
The Main Risk Factors in Type 2 Diabetes for Cognitive Dysfunction, Depression, and Psychosocial Problems: A Systematic Review

Abstract
:1. Introduction
2. Methodology
2.1. Design
2.2. Research Question
2.3. Search Strategy
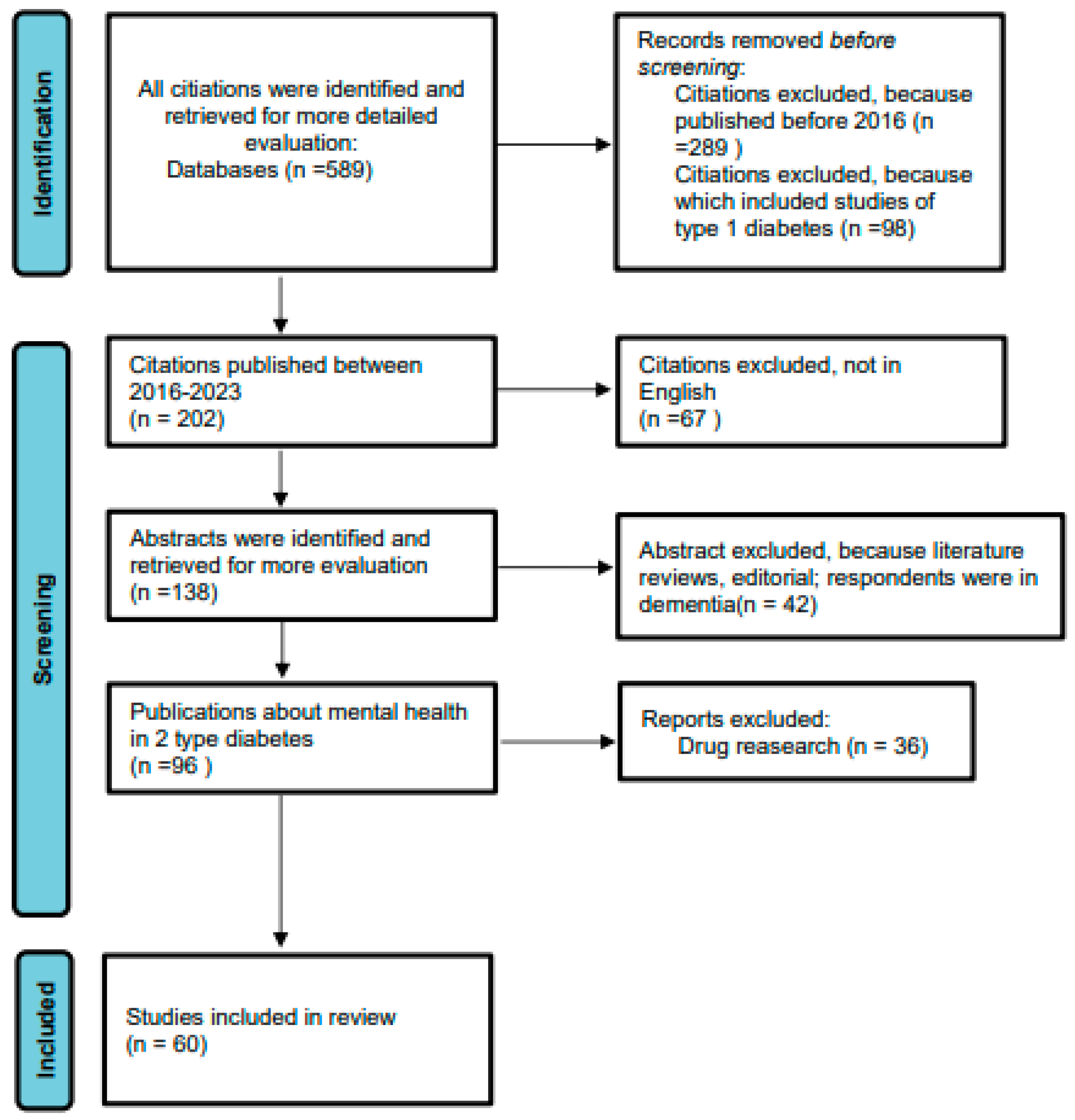
2.4. Screening and Quality Control
2.5. Data Analysis
3. Results
3.1. Risk Factors for Cognitive Impairment in Type 2 Diabetes

{kind=link}
{kind=link}
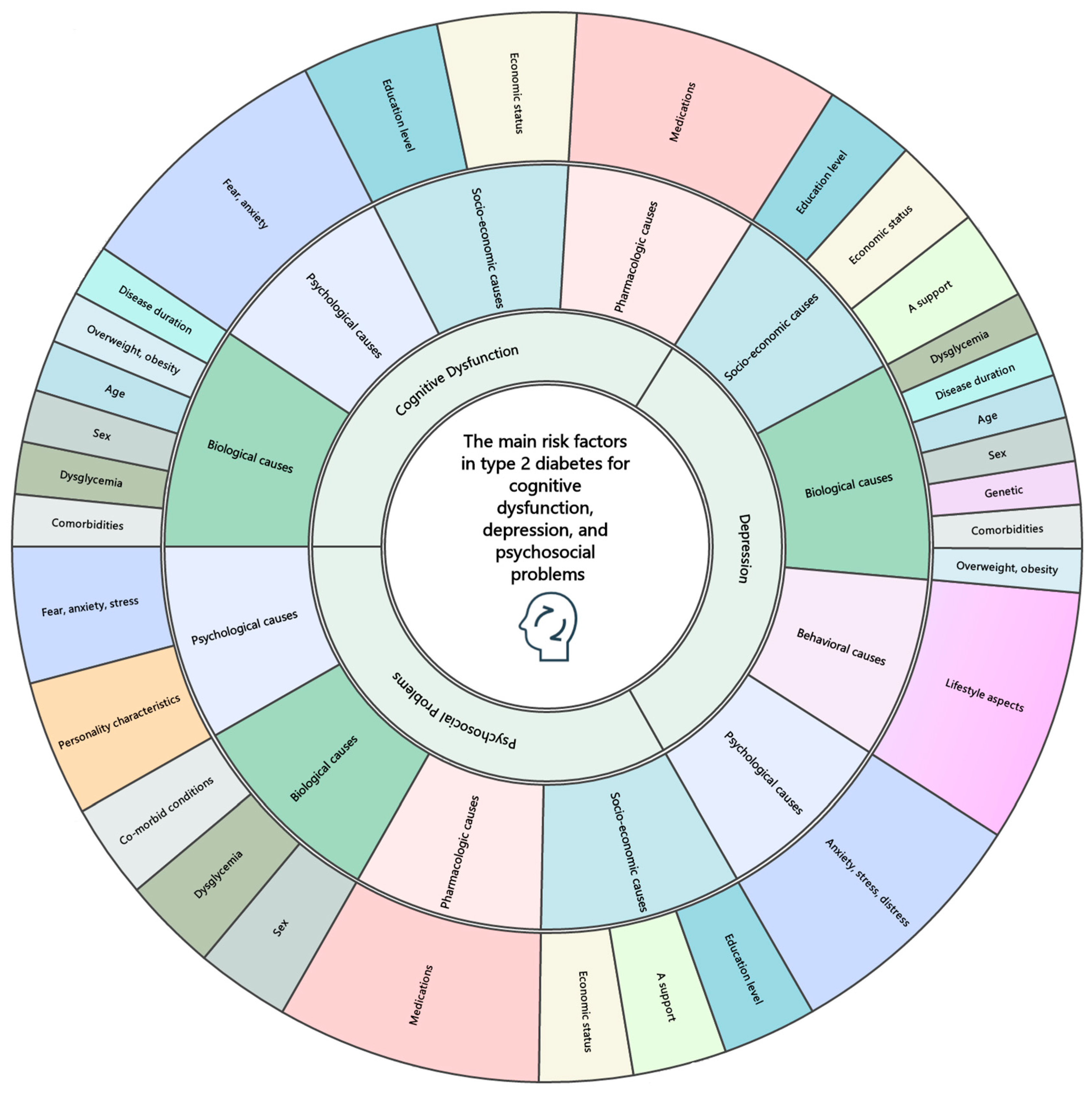
| Category | Subcategory | Substantive Code |
|---|---|---|
| Biological causes | ||
| Comorbidities [16,22,23,24,25] | Micro- and macrovascular diseases, complications, hypertension, cardiovascular diseases, heart rhythm disorders, diabetic retinopathy, dyslipidemia, systemic inflammation, diabetic nephropathy, stroke, and sleep apnea | |
| Disease duration [5,28,36,37] | Long-term diabetes, disease duration, disease duration over five years, and disease progression | |
| Overweight, obesity [16,23,38,39,40,41] | Overweight, obesity, body mass index (BMI), high BMI, and high waist circumference | |
| Age [18,35,36,37,42] | Elderly, age ≤ 65 years, advanced age, middle-aged and older people | |
| Dysglycemia [17,24,28,43,44] | Hypoglycemia, hyperglycemia, low blood sugar, blood sugar fluctuation, hypoglycemia episodes, fasting glucose, high HbA1c, glycemic control, insulin resistance, and chronic hyperglycemia | |
| Sex [19,20,21,23] | Female, male and gender differences | |
| Psychological causes | ||
| Fear, anxiety [5,22,30] | Symptoms of depression, stress, anxiety, and fear | |
| Socio-economic causes | Education level [5,17,22,28] | Education level, schooling under 6 years, and low education level |
| Economic status [6,20,31] | Social status, economic capability, socioeconomic status, unemployment, and access to resources | |
| Pharmacologic causes | Medications [32,33,34,35] | Insulin, beta blockers, polypharmacy, drug side effect, drug interaction, drug effect, time of drug use, and long-term use |
3.2. Risk Factors for Depression in Type 2 Diabetes
3.3. Risk Factors for Psychosocial Problems in Type 2 Diabetes
4. Discussion
4.1. Factors Influencing the Development of Diabetic Cognitive Impairment
4.2. Factors Influencing the Onset of Depression in Diabetes Patients
4.3. Socio-Economic Aspects
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kim, G.M.; Woo, J.M.; Jung, S.Y.; Shin, S.; Song, H.J.; Park, J.; Ahn, J. Positive association between serious psychiatric outcomes and complications of diabetes mellitus in patients with depressive disorders. Int. J. Psychiatry Med. 2015, 50, 131–146. [Google Scholar] [CrossRef]
- Ali, M.K.; Pearson-Stuttard, J.; Selvin, E.; Gregg, E.W. Interpreting global trends in type 2 diabetes complications and mortality. Diabetologia 2022, 65, 3–13. [Google Scholar] [CrossRef]
- Bellary, S.; Kyrou, I.; Brown, J.E.; Bailey, C.J. Type 2 diabetes mellitus in older adults: Clinical considerations and management. Nat. Rev. Endocrinol. 2021, 17, 534–548. [Google Scholar] [CrossRef]
- Longo, M.; Bellastella, G.; Maiorino, M.I.; Meier, J.J.; Esposito, K.; Giugliano, D. Diabetes and Aging: From Treatment Goals to Pharmacologic Therapy. Front. Endocrinol. 2019, 10, 45. [Google Scholar] [CrossRef] [PubMed]
- Bellia, C.; Lombardo, M.; Meloni, M.; Della-Morte, D.; Bellia, A.; Lauro, D. Diabetes and cognitive decline. Adv. Clin. Chem. 2022, 108, 37–71. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Xu, Q.; Yu, J.; Yang, Y.; Wang, Z.; Zhang, B.; Wang, S.; Chen, X.; Zhang, Y.; Zhu, X.; et al. Prevalence and possible factors of cognitive frailty in the elderly with hypertension and diabetes. Front. Cardiovasc. Med. 2022, 9, 1054208. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Wei, G.; Wang, Y.; Liu, T.; Huang, T.; Wei, Q.; Ma, G.; Wang, D. Risk factors for depression in elderly diabetic patients and the effect of metformin on the condition. BMC Public Health 2019, 19, 1063. [Google Scholar] [CrossRef] [PubMed]
- Bettany- Saltikov, J.; McSherry, R. How to Do a Sytematic Literature Review in Nursing: A Step-by-Step Guide; Open University Press: Maidenhead, UK, 2016. [Google Scholar]
- Xiao, Y.; Watson, M. Guidance on Conducting a Systematic Literature Review. J. Plan. Educ. Res. 2019, 39, 93–112. [Google Scholar] [CrossRef]
- Aromataris, E.; Pearson, A. The Systematic Review: An Overview. AJN Am. J. Nurs. 2014, 114, 53–58. [Google Scholar] [CrossRef]
- Aromataris, E. Furthering the science of evidence synthesis with a mix of methods. JBI Evid. Synth. 2020, 18, 2106–2107. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Elo, S.; Kyngas, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Siegel, Z.T.G.; Stenson, K.W. Longitudinal Cohort versus Cross-Sectional Cohort Studies; Hammond, F.M., Malec, J.F., Nick, T.G., Buschbacher, R.M., Eds.; Springer Publishing Company: Berlin/Heidelberg, Germany, 2014; pp. 32–33. [Google Scholar]
- Bezerra, C.T.; Grande, A.J.; Galvão, V.K.; Santos, D.H.M.D.; Atallah, Á.N.; Silva, V. Assessment of the strength of recommendation and quality of evidence: GRADE checklist. A descriptive study. Sao Paulo Med. J. 2022, 140, 829–836. [Google Scholar] [CrossRef] [PubMed]
- Xia, S.S.; Xia, W.L.; Huang, J.J.; Zou, H.J.; Tao, J.; Yang, Y. The factors contributing to cognitive dysfunction in type 2 diabetic patients. Ann. Transl. Med. 2020, 8, 104. [Google Scholar] [CrossRef]
- Sun, L.; Diao, X.; Gang, X.; Lv, Y.; Zhao, X.; Yang, S.; Gao, Y.; Wang, G. Risk Factors for Cognitive Impairment in Patients with Type 2 Diabetes. J. Diabetes Res. 2020, 2020, 4591938. [Google Scholar] [CrossRef]
- Cigolle, C.T.; Blaum, C.S.; Lyu, C.; Ha, J.; Kabeto, M.; Zhong, J. Associations of Age at Diagnosis and Duration of Diabetes with Morbidity and Mortality Among Older Adults. JAMA Netw. Open 2022, 5, e2232766. [Google Scholar] [CrossRef] [PubMed]
- Levine, D.A.; Gross, A.L.; Briceño, E.M.; Tilton, N.; Giordani, B.J.; Sussman, J.B.; Hayward, R.A.; Burke, J.F.; Hingtgen, S.; Elkind, M.S.V.; et al. Sex Differences in Cognitive Decline Among US Adults. JAMA Netw. Open 2021, 4, e210169. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Xiao, L.D.; Wang, K.; Luo, Y.; Li, X. Gender Differences in Cognitive Impairment among Rural Elderly in China. Int. J. Environ. Res. Public Health 2020, 17, 3724. [Google Scholar] [CrossRef] [PubMed]
- Santabárbara, J.; Villagrasa, B.; Lopez-Anton, R.; De la Cámara, C.; Gracia-García, P.; Lobo, A. Anxiety and Risk of Vascular Dementia in an Elderly Community Sample: The Role of Sex. Brain Sci. 2020, 10, 265. [Google Scholar] [CrossRef]
- de Almeida Faria, A.C.R.; Dall’Agnol, J.F.; Gouveia, A.M.; de Paiva, C.I.; Segalla, V.C.; Baena, C.P. Risk factors for cognitive decline in type 2 diabetes mellitus patients in Brazil: A prospective observational study. Diabetol. Metab. Syndr. 2022, 14, 105. [Google Scholar] [CrossRef]
- Milani, S.A.; Lopez, D.S.; Downer, B.; Samper-Ternent, R.; Wong, R. Effects of diabetes and obesity on cognitive impairment and mortality in older mexicans. Arch. Gerontol. Geriatr. 2022, 99, 104581. [Google Scholar] [CrossRef] [PubMed]
- Rhmari Tlemcani, F.Z.; Elamari, S.; Motaib, I.; Laidi, S.; Alidrissi, N.; Ahid, S.; Chadli, A. Factors Associated with Mild Cognitive Impairment in Patients with Type 2 Diabetes: A Cohort Study. Cureus 2022, 14, e28305. [Google Scholar] [CrossRef] [PubMed]
- Palta, P.; Carlson, M.C.; Crum, R.M.; Colantuoni, E.; Sharrett, A.R.; Yasar, S.; Nahin, R.L.; DeKosky, S.T.; Snitz, B.; Lopez, O.; et al. Diabetes and Cognitive Decline in Older Adults: The Ginkgo Evaluation of Memory Study. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 73, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Livny, A.; Ravona-Springer, R.; Heymann, A.; Priess, R.; Kushnir, T.; Tsarfaty, G.; Rabinov, L.; Moran, R.; Tik, N.; Moshier, E.; et al. Haptoglobin 1-1 Genotype Modulates the Association of Glycemic Control with Hippocampal Volume in Elderly Individuals With Type 2 Diabetes. Diabetes 2017, 66, 2927–2932. [Google Scholar] [CrossRef]
- Dove, A.; Shang, Y.; Xu, W.; Grande, G.; Laukka, E.J.; Fratiglioni, L.; Marseglia, A. The impact of diabetes on cognitive impairment and its progression to dementia. Alzheimers Dement. 2021, 17, 1769–1778. [Google Scholar] [CrossRef] [PubMed]
- Mallorqui-Bague, N.; Lozano-Madrid, M.; Toledo, E.; Corella, D.; Salas-Salvado, J.; Cuenca-Royo, A.; Vioque, J.; Romaguera, D.; Martinez, J.A.; Warnberg, J.; et al. Type 2 diabetes and cognitive impairment in an older population with overweight or obesity and metabolic syndrome: Baseline cross-sectional analysis of the PREDIMED-plus study. Sci. Rep. 2018, 8, 16128. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, N.; Chaturvedi, S.K. Depressive symptoms and disorders in type 2 diabetes mellitus. Curr. Opin. Psychiatry 2019, 32, 416–421. [Google Scholar] [CrossRef]
- Carr, A.L.; Sluiman, A.J.; Grecian, S.M.; Forster, R.; McLachlan, S.; Strachan, M.W.J.; Price, J.F. Depression as a risk factor for dementia in older people with type 2 diabetes and the mediating effect of inflammation. Diabetologia 2021, 64, 448–457. [Google Scholar] [CrossRef]
- Larnyo, E.; Dai, B.; Nutakor, J.A.; Ampon-Wireko, S.; Larnyo, A.; Appiah, R. Examining the impact of socioeconomic status, demographic characteristics, lifestyle, and other risk factors on adults’ cognitive functioning in developing countries: An analysis of five selected WHO SAGE Wave 1 Countries. Int. J. Equity Health 2022, 21, 31. [Google Scholar] [CrossRef]
- Bohlken, J.; Jacob, L.; Kostev, K. Association Between the Use of Antihyperglycemic Drugs and Dementia Risk: A Case-Control Study. J. Alzheimers Dis. 2018, 66, 725–732. [Google Scholar] [CrossRef]
- Gomez-Martinez, C.; Babio, N.; Julvez, J.; Becerra-Tomas, N.; Martinez-Gonzalez, M.A.; Corella, D.; Castaner, O.; Romaguera, D.; Vioque, J.; Alonso-Gomez, A.M.; et al. Glycemic Dysregulations Are Associated With Worsening Cognitive Function in Older Participants at High Risk of Cardiovascular Disease: Two-Year Follow-up in the PREDIMED-Plus Study. Front. Endocrinol. 2021, 12, 754347. [Google Scholar] [CrossRef] [PubMed]
- Tsujimoto, T.; Sugiyama, T.; Shapiro, M.F.; Noda, M.; Kajio, H. Risk of Cardiovascular Events in Patients With Diabetes Mellitus on beta-Blockers. Hypertension 2017, 70, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Holm, H.; Ricci, F.; Di Martino, G.; Bachus, E.; Nilsson, E.D.; Ballerini, P.; Melander, O.; Hansson, O.; Nagga, K.; Magnusson, M.; et al. Beta-blocker therapy and risk of vascular dementia: A population-based prospective study. Vascul. Pharmacol. 2020, 125–126, 106649. [Google Scholar] [CrossRef]
- Antal, B.; McMahon, L.P.; Sultan, S.F.; Lithen, A.; Wexler, D.J.; Dickerson, B.; Ratai, E.M.; Mujica-Parodi, L.R. Type 2 diabetes mellitus accelerates brain aging and cognitive decline: Complementary findings from UK Biobank and meta-analyses. eLife 2022, 11, 1–24. [Google Scholar] [CrossRef]
- Frison, E.; Proust-Lima, C.; Mangin, J.F.; Habert, M.O.; Bombois, S.; Ousset, P.J.; Pasquier, F.; Hanon, O.; Paquet, C.; Gabelle, A.; et al. Diabetes Mellitus and Cognition: Pathway Analysis in the MEMENTO Cohort. Neurology 2021, 97, e836–e848. [Google Scholar] [CrossRef] [PubMed]
- Xing, Z.; Long, C.; Hu, X.; Chai, X. Obesity is associated with greater cognitive function in patients with type 2 diabetes mellitus. Front. Endocrinol. 2022, 13, 953826. [Google Scholar] [CrossRef] [PubMed]
- Quaye, E.; Galecki, A.T.; Tilton, N.; Whitney, R.; Briceño, E.M.; Elkind, M.S.V.; Fitzpatrick, A.L.; Gottesman, R.F.; Griswold, M.; Gross, A.L.; et al. Association of Obesity With Cognitive Decline in Black and White Americans. Neurology 2023, 100, e220–e231. [Google Scholar] [CrossRef]
- Ganguli, M.; Beer, J.C.; Zmuda, J.M.; Ryan, C.M.; Sullivan, K.J.; Chang, C.-C.H.; Rao, R.H. Aging, Diabetes, Obesity, and Cognitive Decline: A Population-Based Study. J. Am. Geriatr. Soc. 2020, 68, 991–998. [Google Scholar] [CrossRef]
- Anand, S.S.; Friedrich, M.G.; Lee, D.S.; Awadalla, P.; Després, J.P.; Desai, D.; de Souza, R.J.; Dummer, T.; Parraga, G.; Larose, E.; et al. Evaluation of Adiposity and Cognitive Function in Adults. JAMA Netw. Open 2022, 5, e2146324. [Google Scholar] [CrossRef]
- Callisaya, M.L.; Beare, R.; Moran, C.; Phan, T.; Wang, W.; Srikanth, V.K. Type 2 diabetes mellitus, brain atrophy and cognitive decline in older people: A longitudinal study. Diabetologia 2019, 62, 448–458. [Google Scholar] [CrossRef]
- Xie, K.; Perna, L.; Schottker, B.; Kliegel, M.; Brenner, H.; Mons, U. Type 2 diabetes mellitus and cognitive decline in older adults in Germany—Results from a population-based cohort. BMC Geriatr. 2022, 22, 455. [Google Scholar] [CrossRef] [PubMed]
- Cholerton, B.; Omidpanah, A.; Verney, S.P.; Nelson, L.A.; Baker, L.D.; Suchy-Dicey, A.; Longstreth, W.T., Jr.; Howard, B.V.; Henderson, J.A.; Montine, T.J.; et al. Type 2 diabetes and later cognitive function in older American Indians: The Strong Heart Study. Int. J. Geriatr. Psychiatry 2019, 34, 1050–1057. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, P.; Ronkainen, J.; Nedelec, R.; Tolvanen, M.; Lowry, E.; Miettunen, J.; Jarvelin, M.-R.; Sebert, S. The relationship of life-course patterns of adiposity with type 2 diabetes, depression, and their comorbidity in the Northern Finland Birth Cohort 1966. Int. J. Obes. 2022, 46, 1470–1477. [Google Scholar] [CrossRef]
- Omar, S.M.; Musa, I.R.; Idrees, M.B.; Adam, I. Prevalence of depression and associated factors among patients with type 2 diabetes mellitus in eastern Sudan. BMC Psychiatry 2021, 21, 336. [Google Scholar] [CrossRef]
- Al-Ayed, M.; Moosa, S.R.; Robert, A.A.; Al Dawish, M. Anxiety, depression and their associated risk factors among patients with diabetic foot ulcer: A two center cross-sectional study in Jordan and Saudi Arabia. Diabetes Metab. Syndr. 2021, 15, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Biggers, A.; Sharp, L.K.; Nimitphong, H.; Saetung, S.; Siwasaranond, N.; Manodpitipong, A.; Crowley, S.J.; Hood, M.M.; Gerber, B.S.; Reutrakul, S. Relationship between depression, sleep quality, and hypoglycemia among persons with type 2 diabetes. J. Clin. Transl. Endocrinol. 2019, 15, 62–64. [Google Scholar] [CrossRef]
- Riaz, B.K.; Selim, S.; Neo, M.; Karim, M.N.; Zaman, M.M. Risk of Depression among Early Onset Type 2 Diabetes Mellitus Patients. Dubai Diabetes Endocrinol. J. 2021, 27, 55–65. [Google Scholar] [CrossRef]
- Birhanu, H.; Zenu, S.; Sheleme, T.; Tefera Kefeni, B. Magnitude of depression and its associated factors among patients with diabetes mellitus at public hospitals in Southwest Ethiopia, 2021. Sci. Rep. 2022, 12, 22134. [Google Scholar] [CrossRef] [PubMed]
- Benmaamar, S.; Lazar, N.; El Harch, I.; Maiouak, M.; Qarmiche, N.; Otmani, N.; Salhi, H.; Tachfouti, N.; El Ouahabi, H.; El Fakir, S. Depression, and anxiety in patients with diabetes in a Moroccan region. L’Encéphale 2022, 48, 601–606. [Google Scholar] [CrossRef]
- Sunny, A.K.; Khanal, V.K.; Sah, R.B.; Ghimire, A. Depression among people living with type 2 diabetes in an urbanizing community of Nepal. PLoS ONE 2019, 14, e0218119. [Google Scholar] [CrossRef]
- Mukeshimana, M.; Chironda, G. Depression and Associated Factors Among the Patients with Type 2 Diabetes in Rwanda. Ethiop. J. Health Sci. 2019, 29, 709–718. [Google Scholar] [CrossRef]
- Cardenas, L.; Cabezas, M.D.C.; Munoz, A.; Proano, J.L.; Mino, C.; Aguirre, N. Prevalence and risk factors of depression, anxiety, and stress in an Ecuadorian outpatient population with type II diabetes mellitus: A cross-sectional study (STROBE). Medicine 2022, 101, e30697. [Google Scholar] [CrossRef] [PubMed]
- Kec, D.; Rajdova, A.; Raputova, J.; Adamova, B.; Srotova, I.; Nekvapilova, E.K.; Michalcakova, R.N.; Horakova, M.; Belobradkova, J.; Olsovsky, J.; et al. Risk factors for depression and anxiety in painful and painless diabetic polyneuropathy: A multicentre observational cross-sectional study. Eur. J. Pain 2022, 26, 370–389. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Chen, S.; Xu, K.; Wang, Y.; Zhang, H.; Wang, L.; He, W. Prevalence and associated factors of depression and anxiety among Chinese diabetic retinopathy patients: A cross-sectional study. PLoS ONE 2022, 17, e0267848. [Google Scholar] [CrossRef] [PubMed]
- Repple, J.; König, A.; de Lange, S.C.; Opel, N.; Redlich, R.; Meinert, S.; Grotegerd, D.; Mauritz, M.; Hahn, T.; Borgers, T.; et al. Association Between Genetic Risk for Type 2 Diabetes and Structural Brain Connectivity in Major Depressive Disorder. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2022, 7, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.; Syed, S.; Wu, R.; Postolache, T.T.; Gragnoli, C. Familial Linkage and Association of the NR3C1 Gene with Type 2 Diabetes and Depression Comorbidity. Int. J. Mol. Sci. 2022, 23, 11951. [Google Scholar] [CrossRef] [PubMed]
- Rohde, C.; Nielsen, J.S.; Schöllhammer Knudsen, J.; Thomsen, R.W.; Østergaard, S.D. Risk factors associated with mortality among individuals with type 2 diabetes and depression across two cohorts. Eur. J. Endocrinol. 2022, 187, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Teel, C.; Sabus, C.; McGinnis, P.; Kluding, P. Fatigue in Type 2 Diabetes: Impact on Quality of Life and Predictors. PLoS ONE 2016, 11, e0165652. [Google Scholar] [CrossRef]
- Sharma, K.; Dhungana, G.; Adhikari, S.; Bista Pandey, A.; Sharma, M. Depression and Anxiety among Patients with Type II Diabetes Mellitus in Chitwan Medical College Teaching Hospital, Nepal. Nurs. Res. Pract. 2021, 2021, 8846915. [Google Scholar] [CrossRef]
- Bruce, D.G.; Davis, W.A.; Starkstein, S.E.; Davis, T.M.E. Clinical risk factors for depressive syndrome in Type 2 diabetes: The Fremantle Diabetes Study. Diabet. Med. 2018, 35, 903–910. [Google Scholar] [CrossRef]
- Barker, M.M.; Davies, M.J.; Zaccardi, F.; Brady, E.M.; Hall, A.P.; Henson, J.J.; Khunti, K.; Lake, A.; Redman, E.L.; Rowlands, A.V.; et al. Age at Diagnosis of Type 2 Diabetes and Depressive Symptoms, Diabetes-Specific Distress, and Self-Compassion. Diabetes Care 2023, 46, 579–586. [Google Scholar] [CrossRef]
- Hoogendoorn, C.J.; Schechter, C.B.; Llabre, M.M.; Walker, E.A.; Gonzalez, J.S. Distress and Type 2 Diabetes Self-Care: Putting the Pieces Together. Ann. Behav. Med. 2020, 55, 938–948. [Google Scholar] [CrossRef]
- Hu, Y.; Li, L.; Zhang, J. Diabetes Distress in Young Adults with Type 2 Diabetes: A Cross-Sectional Survey in China. J. Diabetes Res. 2020, 2020, 4814378. [Google Scholar] [CrossRef] [PubMed]
- Pilv, L.; Rätsep, A.; Oona, M.; Kalda, R. Prevalent Obstacles and Predictors for People Living with Type 2 Diabetes. Int. J. Fam. Med. 2012, 2012, 842912. [Google Scholar] [CrossRef]
- Abate, T.W.; Gedamu, H. Psychosocial and clinical factors associated with depression among individuals with diabetes in Bahir Dar City Administrative, Northwest Ethiopia. Ann. Gen. Psychiatry 2020, 19, 18. [Google Scholar] [CrossRef]
- Verma, S.; Agarwal, S.; Tashok, S.; Verma, A.; Giri, R. Cognitive impairment in type 2 diabetes and its impact on daily living and self-care: A case—Control study in Kanpur, North India. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102147. [Google Scholar] [CrossRef]
- Lara-Morales, A.; Gandarillas-Grande, A.; Díaz-Holgado, A.; Serrano-Gallardo, P. Psychosocial factors in adherence to pharmacological treatment and diabetes mellitus control in patients over 65. Aten. Primaria 2022, 54, 102302. [Google Scholar] [CrossRef]
- McBrien, K.A.; Naugler, C.; Ivers, N.; Weaver, R.G.; Campbell, D.; Desveaux, L.; Hemmelgarn, B.R.; Edwards, A.L.; Saad, N.; Nicholas, D.; et al. Barriers to care in patients with diabetes and poor glycemic control—A cross-sectional survey. PLoS ONE 2017, 12, e0176135. [Google Scholar] [CrossRef]
- Kuniss, N.; Kramer, G.; Müller, U.A.; Wolf, G.; Kloos, C. Diabetes related distress is high in inpatients with diabetes. Diabetol. Metab. Syndr. 2021, 13, 40. [Google Scholar] [CrossRef]
- Bak, E.; Marcisz, C.; Krzeminska, S.; Dobrzyn-Matusiak, D.; Foltyn, A.; Drosdzol-Cop, A. Relationships of Sexual Dysfunction with Depression and Acceptance of Illness in Women and Men with Type 2 Diabetes Mellitus. Int. J. Environ. Res. Public Health 2017, 14, 1073. [Google Scholar] [CrossRef]
- Abuhegazy, H.; Mujairi, A.; Banah, F.; Agdi, Y.; Elkeshishi, H.; Kamel, A.; Abdullah, A.; Elsheikh, M. Depression and Associated Risk Factors Among Type 2 Diabetic Patients: A Cross Sectional Study on a Convenience Sample from the Diabetic Center, Khamis Mushait; Saudi Arabia. Neuropsychiatr. Dis. Treat. 2022, 18, 1975–1984. [Google Scholar] [CrossRef] [PubMed]
- Naicker, K.; Johnson, J.A.; Skogen, J.C.; Manuel, D.; Øverland, S.; Sivertsen, B.; Colman, I. Type 2 Diabetes and Comorbid Symptoms of Depression and Anxiety: Longitudinal Associations with Mortality Risk. Diabetes Care 2017, 40, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Novak, J.R.; Anderson, J.R.; Johnson, M.D.; Hardy, N.R.; Walker, A.; Wilcox, A.; Lewis, V.L.; Robbins, D.C. Does Personality Matter in Diabetes Adherence? Exploring the Pathways between Neuroticism and Patient Adherence in Couples with Type 2 Diabetes. Appl. Psychol. Health Well Being 2017, 9, 207–227. [Google Scholar] [CrossRef]
- Shao, Y.; Yin, H.; Wan, C. Type D personality as a predictor of self-efficacy and social support in patients with type 2 diabetes mellitus. Neuropsychiatr. Dis. Treat. 2017, 13, 855–861. [Google Scholar] [CrossRef] [PubMed]
- Walker, R.J.; Garacci, E.; Palatnik, A.; Ozieh, M.N.; Egede, L.E. The Longitudinal Influence of Social Determinants of Health on Glycemic Control in Elderly Adults with Diabetes. Diabetes Care 2020, 43, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Young-Hyman, D.; de Groot, M.; Hill-Briggs, F.; Gonzalez, J.S.; Hood, K.; Peyrot, M. Response to Comment on Young-Hyman et al. Psychosocial Care for People with Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016;39:2126–2140. Diabetes Care 2018, 41, e33–e34. [Google Scholar] [CrossRef]
- Young, C.F.; Mullin, R.; Moverley, J.A.; Shubrook, J.H. Associations between diabetes-related distress and predicted cardiovascular complication risks in patients with type 2 diabetes. J. Osteopath. Med. 2022, 122, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Ebrahim, M.; Tamiru, D.; Hawulte, B.; Misgana, T. Prevalence, and associated factors of depression among diabetic outpatients attending diabetic clinic at public hospitals in Eastern Ethiopia: A cross-sectional study. SAGE Open Med. 2021, 9, 20503121211066244. [Google Scholar] [CrossRef]
- Engidaw, N.A.; Wubetu, A.D.; Basha, E.A. Prevalence of depression and its associated factors among patients with diabetes mellitus at Tirunesh-Beijing general hospital, Addis Ababa, Ethiopia. BMC Public Health 2020, 20, 266. [Google Scholar] [CrossRef]
- Adu, M.D.; Malabu, U.H.; Malau-Aduli, A.E.O.; Malau-Aduli, B.S. Enablers and barriers to effective diabetes self-management: A multi-national investigation. PLoS ONE 2019, 14, e0217771. [Google Scholar] [CrossRef]
- Ijaz, S.; Muazzam, A.; Malik, S. Development, and validation of psychosocial problems scale for type 2 diabetes (PPSTD). J. Pak. Med. Assoc. 2020, 70, 964–968. [Google Scholar] [CrossRef]
- Guo, H.; Wang, X.; Mao, T.; Li, X.; Wu, M.; Chen, J. How psychosocial outcomes impact on the self-reported health status in type 2 diabetes patients: Findings from the Diabetes Attitudes, Wishes and Needs (DAWN) study in eastern China. PLoS ONE 2018, 13, e0190484. [Google Scholar] [CrossRef] [PubMed]
- Ehtewish, H.; Arredouani, A.; El-Agnaf, O. Diagnostic, Prognostic, and Mechanistic Biomarkers of Diabetes Mellitus-Associated Cognitive Decline. Int. J. Mol. Sci. 2022, 23, 6144. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, J.M.; Baptista, F.I.; Macedo, M.P.; Ambrosio, A.F. Inside the Diabetic Brain: Role of Different Players Involved in Cognitive Decline. ACS Chem. Neurosci. 2016, 7, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Zilliox, L.A.; Chadrasekaran, K.; Kwan, J.Y.; Russell, J.W. Diabetes and Cognitive Impairment. Curr. Diab. Rep. 2016, 16, 87. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.Y.; Wang, X.G. Mild cognitive impairment in type 2 diabetes mellitus and related risk factors: A review. Rev. Neurosci. 2017, 28, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Feinkohl, I.; Price, J.F.; Strachan, M.W.; Frier, B.M. The impact of diabetes on cognitive decline: Potential vascular, metabolic, and psychosocial risk factors. Alzheimers. Res. Ther. 2015, 7, 46. [Google Scholar] [CrossRef] [PubMed]
- Pal, K.; Mukadam, N.; Petersen, I.; Cooper, C. Mild cognitive impairment, and progression to dementia in people with diabetes, prediabetes, and metabolic syndrome: A systematic review and meta-analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 1149–1160. [Google Scholar] [CrossRef]
- Wu, M.; Mei, F.; Hu, K.; Feng, L.; Wang, Z.; Gao, Q.; Chen, F.; Zhao, L.; Li, X.; Ma, B. Diabetic retinopathy and cognitive dysfunction: A systematic review and meta-analysis. Acta Diabetol. 2022, 59, 443–459. [Google Scholar] [CrossRef]
- Alghamdi, B.S. The neuroprotective role of melatonin in neurological disorders. J. Neurosci. Res. 2018, 96, 1136–1149. [Google Scholar] [CrossRef]
- de Groot, M.; Golden, S.H.; Wagner, J. Psychological conditions in adults with diabetes. Am. Psychol 2016, 71, 552–562. [Google Scholar] [CrossRef]
- Badescu, S.V.; Tataru, C.; Kobylinska, L.; Georgescu, E.L.; Zahiu, D.M.; Zagrean, A.M.; Zagrean, L. The association between Diabetes mellitus and Depression. J. Med. Life 2016, 9, 120–125. [Google Scholar]
- Berge, L.I.; Riise, T. Comorbidity between Type 2 Diabetes and Depression in the Adult Population: Directions of the Association and Its Possible Pathophysiological Mechanisms. Int. J. Endocrinol. 2015, 2015, 164760. [Google Scholar] [CrossRef]
- Meurs, M.; Roest, A.M.; Wolffenbuttel, B.H.; Stolk, R.P.; de Jonge, P.; Rosmalen, J.G. Association of Depressive and Anxiety Disorders with Diagnosed Versus Undiagnosed Diabetes: An Epidemiological Study of 90,686 Participants. Psychosom. Med. 2016, 78, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Samy, A.L.; Hairi, N.N.; Low, W.Y. Psychosocial stress, sleep deprivation, and its impact on type II diabetes mellitus: Policies, guidelines, and initiatives from Malaysia. FASEB Bioadv. 2021, 3, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Nous, A.; Engelborghs, S.; Smolders, I. Melatonin levels in the Alzheimer’s disease continuum: A systematic review. Alzheimers. Res. Ther. 2021, 13, 52. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 5. Facilitating Behavior Change and Well-being to Improve Health Outcomes: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43 (Suppl. S1), S48–S65. [Google Scholar] [CrossRef] [PubMed]
- Beck, J.; Greenwood, D.A.; Blanton, L.; Bollinger, S.T.; Butcher, M.K.; Condon, J.E.; Cypress, M.; Faulkner, P.; Fischl, A.H.; Francis, T.; et al. 2017 National Standards for Diabetes Self-Management Education and Support. Sci. Diabetes Self Manag. Care 2021, 47, 14–29. [Google Scholar] [CrossRef]
- Huang, J.; Peng, W.; Ding, S.; Xiong, S.; Liu, Z. Fear of hypoglycemia and associated factors in hospitalized patients with type 2 diabetes: A cross-sectional study. Sci. Rep. 2022, 12, 20338. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]


| Databases from 2013 to 2023 | Records Retrieved | Records after Title and Abstract Screening | Full-Text Articles Assessed for Eligibility | Studies Included after Quality Appraisal * |
|---|---|---|---|---|
| PubMed | 112 | 97 | 38 | 30 |
| Medline | 58 | 11 | 3 | 3 |
| EBSCOhost | 110 | 69 | 2 | 2 |
| EBSCO Discovery Service | 68 | 68 | 5 | 3 |
| Scopus | 82 | 32 | 2 | 2 |
| ScienceDirect | 49 | 1 | 0 | 0 |
| Web of Science | 115 | 88 | 15 | 10 |
| Total from all databases | 589 | 387 | 65 | 60 |
| Aspect | Description |
|---|---|
| Reviewers | Maarja Randväli, Toomas Toomsoo, Jekaterina Šteinmiller |
| Review aims and questions | Research Aim: The aim of this systematic review is to comprehensively examine and synthesize the existing international literature on the modeling of risk factors in type 2 diabetes for cognitive dysfunction, depression, and psychosocial challenges, focusing on an adult patient and understanding what similarities there are of the risk factors together. Revised Research Questions:
|
| Review type | A systematic review of the international literature. |
| Language | English |
| Study designs | Studies based on original research employing qualitative, quantitative, or mixed methods approaches will be considered for inclusion. Exclusions will be made for reviews, commentaries, letters, case reports, case studies, and books. Grey literature encompasses existing guidelines and profiles utilized in diverse healthcare environments, available online and retrievable through Google and other standard search engines. |
| PICO statement | Population (P): Adult patients, who had diagnosed with type 2 diabetes. Interest (I): Risk factors associated with complications of type 2 diabetes. Context (Co): Risk factors related to the association between cognitive dysfunction, depression, and psychosocial challenges in type 2 diabetes. The incidence, severity, or changes in cognitive dysfunction, depression, and psychosocial challenges and their impact on quality of life. |
| Literature search | Assistance will be sought from a librarian, through consultation, to help ensure the accuracy and precision of the search process. The following search terms were used: “type 2 diabetes” AND “cognitive disorders” AND “depression” AND “psychosocial problems” AND “risk factors”. These terms were combined using Boolean operators “OR” and “AND”. Comprehensive research and evidence on the main risk factors emerged from electronic databases. Electronic databases such as PubMed [including MEDLINE], Scopus, Cinahl, ProQuest, Web of Science, and Ebsco will be searched to retrieve studies published without time limits. Cross-referencing from the bibliographies of retrieved articles will be conducted, and current review papers will be considered to enhance the comprehensiveness of the search. Population Keywords: type 2 diabetes * OR risk factors * OR complications * Concept 1: Cognitive impairment: Cognitive dysfunction or mild cognitive problems or general cognitive problems. Risk factors for cognitive impairment OR causes of cognitive dysfunction*. Concept 2: Depression: Risk factors for depression in type 2 diabetes OR causes of depression in diabetes*. Concept 3: Psychosocial problems: Risk factors for psychosocial problems in type 2 diabetes OR causes of psychosocial problems in diabetes*. Search Strings: (Population Keywords) AND (Concept 1: Cognitive impairment Keywords). (Concept 2: depression in type 2 diabetes) AND (Concept 3: Psychosocial problems Setting Keywords). |
| Literature selection | The research team will independently review the titles, abstracts, and full texts of all original studies. Together, they will determine whether to include or exclude these studies, making their decisions in accordance with the established eligibility criteria. The inclusion criteria for original and scientific content are as follows: studies must be focused on the phenomenon in question; conducted within the context of medical services; involve medical personnel operating in a multidisciplinary team that addresses type 2 diabetes complications; and be published in peer-reviewed journals in English. Methodological checklists based on each article’s research design: Tools for Critical Appraisal—Systematic Reviews and Other Reviews. Types—Research Guides at Temple University. |
| Research synthesis | A data extraction table will be created to organize and import information from the chosen studies, categorizing their specifics. Additionally, an analytical framework will be established using tables to aggregate, summarize, and contrast the findings of these studies in the context of the review topic. The results of the review will be aligned with a theoretical framework that focuses on the primary risk factors associated with type 2 diabetes. |
| Equator guideline | The process of reporting the review will be guided by the methodological checklist of the extension of PRISMA for scoping reviews (PRISMA): http://www.equator-network.org/reporting-guidelines/prisma/ (accessed on 10 October 2023) |
| Funding sources/sponsors | This research received no funding to carry it out, but will obtain funding for publication in an open-access journal. |
| Conflicts of interest | The authors affirm that this research was conducted without any commercial or financial ties that might be interpreted as a conflict of interest. They retain copyright to this article and hold the intellectual property rights for this study and any other concepts derived from it. |
| Category | Subcategory | Substantive Code |
|---|---|---|
| Biological causes | Overweight, obesity [7,45,46] | Overweight, waist circumference, obesity, and body mass index (BMI) |
| Dysglycemia [47,48,49] | Hypo- and hyperglycemia, HbA1c, blood sugar fluctuation, and effect of hyperglycemia | |
| Comorbidities [20,47,55,56] | Micro- and macrovascular complications, hippocampal atrophy, damage to the HPA axis, inflammatory processes, immune inflammation, dyslipidemia, cardiac arrhythmias, overweight, obesity, dementia, pain, and sleep apnea | |
| Age [51,52,53,54] | Elderly, age groups, age over 65, and age at onset of illness | |
| Genetics [57,58] | Genetic predisposition, genetics, and NR3C1 gene | |
| Sex [47,50,53,54] | Female gender, more common in women, and gender difference | |
| Disease duration [48,49,50] | Duration of the disease, length of the disease, course of the disease, and duration of the disease for more than five years | |
| Behavioral causes | ||
| Lifestyle aspects [48,50,59] | Sleep disorders, disturbed circadian rhythm, fatigue, alcohol consumption, alcoholism, and lack of exercise | |
| Psychological causes | ||
| Anxiety, stress, distress [60,61,64,65] | Anxiety, fear of coping with the disease, anxiety about complications, fatigue, inability to take care of yourself, difficulty with self-care, anxiety about treatment, excessive worry, self-management when coping with the disease, anger and guilt, feelings of helplessness, adaptation problems, and negative attitude towards the disease | |
| Socio-economic causes | ||
| Support [50,52,56] | Family support, family size, social support, lack of support and need for support | |
| Economic status [31,46,47] | Low economic status, inequality, few opportunities, socioeconomic deficit, unemployment, and underemployment | |
| Education level [52,54,62] | Low level of education, incomplete level of education, and level of education |
| Category | Subcategory | Substantive Code |
|---|---|---|
| Psychological causes | ||
| Fear, anxiety, stress [74,80,81] | Fear of complications, fear of hypoglycemia, fear of meeting treatment goals, depression, anxiety, fear of changing lifestyle, anxiety disorders, phobias, anxiety about complications, anxiety about lack of knowledge, emotional experiences, emotional distress, concern about disease management, support, emotional burden, and health care services’ availability | |
| Personality characteristics [75,76] | Personality, personality traits, D-type personality, neuroticism, and temperament | |
| Social causes | ||
| Economic status [47,70,77] | Social inequality, economic difficulties, expensive treatment, regional location, and lack of health insurance | |
| Support [69,78,81,83] | Support, family involvement, support from healthcare professionals, social isolation, support from support networks (family and friends, spouse), and psychological support | |
| Education level [22,28,82] | Few skills and knowledge about coping with the disease, use of new technologies, knowledge about diabetes, lack of information, insufficient information, ineffective teaching method, economic opportunities, level of education, ability to find information, information on the web, understanding information, literacy and numeracy, and level of education | |
| Biological causes | ||
| Comorbidities [73,84] | Psychiatric diseases, dementia, obsessive compulsive behavior, sleep disorders, sleep apnea, depression, eating disorders, micro- and macrovascular complications, disease duration, obesity, malignant tumors, stroke, erectile dysfunction, and sexual dysfunction | |
| Sex [49,67,68,69] | Female gender, woman, and gender differences | |
| Dysglycemia [49,70,71,72] | Hyper- and hypoglycemia, blood sugar fluctuations, low blood sugar control, and HbA1c level | |
| Pharmacologic causes | ||
| Medications [49,71,73] | Drug administration, injection, drug side effects, duration of insulin treatment, and insulin |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Randväli, M.; Toomsoo, T.; Šteinmiller, J. The Main Risk Factors in Type 2 Diabetes for Cognitive Dysfunction, Depression, and Psychosocial Problems: A Systematic Review. Diabetology 2024, 5, 40-59. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology5010004
Randväli M, Toomsoo T, Šteinmiller J. The Main Risk Factors in Type 2 Diabetes for Cognitive Dysfunction, Depression, and Psychosocial Problems: A Systematic Review. Diabetology. 2024; 5(1):40-59. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology5010004
Chicago/Turabian StyleRandväli, Maarja, Toomas Toomsoo, and Jekaterina Šteinmiller. 2024. "The Main Risk Factors in Type 2 Diabetes for Cognitive Dysfunction, Depression, and Psychosocial Problems: A Systematic Review" Diabetology 5, no. 1: 40-59. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology5010004