


Effect of Electrodeposited Gold Coatings on Micro-Gaps, Surface Profile and Bacterial Leakage of Cast UCLA Abutments Attached to External Hexagon Dental Implants
Abstract
:1. Introduction
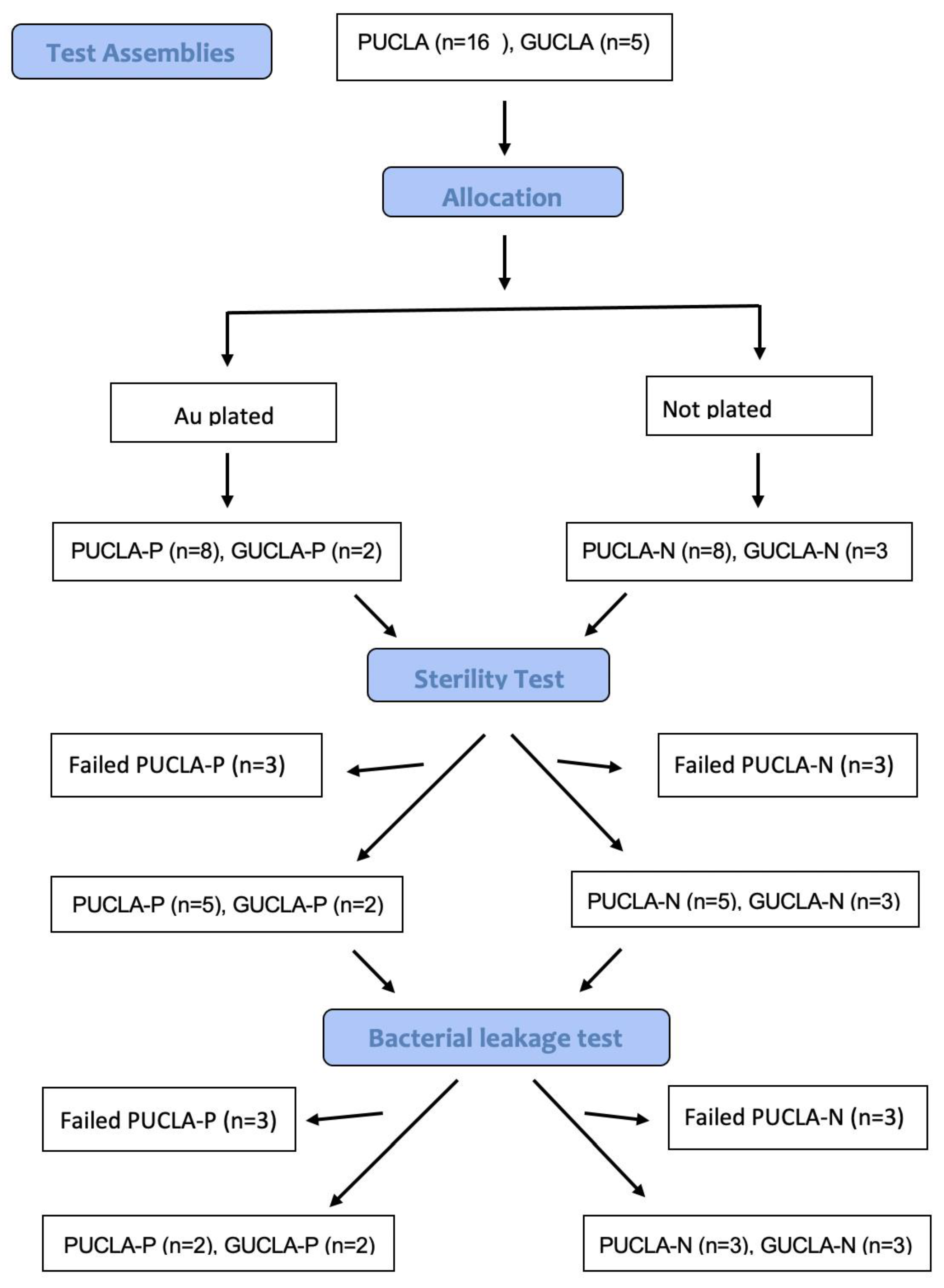
2. Materials and Methods
2.1. Abutment Preparation
2.2. SEM Evaluation of External Perimeter Micro-Gaps
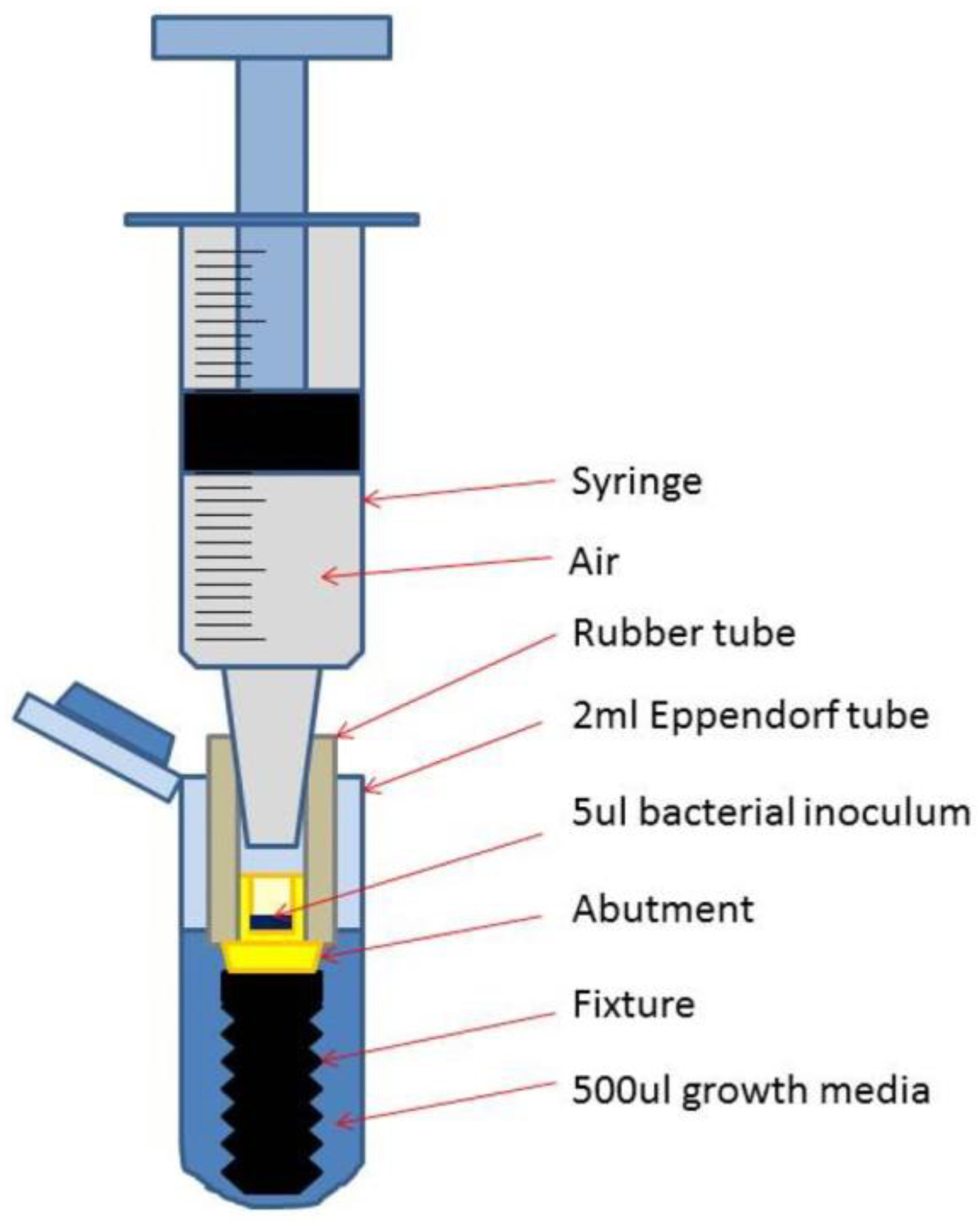
2.3. Micro-Gap Leakage Test
3. Results
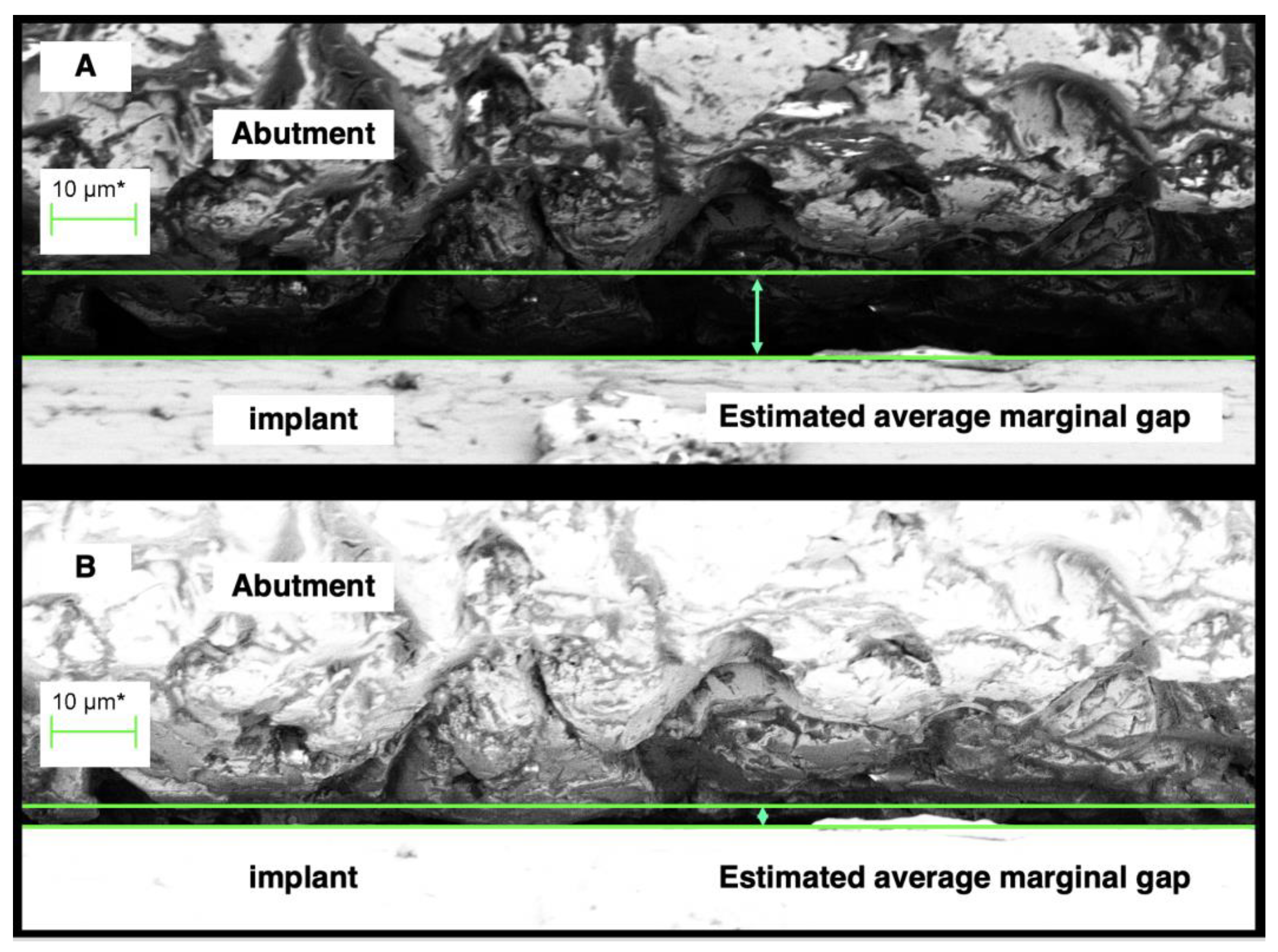
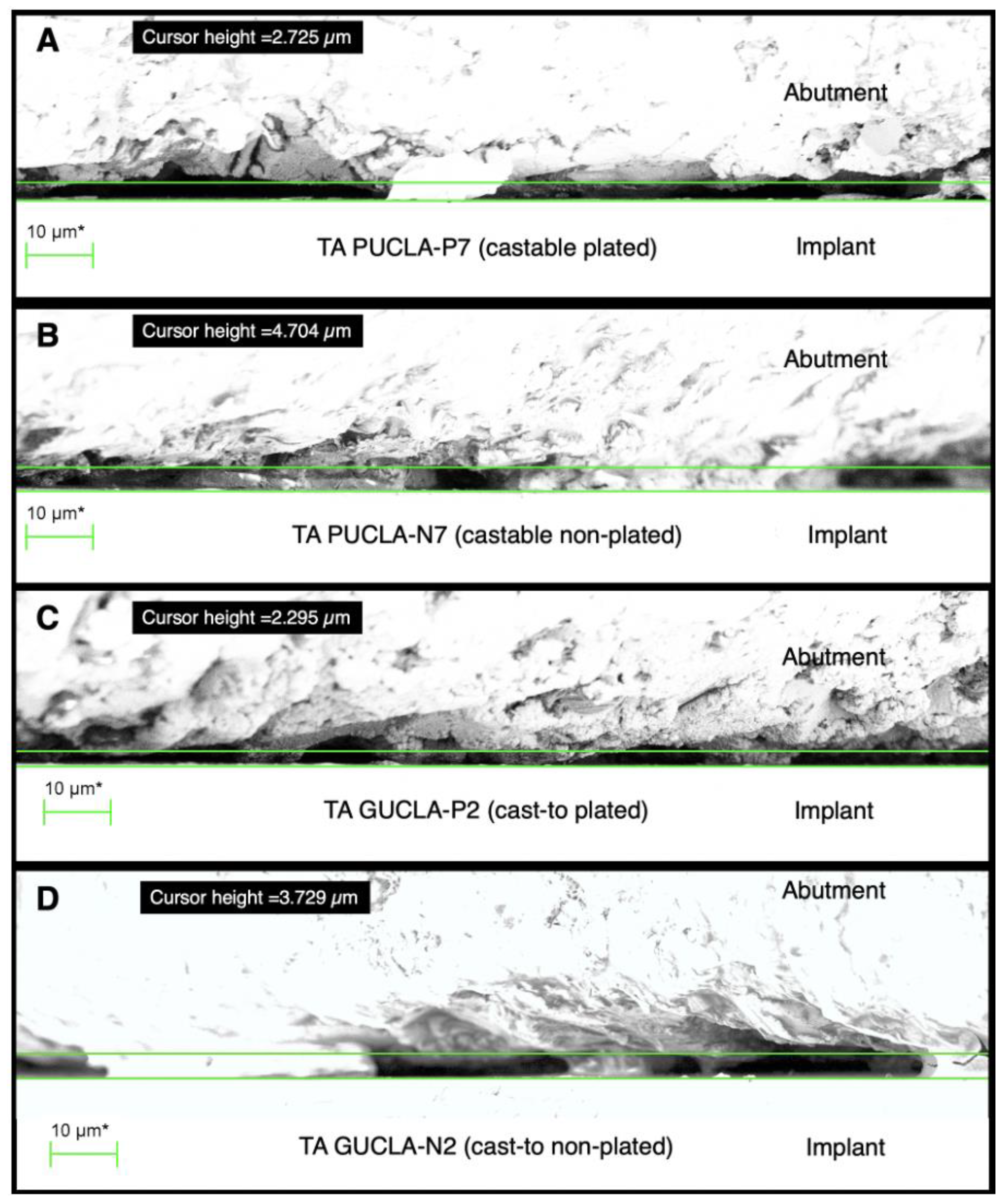
3.1. SEM Evaluation of External Perimeter Micro-Gaps
3.2. Micro-Gap Leakage Test
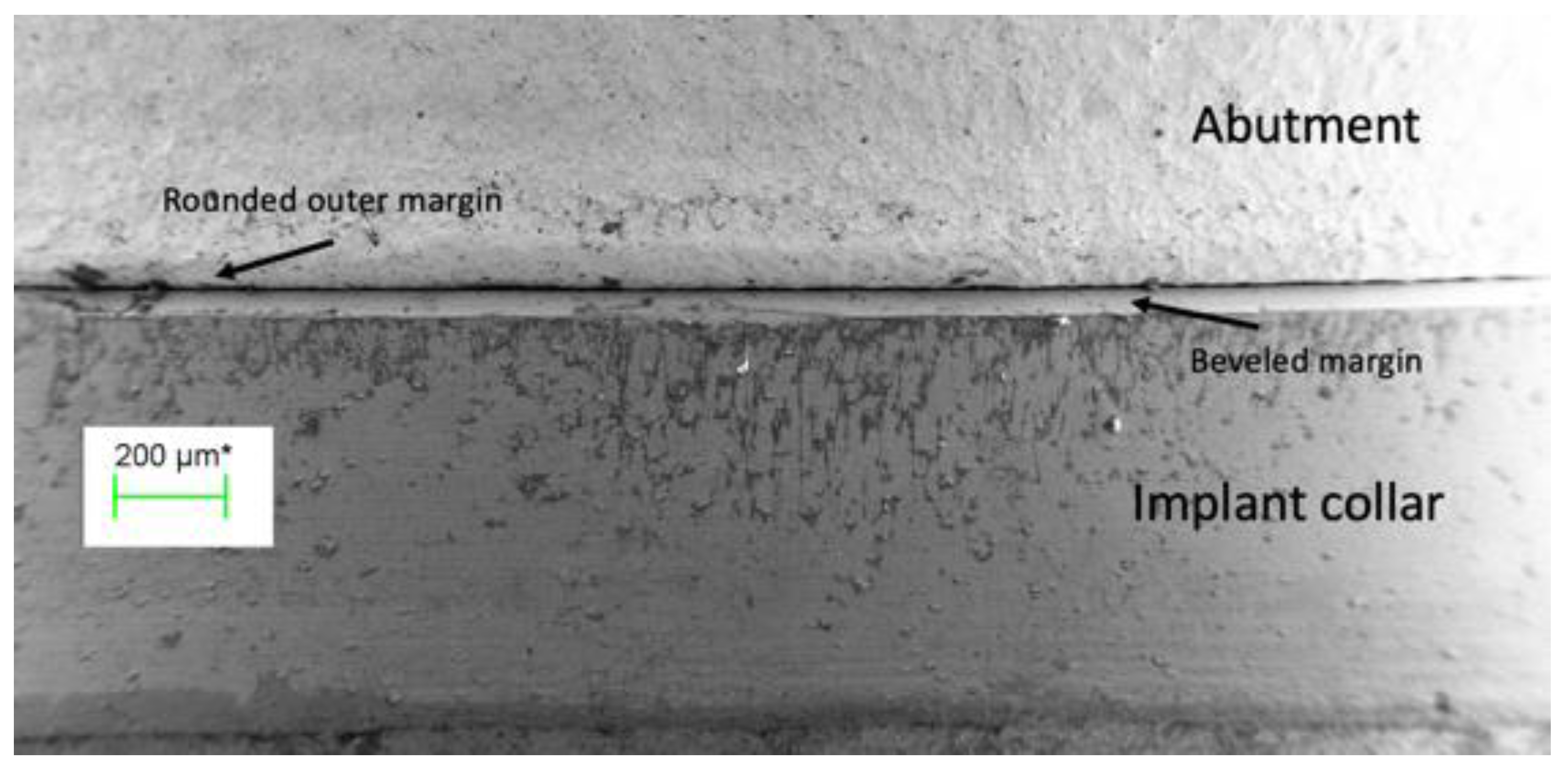
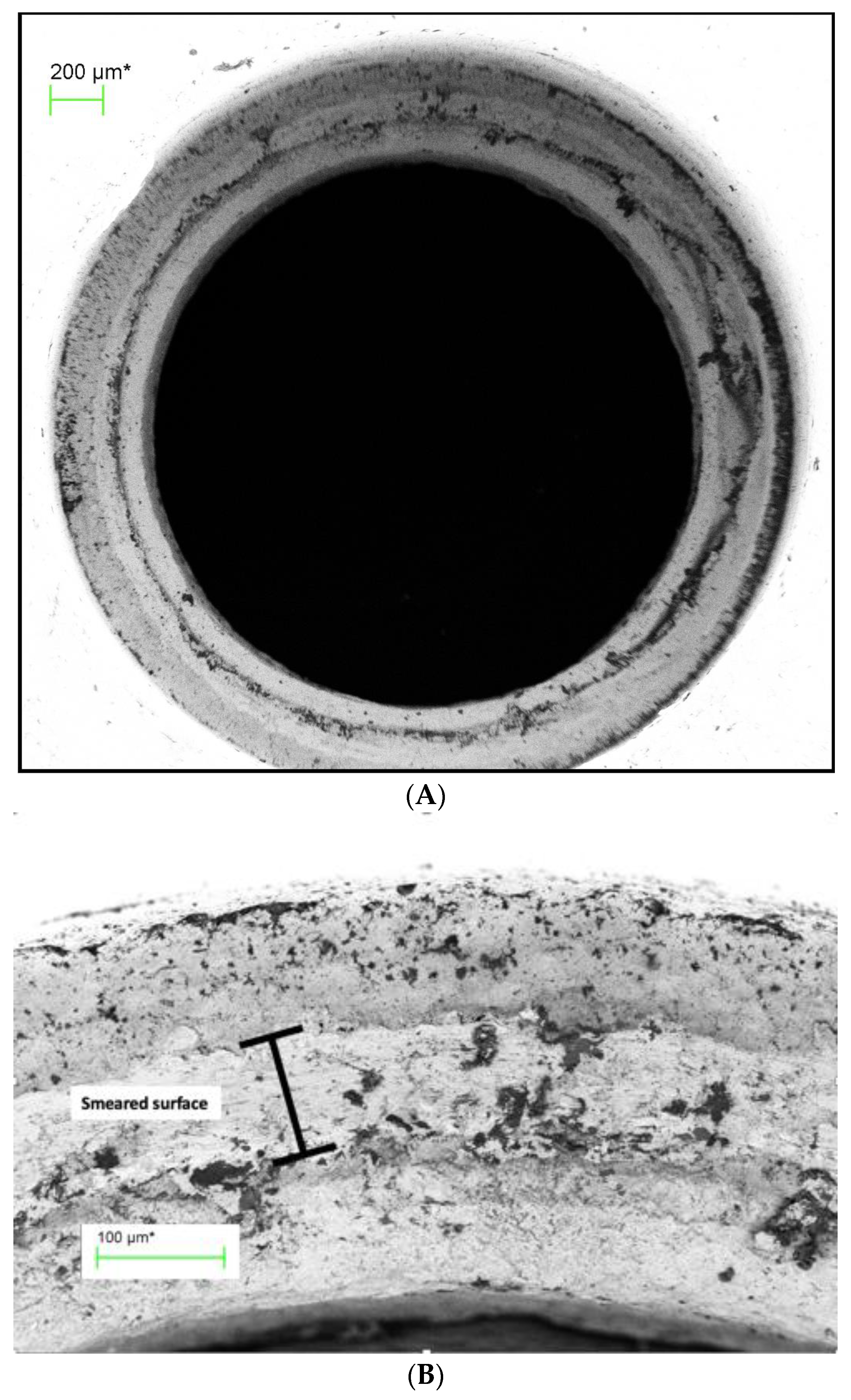
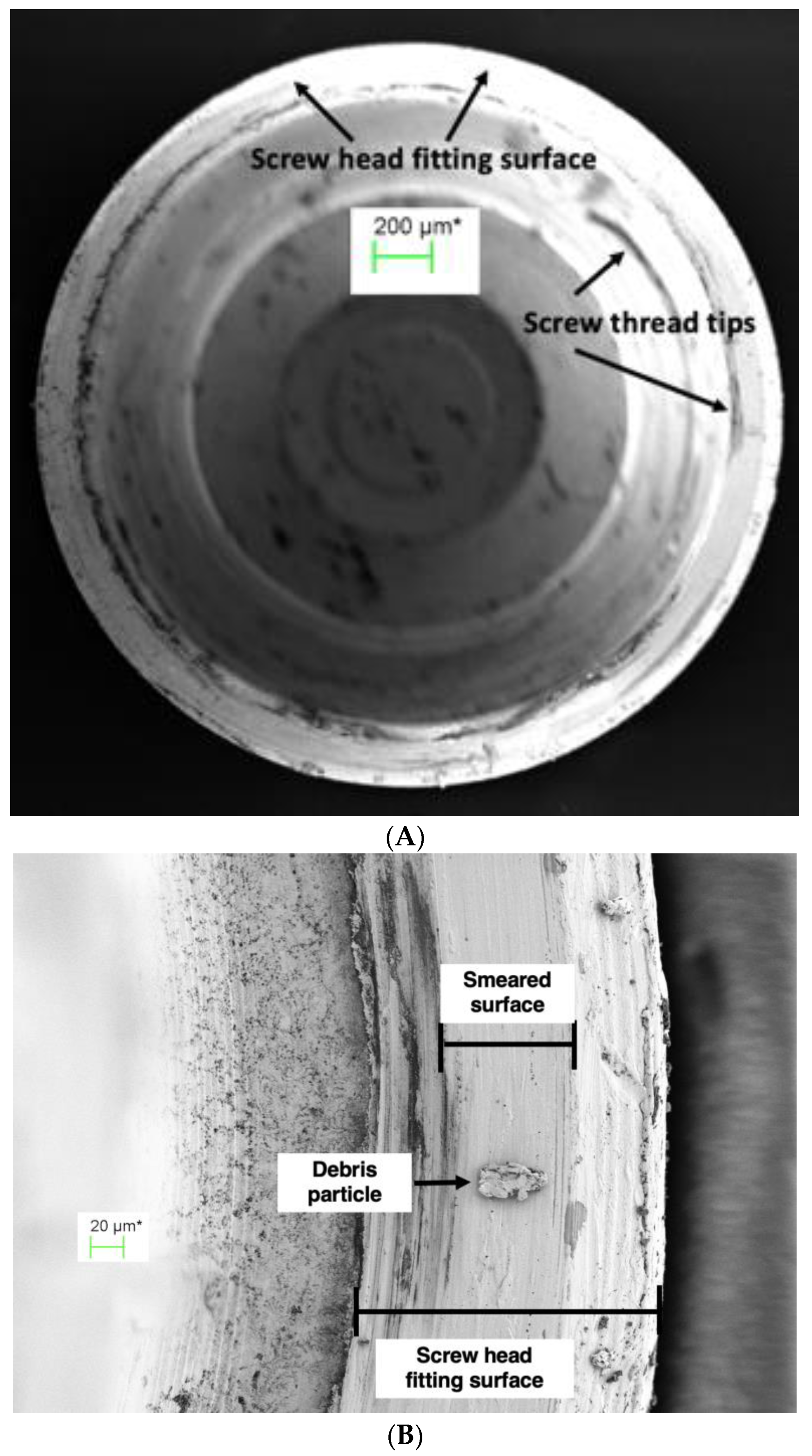
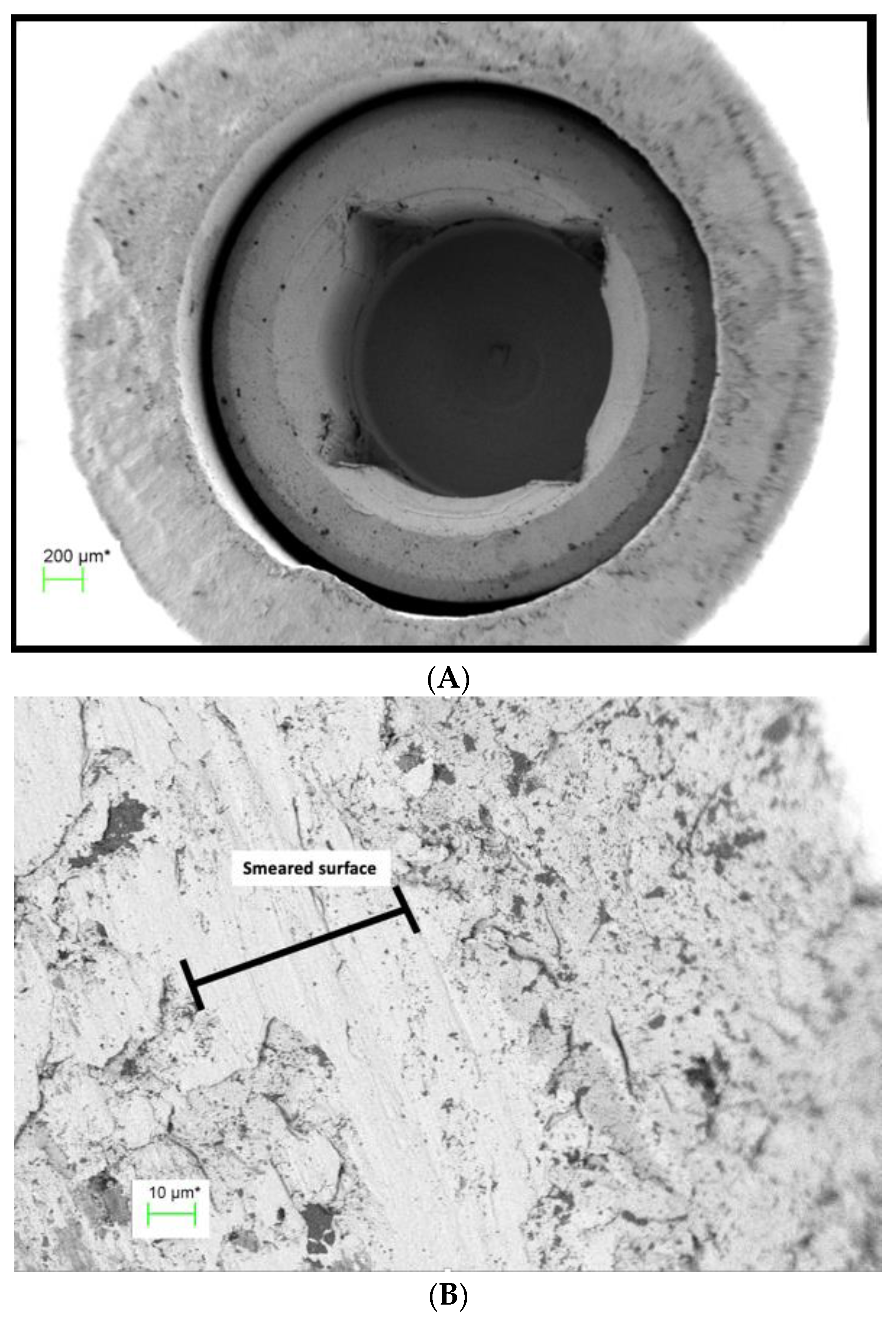
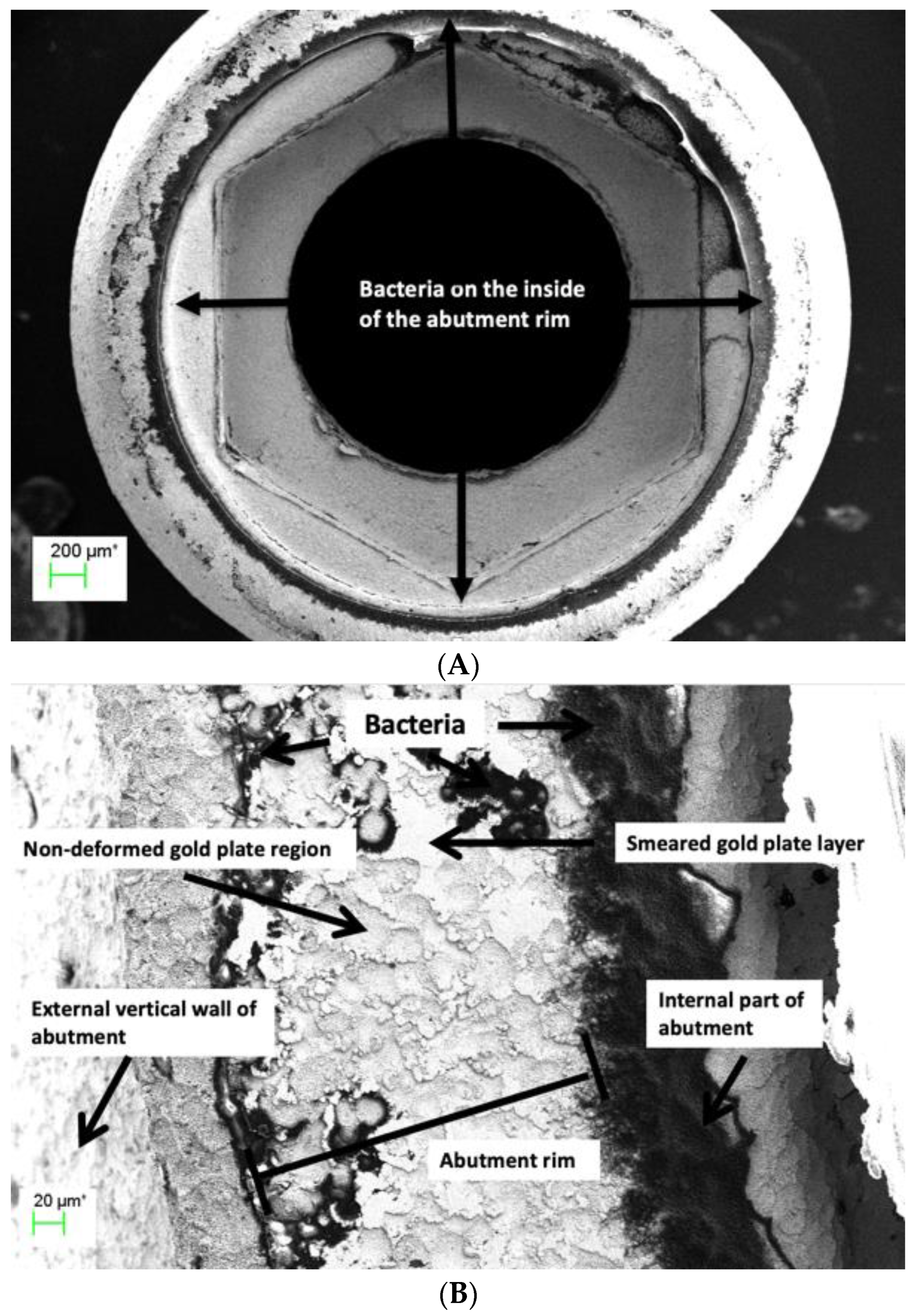
3.3. SEM Qualitative Assessment of Connecting Surface Profiles
4. Discussion
5. Conclusions
- Abutment connecting surfaces, both Au-plated and not Au-plated, showed plastic deformation (smearing) in variable mosaic patterns across the micro-gap with the high-gold-content alloys used in the study.
- External micro-gap measurements do not give a true indication of the profiles and approximation of the abutment/implant connecting surfaces.
- External micro-gap dimensions of cast external hexagon abutments with and without Au plating measured under shadow, eliminating silhouette illumination, averaged < 5 μm and were equivalent to those of the machined abutments.
- An uninterrupted smeared layer across the abutment fitting surface can provide an effective barrier to the egress of bacteria from the internal regions of the implant.
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| UCLA | University of California at Los Angeles abutments |
| PUCLA | Plastic castable University of California at Los Angeles abutments |
| GUCLA | Machined cast-to-University-of-California-at-Los-Angeles abutments |
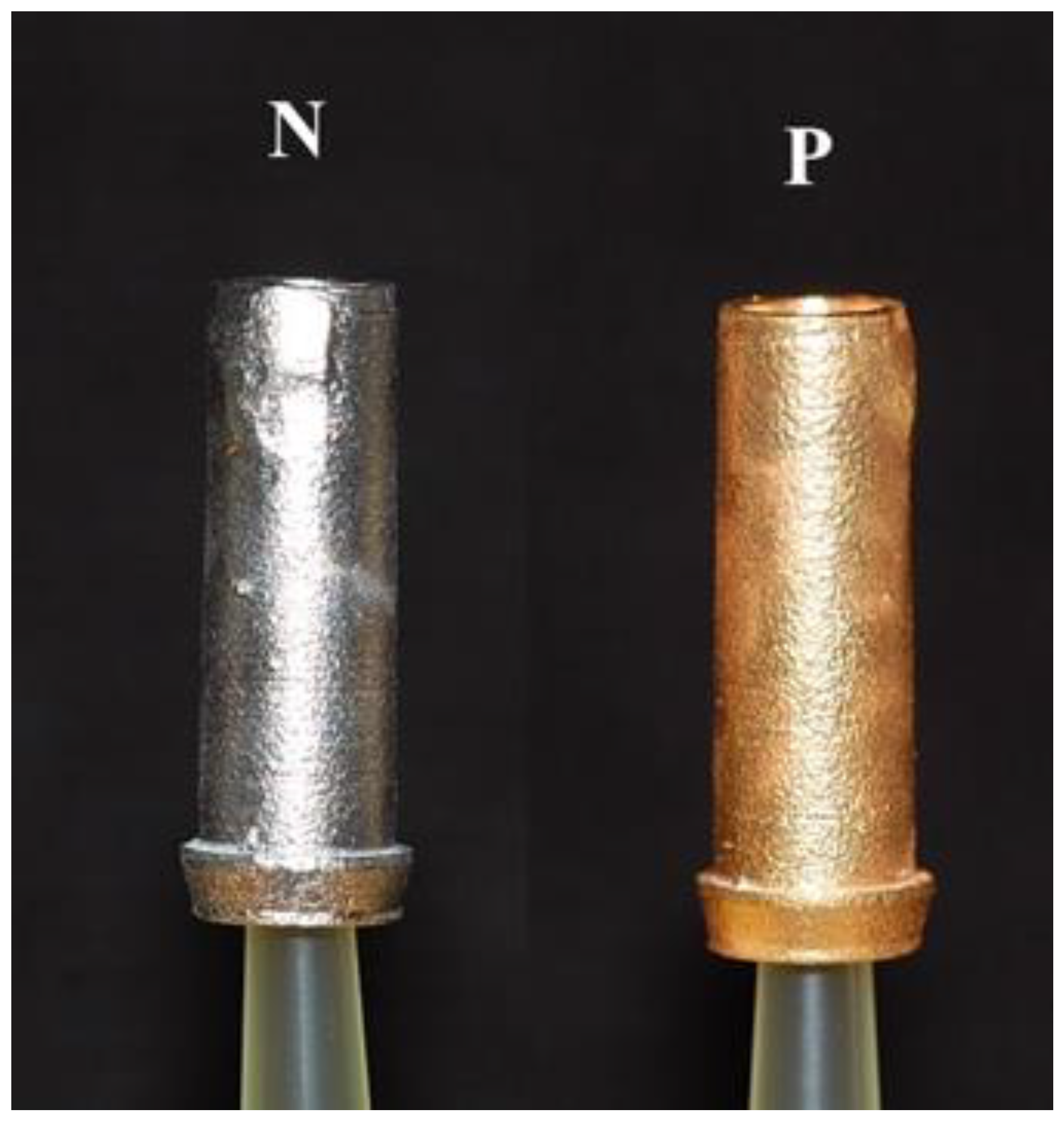
| UCLA-P | University of California at Los Angeles abutments electrolytically gold-plated |
| UCLA-N | University of California at Los Angeles abutments not electrolytically gold-plated |
| IAC | Implant-abutment combinations |
| TA | Test assembly |
| MBL | Marginal bone level |
| SEM | Scanning electron microscope |
| μm | Microns |
| nm | Nanometres |
| E. coli | Eschericia coli |
| BHI | Brain heart infusion medium |
| μL | Microlitre |
| CAM | Computer-assisted manufacture |
| 3D | Three dimensional |
References
- Choi, S.; Kang, Y.S.; Yeo, I.-S.L. Influence of implant-abutment connection biomechanics on biological response: A literature review of interfaces between implants and abutments of titanium and zirconia. Prosthesis 2023, 5, 527–538. [Google Scholar] [CrossRef]
- Jansen, V.K.; Conrads, G.; Richter, E.J. Microbial leakage and marginal fit of the implant-abutment interface. Int. J. Oral Maxillofac. Implants 1997, 12, 527–540. [Google Scholar]
- Vélez, J.; Peláez, J.; López-Suárez, C.; Agustín-Panadero, R.; Tobar, C.; Suárez, M.J. Influence of implant connection abutment design and screw insertion torque on implant-abutment misfit. J. Clin. Med. 2020, 9, 2365. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.B.; Brunski, J.B.; Hurley, E. Effects of fabrication, finishing and polishing procedures on preload in prostheses using conventional “gold” and plastic cylinders. Int. J. Oral Maxillofac. Implants 1996, 11, 589–598. [Google Scholar]
- Byrne, D.; Houston, F.; Cleary, R.; Claffey, N. The fit of cast and machined implant abutments. J. Prosthet. Dent. 1998, 80, 184–192. [Google Scholar] [CrossRef] [PubMed]
- De Mori, R.; Ribeiro, C.F.; Neves, A.C.C. Evaluation of castable and premachined meatal base abutment/implant interfaces before and after cyclical loading. Implant. Dent. 2014, 23, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Dias, E.C.L.D.C.E.M.; Bisognin, E.D.C.; Harari, N.D.; Machado, S.J.; Da Silva, C.P.; Soares, G.D.D.A.; Vidigal, G.M. Evaluation of implant-abutment microgap and bacterial leakage in five external-hex implant systems: An in vitro study. Int. J. Oral Maxillofac. Implants 2012, 27, 346–351. [Google Scholar]
- Pera, F.; Pesce, P.; Menini, M.; Fanelli, F.; Kim, B.-C.; Zhurakivska, K.; Mayer, Y.; Isola, F.; Cianciotta, G.; Crupi, A.; et al. Immediate loading full-arch rehabilitation using transmucosal tissue-level implants with different variables associated: A one-year observational study. Dent. Oral Sc. 2023, 72, 230–238. [Google Scholar] [CrossRef]
- Broggini, N.; McManus, L.; Hermann, J.; Medina, R.; Oates, T.; Schenk, R.; Buser, D.; Mellonig, J.; Cochran, D. Persistent acute inflammation at the implant-abutment interface. J. Dent. Res. 2003, 82, 232–237. [Google Scholar] [CrossRef]
- Hermann, J.S.; Cochran, D.L.; Hermann, J.S.; Buser, D.; Schenk, R.K.; Schoolfield, J.D. Biologic width around one- and two- piece titanium implants. Clin. Oral Implants Res. 2001, 12, 559–571. [Google Scholar] [CrossRef]
- Hermann, J.S.; Schoolfield, J.D.; Schenk, R.K.; Buser, D.; Cochran, D.L. Influence of the size of the microgap on crestal bone changes around titanium implants. A histomeric evaluation of unloaded non-submerged implants in the canine mandible. J. Periodontol. 2001, 72, 1372–1383. [Google Scholar] [CrossRef] [PubMed]
- King, G.N.; Hermann, J.S.; Schoolfield, J.D.; Buser, D.; Cochran, D.L. Influence of the size of the microgap on crestal bone levels in non-submerged dental implants: A radiographic study in the canine mandible. J. Periodontol. 2002, 73, 1111–1117. [Google Scholar] [CrossRef] [PubMed]
- Sahin, S.; Çehreli, M.C. The significance of passive framework fit in implant prosthodontics: Current status. Implant. Dent. 2001, 10, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Dahlin, C.; Jemt, T.; Sennerby, L.; Turri, A.; Wennerberg, A. Is marginal bone loss around oral implants the result of a provoked foreign body reaction? Clin. Implants Dent. Relat. Res. 2014, 16, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Jemt, T.; Mölne, J.; Tengvall, P.; Wennerberg, A. On inflammation-immunological balance theory–a critical apprehension of disease concepts around implants: Mucositis and marginal bone loss may represent normal conditions and not necessarily a state of disease. Clin. Implants Dent. Rel. Res. 2019, 21, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Winkler, S.; Ring, K.; Ring, J.D.; Boberick, K.G. Implant screw mechanics and the settling effect: Overview. J. Oral Implants 2003, 29, 242–245. [Google Scholar] [CrossRef]
- Tribst, J.P.M.; Piva, A.M.d.O.D.; da Silva-Concílio, L.R.; Ausiello, P.; Kalman, L. Influence of implant-abutment contact surfaces and prosthetic screw tightening on the stress concentration, fatigue life and microgap formation. A finite element analysis. Oral 2021, 1, 88–101. [Google Scholar] [CrossRef]
- Sasada, Y.; Cochran, D.L. Implant-abutment connections: A review of biologic consequences and peri-implantitis implications. Int. J. Oral Maxillofac. Implants 2017, 32, 1296–1307. [Google Scholar] [CrossRef]
- Walton, T.R. The up-to-14-year survival and complication burden of 256 TiUnite implants supporting one-piece cast abutment/metal-ceramic implant-supportedsinglecrowns. Int. J. Oral Maxillofac. Implants 2016, 31, 1349–1358. [Google Scholar] [CrossRef]
- Silva, M.D.; Walton, T.R.; Alrabeah, G.O.; Layton, D.M.; Petridis, H. Comparison of corrosion products from implant and various gold-based abutment couplings: The effect of gold plating. J. Oral Implantol. 2021, 47, 370–379. [Google Scholar] [CrossRef]
- Wachi, T.; Shuto, T.; Shinohara, Y.; Matono, Y.; Makihira, S. Release of titanium ions from an implant surface and their effect on cytokine production related to alveolar bone resorption. Toxicology 2015, 327, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Alrabeah, G.O.; Brett, P.; Knowles, J.C.; Petridis, H. The effect of metal ions released from different dental implant-abutment couples on osteoblast function and secretion of bone resorbing mediators. J. Dent. 2017, 66, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.P.; Merin, J.P.; Nakano, T.; Kato, T.; Kitade, Y.; Okamoto, T. Inhibition of the DNA-binding activity of NF-ĸB by gold compounds in vitro. FEBS Lett. 1995, 361, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Zainali, K.; Danscher, G.; Jakobsen, T.; Jakobsen, S.S.; Baas, J.; Møller, P.; Bechtold, J.E.; Soballe, K. Effects of gold coating on experimental implant fixation. J. Biomed. Mater. Res. 2009, 88A, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Walton, T.R. Characterisation and electroplated gold coatings for dental applications: Estimation of thickness using non-destructive electron-probe microanalysis related to plating time. Coatings 2021, 11, 874. [Google Scholar] [CrossRef]
- Tsuge, T.; Hagiwara, Y. Influence of lateral-oblique cyclic loading on abutment screw loosening of internal and external hexagon implants. Dent. Mater. J. 2009, 28, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Kano, S.C.; Binon, P.; Bonfante, G.; Curtis, D.A. Effect of casting procedure on screw loosening in UCLA-type abutments. J. Prosthodont. 2006, 15, 77–81. [Google Scholar] [CrossRef]
- Øilo, M.; Nesse, H.; Lundberg, O.J.; Gjerdet, N.R. Mechanical properties of cobalt-chromium 3-unit fixed dental prostheses fabricated by casting, milling, and additive manufacturing. J. Prosthet. Dent. 2018, 120, 156.e1–156.e7. [Google Scholar] [CrossRef]
- Presotto, A.G.C.; Cordeiro, J.M.; Presotto, J.G.C.; Rangel, E.C.; da Cruz, N.C.; Landers, R.; Barao, V.A.R.; Mesquita, M.F. Feasibility of 3D printed Co-Cr alloy for dental prostheses applications. J. Alloys Compd. 2021, 862, 158171. [Google Scholar] [CrossRef]
- Wilson, T.G. The positive relationship between excess cement and peri-implant disease.: A clinical endoscopic study. J. Periodontol. 2009, 80, 1388–1392. [Google Scholar] [CrossRef]
- Fretwurst, T.; Buzanich, G.; Nahles, S.; Woelber, J.P.; Riesemeier, H.; Nelson, K. Metal elements in tissue with dental peri-implantitis: A pilot study. Clin. Oral Impl. Res. 2016, 27, 1178–1186. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Reichl, F.-X.; Wang, Y.; Michalke, B.; Milz, S.; Yang, Y.; Stolper, P.; Lindemaier, G.; Graw, M.; Hickel, R.; et al. Analysis of titanium and other metals in human jawbones with dental implants–A case series study. Dent. Mater. 2016, 32, 1042–1051. [Google Scholar] [CrossRef] [PubMed]
- Jeon, K.I.; Jeong, J.Y.; Jue, D.M. Thiol-reactive metal compounds inhibit NF-ĸB activation by blocking IĸB kinase. J. Immunol. 2000, 164, 5981–5989. [Google Scholar] [CrossRef] [PubMed]
- Basova, T.V.; Vikulova, E.S.; Dorovskikh, S.I.; Hassan, A.; Morozova, N.B. The use of noble metal coatings and nanoparticles for the modification of medical implant materials. Mater. Des. 2021, 204, 109672. [Google Scholar] [CrossRef]
- Traver-Mendes, V.; Camps-Font, O.; Ventura, F.; Nicolau-Sansó, M.A.; Subirà-Pifarré, C.; Figueiredo, R.; Valmaseda-Castellón, E. In-vitro characterization of an anodized surface of a dental implant collar and dental abutment on peri-implant cellular response. Materials 2023, 16, 6012. [Google Scholar] [CrossRef] [PubMed]
- Kunrath, M.F.; Gerhardt, M.d.N. Trans mucosal platforms for dental implants: Strategies to induce muco-integration and shield peri-implant diseases. Dental. Mater. 2023, 39, 846–859. [Google Scholar] [CrossRef]
- van Oirschot, B.A.; Zhang, Y.; Alghamdi, H.S.; Cordeiro, J.M.; Nagay, B.E.; Barao, V.A.; de Avila, E.D.; van den Beuchen, J.J. Surface engineering for dental implantology: Favoring tissue responses along the implant. Tissue. Eng. Part A 2022, 28, 555–572. [Google Scholar] [CrossRef]
- Park, C.I.; Choe, H.C.; Chung, C.H. Effect of surface coating on the screw loosening of dental abutment screws. Met. Mater. Int. 2004, 10, 549–553. [Google Scholar] [CrossRef]
- Yi, Y.; Koak, J.-Y.; Kim, S.-K.; Lee, S.-J.; Heo, S.-J. Comparison of implant component fractures in external and internal type: A 12-year retrospective study. J. Adv. Prosthodont. 2018, 10, 155–162. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Element | Composition % |
|---|---|
| Gold—Au | 75 |
| Palladium—Pd | 19 |
| Silver—Ag | 1 |
| Copper—Cu | 0.44 |
| Zinc—Zn | 0.5 |
| Tin—Sn | 2 |
| Indium | 2 |
| Iridium—Ir | 0.01 |
| Ruthenium—Ru | 0.06 |
| TA | Description | MG-1 | MG-2 | MG-3 | Mean MG |
|---|---|---|---|---|---|
| 1 | PUCLA-P1 | 3.2 | 3.2 | 2.9 | 3.1 |
| 2 | PUCLA-P2 | 4.7 | 2.9 | 1.8 | 3.1 |
| 3 | PUCLA-P3 | 1.7 | 1.4 | 2.5 | 2.5 |
| 4 | PUCLA-P4 | 1.9 | 1.0 | 1.3 | 1.3 |
| TA | Media/Dilution | Bubbles | Mean Microgap μm | ||||
|---|---|---|---|---|---|---|---|
| 430 μL | 50 μL | 1:100 | 1:1000 | 1:10,000 | |||
| PUCLA-P2 | ~600 | 188 | 40 | 7 | 1 | No | 3.1 |
| PUCLA-P3 | ~350 | 206 | 17 | 1 | 0 | No | 2.5 |
| PUCLA-P4 | ~350 | 152 | 24 | 1 | 0 | No | 1.3 |
| PUCLA-P6 | 0 | - | - | - | - | No | 2.8 |
| PUCLA-P7 | 0 | - | - | - | - | No | 1.7 |
| PUCLA-N3 | xxx | xx | 295 | 81 | 9 | No | 3.7 |
| PUCLA-N5 | 0 | - | - | - | - | No | 4.6 |
| PUCLA-N6 | 0 | - | - | - | - | No | 3.5 |
| PUCLA-N7 | 0 | - | - | - | - | No | 4.7 |
| PUCLA-N8 | xxx | xxx | xxx | ~500 | 80 | Yes | 4.9 |
| GUCLA-N1 | 0 | - | - | - | - | No | 3.8 |
| GUCLA-N2 | 0 | - | - | - | - | No | 4.1 |
| GUCLA-N3 | 0 | - | - | - | - | No | 2.9 |
| GUCLA-P1 | 0 | - | - | - | - | No | 3.0 |
| GUCLA-P2 | 0 | - | - | - | - | No | 3.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walton, T.R. Effect of Electrodeposited Gold Coatings on Micro-Gaps, Surface Profile and Bacterial Leakage of Cast UCLA Abutments Attached to External Hexagon Dental Implants. Coatings 2023, 13, 1976. https://0-doi-org.brum.beds.ac.uk/10.3390/coatings13121976
Walton TR. Effect of Electrodeposited Gold Coatings on Micro-Gaps, Surface Profile and Bacterial Leakage of Cast UCLA Abutments Attached to External Hexagon Dental Implants. Coatings. 2023; 13(12):1976. https://0-doi-org.brum.beds.ac.uk/10.3390/coatings13121976
Chicago/Turabian StyleWalton, Terry R. 2023. "Effect of Electrodeposited Gold Coatings on Micro-Gaps, Surface Profile and Bacterial Leakage of Cast UCLA Abutments Attached to External Hexagon Dental Implants" Coatings 13, no. 12: 1976. https://0-doi-org.brum.beds.ac.uk/10.3390/coatings13121976