. Theriogenology 2012, 77, 952–958. [Google Scholar] [CrossRef] [PubMed]
- Newcombe, J.R. Field observations on the use of a progesterone-releasing intravaginal device to induce estrus and ovulation in seasonally anestrous mares. J. Equine Vet. Sci. 2002, 22, 378–382. [Google Scholar] [CrossRef]
- Handler, J.; Schönlieb, S.; Hoppen, H.O.; Aurich, C. Seasonal effects on attempts to synchronize estrus and ovulation by intravaginal application of progesterone-releasing device (PRIDTM) in mares. Theriogenology 2006, 65, 1145–1158. [Google Scholar] [CrossRef]
- Canisso, I.F.; Gallacher, K.; Gilbert, M.A.; Korn, A.; Schweizer, C.M.; Bedford-Guaus, S.J.; Gilbert, R.O. Preovulatory progestagen treatment in mares fails to delay ovulation. Vet. J. 2013, 197, 324–328. [Google Scholar] [CrossRef]
- Donadeu, F.X.; Watson, E.D. Seasonal changes in ovarian activity: Lessons learnt from the horse. Anim. Reprod. Sci. 2007, 100, 225–242. [Google Scholar] [CrossRef]
- Aurich, C. Reproductive cycles of horses. Anim. Reprod. Sci. 2011, 124, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Henneke, D.R.; Potter, G.D.; Kreider, J.L.; Yeates, B.F. Relationship between condition score, physical measurements and body fat percentage in mares. Equine Vet. J. 1983, 15, 371–372. [Google Scholar] [CrossRef] [PubMed]
- Polasek, T.C.M.; Kozicki, L.E.; Pedrosa, V.B.; Weiss, R.R.; Bertol, M.A.F.; Camargo, C.E.; Talini, R. Impact of a progesterone-releasing intravaginal device and inflammatory reaction on ovarian activity in embryo-recipient anestrus mares. Theriogenology 2017, 90, 175–184. [Google Scholar] [CrossRef]
- McCue, P.M.; DeLuca, C.A.; Ferris, R.A.; Wall, J.J. How to evaluate equine embryos. In Proceedings of the 55th American Association of Equine Practitioners, Las Vegas, Negava, 5–9 December 2009; pp. 252–256. [Google Scholar]
- Alvarenga, M.A.; Landim-Alvarenga, F.C.; Meira, C. Modifications in the technique used to recover equine embryos. Equine Vet. J. 2010, 25, 111–112. [Google Scholar] [CrossRef]
- Taylor, R. Interpretation of the correlation coefficient. J. Diagn. Med. Sonogr. 1990, 6, 35–39. [Google Scholar] [CrossRef]
- Hanlon, D.W.; Evans, M.J.; Firth, E.C. Effects of intravaginal progesterone on follicular dynamics and FSH, LH and progesterone concentrations in transitional mares. Anim. Reprod. Sci. 2010, 121, 32–34. [Google Scholar] [CrossRef]
- Handler, J.; Schönlieb, S.; Hoppen, H.O.; Aurich, C. Influence of reproductive stage at PRIDTM insertion on synchronization of estrus and ovulation in mares. Anim. Reprod. Sci. 2007, 97, 382–393. [Google Scholar] [CrossRef]
- Rigoleto Júnior, W.L.; Dias de Camargo Neto, W.; de Paula Nogueira, G.; Ferrari, T.A.; Bertan Membrive, C.M.; Giometti, I.C.; Castilho, C. Serum progesterone and conception rates in acyclic embryo recipient mares using a bovine progesterone-releasing intravaginal device. J. Equine Vet. Sci. 2021, 97, 103325. [Google Scholar] [CrossRef] [PubMed]
- Pohp, O.; Buff, S.; Gamier, F.; Guérin, P.; Lefranc, A.C. Pharmacokinetic analysis during intravaginal progesterone-releasing devices (PRID®/CIDR®) application in the mare. Pferdeheilkunde 2009, 25, 105–110. [Google Scholar] [CrossRef] [Green Version]
- Botelho, J.H.V.; Pessoa, G.O.; Rocha, L.G.P.; Yeste, M. Hormone supplementation protocol using estradiol benzoate and long-acting progesterone is efficient in maintaining pregnancy of anovulatory recipient mares during autumn transitional phase. Anim. Reprod. Sci. 2015, 153, 39–43. [Google Scholar] [CrossRef]
- Beyer, T.; Rink, B.E.; Scarlet, D.; Walter, I.; Kunert, S.; Aurich, C. Early luteal phase progestin concentration influences endometrial function in pregnant mares. Theriogenology 2019, 125, 236–241. [Google Scholar] [CrossRef]
- Bazer, F.W.; Spencer, T.E.; Johnson, G.A.; Burghardt, R.C.; Wu, G. Comparative aspects of implantation. Reproduction 2009, 138, 195–209. [Google Scholar] [CrossRef] [Green Version]
- Spencer, T.E.; Bazer, F.W. Biology of progesterone action during pregnancy recognition and maintenance of pregnancy. Anim. Biotechnol. 2002, 7, 1879–1898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto, M.R.; Miragaya, M.H.; Burns, P.; Douglas, R.; Neild, D.M. Strategies for increasing reproductive efficiency in a commercial embryo transfer program with high performance donor mares under training. J. Equine Vet. Sci. 2017, 54, 93–97. [Google Scholar] [CrossRef]
- Canisso, I.F.; Beltaire, K.A.; Bedford-Guaus, S.J. Premature luteal regression in a pregnant mare and subsequent pregnancy maintenance with the use of oral altrenogest. Equine Vet. J. 2012, 45, 97–100. [Google Scholar] [CrossRef] [PubMed]
- Carnevale, E.M.; Ramirez, R.J.; Squires, E.L.; Alvarenga, M.A.; Vanderwall, D.K.; McCue, P.M. Factors affecting pregnancy rates and early embryonic death after equine embryo transfer. Theriogenology 2000, 54, 965–979. [Google Scholar] [CrossRef]
- Kaercher, F.; Kozicki, L.E.; Camargo, C.E.; Weiss, R.R.; dos Santos, I.W.; Muradas, P.R.; Bertol, M.A.F.; de Abreu, R.A. Embryo Transfer in Anovulatory Recipient Mares Treated with Estradiol Benzoate and Long-Acting Progesterone. J. Equine Vet. Sci. 2013, 33, 205–209. [Google Scholar] [CrossRef]
- Wilsher, S.; Clutton-Brock, A.; Allen, W.R. Successful transfer of day 10 horse embryos: Influence of donor-recipient asynchrony on embryo development. Reproduction 2010, 139, 575–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacob, J.C.F.; Haag, K.T.; Santos, G.O.; Oliveira, J.P.; Gastal, M.O.; Gastal, E.L. Effect of embryo age and recipient asynchrony on pregnancy rates in a commercial equine embryo transfer program. Theriogenology 2012, 77, 1159–1166. [Google Scholar] [CrossRef] [PubMed]
- Cuervo-Arango, J.; Clark, A. The first ovulation of the breeding season in the mare: The effect of progesterone priming on pregnancy rate and breeding management (hCG response rate and number of services per cycle and mare). Anim. Reprod. Sci. 2010, 118, 265–269. [Google Scholar] [CrossRef]
- Mateu-Sánchez, S.; Newcombe, J.R.; Garcés-Narro, C.; Cuervo-Arango, J. The period of the follicular phase during which the uterus of mares shows estrus-like echotexture influences the subsequent pregnancy rate. Theriogenology 2016, 86, 1506–1515. [Google Scholar] [CrossRef] [PubMed]
- Cuervo-Arango, J.; Claes, A.N.; Ruijter-Villani, M.; Stout, T.A. Likelihood of pregnancy after embryo transfer is reduced in recipient mares with a short preceding oestrus. Equine Vet. J. 2018, 50, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Allen, W.R. Luteal deficiency and embryo mortality in the mare. Reprod. Domest. Anim. 2001, 36, 121–131. [Google Scholar] [CrossRef]
- Aupperle, H.; Özgen, S.; Schoon, H.A.; Schoon, D.; Hoppen, H.O.; Sieme, H.; Tannapfel, A. Cyclical endometrial steroid hormone receptor expression and proliferation intensity in the mare. Equine Vet. J. 2000, 32, 228–232. [Google Scholar] [CrossRef]
- Hartt, L.S.; Carling, S.J.; Joyce, M.M.; Johnson, G.A.; Vanderwall, D.K.; Ott, T.L. Temporal and spatial associations of oestrogen receptor alpha and progesterone receptor in the endometrium of cyclic and early pregnant mares. Reproduction 2005, 130, 241–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gebhardt, S.; Merkl, M.; Herbach, N.; Wanke, R.; Handler, J.; Bauersachs, S. Exploration of global gene expression changes during the estrous cycle in equine endometrium. Biol. Reprod. 2012, 87, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Day of Synchronization | D4 | D5 | D6 | D7 | D8 | Total |
|---|---|---|---|---|---|---|
| Categories | ||||||
| Absent | 11 | 6 | 2 | 0 | 0 | 19 |
| Mild | 24 | 19 | 27 | 11 | 9 | 90 |
| Moderate | 2 | 0 | 6 | 8 | 5 | 21 |
| Severe | 0 | 0 | 0 | 0 | 1 | 1 |
| Total | 37 | 25 | 35 | 19 | 15 | 131 |
| Pregnancy rates | 73% (27/37) | 76% (19/25) | 69% (24/35) | 68% (13/19) | 71% (10/14) | 72% (93/130) |
| Pregnancy losses | 11% (3/27) | 11% (2/19) | 8% (2/24) | 15% (2/13) | 20% (2/10) | 12% (11/93) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Segabinazzi, L.G.T.M.; Andrade, L.R.P., Jr.; Alvarenga, M.A.; Dell’Aqua, J.A., Jr.; Canisso, I.F. Use of Intravaginal Progesterone-Releasing Device Results in Similar Pregnancy Rates and Losses to Long-Acting Progesterone to Synchronize Acyclic Embryo Recipient Mares. Vet. Sci. 2021, 8, 190. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci8090190
Segabinazzi LGTM, Andrade LRP Jr., Alvarenga MA, Dell’Aqua JA Jr., Canisso IF. Use of Intravaginal Progesterone-Releasing Device Results in Similar Pregnancy Rates and Losses to Long-Acting Progesterone to Synchronize Acyclic Embryo Recipient Mares. Veterinary Sciences. 2021; 8(9):190. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci8090190
Chicago/Turabian StyleSegabinazzi, Lorenzo G. T. M., Luiz R. P. Andrade, Jr., Marco A. Alvarenga, Jose A. Dell’Aqua, Jr., and Igor F. Canisso. 2021. "Use of Intravaginal Progesterone-Releasing Device Results in Similar Pregnancy Rates and Losses to Long-Acting Progesterone to Synchronize Acyclic Embryo Recipient Mares" Veterinary Sciences 8, no. 9: 190. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci8090190