
Language Profiles of School-Aged Children with 22q11.2 Copy Number Variants
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
- Were both cohorts (Leuven and Philadelphia) sufficiently comparable to combine the data?
- 2.
- Were language skills of the two CNV groups (22q11.2Dup, 22q11.2DS) comparable to the scores of typically developing peers (norm group scores)?
- 3.
- Which language skills did children with 22q11.2Dup show in relation to age-matched children with 22q11.2DS?
- 4.
- Did confounding factors have an impact on the language outcome, such as sex, comorbid ASD, ADHD, inheritance pattern, socioeconomic status (SES), and medical issues such as congenital heart disease (CHD), palatal defects, and hearing loss (HL)?
- 5.
- Did genotype–phenotype correlations reveal duplicated regions or genes on 22q11.2 critical for language development?
2. Materials and Methods
2.1. Participants
2.2. Research Design
2.3. Measurements
2.4. Data Analysis
3. Results
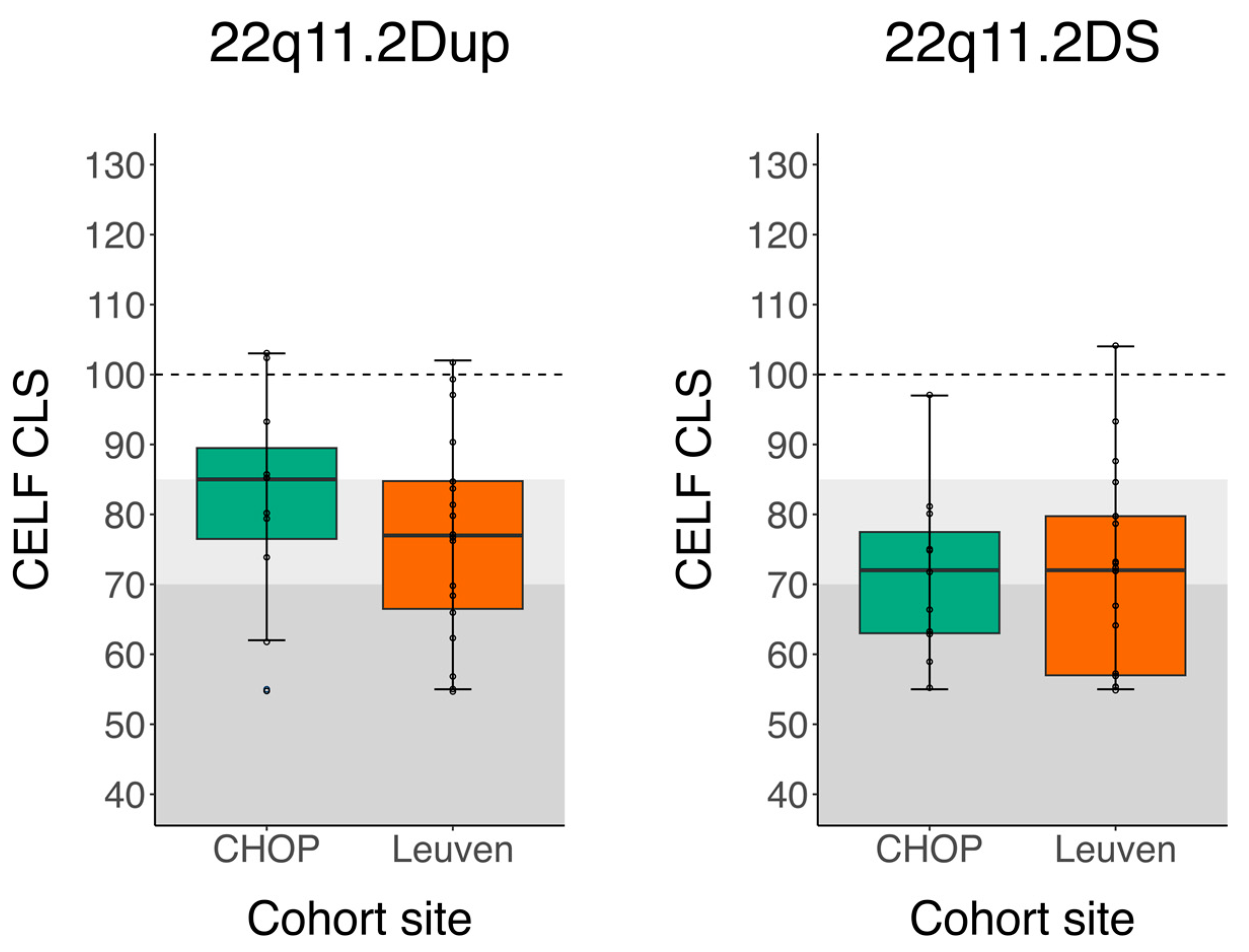
3.1. Cohort Site Differences
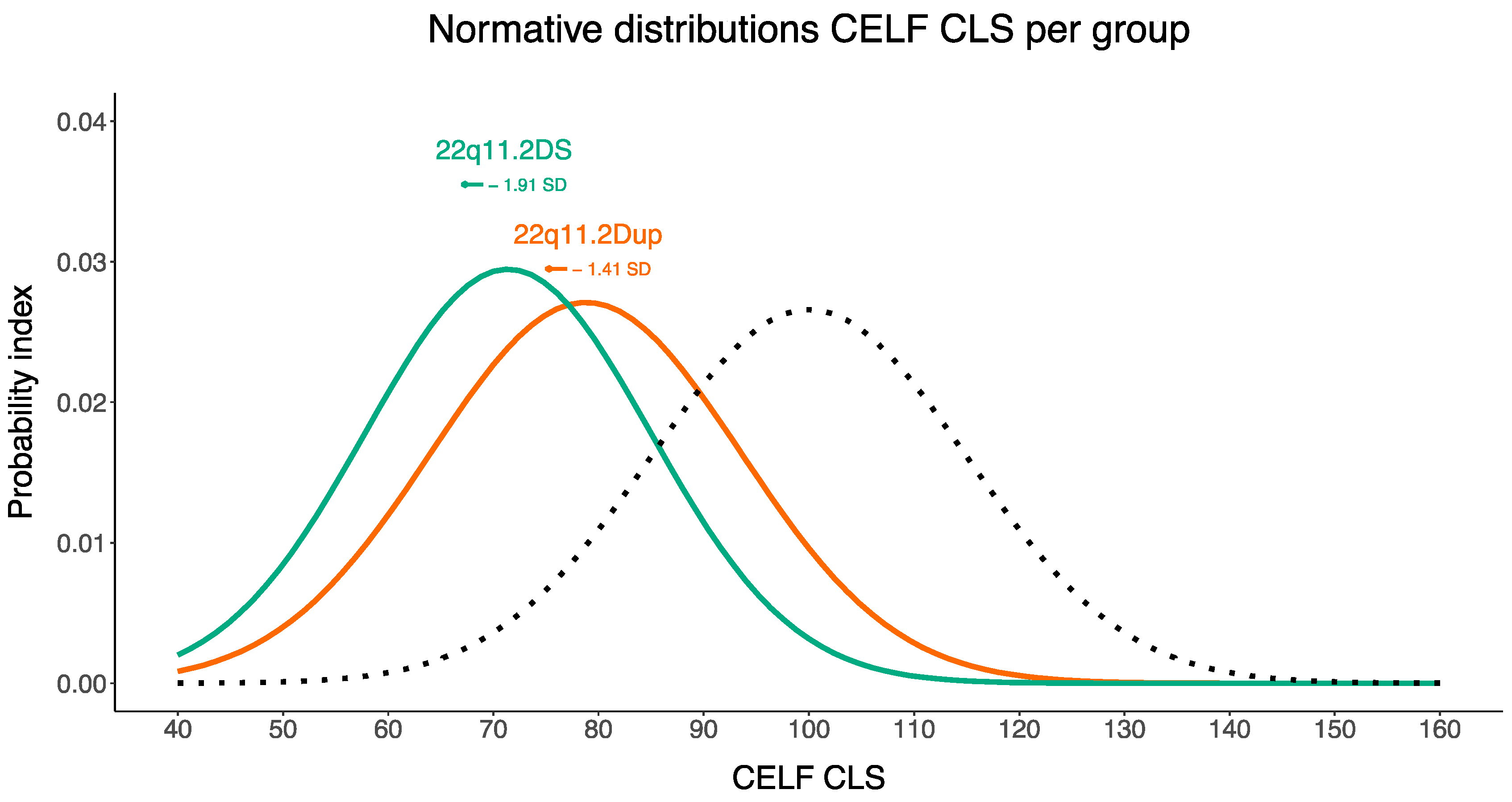
3.2. 22q11.2 CNVs Compared to Norm Group Scores
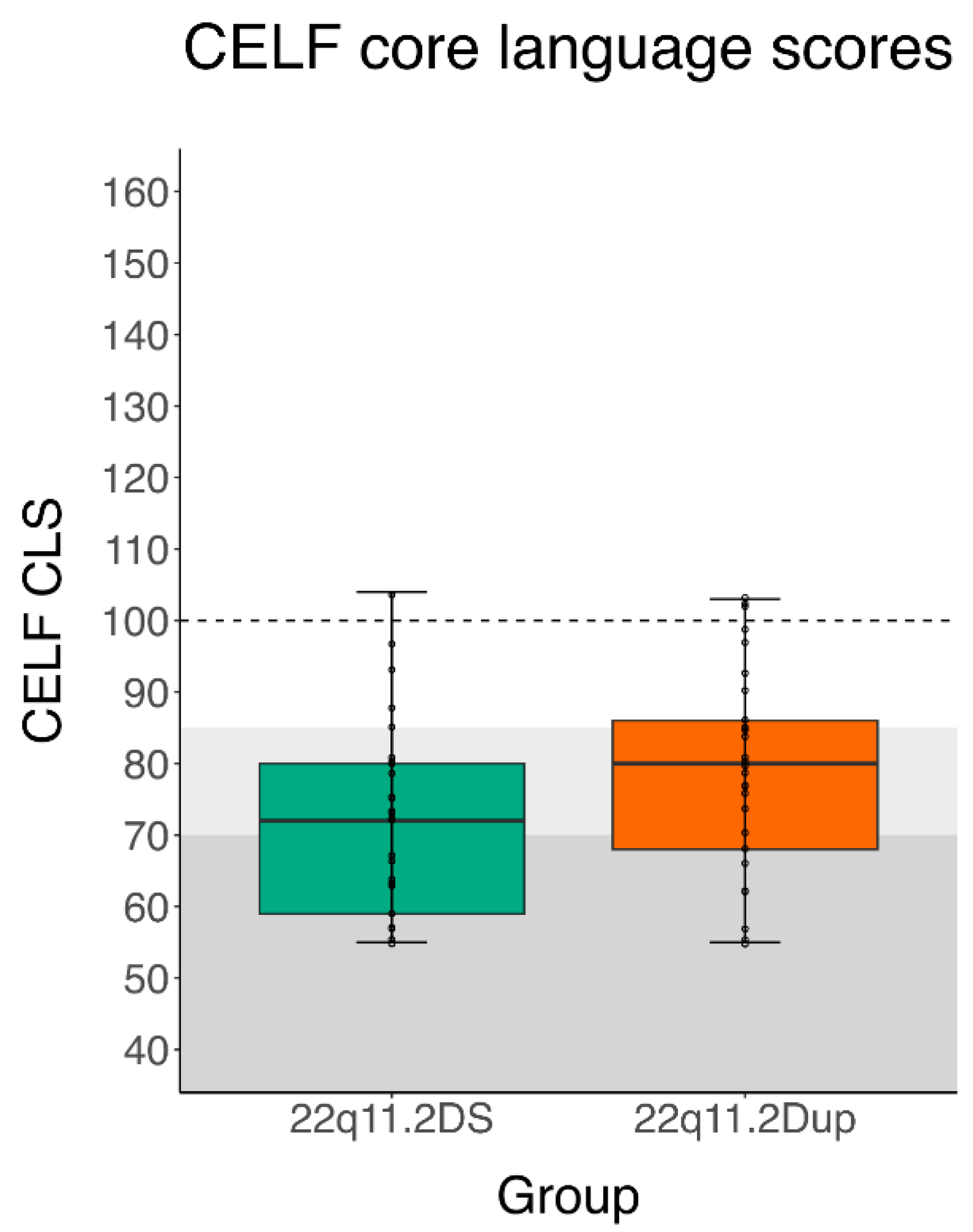
3.3. Quantitative and Qualitative Cross-CNV Comparisons
3.4. Influence of Confounding Factors
3.5. Genotype–Phenotype Correlations
4. Discussion
Strengths, Limitations, and Future
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Solot, C.B.; Sell, D.; Mayne, A.; Baylis, A.L.; Persson, C.; Jackson, O.; McDonald-McGinn, D.M. Speech-Language Disorders in 22q11.2 Deletion Syndrome: Best Practices for Diagnosis and Management. Am. J. Speech. Lang. Pathol. 2019, 28, 984–999. [Google Scholar] [CrossRef] [Green Version]
- Van Den Heuvel, E.; Manders, E.; Swillen, A.; Zink, I. Atypical Language Characteristics and Trajectories in Children with 22q11.2 Deletion Syndrome. J. Commun. Disord. 2018, 75, 37–56. [Google Scholar] [CrossRef]
- Wenger, T.L.; Miller, J.S.; DePolo, L.M.; de Marchena, A.B.; Clements, C.C.; Emanuel, B.S.; Zackai, E.H.; McDonald-McGinn, D.M.; Schultz, R.T. 22q11.2 Duplication Syndrome: Elevated Rate of Autism Spectrum Disorder and Need for Medical Screening. Mol. Autism. 2016, 7, 27. [Google Scholar] [CrossRef] [Green Version]
- Portnoï, M.-F. Microduplication 22q11.2: A New Chromosomal Syndrome. Eur. J. Med. Genet 2009, 52, 88–93. [Google Scholar] [CrossRef]
- Verbesselt, J.; Zink, I.; Breckpot, J.; Swillen, A. Cross-sectional and Longitudinal Findings in Patients with Proximal 22q11.2 Duplication: A Retrospective Chart Study. Am. J. Med. Genet. A 2022, 188, 46–57. [Google Scholar] [CrossRef]
- Van Campenhout, S.; Devriendt, K.; Breckpot, J.; Frijns, J.-P.; Peeters, H.; van Buggenhout, G.; van Esch, H.; Maes, B.; Swillen, A. Microduplication 22q11.2: A Description of the Clinical, Developmental and Behavioral Characteristics during Childhood. Genet. Couns. 2012, 23, 135–147. [Google Scholar]
- Wincent, J.; Bruno, D.L.; van Bon, B.W.M.; Bremer, A.; Stewart, H.; Bongers, E.M.H.F.; Ockeloen, C.W.; Willemsen, M.H.; Keays, D.A.D.; Baird, G.; et al. Sixteen New Cases Contributing to the Characterization of Patients with Distal 22q11.2 Microduplications. Mol. Syndromol. 2010, 1, 246–254. [Google Scholar] [CrossRef] [Green Version]
- Woodward, K.J.; Stampalia, J.; Vanyai, H.; Rijhumal, H.; Potts, K.; Taylor, F.; Peverall, J.; Grumball, T.; Sivamoorthy, S.; Alinejad-Rokny, H.; et al. Atypical Nested 22q11.2 Duplications between LCR22B and LCR22D Are Associated with Neurodevelopmental Phenotypes Including Autism Spectrum Disorder with Incomplete Penetrance. Mol. Genet. Genomic. Med. 2019, 7, e00507. [Google Scholar] [CrossRef] [Green Version]
- Cordovez, J.A.; Capasso, J.; Lingao, M.D.; Sadagopan, K.A.; Spaeth, G.L.; Wasserman, B.N.; Levin, A. Ocular Manifestations of 22q11.2 Microduplication. Ophthalmology 2014, 121, 392–398. [Google Scholar] [CrossRef]
- Courtens, W.; Schramme, I.; Laridon, A. Microduplication 22q11.2: A Benign Polymorphism or a Syndrome with a Very Large Clinical Variability and Reduced Penetrance?—Report of Two Families. Am. J. Med. Genet. A 2008, 146A, 758–763. [Google Scholar] [CrossRef]
- Demily, C.; Lesca, G.; Poisson, A.; Till, M.; Barcia, G.; Chatron, N.; Sanlaville, D.; Munnich, A. Additive Effect of Variably Penetrant 22q11.2 Duplication and Pathogenic Mutations in Autism Spectrum Disorder: To Which Extent Does the Tree Hide the Forest? J. Autism. Dev. Disord. 2018, 48, 2886–2889. [Google Scholar] [CrossRef]
- Yu, A.; Turbiville, D.; Xu, F.; Ray, J.W.; Britt, A.D.; Lupo, P.J.; Jain, S.K.; Shattuck, K.E.; Robinson, S.S.; Dong, J. Genotypic and Phenotypic Variability of 22q11.2 Microduplications: An Institutional Experience. Am. J. Med. Genet A 2019, 179, 2178–2189. [Google Scholar] [CrossRef]
- Verbesselt, J.; Van Den Heuvel, E.; Breckpot, J.; Zink, I.; Swillen, A. Parent-Reported Social-Communicative Skills of Children with 22q11.2 Copy Number Variants and Siblings. Genes 2022, 13, 1801. [Google Scholar] [CrossRef]
- Bishop, D.V.M. The Children’s Communication Checklist-2; Psychological Corporation: London, UK, 2003. [Google Scholar]
- Bishop, D.V.M. Children’s Communication Checklist-2: CCC-2-NL; Geurts, H.M., Ed.; Pearson Assessment and Information B.V.: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Swillen, A.; McDonald-Mcginn, D. Developmental Trajectories in 22q11.2 Deletion Syndrome. Am. J. Med. Genet. C Semin. Med. Genet. 2015, 169, 172–181. [Google Scholar] [CrossRef] [Green Version]
- Van Den Heuvel, E.; Jonkers, E.; Rombouts, E.; Manders, E.; Zink, I.; Swillen, A. Exploratory Study on Cognitive Abilities and Social Responsiveness in Children with 22q11.2 Deletion Syndrome (22q11DS) and Children with Idiopathic Intellectual Disability (IID). Res. Dev. Disabil. 2018, 81, 89–102. [Google Scholar] [CrossRef]
- McDonald-McGinn, D.M.; Sullivan, K.E.; Marino, B.; Philip, N.; Swillen, A.; Vorstman, J.A.S.; Zackai, E.H.; Emanuel, B.S.; Vermeesch, J.R.; Morrow, B.E.; et al. 22q11.2 Deletion Syndrome. Nat. Rev. Dis. Primers. 2015, 1, 15071. [Google Scholar] [CrossRef] [Green Version]
- Cummins, J. Language, Power and Pedagogy—Bilingual Children in the Crossfire; Multilingual Matters Ltd.: Clevedon, UK, 2000; ISBN 1-85359-474-1. [Google Scholar]
- Kohnert, K.; Ebert, K.D.; Pham, G.T. Language Disorders in Bilingual Children; Plural Publishing Inc.: San Diego, CA, USA, 2021; ISBN 9781635501896. [Google Scholar]
- De Houwer, A. Bilingual Development in Childhood (Elements in Child Development); Cambridge University Press: Cambridge, UK, 2021; ISBN 978-1-108-79139-7. [Google Scholar]
- Barre, N.; Morgan, A.; Doyle, L.W.; Anderson, P.J. Language Abilities in Children Who Were Very Preterm and/or Very Low Birth Weight: A Meta-Analysis. J. Pediatr. 2011, 158, 766–774.e1. [Google Scholar] [CrossRef]
- Crosbie, S.; Holm, A.; Wandschneider, S.; Hemsley, G. Narrative Skills of Children Born Preterm. Int. J. Lang. Commun. Disord. 2011, 46, 83–94. [Google Scholar] [CrossRef]
- Lieu, J.E.C.; Kenna, M.; Anne, S.; Davidson, L. Hearing Loss in Children: A Review. JAMA—J. Am. Med. Assoc. 2020, 324, 2195–2205. [Google Scholar] [CrossRef]
- OECD. Education at a Glance 2017: OECD Indicators; Education at a Glance; OECD Publishing: Paris, France, 2017; ISBN 9789264279766. [Google Scholar]
- UNESCO Institute for Statistics. International Standard Classification of Education: ISCED 2011; UNESCO Institute for Statistics: Paris, France, 2012; ISBN 9789291891238. [Google Scholar]
- Billett, J.; Cowie, M.R.; Gatzoulis, M.A.; Vonder Muhll, I.F.; Majeed, A. Comorbidity, Healthcare Utilisation and Process of Care Measures in Patients with Congenital Heart Disease in the UK: Cross-Sectional, Population-Based Study with Case-Control Analysis. Heart 2008, 94, 1194–1199. [Google Scholar] [CrossRef] [Green Version]
- Michel, O. The New WHO Classification of Hearing Loss: What Changed in 2021? HNO 2021, 69, 927–930. [Google Scholar] [CrossRef]
- Mervis, C.B.; Klein-Tasman, B.P. Methodological Issues in Group-Matching Designs: α Levels for Control Variable Comparisons and Measurement Characteristics of Control and Target Variables. J. Autism. Dev. Disord. 2004, 34, 7–17. [Google Scholar] [CrossRef]
- Mervis, C.B. Cross-Etiology Comparisons of Cognitive and Language Development. In Developmental Language Disorders—From Phenotypes to Etiologies; Lawrence Erlbaum Associates, Publishers: Mahwah, NJ, USA, 2004; pp. 153–186. ISBN 0-8058-4662-X. [Google Scholar]
- Kort, W.; Compaan, E.L.; Schittekatte, M.; Dekker, P.H. Clinical Evaluation of Language Fundamentals (CELF–4–NL) Nederlandse Versie. Handleiding [CELF–4 Dutch Adaptation Manual]; Pearson: Amsterdam, The Netherlands, 2010. [Google Scholar]
- De Jong, J. Clinical Evaluation of Language Fundamentals—Preschool—Second Edition. Nederlandstalige Versie. Handleiding [CELF-P2-NL: Dutch Adaptation Manual]; Pearson: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Semel, E.; Wiig, E.H.; Secord, W.A. Clinical Evaluation of Language Fundamentals, Fourth Edition (CELF-4); The Psychological Corporation/HA Harcourt Assessment Company: Toronto, ON, Canada, 2003. [Google Scholar]
- Wiig, E.H.; Semel, E.; Secord, W.A. Clinical Evaluation of Language Fundamentals–Fifth Edition (CELF-5); MN: NCS Pearson: Bloomington, IN, USA, 2013. [Google Scholar]
- Paslawski, T. The Clinical Evaluation of Language Fundamentals, Fourth Edition (CELF-4). Can. J. Sch. Psychol. 2005, 20, 129–134. [Google Scholar] [CrossRef]
- Semel, E.; Secord, W.A.; Wiig, E.H. Clinical Evaluation of Language Fundamentals 3rd Edition (CELF-3); Psychological Corporation: San Antonio, TX, USA, 1995. [Google Scholar]
- Coret, M.C.; McCrimmon, A.W. Test Review: Wiig, E.H., Semel, E., & Secord, W.A. (2013). Clinical Evaluation of Language Fundamentals–Fifth Edition (CELF-5). J. Psychoeduc. Assess. 2015, 33, 495–500. [Google Scholar] [CrossRef] [Green Version]
- Ellis, P.D. The Essential Guide to Effect Sizes; Cambridge University Press: Cambridge, UK, 2010; ISBN 978-0-521-19423-5. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- JASP Team. JASP (Version 0.16.4) [Computer Software]; Jasp Team: Amsterdam, The Netherlands, 2022. [Google Scholar]
- R Core Team R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017.
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; ISBN 978-3-319-24277-4. [Google Scholar]
- Butensky, A.; de Rinaldis, C.P.; Patel, S.; Edman, S.; Bailey, A.; McGinn, D.E.; Zackai, E.; Crowley, T.B.; McDonald-McGinn, D.M.; Min, J.; et al. Cardiac Evaluation of Patients with 22q11.2 Duplication Syndrome. Am. J. Med. Genet. A 2020, 185, 753–758. [Google Scholar] [CrossRef]
- Chawner, S.J.R.A.; Doherty, J.L.; Anney, R.J.L.; Antshel, K.M.; Bearden, C.E.; Bernier, R.; Chung, W.K.; Clements, C.C.; Curran, S.R.; Cuturilo, G.; et al. A Genetics-First Approach to Dissecting the Heterogeneity of Autism: Phenotypic Comparison of Autism Risk Copy Number Variants. Am. J. Psych. 2021, 178, 77–86. [Google Scholar] [CrossRef]
- Lin, A.; Vajdi, A.; Kushan-Wells, L.; Helleman, G.; Hansen, L.P.; Jonas, R.K.; Jalbrzikowski, M.; Kingsbury, L.; Raznahan, A.; Bearden, C.E. Reciprocal Copy Number Variations at 22q11.2 Produce Distinct and Convergent Neurobehavioral Impairments Relevant for Schizophrenia and Autism Spectrum Disorder. Biol. Psychiatry 2020, 88, 260–272. [Google Scholar] [CrossRef]
- Clements, C.C.; Wenger, T.L.; Zoltowski, A.R.; Bertollo, J.R.; Miller, J.S.; de Marchena, A.B.; Mitteer, L.M.; Carey, J.C.; Yerys, B.E.; Zackai, E.H.; et al. Critical Region within 22q11.2 Linked to Higher Rate of Autism Spectrum Disorder. Mol. Autism. 2017, 8, 58. [Google Scholar] [CrossRef] [Green Version]
- Dupont, C.; Grati, F.R.; Choy, K.W.; Jaillard, S.; Toutain, J.; Maurin, M.; Martínez-Conejero, J.A.; Beneteau, C.; Coussement, A.; Molina-Gomes, D.; et al. Prenatal Diagnosis of 24 Cases of Microduplication 22q11.2: An Investigation of Phenotype-Genotype Correlations. Prenat. Diagn. 2015, 35, 35–43. [Google Scholar] [CrossRef]
- Ensenauer, R.E.; Adeyinka, A.; Flynn, H.C.; Michels, V.V.; Lindor, N.M.; Dawson, D.B.; Thorland, E.C.; Lorentz, C.P.; Goldstein, J.L.; McDonald, M.T.; et al. Microduplication 22q11.2, an Emerging Syndrome: Clinical, Cytogenetic, and Molecular Analysis of Thirteen Patients. Am. J. Hum. Genet. 2003, 73, 1027–1040. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Liu, X.; Gao, H.; He, R.; Zhao, Y. Identifying of 22q11.2 Variations in Chinese Patients with Development Delay. BMC Med. Genom. 2021, 14, 26. [Google Scholar] [CrossRef]
- Olsen, L.; Sparsø, T.; Weinsheimer, S.M.; dos Santos, M.B.Q.; Mazin, W.; Rosengren, A.; Sanchez, X.C.; Hoeffding, L.K.; Schmock, H.; Baekvad-Hansen, M.; et al. Prevalence of Rearrangements in the 22q11.2 Region and Population-Based Risk of Neuropsychiatric and Developmental Disorders in a Danish Population: A Case-Cohort Study. Lancet Psych. 2018, 5, 573–580. [Google Scholar] [CrossRef] [Green Version]
- Campbell, I.M.; Sheppard, S.E.; Crowley, T.B.; McGinn, D.E.; Bailey, A.; McGinn, M.J.; Unolt, M.; Homans, J.F.; Chen, E.Y.; Salmons, H.I.; et al. What Is New with 22q? An Update from the 22q and You Center at the Children’s Hospital of Philadelphia. Am. J. Med. Genet. A 2018, 176, 2058–2069. [Google Scholar] [CrossRef]
- Biswas, A.B.; Furniss, F. Cognitive Phenotype and Psychiatric Disorder in 22q11.2 Deletion Syndrome: A Review. Res. Dev. Disabil. 2016, 53–54, 242–257. [Google Scholar] [CrossRef]
- Olszewski, A.K.; Radoeva, P.D.; Fremont, W.; Kates, W.R.; Antshel, K.M. Is Child Intelligence Associated with Parent and Sibling Intelligence in Individuals with Developmental Disorders? An Investigation in Youth with 22q11.2 Deletion (Velo-Cardio-Facial) Syndrome. Res. Dev. Disabil. 2014, 35, 3582–3590. [Google Scholar] [CrossRef] [Green Version]
- Fiksinski, A.M.; Bearden, C.E.; Bassett, A.S.; Kahn, R.S.; Zinkstok, J.R.; Hooper, S.R.; Tempelaar, W.; Vorstman, J.A.S.; Breetvelt, E.J. A Normative Chart for Cognitive Development in a Genetically Selected Population. Neuropsychopharmacology 2021, 47, 1379–1386. [Google Scholar] [CrossRef]
- De Smedt, B.; Devriendt, K.; Fryns, J.P.; Vogels, A.; Gewillig, M.; Swillen, A. Intellectual Abilities in a Large Sample of Children with Velo-Cardio-Facial Syndrome: An Update. J. Intellect. Disabil. Res. 2007, 51, 666–670. [Google Scholar] [CrossRef]
- Chow, E.W.C.; Watson, M.; Young, D.A.; Bassett, A.S. Neurocognitive Profile in 22q11 Deletion Syndrome and Schizophrenia. Schizophr. Res. 2006, 87, 270–278. [Google Scholar] [CrossRef] [Green Version]
- Modenato, C.; Martin-Brevet, S.; Moreau, C.A.; Rodriguez-Herreros, B.; Kumar, K.; Draganski, B.; Sønderby, I.E.; Jacquemont, S. Lessons Learned From Neuroimaging Studies of Copy Number Variants: A Systematic Review. Biol. Psych. 2021, 90, 596–610. [Google Scholar] [CrossRef]
- Modenato, C.; Kumar, K.; Moreau, C.; Martin-Brevet, S.; Huguet, G.; Schramm, C.; Jean-Louis, M.; Martin, C.O.; Younis, N.; Tamer, P.; et al. Effects of Eight Neuropsychiatric Copy Number Variants on Human Brain Structure. Transl. Psych. 2021, 11, 399. [Google Scholar] [CrossRef]
- Goldenberg, P. An Update on Common Chromosome Microdeletion and Microduplication Syndromes. Pediatr Ann 2018, 47, e198–e203. [Google Scholar] [CrossRef]
- Pizzo, L.; Jensen, M.; Polyak, A.; Rosenfeld, J.A.; Mannik, K.; Krishnan, A.; McCready, E.; Pichon, O.; le Caignec, C.; van Dijck, A.; et al. Rare Variants in the Genetic Background Modulate Cognitive and Developmental Phenotypes in Individuals Carrying Disease-Associated Variants. Genet. Med. 2019, 21, 816–825. [Google Scholar] [CrossRef] [Green Version]
- Persson, C.; Niklasson, L.; Óskarsdóttir, S.; Johansson, S.; Jönsson, R.; Söderpalm, E. Language Skills in 5–8-year-old Children with 22q11 Deletion Syndrome. Int. J. Lang. Commun. Disord. 2006, 41, 313–333. [Google Scholar] [CrossRef]
- Solot, C.B.; Gerdes, M.; Kirschner, R.E.; McDonald-McGinn, D.M.; Moss, E.; Woodin, M.; Aleman, D.; Zackai, E.H.; Wang, P.P. Communication Issues in 22q11.2 Deletion Syndrome: Children at Risk. Genet. Med. 2001, 3, 67–71. [Google Scholar] [CrossRef] [Green Version]
- Glaser, B.; Mumme, D.L.; Blasey, C.; Morris, M.A.; Dahoun, S.P.; Antonarakis, S.E.; Reiss, A.L.; Eliez, S. Language Skills in Children with Velocardiofacial Syndrome (Deletion 22q11.2). J. Pediatr. 2002, 140, 753–758. [Google Scholar] [CrossRef] [Green Version]
- Gerdes, M.; Solot, C.; Wang, P.P.; McDonald-McGinn, D.M.; Zackai, E.H. Taking Advantage of Early Diagnosis: Preschool Children with the 22q11.2 Deletion. Genet. Med. 2001, 3, 40–44. [Google Scholar] [CrossRef] [Green Version]
- Montojo, C.A.; Ibrahim, A.; Karlsgodt, K.H.; Chow, C.; Hilton, A.E.; Jonas, R.K.; Vesagas, T.K.; Bearden, C.E. Disrupted Working Memory Circuitry and Psychotic Symptoms in 22q11.2 Deletion Syndrome. Neuroimage Clin. 2014, 4, 392–402. [Google Scholar] [CrossRef] [Green Version]
- Antshel, K.M.; Fremont, W.; Ramanathan, S.; Kates, W.R. Predicting Cognition and Psychosis in Young Adults with 22q11.2 Deletion Syndrome. Schizophr. Bull. 2017, 43, 833–842. [Google Scholar] [CrossRef] [Green Version]
- Maeder, J.; Schneider, M.; Bostelmann, M.; Debbané, M.; Glaser, B.; Menghetti, S.; Schaer, M.; Eliez, S. Developmental Trajectories of Executive Functions in 22q11.2 Deletion Syndrome. J. Neurodev. Disord. 2016, 8, 10. [Google Scholar] [CrossRef] [Green Version]
- Swillen, A.; Moss, E.; Duijff, S. Neurodevelopmental Outcome in 22q11.2 Deletion Syndrome and Management. Am J Med. Genet. A 2018, 176, 2160–2166. [Google Scholar] [CrossRef]
- Maeder, J.; Zuber, S.; Schneider, M.; Kliegel, M.; Eliez, S. Age-Related Improvements in Executive Functions and Focal Attention in 22q11.2 Deletion Syndrome Vary Across Domain and Task. J. Int. Neuropsychol. Soc. 2022, 28, 337–350. [Google Scholar] [CrossRef]
- Moberg, P.J.; Richman, M.J.; Roalf, D.R.; Morse, C.L.; Graefe, A.C.; Brennan, L.; Vickers, K.; Tsering, W.; Kamath, V.; Turetsky, B.I.; et al. Neurocognitive Functioning in Patients with 22q11.2 Deletion Syndrome: A Meta-Analytic Review. Behav. Genet. 2018, 48, 259–270. [Google Scholar] [CrossRef]
- Van Den Heuvel, E.; ReuterskiöLd, C.; Solot, C.; Manders, E.; Swillen, A.; Zink, I. Referential Communication Abilities in Children with 22q11.2 Deletion Syndrome. Int. J. Speech Lang. Pathol. 2017, 19, 490–502. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| 22q11.2DS | 22q11.2Dup | |||
|---|---|---|---|---|
| Native Language (Country of Residence) | Dutch (Belgium) | English (USA) | Dutch (Belgium) | English (USA) |
| Sample Size (n) | 18 | 11 | 18 | 11 |
| Sex (n, %) Male Female | 12 (67%) | 8 (73%) | 10 (56%) | 7 (64%) |
| 6 (33%) | 3 (27%) | 8 (44%) | 4 (36%) | |
| Chronological age (yrs.mo) Average (SD) Median Range | ||||
| 10.10 (2.8) | 9.1 (2.5) | 10.10 (2.7) | 9.1 (2.5) | |
| 11.3 | 8.2 | 11.2 | 8.3 | |
| 6.7–15.2 | 6.4–13.2 | 6.11–15.5 | 6.4–13.3 | |
| Type of education (n, %) Special education Regular education Regular with assistance Homeschool Unknown | ||||
| 11 (61%) 6 (33%) | 2 (18%) 0 (0%) | 7 (39%) 6 (33%) | 3 (27%) 2 (18%) | |
| 1 (6%) 0 (0%) 0 (0%) | 6 (55%) 0 (0%) 3 (27%) | 5 (28%) 0 (0%) 0 (0%) | 3 (27%) 2 (18%) 1 (10%) | |
| SES High Middle Low Unknown | 8 (44%) 10 (56%) 0 (0%) 0 (0%) | 5 (45%) 5 (45%) 0 (0%) 1 (10%) | 11 (61%) 6 (33%) 1 (6%) 0 (0%) | 2 (18%) 4 (36%) 1 (10%) 4 (36%) |
| Speech-language delays (n, %) | 18/18 (100%) | 4/5 (80%) | 14/18 (78%) | 4/9 (44%) |
| Speech-language therapy (n, %) | 18/18 (100%) | 5/5 (100%) | 15/18 (83%) | 9/11 (82%) |
| Formal NDD diagnoses (n, %) | ||||
| ASD | 7/18 (39%) | 0/4 (0%) | 2/18 (11%) | 4/11 (36%) |
| ADHD | 3/18 (17%) | 0/4 (0%) | 3/18 (17%) | 3/10 (30%) |
| Inheritance pattern (n, %) De novo Inherited: Maternally inherited Paternally inherited Unknown | 17/18 (94%) | 4/11 (36%) | 8/18 (44%) | 1/11 (10%) |
| 1/18 (6%) 1/1 (100%) 0/1 (0%) | 0/11 (0%) 0/0 (0%) 0/0 (0%) | 7/18 (39%) 2/7 (29%) 5/7 (71%) | 5/11 (54%) 2/5 (40%) 3/5 (60%) | |
| 0/18 (0%) | 7/11 (64%) | 3/18 (17%) | 5/11 (54%) | |
| Medical issues (n, %) | ||||
| CHD | 10/18 (56%) | 7/11 (64%) | 2/18 (11%) | 1/11 (10%) |
| Palatal defects | 11/18 (61%) | 11/11 (100%) | 4/18 (22%) | 0/11 (0%) |
| Mild HL | 9/18 (50%) | 1/6 (17%) | 2/18 (11%) | 3/11 (27%) |
| 22q11.2Dup Dutch (n = 18) | 22q11.2Dup English (n = 11) | Statistical Outcomes Independent t-Test | 22q11.2DS Dutch (n = 18) | 22q11.2DS English (n = 11) | Statistical Outcomes Independent t-Test | |
|---|---|---|---|---|---|---|
| CELF CLS Mean (SD) Range 95% Confidence interval | 76.72 (14.67) 55.00–102.00 69.43–84.02 | 82.18 (14.84) 55.00–103.00 72.21–92.15 | t = 0.968 p = 0.342 | 71.33 (14.74) 55.00–104.00 64.00–78.66 | 71.46 (12.00) 55.00–97.00 63.39–79.52 | t = 0.023 p = 0.982 |
| CELF RS + FS Mean (SD) Range 95% Confidence interval | 11.83 (6.19) 2.00–24.00 8.76–14.91 | 13.09 (5.89) 4.00–22.00 9.13–17.05 | t = 0.541 p = 0.593 | 10.28 (5.42) 2.00–20.00 7.58–12.97 | 11.46 (3.91) 8.00–20.00 8.83–14.08 | W = 107.000 p = 0.734 |
| Scores | 22q11.2DS | 22q11.2Dup | Statistical Outcomes Paired t-Test | |
|---|---|---|---|---|
| CHOP + Leuven (n = 29) | CELF CLS Mean (SD) Range 95% Confidence interval | 71.38 (13.54) 55.00–104.00 66.23–76.53 | 78.79 (14.72) 55.00–103.00 73.19–84.39 | t = 1.982 p = 0.057 d = 0.368 |
| CELF RS + FS Mean (SD) Range 95% Confidence interval | 10.72 (4.86) 2.00–20.00 8.87–12.57 | 12.31 (6.00) 2.00–24.00 10.03–14.59 | t = 1.219 p = 0.233 d = 0.226 | |
| Leuven (n = 18) | CELF CLS Mean (SD) Range 95% Confidence interval | 71.33 (14.74) 55.00–104.00 64.00–78.66 | 76.72 (14.67) 55.00–102.00 69.43–84.02 | t = 1.153 p = 0.265 d = 0.272 |
| CELF RS + FS Mean (SD) Range 95% Confidence interval | 10.28 (5.42) 2.00–20.00 7.58–12.97 | 11.83 (6.19) 2.00–24.00 8.76–14.91 | t = 0.906 p = 0.378 d = 0.214 | |
| CHOP (n = 11) | CELF CLS Mean (SD) Range 95% Confidence interval | 71.46 (12.00) 55.00–97.00 63.39–79.52 | 82.18 (14.84) 55.00–103.00 72.21–92.15 | t = 1.681 p = 0.124 d = 0.507 |
| CELF RS + FS Mean (SD) Range 95% Confidence interval | 11.46 (3.91) 8.00–20.00 8.83–14.08 | 13.09 (5.89) 4.00–22.00 9.13–17.05 | t = 0.790 p = 0.448 d = 0.238 |
| 22q11.2DS | 22q11.2Dup | ||
|---|---|---|---|
| Composite scores | CELF CLS (< −1 SD & < −2 SD) Mild–moderate < −1 SD Severe < −2 SD | 24/29 (83%) 11/29 (38%) 13/29 (45%) | 18/29 (62%) 10/29 (34%) 8/29 (28%) |
| CELF RLI | 10/12 (83%) * | 19/27 (70%) | |
| CELF ELI | 11/12 (92%) | 18/28 (64%) | |
| Subtest scores Receptive | CFD | 21/29 (72%) | 17/27 (63%) |
| SS / SR | 14/27 (52%) | 15/28 (54%) | |
| WC | 11/19 (58%) | 10/29 (34%) | |
| Subtest scores Expressive | RS | 16/29 (55%) | 19/29 (66%) |
| FS | 22/29 (76%) | 15/29 (52%) | |
| WS (5.0–8.11 years) | 5/10 (50%) | 6/12 (50%) | |
| EV (5.0–9.11 years) | 4/7 (57%) | 2/7 (28%) | |
| 10.00 years) | 9/10 (90%) | 6/12 (50%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verbesselt, J.; Solot, C.B.; Van Den Heuvel, E.; Crowley, T.B.; Giunta, V.; Breckpot, J.; McDonald-McGinn, D.M.; Zink, I.; Swillen, A. Language Profiles of School-Aged Children with 22q11.2 Copy Number Variants. Genes 2023, 14, 679. https://0-doi-org.brum.beds.ac.uk/10.3390/genes14030679
Verbesselt J, Solot CB, Van Den Heuvel E, Crowley TB, Giunta V, Breckpot J, McDonald-McGinn DM, Zink I, Swillen A. Language Profiles of School-Aged Children with 22q11.2 Copy Number Variants. Genes. 2023; 14(3):679. https://0-doi-org.brum.beds.ac.uk/10.3390/genes14030679
Chicago/Turabian StyleVerbesselt, Jente, Cynthia B. Solot, Ellen Van Den Heuvel, T. Blaine Crowley, Victoria Giunta, Jeroen Breckpot, Donna M. McDonald-McGinn, Inge Zink, and Ann Swillen. 2023. "Language Profiles of School-Aged Children with 22q11.2 Copy Number Variants" Genes 14, no. 3: 679. https://0-doi-org.brum.beds.ac.uk/10.3390/genes14030679