

Health-Care Seeking Behavior and Treatment of Menstrual Migraine among Danish Women—A Social Media Study

1
Department of Neurology, Danish Headache Center, Copenhagen University Hospital, 2600 Glostrup, Denmark
2
Pfizer Denmark, 2750 Ballerup, Denmark
*
Author to whom correspondence should be addressed.
Women 2023, 3(3), 385-395; https://0-doi-org.brum.beds.ac.uk/10.3390/women3030029
Submission received: 2 June 2023
/
Revised: 30 June 2023
/
Accepted: 5 July 2023
/
Published: 17 July 2023
(This article belongs to the Topic Women's Health and Aging)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:An estimated 4–8% of all women, and 16–25% of women with migraine, have menstrual migraine (MM), which causes considerable disability, but is underdiagnosed and undertreated. We investigated the burden of disease, health-care seeking behavior, and treatment practices among women with MM, using social media. In 12 days, 6246 women answered an online survey, allowing for diagnosis of MM by the International Classification of Headache Disorders third edition (ICHD-3). In total, 47% had MM, 21% had non-menstrual migraine (nMM), and 15% had probable menstrual migraine (pMM). Among women with MM, 61% had missed out on school/work and 69% on family, leisure, or social activities in the last 3 months. Fifty-four percent had consulted a health-care practitioner about their MM, of whom thirty-seven percent had received information about medical treatment of MM. A total of 85% used medicine in connection with MM, either over-the-counter medication only (57%), prescription medication only (24%), or both. Social media offers an efficient and less expensive recruitment platform for population-based studies on MM and is a useful tool to raise public awareness about MM. Moreover, this study confirms the significant impact of MM on women’s everyday lives and the challenges it poses to their regular activities.
1. Introduction
Menstrual migraine (MM) is defined as migraine occurring on the first day of menstruation ±2 days in at least two out of three menstrual cycles [1]. It is estimated that 4–8% of all women, and 16–25% of women with migraine, have migraine attacks in connection with their menstruation [2,3,4,5,6]. Migraine incidence peaks around the first day of menstruation, and the pathophysiological causes, although still elusive, revolve around the premenstrual estrogen withdrawal and prostaglandin release [5]. MM, like non-menstrual migraine (nMM) occurring outside of the menstrual cycle, can be treated with over-the-counter (OTC) medications or acute or preventive migraine prescription drugs, but MM may be more painful, have longer duration, and be less responsive to medication than nMM [5,7].
People with MM and nMM have a high burden of disease due to both symptoms of migraine and how they affect their work and social life. One study found that women had increased frequency, intensity, and duration of pain and associated symptoms such as nausea, photophobia, phonophobia, osmophobia, allodynia, cranial autonomic symptoms (facial/forehead sweating, lacrimation, ptosis, conjunctival injection, rhinorrhea, nasal congestion, and miosis), and mental health problems compared with men, and overall carried 79% of the migraine disease burden and had a lower effect from OTC medication [2]. Another study with the Headache Impact Test—6 item (HIT-6) and Migraine Disability Assessment Scale (MIDAS), measuring, i.e., housework, work for pay, and leisure time, found that HIT-6 and MIDAS scores were significantly higher for the group with MM and menstrual-associated migraine compared with the group with migraine unrelated to menstruation [8]. Additionally, migraine has an economic impact due to both direct medical costs and indirect costs due to lost productivity, and possibly unemployment and underemployment [9]. Despite this high burden of disease, migraine, including MM, is underdiagnosed and undertreated [10,11]. Even in Denmark, with free access to universal health care and substantial reimbursement of prescribed drug purchases, many migraine patients do not consult a health-care practitioner for their migraine [12], and among those who do, only about 20% receive information about triptans as a potential treatment option [13]. The low diagnosis rate has potential implications for school, work, family, and social life [14,15]. In Denmark, people with migraine had 1.7 million more visits to the GP and 3.8 million more sick days than people without migraine [15].
Research on MM in patients attending tertiary headache centers or based on population studies [6,8,16] may be both time consuming and costly. Health-care professionals and researchers are increasingly leveraging social media to recruit patients for clinical research, as it facilitates reaching a large audience for a relatively low cost [17,18], and this method has also been utilized in headache research [12,19,20]. Social media studies may also contribute to breaking down barriers between physicians and patients and improving how patient perspectives are included in clinical research [19,21,22].
In Denmark, the use of social media is prevalent, with 85.3% of the total Danish population using social media at the start of 2022. Facebook had 3.6 million users (52.1% female, 47.9% male) and Instagram had 2.70 million users (57.4% female, 42.6% male), presumably +13 years of age as required by these platforms [23]. Since migraine in women often debuts after puberty, and peaks in incidence at 20–24 years of age and prevalence at 35–39 years of age [2,24,25], we assumed that a large part of the undiagnosed population with MM would be present on social media, and we therefore wanted to use social media to investigate the burden of disease related to MM, health-care seeking behavior among women with MM, and treatment practices for MM including self-treatment and prescribed treatment.
2. Results
2.1. Recruitment
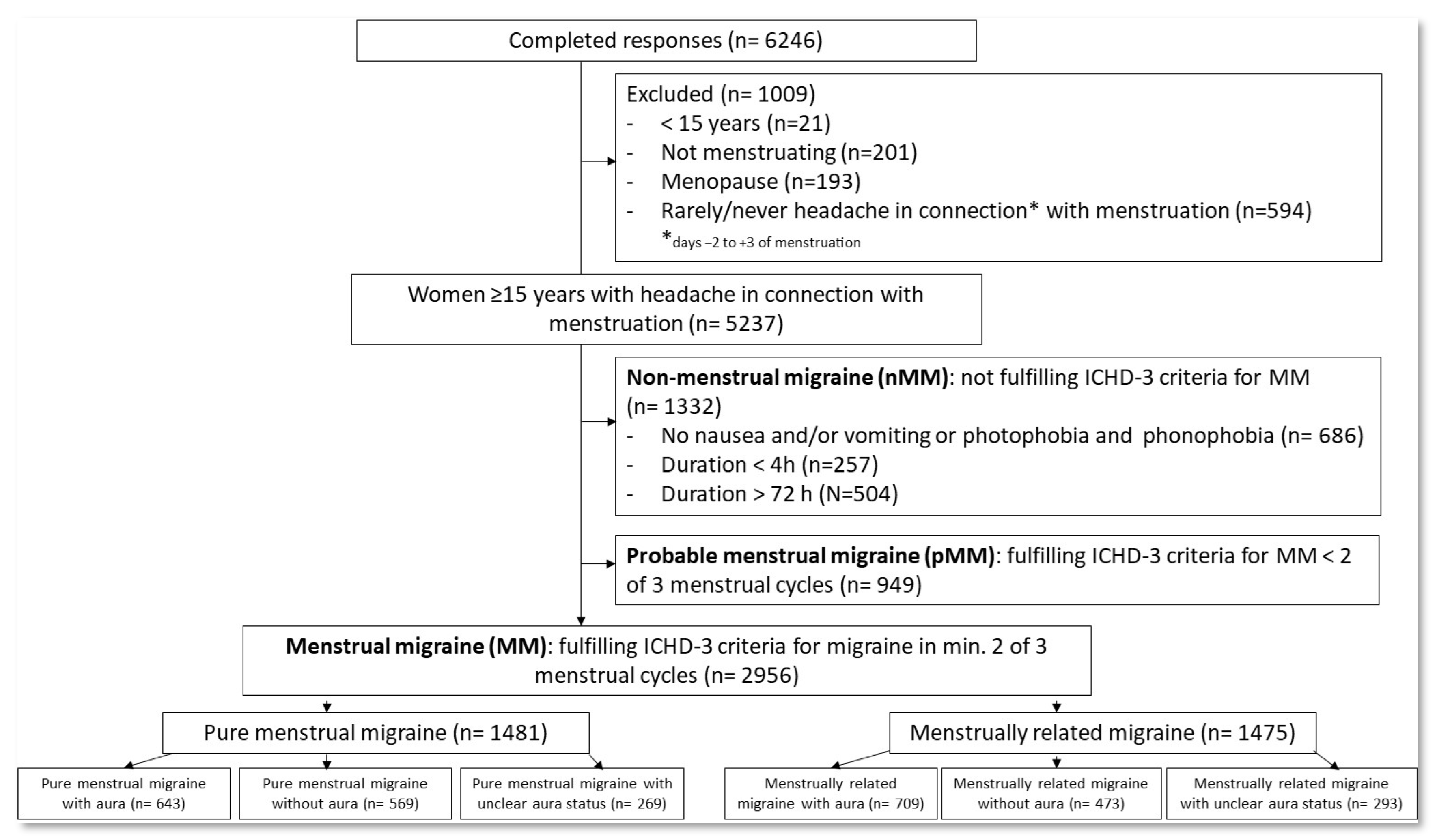
Recruitment from Instagram Stories appeared more effective than Facebook (6746 vs. 4507 clicks, respectively), resulting in 6246 women completing the survey in 12 days, corresponding to 55.6% of clicks resulting in a completed response. As described in Figure 1, after excluding individuals < 15 years of age, without menstruation, or without headache (n= 1009), 2956 women (47%) fulfilled the ICHD-3 criteria for MM (duration of headache/migraine lasting 4–71 h, while also experiencing accompanying symptoms such as nausea and/or vomiting, and/or photophobia and phonophobia, and having these symptoms in at least two out of three menstrual cycles. We did not, however, capture if they had had at least five attacks). There was an almost even split between those who had pure MM (occurring in at least two out of three menstrual cycles and at no other times of the cycle) (50.1%, n = 1481) and those who had MM related to menstruation (occurring in at least two out of three menstrual cycles, and additionally at other times of the cycle) (49.9%, n = 1475) [1]. In total, 2281 women did not fulfill the MM criteria, 1332 (21%) because of not fulfilling the ICHD-3-defined symptoms of migraine (non-menstrual migraine (nMM)), and 949 (15%) because they did not have migraine in at least two out of three menstrual cycles (probable menstrual migraine (pMM)).
2.2. Demography and Clinical Characteristics
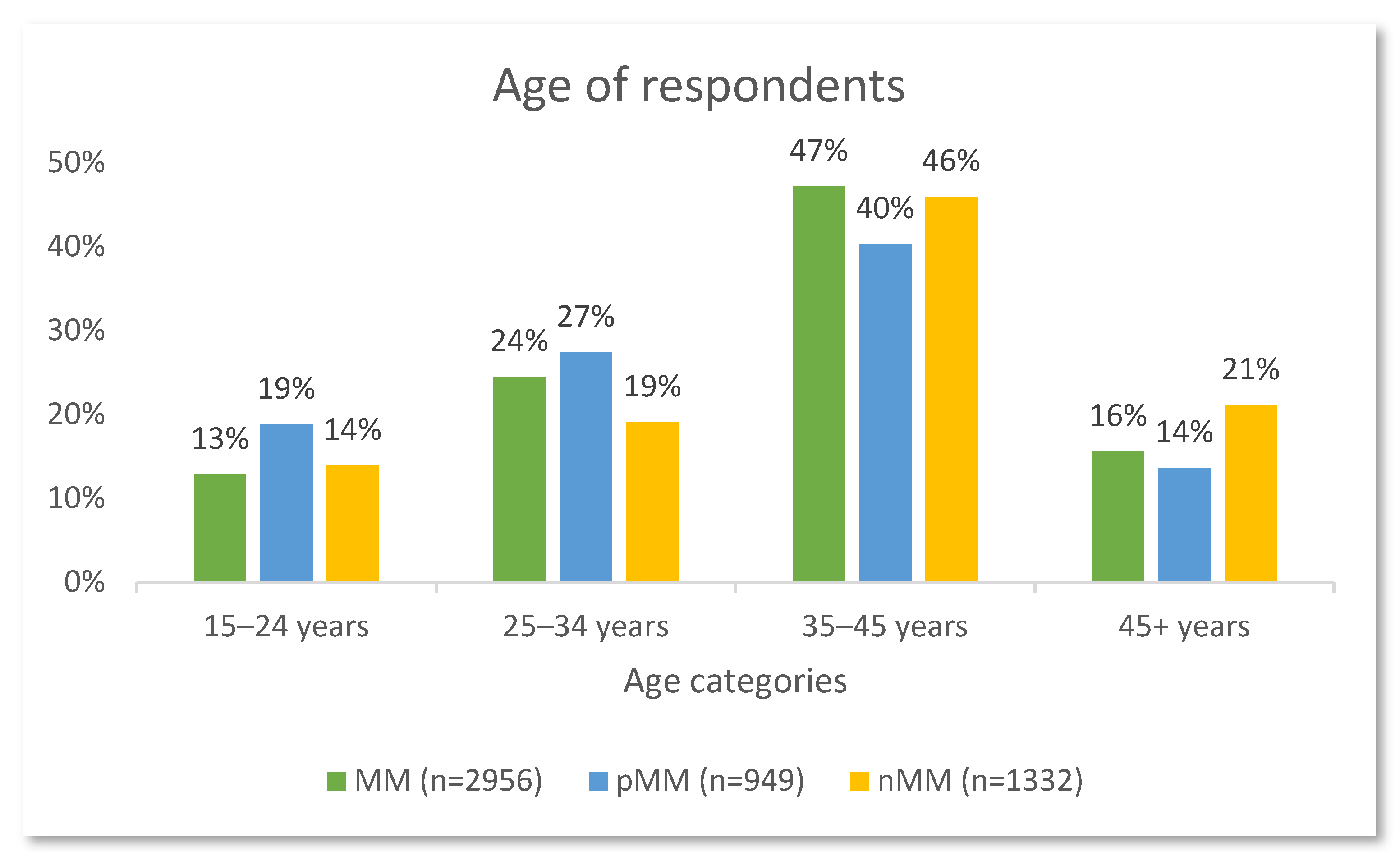
The age categories of respondents are depicted in Figure 2. The majority of respondents were between 35 and 45 years of age.
Among women with MM, 46% had symptoms of aura, while 35% had no aura, and 19% had unclear aura status (meaning they responded ‘Other’ or ‘Don’t know’ on questions related to aura symptoms). Further, 46% had a biological parent or grandparent with migraine, compared with 47% of those with pMM and 37% of those with nMM.
2.3. Burden of Disease
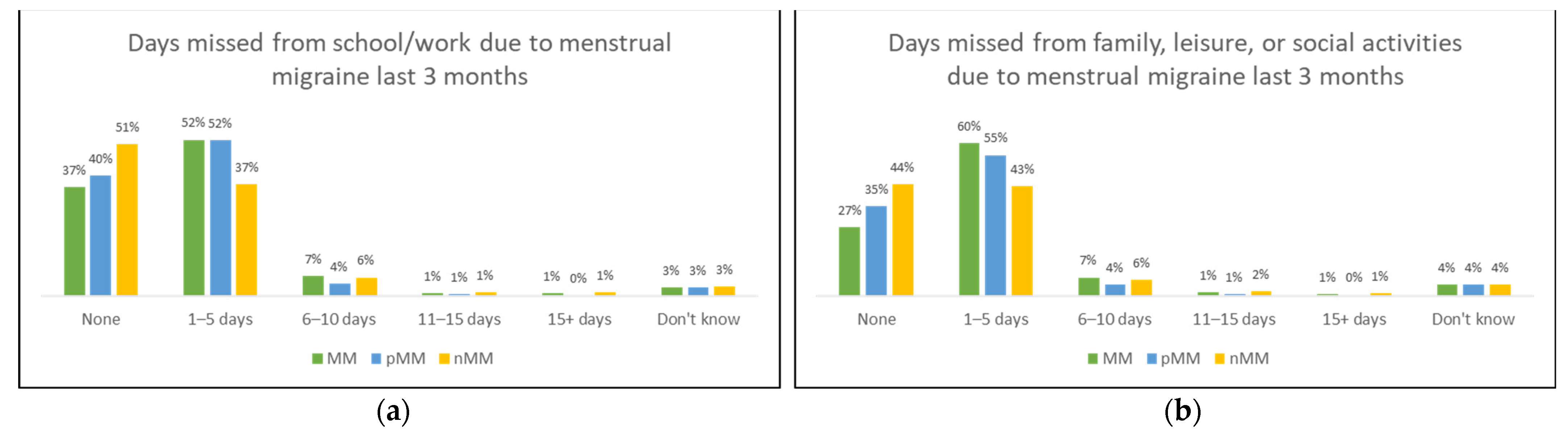
Utilizing questions from the MIDAS questionnaire, we asked about both burden of disease related to migraine, and then to menstrual migraine, and present findings from the latter. The women with MM appeared more burdened by their menstrual migraine than the women with pMM and nMM. Six out of ten (61%) with MM had missed out on school or work during the last 3 months due to MM; see Figure 3a. A total of 52% had missed 1–5 days, 7% missed 6–10 days, 1% missed 11–15 days, and 1% missed more than 15 days. Similarly, 69% had missed out on family, social, or leisure activities in the last three months due to MM, see Figure 3b; 60% had missed 1–5 days, 7% 6–10 days, 1% 11–15 days, and 1% +15 days. Overall, more women with pMM than nMM had missed out on both school/work and family, leisure, and social activities.
2.4. Health-Care Seeking Behavior
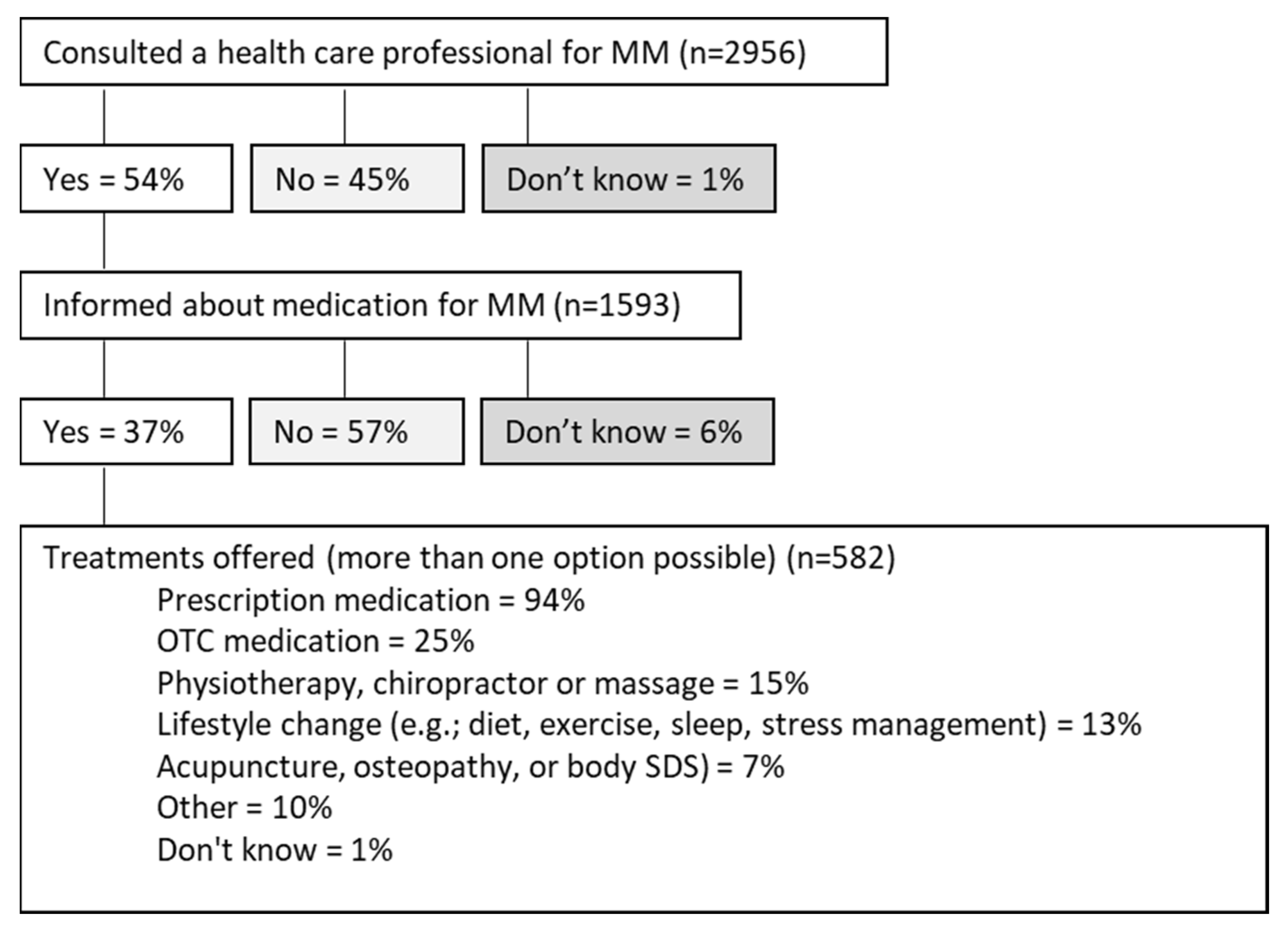
Among women with MM, 54% reported they had consulted a health-care professional (GP, neurologist, or an emergency room) regarding their MM; see Figure 4. Among those who did seek medical help, one in three (37%) had been informed about treatment to treat menstrual migraine. Almost all who were informed about treatment (94%) were offered or accepted prescription medication (e.g., birth control or medicine ending in ‘-triptan’), while 25% were offered or accepted OTC medication (e.g., paracetamol or ibuprofen). In comparison, 39% of women with pMM and 43% of women with nMM had consulted a health-care professional, 35% in each group had been informed about treatment options, and 97% and 90%, respectively, had been offered or accepted prescription medication.
2.5. Treatment of Menstrual Migraine
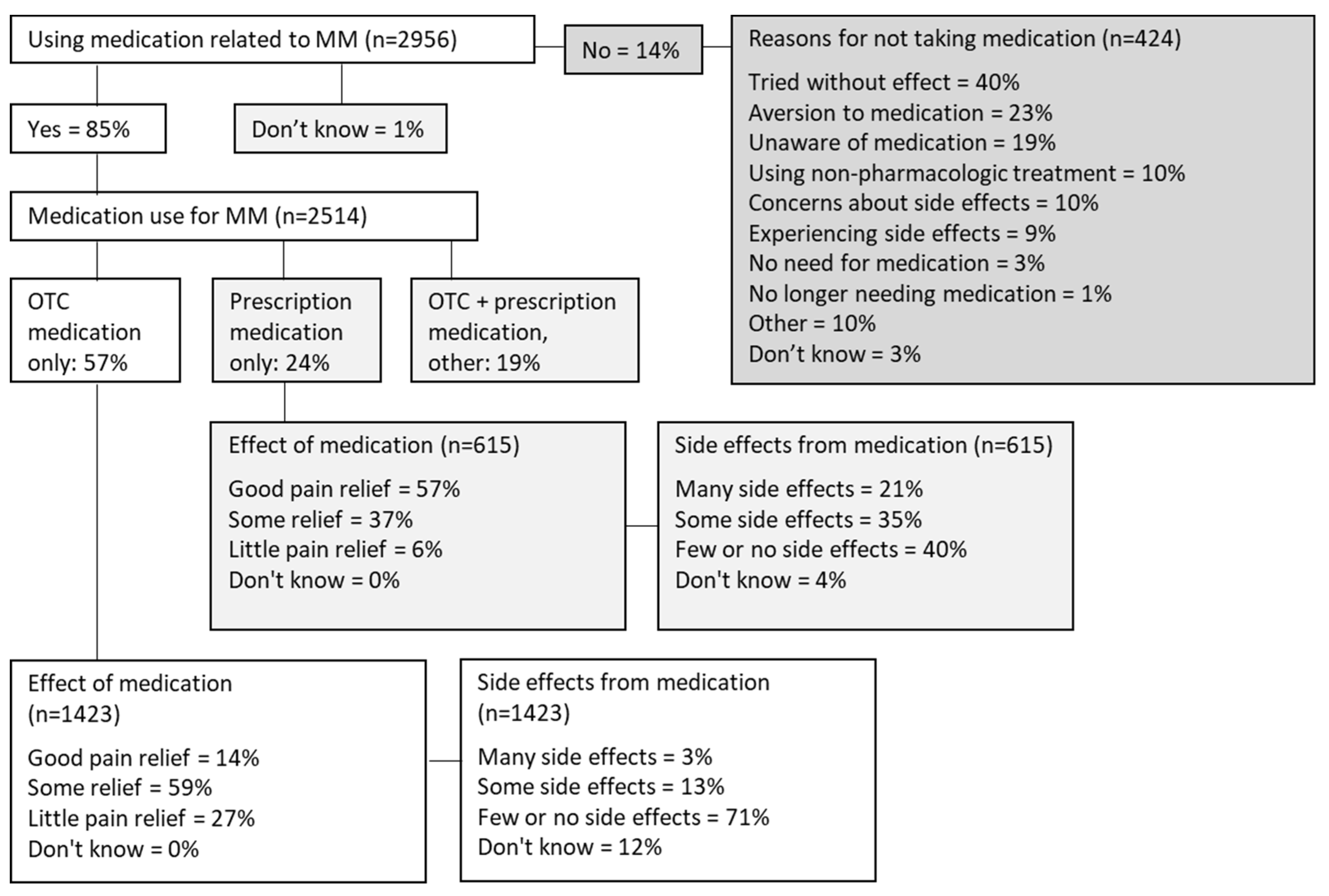
Among women with MM, 85% used medication in connection with MM, see Figure 5, among whom 57% used OTC medication only, 24% used prescription medication (unspecified) only, and 19% used either both or answered ‘other’. Among those who used OTC medication only, 73% had good or some pain relief and 16% had many or some adverse events. In comparison, 94% of those who used prescription medication had good or some pain relief, but 56% had many or some adverse events. Fourteen percent did not use medication for MM. The reported causes of not using medication included previous unsuccessful attempts (40%), aversion to medication (23%), lack of awareness regarding the possibility of using medication to manage migraine (19%), and 10% worried about adverse events due to medication. Among women with pMM, 78% used medication to treat MM; 66% used OTC medication only and 19% used prescription medication only. Among those who used OTC medication only, 80% had good or some pain relief, and 14% had many or some adverse events. Among those who used prescription medication only, 93% had good or some pain relief and 49% had many or some adverse events. Among women with nMM, 81% used medication to treat MM; 66% used OTC medication only and 21% used prescription medication only. Among those who used OTC medication only, 75% had good or some pain relief, and 16% had many or some adverse events. Among those who used prescription medication only, 93% had good or some pain relief and 53% had many or some adverse events.
3. Discussion
In this descriptive social media study, we utilized an online anonymized menstrual migraine questionnaire. In only 12 days, we received complete data responses from 6246 women, 47% (n = 2956) fulfilled the ICHD-3 diagnostic criteria for MM, 15% (n = 949) were considered pMM, and 21% (n = 1332) were considered nMM.
3.1. Burden of Disease Due to Menstrual Migraine
Confirming the burden of disease due to menstrual migraine [8], more than half of women with MM had missed out on school/work, as well as family, social, or leisure activities in the last 3 months due to menstrual migraine. Similar numbers were reported among women with nMM and pMM. This could indicate that some respondents, upon clinical examination and discussion with a health-care professional, would possibly fulfill criteria for MM, or that MM is not adequately captured by the current diagnostic criteria of MM [6]. We also asked respondents about the total 3-month burden of disease related to migraine (not just menstrual migraine), but since results were approximately the same, concluded that respondents had difficulties understanding the difference between the questions and will revise these for future studies.
3.2. Health-Care Seeking Behavior among Women with Menstrual Migraine
Our study found that 45% of women with MM did not contact a health-care provider regarding their MM and even fewer had discussed treatment options with their health-care provider. This is higher than previous studies on migraine in general, which have found that 25% [12] and 37% [13] of participants with migraine or headache never contacted a health-care professional. This difference may either reflect methodological differences or suggest that women with MM seek health-care providers to a lesser extent than individuals with migraine or headache not related to menstruation. Among the women with MM who did seek health care, only 37% had been informed about treatment options specific for menstrual migraine. Although these could include both OTC and prescription medication, previous studies have shown that only 20% receive information about triptans as a potential treatment option for migraine [13]. Among the women who were informed about treatment options, the majority (94%) had been offered or accepted prescription medication and only 25% OTC medication, possibly reflecting that women with MM who seek a health-care professional already treat their MM with OTC and need further treatment options. However, in Denmark, certain medications that are available OTC can be bought at a lower price with a prescription from a health-care professional, which could have confused the respondents. Future studies should explore to which degree acute or preventive treatment including hormonal contraception, OTC, and prescription medication are discussed with, offered to, or accepted by women with MM. Among women with MM who used OTC medications only, 16% had many or some side effects, compared with 56% of those who used prescription medication only. Although we did not ask about the specific medications, the existence of many treatment options should allow for patients to find a treatment with fewer adverse events. Specifically for triptans, patients should try three different triptans, each during three different attacks, before concluding the treatment to be ineffective [26]. However, studies have shown that there is an insufficient adherence to the therapeutic guideline for acute migraine treatment [13]. The reasons for individuals not seeking medical advice for MM, or not receiving a diagnosis or appropriate treatment, may be manyfold. In general, there is a lack of knowledge about migraine among undiagnosed patients [27], stigma, and self-stigma related to migraine [28,29], menstruation [30], and women’s pain in general [31]. Women with dysmenorrhea, another condition occurring during menstruation which is also underdiagnosed and undertreated [32], have reported not seeking health care due to the belief that their symptoms were merely part of being a woman and that their symptoms would not be taken seriously by their health-care provider [33]. Future studies should explore whether the same reasons apply to patients with MM, and whether there is a difference between MM and migraine not related to menstruation. As triptans are underused [13,34], education of GPs on the diagnosis and treatment of migraine remains a priority [35].
3.3. Social Media Offers an Efficient and Appropriate Platform for Studies on Menstrual Migraine in the General Population
This social media survey offers several advantages, such as efficient and inexpensive real-time access to a large population of participants, many of whom may not self-identify as patients, and, thus, social media combines research and disease awareness. For research on MM, our study demonstrates that social media offers a good recruitment platform, since women of reproductive age are active users of social media, and the platform allows for understanding of the burden of disease and health-care seeking and treatment behavior, and may thus complement larger and more complex population-based studies such as the Danish Migraine Population Cohort (DaMP) [2]. Social media may be used for clinical research, and researchers and clinicians may use social media to communicate evidence-based health-care information to the public and contribute to countering the prevalent misinformation on the Internet [36].
3.4. Limitations
While social media presents a promising avenue to efficiently collect data, it is important to recognize the limitations of these digital platforms. For instance, it is important to strike a balance between scientific accuracy and ability to reach and engage with patients, since health literacy is a prevalent problem affected by the number and complexity of questions [37]. This social media study ensured the inclusion of undiagnosed women, who might not have considered that their symptoms were caused by migraine. An alternative approach would have been to collaborate with patient organizations or special interest groups for diagnosed patients active on social media, such as was done in a social media study exploring the use of complementary and integrative medicine (CIM) in people with migraine [19], but this approach would have excluded undiagnosed women and women unaware of their symptoms. We recognize the inherent challenge in using a questionnaire-based anonymous approach that does not quality-check the responses obtained, thus allowing for theoretical fake or dishonest responses. However, we believe this risk to be minimal due to both the IP address restrictions (a responder could only respond one time from one device), the volume of responses we obtained, and the difference in type of questions that were used (using both multiple-choice and scale questions). The methodological strengths of the study were that we used a validated questionnaire for migraine [2] and ICHD-3-defined diagnosis of MM as well as a subset of the validated MIDAS questionnaire related to burden of disease. However, due to the anonymous nature of the questionnaire, we did not capture detailed demographic information such as onset and duration of MM, residence, educational history, financial information, marital status, or data on pregnancy and childbirth. We evaluated the wording of the questions with communication experts and representatives from patient organizations but realized upon analysis that questions related to burden of disease, to understanding of medicine for treatment of migraine, particularly the difference between OTC and prescription medicine, as well as the duration of symptoms (last 3 months) or time since health-care seeking behavior (no specified time), could be ambiguous and have influenced the quality of results. Researchers using social media have limited control over the research environment, as the platforms’ algorithms or policies can impact participant recruitment, data collection, and analysis. However, we collected a large amount of data in a short time span, indicating that MM is a widespread disorder which needs more attention, and that social media is a time-efficient and inexpensive data source that should be utilized to understand MM in the general population. We found that 46% had MM with aura—a considerably higher number than has been published previously [6,16,38]. This may be due to the respondents misunderstanding the question, since 19% reported ‘other’ or ‘don’t know’ to this question. One possibility is that questions related to aura were confused with, e.g., photophobia. Future studies should implement a picture to visualize aura and limit this misunderstanding. Moreover, respondents should be allowed further options to describe whether the symptoms occurred during ‘some’ or ‘most’ migraine attacks, within or outside the menstrual period, and frequency. As the presence of aura may affect decisions about contraception, this should be explored further. We found that around 50% had pure menstrual migraine, which is considerably larger than found in clinical studies and in population-based cohorts [6]. This may be due to recall bias due to the retrospective nature of self-reported questionnaire studies. With these limitations in mind, not only can social media be used for clinical research, but researchers and clinicians can use social media to communicate evidence-based health-care information to the public and contribute to countering the prevalence of misinformation on the Internet.
4. Materials and Methods
4.1. Survey Administration
This study was conducted as an anonymous online survey using Microsoft Forms via paid advertising (approx. 4000 USD) on the social media platforms Facebook (through the ‘Pfizer Denmark’ page) and Instagram Stories in Denmark in November 2022. We consulted a marketing agency (Kompas Kommunikation) to provide consultation on the development of the survey and to develop imagery and content plan (approx. 12,500 USD). The survey anonymously targeted menstruating Danish women 15 years and older and experiencing migraine from days −2 to +3 of the menstrual cycle, as defined in ICHD-3 [1]. The survey questions included screening questions related to having menstruation and migraine, ICHD-3-related diagnostic questions [1], questions 1 and 5 from the MIDAS questionnaire related to missing school/work and family/social/leisure activities in the last 3 months [39], and questions related to health-care seeking behavior and treatment experience. For questions related to treatment of migraine, we provided examples related to over-the-counter medication such as paracetamol and ibuprofen, as we expected these to be well-known to most people, and for prescription treatment we left it open to interpretation in the question related to self-treatment but provided examples such as birth control and medicine ending with ‘-triptan’ in the question related to dialogue with a health-care professional (triptans have, until very recently, been the only acute migraine treatment available on prescription in Denmark). A full version of the questionnaire, translated to English by the authors, is available as Supplementary Material.
Individuals were excluded if they did not menstruate or were post-menopausal, if they were below 14 years of age, if they did not experience headache or migraine symptoms in connection with their menstruation, or if they did not complete the questionnaire. As some individuals may not recognize their symptoms as being caused by migraine, the screening question related to migraine was “How often do you, at the same time as your menstrual period, experience severe headache, migraine or visual disturbances lasting 5–60 min followed by headache?”.
The survey structure was a combination of multiple-choice and scale questions, with standardized response options to facilitate quantitative data collection for measuring and comparison. Some questions related to health-care seeking behavior and treatment choices used branching logic questions, resulting in a maximum of 24 questions. To ensure full anonymity and privacy, there were no open-ended questions, and the survey was posted on Instagram Stories, which does not give the option of commenting, and on Pfizer Denmark’s Facebook, which was monitored 24/7 (no comments were received during the study).
The survey was conducted in Danish and evaluated for comprehension by the marketing agency and representatives of patient organizations within migraine and headache. It was made accessible through computers, smartphones, and tablets, and was estimated to take 10–15 min to complete. It was not possible to re-take the test on the same device with the same IP address. Respondents were not incentivized to participate in the survey. Upon completion, respondents were encouraged to contact their health-care provider in case of questions or concerns related to migraine and to complete a headache diary before doing so, as well as directed to the online resources from the National Knowledge Center for Headache and the Danish patient associations on headache and migraine. The survey was prepared by Pfizer DK in collaboration with Dr. Mona Ameri Chalmer, MD Ph.D., from the Danish Headache Center at Copenhagen University Hospital (Rigshospitalet). The research data were processed and analyzed by Kompas Kommunikation.
4.2. Statistical Analysis
The percentage of respondents selecting each category was reported. This analysis was descriptive in nature and, therefore, no formal hypothesis testing was conducted.
4.3. Permissions and Privacy
This study was conducted in adherence with Pfizer’s policy on personal data and in compliance with regulations on personal data processing and storage. All responses were handled confidentially and anonymously, and data were managed in accordance with GDPR regulations in Denmark. Research involving anonymous questionnaires is exempt from reporting to the national Institutional Review Board (IRB) and from the requirement for informed consent.
5. Conclusions
This social media study found that social media provides a useful recruitment portal for studies on menstrual migraine in the general population. Moreover, social media can be used to further public awareness of menstrual migraine.
Supplementary Materials
The following supporting information can be downloaded at: https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/women3030029/s1, Survey on menstrual migraine.
Author Contributions
Conceptualization, M.A.C. and U.S.L.; methodology, M.A.C. and U.S.L.; formal analysis, M.A.C. and U.S.L.; writing—original draft preparation, U.S.L.; writing—review and editing, M.A.C. and U.S.L.; visualization, M.A.C. and U.S.L.; project administration, U.S.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was financed by Pfizer Denmark.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to exemption regarding questionnaires and interviews from Danish authorities.
Informed Consent Statement
Patient consent was waived due to aggregated, anonymized data.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available as this requires material transfer agreement.
Acknowledgments
The authors thank Peter Jensen of Pfizer Denmark for administrative and technical support in developing the survey.
Conflicts of Interest
MAC has received personal fees from Pfizer Denmark. No honoraria were received in connection with the submitted work. USL is an employee at Pfizer Denmark.
References
- Arnold, M. Headache Classification Committee of the International Headache Society (IHS) the International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Chalmer, M.A.; Kogelman, L.J.A.; Callesen, I.; Christensen, C.G.; Techlo, T.R.; Moller, P.L.; Davidsson, O.B.; Olofsson, I.A.; Schwinn, M.; Mikkelsen, S.; et al. Sex differences in clinical characteristics of migraine and its burden: A population-based study. Eur. J. Neurol. 2023, 30, 1774–1784. [Google Scholar] [CrossRef] [PubMed]
- Mattsson, P. Hormonal factors in migraine: A population-based study of women aged 40 to 74 years. Headache 2003, 43, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Russell, M.B.; Rasmussen, B.K.; Fenger, K.; Olesen, J. Migraine without aura and migraine with aura are distinct clinical entities: A study of four hundred and eighty-four male and female migraineurs from the general population. Cephalalgia 1996, 16, 239–245. [Google Scholar] [CrossRef]
- Vetvik, K.G.; MacGregor, E.A. Menstrual migraine: A distinct disorder needing greater recognition. Lancet Neurol. 2021, 20, 304–315. [Google Scholar] [CrossRef]
- Chalmer, M.A.; Kogelman, L.J.A.; Ullum, H.; Sørensen, E.; Didriksen, M.; Mikkelsen, S.; Dinh, K.M.; Brodersen, T.; Nielsen, K.R.; Bruun, M.T.; et al. Population-Based Characterization of Menstrual Migraine and Proposed Diagnostic Criteria. JAMA Netw. Open 2023, 6, e2313235. [Google Scholar] [CrossRef]
- Wang, M.; Zhu, G.; Song, Z.; Kong, F. Clinical differences between menstrual migraine and nonmenstrual migraine: A systematic review and meta-analysis of observational studies. J. Neurol. 2023, 270, 1249–1265. [Google Scholar] [CrossRef]
- Pavlović, J.M.; Stewart, W.F.; Bruce, C.A.; Gorman, J.A.; Sun, H.; Buse, D.C.; Lipton, R.B. Burden of migraine related to menses: Results from the AMPP study. J. Headache Pain 2015, 16, 24. [Google Scholar] [CrossRef] [Green Version]
- Vetvik, K.G.; MacGregor, E.A. Sex differences in the epidemiology, clinical features, and pathophysiology of migraine. Lancet Neurol. 2017, 16, 76–87. [Google Scholar] [CrossRef]
- Lipton, R.B.; Stewart, W.F.; Celentano, D.D.; Reed, M.L. Undiagnosed migraine headaches. A comparison of symptom-based and reported physician diagnosis. Arch. Intern. Med. 1992, 152, 1273–1278. [Google Scholar] [CrossRef]
- Schreiber, C.P.; Cady, R.K. Diagnosis of menstrual headache and an open-label study among those with previously undiagnosed menstrually related migraine to evaluate the efficacy of sumatriptan 100 mg. Clin. Ther. 2007, 29, 2511–2519. [Google Scholar] [CrossRef] [PubMed]
- Do, T.P.; Dømgaard, M.; Stefansen, S.; Steiner, T.J.; Ashina, M. Characterizing healthcare utilization patterns in a Danish population with headache: Results from the nationwide headache in Denmark (HINDER) panel. J. Headache Pain 2023, 24, 18. [Google Scholar] [CrossRef] [PubMed]
- Olesen, A.; Schytz, H.W.; Ostrowski, S.R.; Topholm, M.; Nielsen, K.; Erikstrup, C.; Mikkelsen, S.; Pedersen, O.B.; Olesen, J.; Hansen, T.F.; et al. Low adherence to the guideline for the acute treatment of migraine. Sci. Rep. 2022, 12, 8487. [Google Scholar] [CrossRef] [PubMed]
- Le, H.; Tfelt-Hansen, P.; Skytthe, A.; Kyvik, K.O.; Olesen, J. Association between migraine, lifestyle and socioeconomic factors: A population-based cross-sectional study. J. Headache Pain 2011, 12, 157–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flachs, E.M.E.L.; Koch, M.B.; Ryd, J.T.; Dibba, E.; Skov-Ettrup, L.; Juel, K. Statens Institut for Folkesundhed, Syddansk Universitet. In Sygdomsbyrden i Danmark—Sygdomme. København: Sundhedsstyrelsen; Danish Health Authority: København, Denmark, 2015; p. 384. [Google Scholar]
- Vetvik, K.G.; Macgregor, E.A.; Lundqvist, C.; Russell, M.B. Prevalence of menstrual migraine: A population-based study. Cephalalgia 2014, 34, 280–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gelinas, L.; Pierce, R.; Winkler, S.; Cohen, I.G.; Lynch, H.F.; Bierer, B.E. Using Social Media as a Research Recruitment Tool: Ethical Issues and Recommendations. Am. J. Bioeth. 2017, 17, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Arigo, D.; Pagoto, S.; Carter-Harris, L.; Lillie, S.E.; Nebeker, C. Using social media for health research: Methodological and ethical considerations for recruitment and intervention delivery. Digit. Health 2018, 4, 2055207618771757. [Google Scholar] [CrossRef] [Green Version]
- Kuruvilla, D.E.; Mehta, A.; Ravishankar, N.; Cowan, R.P. A patient perspective of complementary and integrative medicine (CIM) for migraine treatment: A social media survey. BMC Complement. Med. Ther. 2021, 21, 58. [Google Scholar] [CrossRef]
- Egan, K.G.; Israel, J.S.; Ghasemzadeh, R.; Afifi, A.M. Evaluation of Migraine Surgery Outcomes through Social Media. Plast. Reconstr. Surg. Glob. Open 2016, 4, e1084. [Google Scholar] [CrossRef]
- Subbiah, V. The next generation of evidence-based medicine. Nat. Med. 2023, 29, 49–58. [Google Scholar] [CrossRef]
- Morgan, G.; Agarwal, N.; Choueiri, T.K.; Dizon, D.S.; Hamilton, E.P.; Markham, M.J.; Lewis, M.; Prowell, T.M.; Rugo, H.S.; Subbiah, V.; et al. The (R)evolution of Social Media in Oncology: Engage, Enlighten, and Encourage. Cancer Discov. 2022, 12, 1620–1624. [Google Scholar] [CrossRef] [PubMed]
- Kepios. Digital 2022: Denmark. Available online: https://datareportal.com/reports/digital-2022-denmark (accessed on 22 March 2022).
- Stewart, W.F.; Wood, C.; Reed, M.L.; Roy, J.; Lipton, R.B. Cumulative lifetime migraine incidence in women and men. Cephalalgia 2008, 28, 1170–1178. [Google Scholar] [CrossRef] [PubMed]
- Ashina, M.; Katsarava, Z.; Do, T.P.; Buse, D.C.; Pozo-Rosich, P.; Özge, A.; Krymchantowski, A.V.; Lebedeva, E.R.; Ravishankar, K.; Yu, S.; et al. Migraine: Epidemiology and systems of care. Lancet 2021, 397, 1485–1495. [Google Scholar] [CrossRef] [PubMed]
- Sacco, S.; Lampl, C.; Amin, F.M.; Braschinsky, M.; Deligianni, C.; Uludüz, D.; Versijpt, J.; Ducros, A.; Gil-Gouveia, R.; Katsarava, Z.; et al. European Headache Federation (EHF) consensus on the definition of effective treatment of a migraine attack and of triptan failure. J. Headache Pain 2022, 23, 133. [Google Scholar] [CrossRef] [PubMed]
- Viana, M.; Khaliq, F.; Zecca, C.; Figuerola, M.D.L.; Sances, G.; Di Piero, V.; Petolicchio, B.; Alessiani, M.; Geppetti, P.; Lupi, C.; et al. Poor patient awareness and frequent misdiagnosis of migraine: Findings from a large transcontinental cohort. Eur. J. Neurol. 2020, 27, 536–541. [Google Scholar] [CrossRef] [Green Version]
- Parikh, S.K.; Young, W.B. Migraine: Stigma in Society. Curr. Pain Headache Rep. 2019, 23, 8. [Google Scholar] [CrossRef]
- Gross, E.; Ruiz de la Torre, E.; Martelletti, P. The Migraine Stigma Kaleidoscope View. Neurol. Ther. 2023, 12, 703–709. [Google Scholar] [CrossRef]
- Johnston-Robledo, I.; Chrisler, J.C. The Menstrual Mark: Menstruation as Social Stigma. In The Palgrave Handbook of Critical Menstruation Studies; Bobel, C., Winkler, I.T., Fahs, B., Hasson, K.A., Kissling, E.A., Roberts, T.A., Eds.; Palgrave Macmillan: Singapore, 2020; pp. 181–199. [Google Scholar]
- Zhang, L.; Losin, E.A.R.; Ashar, Y.K.; Koban, L.; Wager, T.D. Gender Biases in Estimation of Others’ Pain. J. Pain 2021, 22, 1048–1059. [Google Scholar] [CrossRef]
- Itani, R.; Soubra, L.; Karout, S.; Rahme, D.; Karout, L.; Khojah, H.M.J. Primary Dysmenorrhea: Pathophysiology, Diagnosis, and Treatment Updates. Korean J. Fam. Med. 2022, 43, 101–108. [Google Scholar] [CrossRef]
- Chen, C.X.; Shieh, C.; Draucker, C.B.; Carpenter, J.S. Reasons women do not seek health care for dysmenorrhea. J. Clin. Nurs. 2018, 27, e301–e308. [Google Scholar] [CrossRef] [Green Version]
- Davidsson, O.B.; Olofsson, I.A.; Kogelman, L.J.; Andersen, M.A.; Rostgaard, K.; Hjalgrim, H.; Olesen, J.; Hansen, T.F. Twenty-five years of triptans—A nationwide population study. Cephalalgia 2021, 41, 894–904. [Google Scholar] [CrossRef]
- Sheftell, F.D.; Tepper, S.J.; Bigal, M.E. Migraine: Barriers for care. Neurol. Sci. 2005, 26, s140–s142. [Google Scholar] [CrossRef] [PubMed]
- Saffi, H.; Do, T.P.; Hansen, J.M.; Dodick, D.W.; Ashina, M. The migraine landscape on YouTube: A review of YouTube as a source of information on migraine. Cephalalgia 2020, 40, 1363–1369. [Google Scholar] [CrossRef] [PubMed]
- Santana, S.; Brach, C.; Harris, L.; Ochiai, E.; Blakey, C.; Bevington, F.; Kleinman, D.; Pronk, N. Updating Health Literacy for Healthy People 2030: Defining Its Importance for a New Decade in Public Health. J. Public Health Manag. Pract. 2021, 27, S258–S264. [Google Scholar] [CrossRef] [PubMed]
- MacGregor, E.A. Menstrual migraine. Curr. Opin. Neurol. 2008, 21, 309–315. [Google Scholar] [CrossRef]
- Stewart, W.F.; Lipton, R.B.; Kolodner, K.B.; Sawyer, J.; Lee, C.; Liberman, J.N. Validity of the Migraine Disability Assessment (MIDAS) score in comparison to a diary-based measure in a population sample of migraine sufferers. Pain 2000, 88, 41–52. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of responses. MM: menstrual migraine; nMM: non-menstrual migraine; pMM: probable menstrual migraine.
Figure 1.
Flowchart of responses. MM: menstrual migraine; nMM: non-menstrual migraine; pMM: probable menstrual migraine.

Figure 2.
Age categories of respondents fulfilling and not fulfilling ICHD-3 criteria for MM. MM: menstrual migraine; nMM: non-menstrual migraine; pMM: probable menstrual migraine.
Figure 2.
Age categories of respondents fulfilling and not fulfilling ICHD-3 criteria for MM. MM: menstrual migraine; nMM: non-menstrual migraine; pMM: probable menstrual migraine.

Figure 3.
Days missed during last 3 months due to menstrual migraine or headache: (a) school or work; (b) family, social, and leisure activities. MM: menstrual migraine; nMM: non-menstrual migraine; pMM: probable menstrual migraine.
Figure 3.
Days missed during last 3 months due to menstrual migraine or headache: (a) school or work; (b) family, social, and leisure activities. MM: menstrual migraine; nMM: non-menstrual migraine; pMM: probable menstrual migraine.

Figure 4.
Health-care seeking behavior of women with MM. MM: menstrual migraine; OTC: over-the-counter.
Figure 4.
Health-care seeking behavior of women with MM. MM: menstrual migraine; OTC: over-the-counter.

Figure 5.
Treatment of MM. MM: menstrual migraine; OTC: over-the-counter.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chalmer, M.A.; Lønberg, U.S. Health-Care Seeking Behavior and Treatment of Menstrual Migraine among Danish Women—A Social Media Study. Women 2023, 3, 385-395. https://0-doi-org.brum.beds.ac.uk/10.3390/women3030029
AMA Style
Chalmer MA, Lønberg US. Health-Care Seeking Behavior and Treatment of Menstrual Migraine among Danish Women—A Social Media Study. Women. 2023; 3(3):385-395. https://0-doi-org.brum.beds.ac.uk/10.3390/women3030029
Chicago/Turabian StyleChalmer, Mona Ameri, and Ulla Sofie Lønberg. 2023. "Health-Care Seeking Behavior and Treatment of Menstrual Migraine among Danish Women—A Social Media Study" Women 3, no. 3: 385-395. https://0-doi-org.brum.beds.ac.uk/10.3390/women3030029