
The Prognostic Value of the De Ritis Ratio for Progression-Free Survival in Patients with NET Undergoing [177Lu]Lu-DOTATOC-PRRT: A Retrospective Analysis

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patients
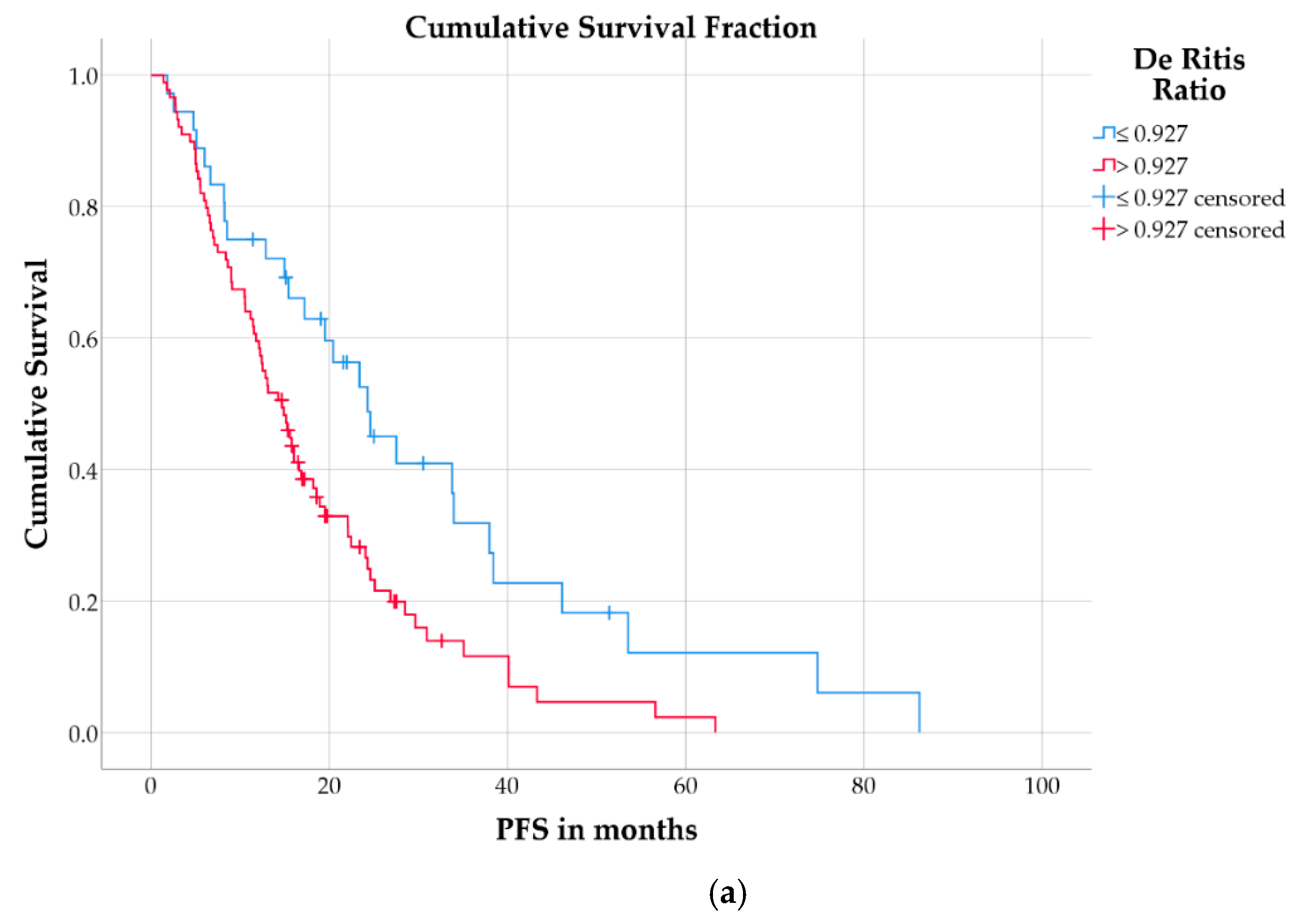
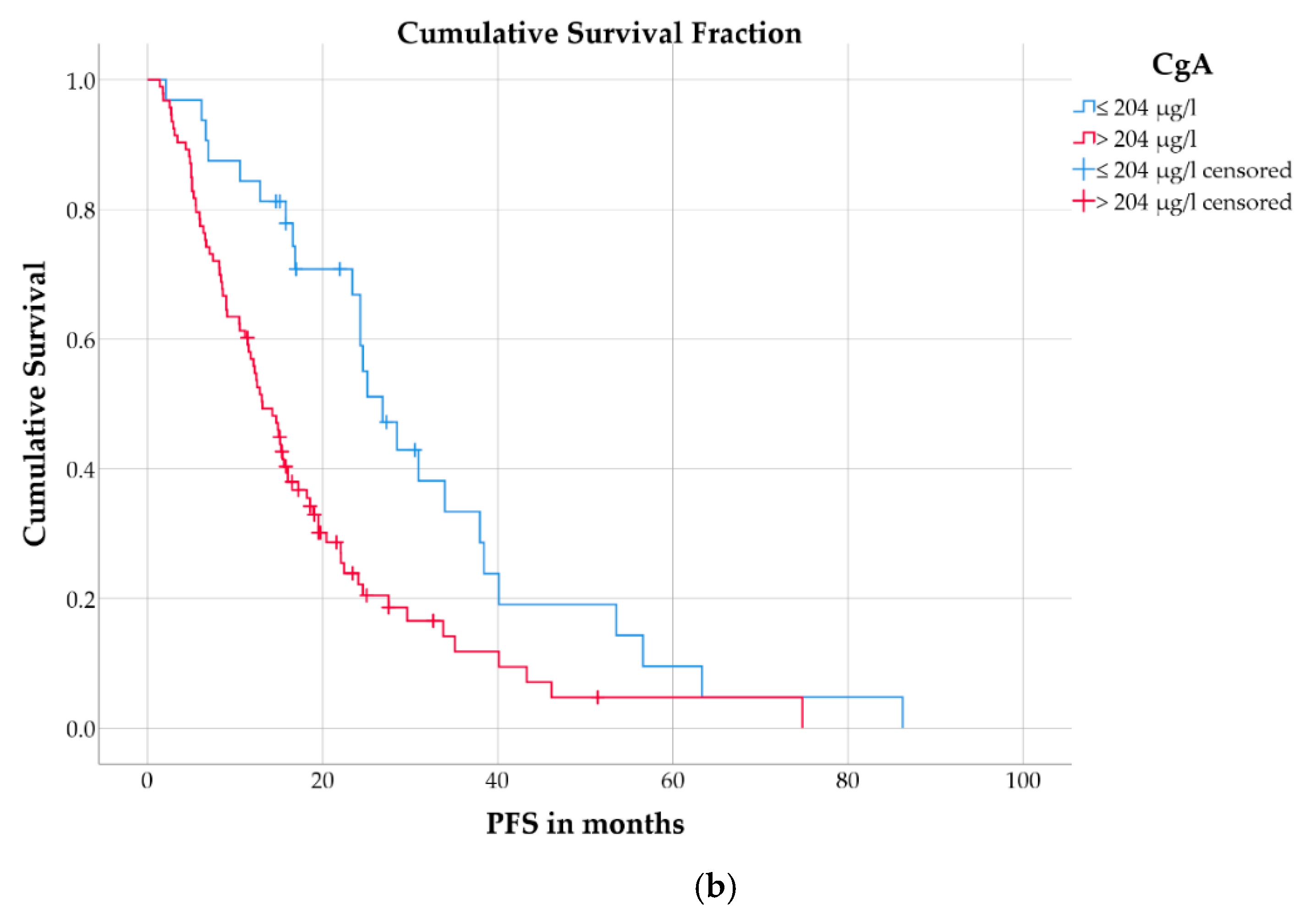
2.2. Progression Free Survival
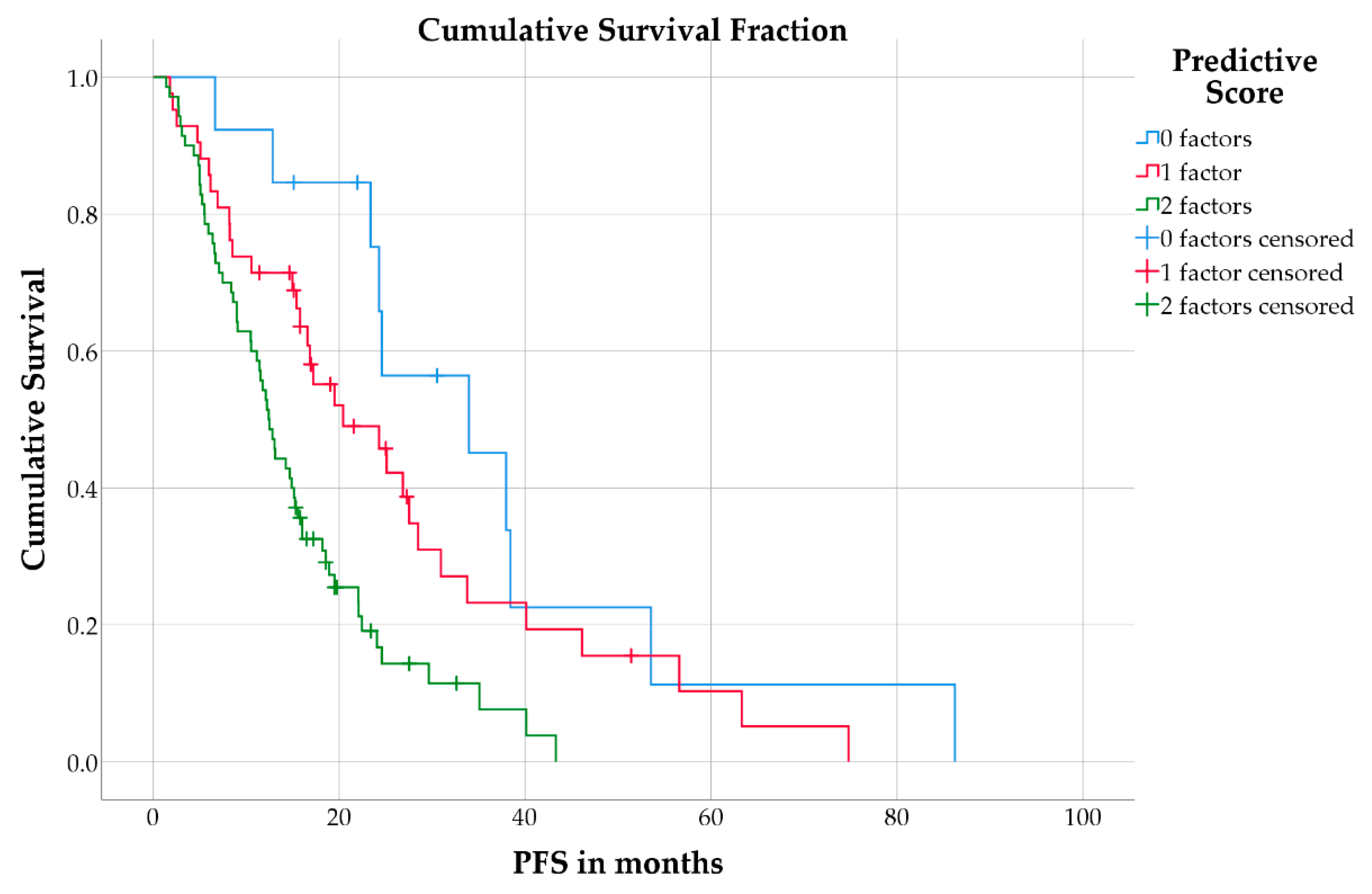
2.3. Predictive Model for Progression-Free Survival
3. Discussion
4. Materials and Methods
4.1. Patient Population
4.2. [177Lu]Lu-DOTATOC-PRRT and Response Assessment
4.3. Evaluation
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the incidence, prevalence, and survival outcomes in patients with neuroendocrine tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef]
- Huguet, I.; Grossman, A.B.; O’Toole, D. Changes in the epidemiology of neuroendocrine tumours. Neuroendocrinology 2017, 104, 105–111. [Google Scholar] [CrossRef]
- Pavel, M.; O’Toole, D.; Costa, F.; Capdevila, J.; Gross, D.; Kianmanesh, R.; Krenning, E.; Knigge, U.; Salazar, R.; Pape, U.F.; et al. ENETS consensus guidelines update for the management of distant metastatic disease of intestinal, pancreatic, bronchial neuroendocrine neoplasms (NEN) and NEN of unknown primary site. Neuroendocrinology 2016, 103, 172–185. [Google Scholar] [CrossRef]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 trial of (177) Lu-dotatate for midgut neuroendocrine tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Hamiditabar, M.; Ali, M.; Roys, J.; Wolin, E.M.; O’Dorisio, T.M.; Ranganathan, D.; Tworowska, I.; Strosberg, J.R.; Delpassand, E.S. Peptide receptor radionuclide therapy with 177Lu-octreotate in patients with somatostatin receptor expressing neuroendocrine tumors: Six years’ assessment. Clin. Nucl. Med. 2017, 42, 436–443. [Google Scholar] [CrossRef]
- Brabander, T.; van der Zwan, W.A.; Teunissen, J.J.M.; Kam, B.L.R.; Feelders, R.A.; de Herder, W.W.; van Eijck, C.H.J.; Franssen, G.J.H.; Krenning, E.P.; Kwekkeboom, D.J. Long-term efficacy, survival, and safety of [(177) Lu-DOTA (0), Tyr (3)] octreotate in patients with gastroenteropancreatic and bronchial neuroendocrine tumors. Clin. Cancer Res. 2017, 23, 4617–4624. [Google Scholar] [CrossRef] [Green Version]
- Saravana-Bawan, B.; Bajwa, A.; Paterson, J.; McEwan, A.J.B.; McMullen, T.P.W. Efficacy of 177Lu peptide receptor radionuclide therapy for the treatment of neuroendocrine tumors: A meta-analysis. Clin. Nucl. Med. 2019, 44, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Ezziddin, S.; Opitz, M.; Attassi, M.; Biermann, K.; Sabet, A.; Guhlke, S.; Brockmann, H.; Willinek, W.; Wardelmann, E.; Biersack, H.J.; et al. Impact of the Ki-67 proliferation index on response to peptide receptor radionuclide therapy. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 459–466. [Google Scholar] [CrossRef]
- Ezziddin, S.; Attassi, M.; Yong-Hing, C.J.; Ahmadzadehfar, H.; Willinek, W.; Grunwald, F.; Guhlke, S.; Biersack, H.J.; Sabet, A. Predictors of long-term outcome in patients with well-differentiated gastroenteropancreatic neuroendocrine tumors after peptide receptor radionuclide therapy with 177Lu-octreotate. J. Nucl. Med. 2014, 55, 183–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aalbersberg, E.A.; Huizing, D.M.V.; Walraven, I.; de Wit-van der Veen, B.J.; Kulkarni, H.R.; Singh, A.; Stokkel, M.P.M.; Baum, R.P. Parameters to predict progression-free and overall survival after peptide receptor radionuclide therapy: A multivariate analysis in 782 patients. J. Nucl. Med. 2019, 60, 1259–1265. [Google Scholar] [CrossRef] [Green Version]
- Di Giacinto, P.; Rota, F.; Rizza, L.; Campana, D.; Isidori, A.; Lania, A.; Lenzi, A.; Zuppi, P.; Baldelli, R. Chromogranin A: From laboratory to clinical aspects of patients with neuroendocrine tumors. Int. J. Endocrinol. 2018, 2018, 8126087. [Google Scholar] [CrossRef]
- Sabet, A.; Dautzenberg, K.; Haslerud, T.; Aouf, A.; Sabet, A.; Simon, B.; Mayer, K.; Biersack, H.J.; Ezziddin, S. Specific efficacy of peptide receptor radionuclide therapy with (177)Lu-octreotate in advanced neuroendocrine tumours of the small intestine. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1238–1246. [Google Scholar] [CrossRef]
- Sharma, N.; Naraev, B.G.; Engelman, E.G.; Zimmerman, M.B.; Bushnell, D.L., Jr.; O’Dorisio, T.M.; O’Dorisio, M.S.; Menda, Y.; Muller-Brand, J.; Howe, J.R.; et al. Peptide receptor radionuclide therapy outcomes in a North American cohort with metastatic well-differentiated neuroendocrine tumors. Pancreas 2017, 46, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [PubMed]
- Wetz, C.; Rogasch, J.; Genseke, P.; Schatka, I.; Furth, C.; Kreissl, M.; Jann, H.; Venerito, M.; Amthauer, H. Asphericity of somatostatin receptor expression in neuroendocrine tumors: An innovative predictor of outcome in everolimus treatment? Diagnostics 2020, 10, 732. [Google Scholar] [CrossRef] [PubMed]
- Wetz, C.; Genseke, P.; Apostolova, I.; Furth, C.; Ghazzawi, S.; Rogasch, J.M.M.; Schatka, I.; Kreissl, M.C.; Hofheinz, F.; Grosser, O.S.; et al. The association of intra-therapeutic heterogeneity of somatostatin receptor expression with morphological treatment response in patients undergoing PRRT with [177Lu]-DOTATATE. PLoS ONE 2019, 14, e0216781. [Google Scholar] [CrossRef]
- Wetz, C.; Apostolova, I.; Steffen, I.G.; Hofheinz, F.; Furth, C.; Kupitz, D.; Ruf, J.; Venerito, M.; Klose, S.; Amthauer, H. Predictive value of asphericity in pretherapeutic [(111) In] DTPA-octreotide SPECT/CT for response to peptide receptor radionuclide therapy with [(177)Lu] DOTATATE. Mol. Imaging Biol. 2017, 19, 437–445. [Google Scholar] [CrossRef]
- Brunner, P.; Jorg, A.C.; Glatz, K.; Bubendorf, L.; Radojewski, P.; Umlauft, M.; Marincek, N.; Spanjol, P.M.; Krause, T.; Dumont, R.A.; et al. The prognostic and predictive value of sstr2-immunohistochemistry and sstr2-targeted imaging in neuroendocrine tumors. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 468–475. [Google Scholar] [CrossRef] [Green Version]
- Werner, R.A.; Lapa, C.; Ilhan, H.; Higuchi, T.; Buck, A.K.; Lehner, S.; Bartenstein, P.; Bengel, F.; Schatka, I.; Muegge, D.O.; et al. Survival prediction in patients undergoing radionuclide therapy based on intratumoral somatostatin-receptor heterogeneity. Oncotarget 2017, 8, 7039–7049. [Google Scholar] [CrossRef] [Green Version]
- De Ritis, F.; Coltorti, M.; Giusti, G. An enzymic test for the diagnosis of viral hepatitis; the transaminase serum activities. Clin. Chim. Acta 1957, 2, 70–74. [Google Scholar] [CrossRef]
- Bezan, A.; Mrsic, E.; Krieger, D.; Stojakovic, T.; Pummer, K.; Zigeuner, R.; Hutterer, G.C.; Pichler, M. The preoperative AST/ALT (De Ritis) ratio represents a poor prognostic factor in a cohort of patients with nonmetastatic renal cell carcinoma. J. Urol. 2015, 194, 30–35. [Google Scholar] [CrossRef]
- Wang, H.; Fang, K.; Zhang, J.; Jiang, Y.; Wang, G.; Zhang, H.; Chen, T.; Shi, X.; Li, Y.; Duan, F.; et al. The significance of De Ritis (aspartate transaminase/alanine transaminase) ratio in predicting pathological outcomes and prognosis in localized prostate cancer patients. Int. Urol. Nephrol. 2017, 49, 1391–1398. [Google Scholar] [CrossRef] [PubMed]
- Ha, Y.S.; Kim, S.W.; Chun, S.Y.; Chung, J.W.; Choi, S.H.; Lee, J.N.; Kim, B.S.; Kim, H.T.; Yoo, E.S.; Kwon, T.G.; et al. Association between De Ritis ratio (aspartate aminotransferase/alanine aminotransferase) and oncological outcomes in bladder cancer patients after radical cystectomy. BMC Urol. 2019, 19, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, X.; Yang, W.X.; Wang, Y.; Shao, Y.X.; Xiong, S.C.; Li, X. The prognostic value of De Ritis (AST/ALT) ratio in patients after surgery for urothelial carcinoma: A systematic review and meta-analysis. Cancer Cell. Int. 2020, 20, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riedl, J.; Posch, F.; Prager, G.; Eisterer, W.; Öhler, L.; Thamer, S.; Wilthoner, K.; Petzer, A.; Pichler, P.; Hubmann, E.; et al. The AST/ALT (De Ritis) ratio predicts clinical outcome in pancreatic cancer patients treated with first-line nab-paclitaxel and gemcitabine: Post-hoc analysis of an Austrian multicenter, non-interventional study. Annals Oncol. 2019, 30, iv78. [Google Scholar] [CrossRef]
- Wu, J.; Li, S.; Wang, Y.; Hu, L. Pretreatment Aspartate Aminotransferase-to-Alanine Aminotransferase (De Ritis) Ratio Predicts the Prognosis of Nonmetastatic Nasopharyngeal Carcinoma. Onco. Targets Ther. 2019, 12, 10077–10087. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Lee, S.E.; Byun, S.S.; Kim, H.H.; Kwak, C.; Hong, S.K. De Ritis ratio (aspartate transaminase/alanine transaminase ratio) as a significant prognostic factor after surgical treatment in patients with clear-cell localized renal cell carcinoma: A propensity score-matched study. BJU Int. 2017, 119, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, T.; Ishihara, H.; Takagi, T.; Fukuda, H.; Yoshida, K.; Iizuka, J.; Kobayashi, H.; Okumi, M.; Ishida, H.; Kondo, T.; et al. The De Ritis (Aspartate transaminase/Alanine transaminase) ratio as a prognosticator in patients with end-stage renal disease-associated Renal Cell Carcinoma. Clin. Genitourin. Cancer 2020, 18, 236–240.e231. [Google Scholar] [CrossRef]
- Yuk, H.D.; Jeong, C.W.; Kwak, C.; Kim, H.H.; Ku, J.H. De Ritis ratio (A. transaminase/A. transaminase) as a significant prognostic factor in patients undergoing radical cystectomy with bladder urothelial carcinoma: A propensity score-matched study. Dis. Markers 2019, 2019, 6702964. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Chen, L.; Wang, Y.; Tan, W.; Huang, Z. Prognostic value of aspartate transaminase to alanine transaminase (De Ritis) ratio in solid tumors: A pooled analysis of 9,400 patients. Oncol. Targets Ther. 2019, 12, 5201–5213. [Google Scholar] [CrossRef] [Green Version]
- Botros, M.; Sikaris, K.A. The de ritis ratio: The test of time. Clin. Biochem. Rev. 2013, 34, 117–130. [Google Scholar] [PubMed]
- Feldstein, A.E.; Canbay, A.; Angulo, P.; Taniai, M.; Burgart, L.J.; Lindor, K.D.; Gores, G.J. Hepatocyte apoptosis and fas expression are prominent features of human nonalcoholic steatohepatitis. Gastroenterology 2003, 125, 437–443. [Google Scholar] [CrossRef]
- Lofthus, D.M.; Stevens, S.R.; Armstrong, P.W.; Granger, C.B.; Mahaffey, K.W. Pattern of liver enzyme elevations in acute ST-elevation myocardial infarction. Coron Artery Dis. 2012, 23, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Mori, K.; Janisch, F.; Mostafaei, H.; Kimura, S.; Lysenko, I.; Karakiewicz, P.I.; Briganti, A.; Enikeev, D.V.; Roupret, M.; Margulis, V.; et al. Prognostic role of preoperative De Ritis ratio in upper tract urothelial carcinoma treated with nephroureterectomy. Urol. Oncol. 2020, 38, e601–617.e624. [Google Scholar] [CrossRef]
- Warburg, O. On the origin of cancer cells. Science 1956, 123, 309–314. [Google Scholar] [CrossRef]
- Hsu, P.P.; Sabatini, D.M. Cancer cell metabolism: Warburg and beyond. Cell 2008, 134, 703–707. [Google Scholar] [CrossRef] [Green Version]
- Fantin, V.R.; St-Pierre, J.; Leder, P. Attenuation of LDH-A expression uncovers a link between glycolysis, mitochondrial physiology, and tumor maintenance. Cancer Cell 2006, 9, 425–434. [Google Scholar] [CrossRef] [Green Version]
- Greenhouse, W.V.; Lehninger, A.L. Occurrence of the malate-aspartate shuttle in various tumor types. Cancer Res. 1976, 36, 1392–1396. [Google Scholar]
- Thornburg, J.M.; Nelson, K.K.; Clem, B.F.; Lane, A.N.; Arumugam, S.; Simmons, A.; Eaton, J.W.; Telang, S.; Chesney, J. Targeting aspartate aminotransferase in breast cancer. Breast Cancer Res. 2008, 10, R84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, J.C.; Pavel, M.; Phan, A.T.; Kulke, M.H.; Hoosen, S.; St Peter, J.; Cherfi, A.; Oberg, K.E. Chromogranin A and neuron-specific enolase as prognostic markers in patients with advanced pNET treated with everolimus. J. Clin. Endocrinol. Metab. 2011, 96, 3741–3749. [Google Scholar] [CrossRef] [Green Version]
- Marotta, V.; Zatelli, M.C.; Sciammarella, C.; Ambrosio, M.R.; Bondanelli, M.; Colao, A.; Faggiano, A. Chromogranin A as circulating marker for diagnosis and management of neuroendocrine neoplasms: More flaws than fame. Endocr. Relat. Cancer 2018, 25, R11–R29. [Google Scholar] [CrossRef]
- Brabander, T.; van der Zwan, W.A.; Teunissen, J.J.M.; Kam, B.L.R.; de Herder, W.W.; Feelders, R.A.; Krenning, E.P.; Kwekkeboom, D.J. Pitfalls in the response evaluation after peptide receptor radionuclide therapy with [(177)Lu-DOTA(0),Tyr(3)]octreotate. Endocr. Relat. Cancer 2017, 24, 243–251. [Google Scholar] [CrossRef] [Green Version]
- Baum, R.P.; Kluge, A.W.; Kulkarni, H.; Schorr-Neufing, U.; Niepsch, K.; Bitterlich, N.; van Echteld, C.J. [(177)Lu-DOTA](0)-D-Phe(1)-Tyr(3)-octreotide ((177)Lu-DOTATOC) for peptide receptor radiotherapy in patients with advanced neuroendocrine tumours: A phase-II study. Theranostics 2016, 6, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Biondi-Zoccai, G.; Romagnoli, E.; Agostoni, P.; Capodanno, D.; Castagno, D.; D’Ascenzo, F.; Sangiorgi, G.; Modena, M.G. Are propensity scores really superior to standard multivariable analysis? Contemp. Clin. Trials 2011, 32, 731–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brazauskas, R.; Logan, B.R. Observational studies: Matching or regression? Biol. Blood Marrow Transplant. 2016, 22, 557–563. [Google Scholar] [CrossRef] [Green Version]
- Ballman, K.V. Biomarker: Predictive or prognostic? J. Clin. Oncol. 2015, 33, 3968–3971. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern cooperative oncology group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Benslama, N.; Bollard, J.; Vercherat, C.; Massoma, P.; Roche, C.; Hervieu, V.; Peron, J.; Lombard-Bohas, C.; Scoazec, J.Y.; Walter, T. Prediction of response to everolimus in neuroendocrine tumors: Evaluation of clinical, biological and histological factors. Investig. New Drugs 2016, 34, 654–662. [Google Scholar] [CrossRef]
- Budczies, J.; Klauschen, F.; Sinn, B.V.; Gyorffy, B.; Schmitt, W.D.; Darb-Esfahani, S.; Denkert, C. Cutoff Finder: A comprehensive and straightforward Web application enabling rapid biomarker cutoff optimization. PLoS ONE 2012, 7, e51862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrell, F.E., Jr.; Lee, K.L.; Mark, D.B. Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n (%) or Median (Range) | p | ||
|---|---|---|---|---|
| Total Cohort | De Ritis Ratio Low | De Ritis Ratio High | ||
| Patient count | 125 | 36 | 89 | |
| Age in years | 66 (35–87) | 59 (37–80) | 69 (35–87) | <0.001 |
| Age >66 years | 65 (52%) | 8 (22%) | 57 (64%) | <0.001 |
| Age ≤66 years | 60 (48%) | 28 (78%) | 32 (36%) | |
| Sex | 0.42 | |||
| Men | 79 (63%) | 25 (69%) | 54 (61%) | |
| Women | 46 (37%) | 11 (31%) | 35 (39%) | |
| ECOG score | 0.68 | |||
| 0 | 90 (72%) | 28 (78%) | 62 (70%) | |
| 1 | 33 (26%) | 8 (22%) | 25 (28%) | |
| 2 | 2 (2%) | - | 2 (2%) | |
| Charlson comorbidity index (CCI) | 1 (0–7) | 1 (0–7) | 1 (0–6) | 0.94 |
| Primary location | 0.57 | |||
| Gastrointestinal | 64 (51%) | 22 (61%) | 42 (47%) | |
| Pancreatic | 30 (24%) | 8 (22%) | 22 (25%) | |
| Pulmonal | 11 (9%) | 2 (6%) | 9 (10%) | |
| CUP | 20 (16%) | 4 (11%) | 16 (18%) | |
| Metastatic disease | 124 (99%) | 36 (100%) | 88 (99%) | |
| Metastatic spread | ||||
| Hepatic | 119 (95%) | 32 (89%) | 87 (98%) | 0.057 |
| Lymphonodal | 104 (83%) | 25 (69%) | 79 (89%) | 0.016 |
| Osseous | 51 (41%) | 12 (33%) | 39 (44%) | 0.32 |
| Peritoneal | 24 (19%) | 4 (11%) | 20 (23%) | 0.21 |
| Pulmonal | 6 (5%) | 2 (6%) | 4 (5%) | 1.0 |
| Functional tumor | 42 (34%) | 11 (31%) | 31 (35%) | 0.68 |
| Hedinger syndrome | 5 (4%) | 1 (3%) | 4 (5%) | 1.0 |
| Grading | 0.65 | |||
| G1 | 24 (19%) | 5 (14%) | 19 (21%) | |
| G2 | 95 (76%) | 29 (81%) | 66 (74%) | |
| G3 | 6 (5%) | 2 (6%) | 4 (5%) | |
| Laboratory parameters | ||||
| Chromogranin A in μg/L | 612 (14–601,700) | 355 (14–5283) | 751 (38–601,700) | 0.027 |
| Chromogranin A >204 μg/L | 93 (74%) | 23 (64%) | 70 (79%) | 0.11 |
| Chromogranin A ≤204 μg/L | 32 (26%) | 13 (36%) | 19 (21%) | |
| AST in U/L | 29 (13–139) | 30 (20–84) | 28 (13–139) | 0.34 |
| ALT in U/L | 28 (10–132) | 46 (23–122) | 23 (10–132) | <0.001 |
| De Ritis ratio | 1.09 (0.46–2.87) | 0.74 (0.46–0.93) | 1.23 (0.93–2.87) | |
| Number of PRRT cycles | 3 (1–6) | 3 (1–5) | 3 (1–6) | 0.084 |
| Previous treatment | ||||
| Operative resection | 78 (62%) | 22 (61%) | 56 (63%) | 0.84 |
| Somatostatin analogues | 87 (70%) | 20 (56%) | 67 (75%) | 0.034 |
| mTOR inhibitor | 24 (19%) | 9 (25%) | 15 (17%) | 0.32 |
| Tyrosine kinase inhibitor | 7 (6%) | 3 (8%) | 4 (5%) | 0.41 |
| Chemotherapy | 38 (30%) | 10 (28%) | 28 (32%) | 0.83 |
| Local ablative therapy | 10 (8%) | 2 (6%) | 8 (9%) | 0.72 |
| Radiation therapy | 6 (5%) | 1 (3%) | 5 (6%) | 0.67 |
| Transcatheter arterial chemoembolization | 9 (7%) | 3 (8%) | 6 (7%) | 0.72 |
| Univariable Cox Regression | Multivariable Cox Regression | |||||
|---|---|---|---|---|---|---|
| Variable | Hazard Ratio | 95% Confidence Interval | p-Value | Hazard Ratio | 95% Confidence Interval | p-Value |
| Age (>66 years) | 1.46 | 0.98–2.18 | 0.061 | 0.97 | 0.61–1.53 | 0.89 |
| Sex (male) | 0.82 | 0.55–1.22 | 0.32 | - | - | - |
| ECOG score | - | - | 0.074 | - | - | 0.22 |
| 0 | reference | reference | ||||
| 1 | 1.41 | 0.89–2.24 | 0.14 | 1.32 | 0.81–2.14 | 0.27 |
| 2 | 4.0 | 0.95–16.84 | 0.059 | 3.08 | 0.70–13.48 | 0.14 |
| Charlson comorbidity index (CCI) | 0.93 | 0.81–1.07 | 0.33 | - | - | - |
| Primary tumor location | - | - | 0.014 | - | - | 0.09 |
| Gastrointestinal | reference | reference | ||||
| Pancreatic | 1.8 | 1.11–2.94 | 0.018 | 1.51 | 0.92–2.47 | 0.11 |
| Pulmonary | 2.62 | 1.30–5.28 | 0.007 | 1.81 | 0.88–3.72 | 0.10 |
| CUP | 1.08 | 0.61–1.94 | 0.79 | 0.79 | 0.43–1.46 | 0.45 |
| Metastatic spread | ||||||
| Hepatic | 0.59 | 0.26–1.35 | 0.21 | - | - | - |
| Lymphonodal | 1.33 | 0.74–2.40 | 0.34 | - | - | - |
| Osseous | 0.93 | 0.62–1.39 | 0.72 | - | - | - |
| Peritoneal | 1.17 | 0.73–1.87 | 0.51 | - | - | - |
| Pulmonary | 1.05 | 0.43–2.58 | 0.92 | - | - | - |
| Functionality | 0.83 | 0.55–1.26 | 0.39 | - | - | - |
| Hedinger syndrome | 1.35 | 0.55–3.33 | 0.52 | - | - | - |
| De Ritis ratio (>0.927) | 1.89 | 1.19–3.0 | 0.007 | 1.7 | 1.01–2.86 | 0.047 |
| CgA (>204 μg/L) | 2.16 | 1.35–3.46 | 0.001 | 2.05 | 1.24–3.39 | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruhwedel, T.; Rogasch, J.M.M.; Huang, K.; Jann, H.; Schatka, I.; Furth, C.; Amthauer, H.; Wetz, C. The Prognostic Value of the De Ritis Ratio for Progression-Free Survival in Patients with NET Undergoing [177Lu]Lu-DOTATOC-PRRT: A Retrospective Analysis. Cancers 2021, 13, 635. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040635
Ruhwedel T, Rogasch JMM, Huang K, Jann H, Schatka I, Furth C, Amthauer H, Wetz C. The Prognostic Value of the De Ritis Ratio for Progression-Free Survival in Patients with NET Undergoing [177Lu]Lu-DOTATOC-PRRT: A Retrospective Analysis. Cancers. 2021; 13(4):635. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040635
Chicago/Turabian StyleRuhwedel, Tristan, Julian M. M. Rogasch, Kai Huang, Henning Jann, Imke Schatka, Christian Furth, Holger Amthauer, and Christoph Wetz. 2021. "The Prognostic Value of the De Ritis Ratio for Progression-Free Survival in Patients with NET Undergoing [177Lu]Lu-DOTATOC-PRRT: A Retrospective Analysis" Cancers 13, no. 4: 635. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040635