
The Scale of Perceptions and Self-Participation in Hemodialysis: Development and Psychometric Evaluation

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants and Setting
2.3. Instruments
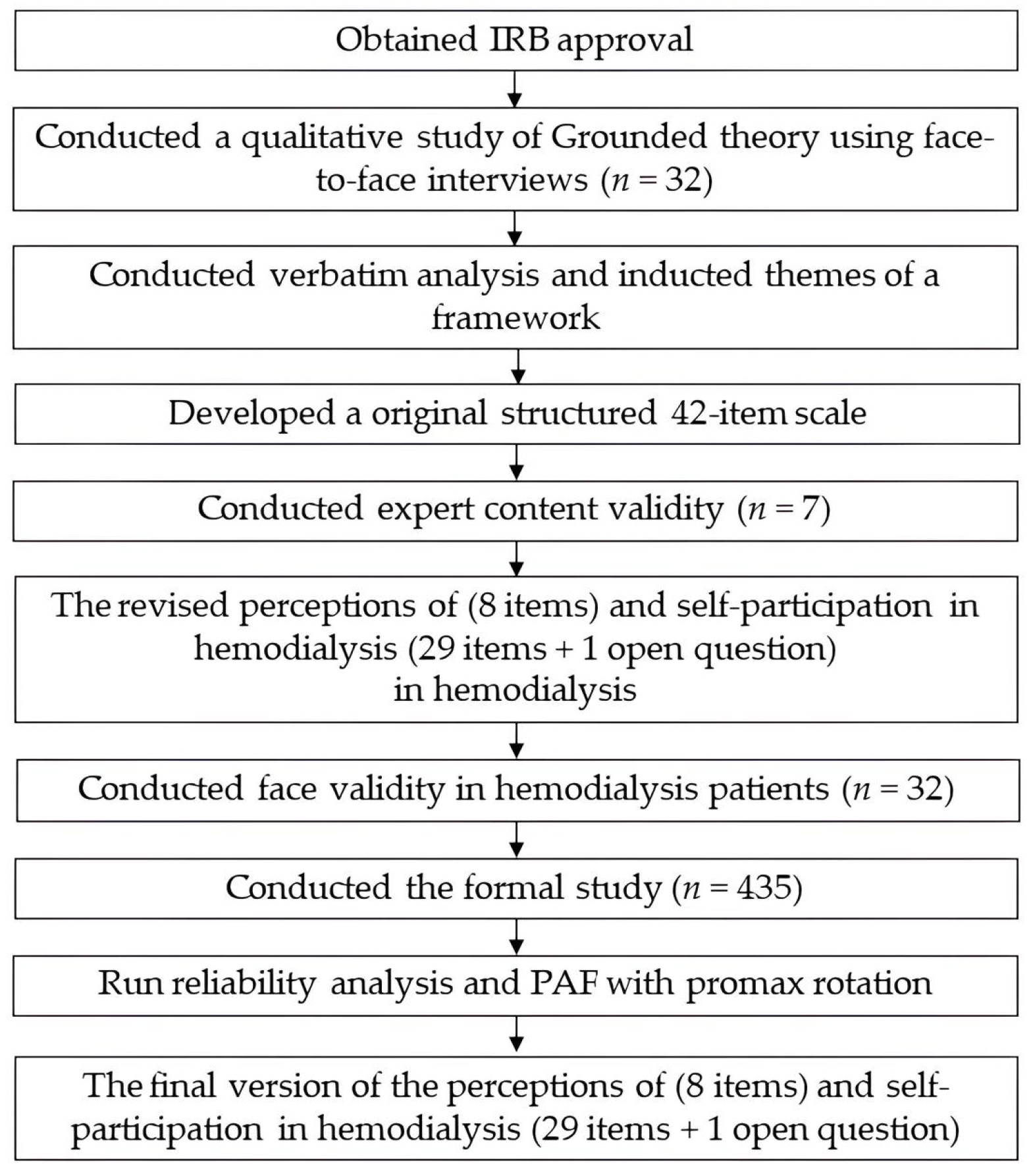
2.4. Procedure
2.5. Ethical Considerations
2.6. Data Analysis
3. Results
3.1. Sociodemographic and Clinical Characteristics of the Participants
3.2. Content Validity
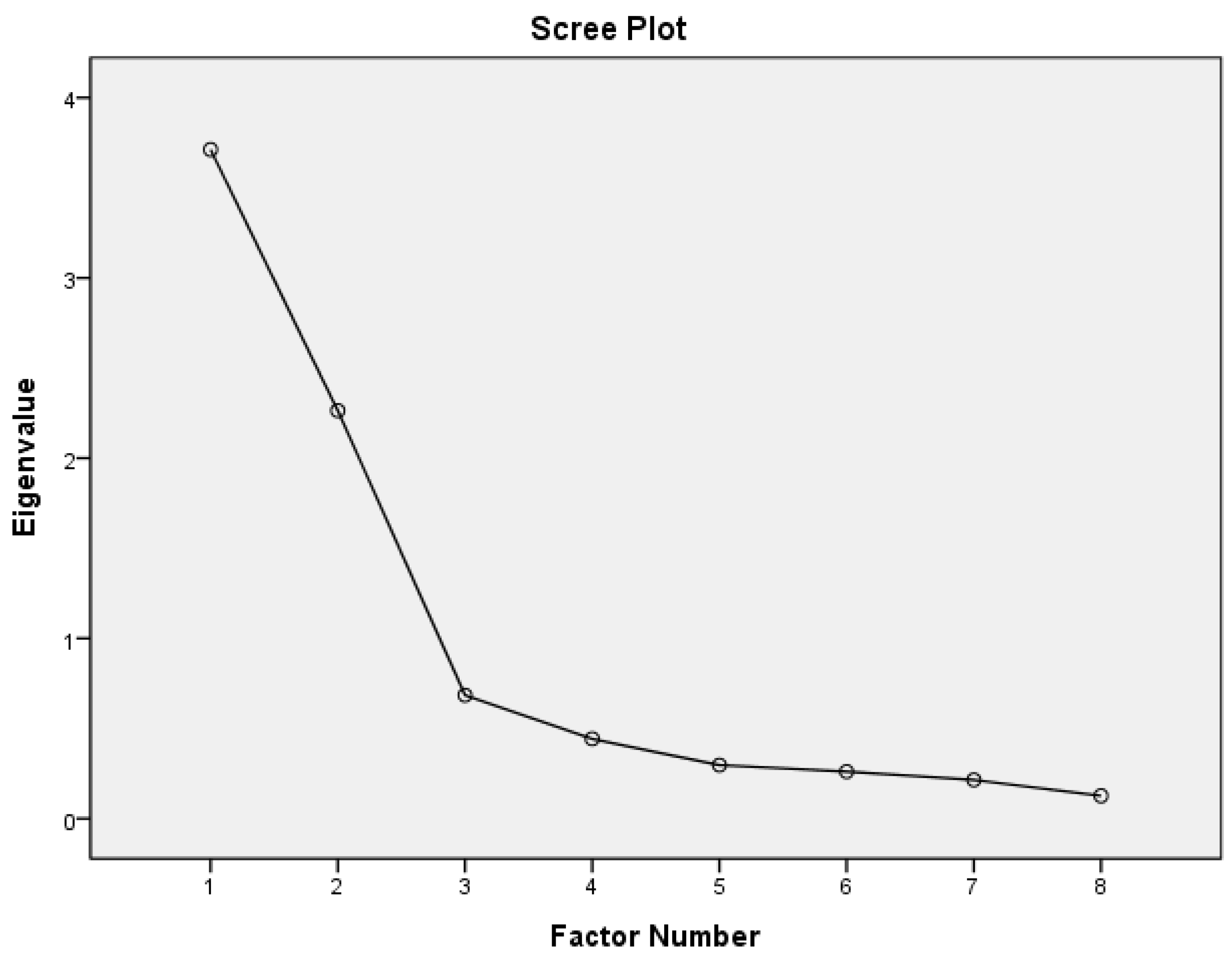
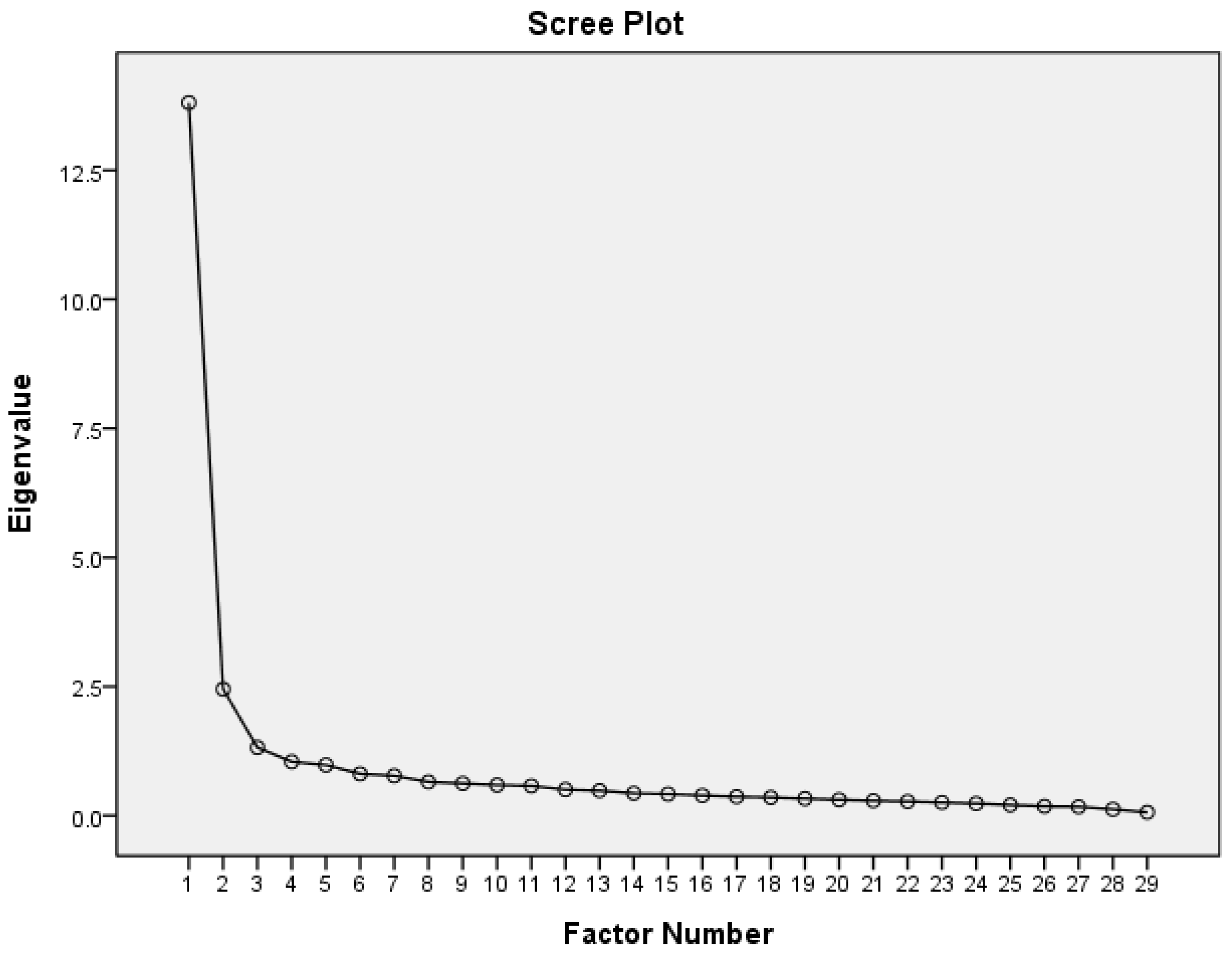
3.3. Construct Validity—Principal Axis Factoring of the Exploratory Factor Analysis
3.4. Construct Validity—Known Groups Method
3.5. Concurrent Validity of the Criterion-Related Validity
3.6. Internal Consistency Reliability
3.7. Descriptive Statistics of the SPSPHD
4. Discussion
4.1. The Aim of the Study and Content Validity
4.2. Construct Validity—PAF of the EFA
4.3. Construct Validity—Known Groups Method
4.4. Concurrent Validity of the Criterion-Related Validity
4.5. Internal Consistency Reliability
4.6. Descriptive Statistics of the SPSPHD
4.7. Limitation of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United States Renal Data System [USRDS]. 2022 USRDS Annual Data Report; National Institutes of Health: Bethesda, MD, USA, 2022. Available online: https://usrds-adr.niddk.nih.gov/2021/end-stage-renal-disease/1-incidence-prevalence-patient-characteristics-and-treatment-modalities (accessed on 22 November 2023).
- Flythe, J.E.; Powell, J.D.; Poulton, C.J.; Westreich, K.D.; Handler, L.; Reeve, B.B.; Carey, T.S. Patient-Reported Outcome Instruments for Physical Symptoms among Patients Receiving Maintenance Dialysis: A Systematic Review. Am. J. Kidney Dis. 2015, 66, 1033–1046. [Google Scholar] [CrossRef] [PubMed]
- Kraus, S.; Voon, V.; Potenza, M. Should Compulsive Sexual Behavior be Considered an Addiction? Addiction 2016, 111, 2097–10600. [Google Scholar] [CrossRef] [PubMed]
- Roshanravan, B.; Khatri, M.; Robinson-Cohen, C.; Levin, G.; Patel, K.V.; de Boer, I.H.; Seliger, S.; Ruzinski, J.; Himmelfarb, J.; Kestenbaum, B. A Prospective Study of Frailty in Nephrology-Referred Patients with CKD. Am. J. Kidney Dis. 2012, 60, 912–921. [Google Scholar] [CrossRef] [PubMed]
- Wagner, J.; Jhaveri, K.D.; Rosen, L.; Sunday, S.; Mathew, A.T.; Fishbane, S. Increased Bone Fractures among Elderly United States Hemodialysis Patients. Nephrol. Dial. Transplant. 2014, 29, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Weisbord, S.D.; Fried, L.F.; Arnold, R.M.; Fine, M.J.; Levenson, D.J.; Peterson, R.A.; Switzer, G.E. Prevalence, Severity, and Importance of Physical and Emotional Symptoms in Chronic Hemodialysis Patients. J. Am. Soc. Nephrol. 2005, 16, 2487–2494. [Google Scholar] [CrossRef] [PubMed]
- Xing, L.; Chen, R.; Diao, Y.; Qian, J.; You, C.; Jiang, X. Do Psychological Interventions Reduce Depression in Hemodialysis Patients?: A Meta-Analysis of Randomized Controlled Trials Following PRISMA. Medicine 2016, 95, e4675. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Society of Nephrology. 2021 Annual Report Kidney disease in Taiwan. J. Formos. Med. Assoc. 2022, 121 (Suppl. S1), S5–S11. Available online: https://www.tsn.org.tw/twrds/20220829/9863f7d3-2a86-4e8d-bcda-e1b4c3593c69/9863f7d3-2a86-4e8d-bcda-e1b4c3593c69.pdf (accessed on 22 November 2023).
- Castro, E.M.; Van Regenmortel, T.; Vanhaecht, K.; Sermeus, W.; Van Hecke, A. Patient Empowerment, Patient Participation and Patient-centeredness in Hospital Care: A Concept Analysis Based on a Literature Review. Patient Educ. Couns. 2016, 99, 1923–1939. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.M.; Funnell, M.M. Patient Empowerment: Myths and Misconceptions. Patient Educ. Couns. 2010, 79, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Borkman, T. Experiential Knowledge: A New Concept for the Analysis of Self-Help Groups. Soc. Serv. Rev. 1976, 50, 445–456. [Google Scholar] [CrossRef]
- Mok, E.; Martinson, I. Empowerment of Chinese Patients with Cancer Through Self-Help Groups in Hong Kong. Cancer Nurs. 2000, 23, 206–213. [Google Scholar] [CrossRef]
- Tsay, S.L.; Healstead, M. Self-Care Self-Efficacy, Depression, and Quality of Life among Patients Receiving Hemodialysis in Taiwan. Int. J. Nurs. Stud. 2002, 39, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Tobiano, G.; Bucknall, T.; Marshall, A.; Guinane, J.; Chaboyer, W. Nurses’ Views of Patient Participation in Nursing Care. J. Adv. Nurs. 2015, 71, 2741–2752. [Google Scholar] [CrossRef]
- Årestedt, L.; Martinsson, C.; Hjelm, C.; Uhlin, F.; Eldh, A.C. Patient Participation in Dialysis Care—A Qualitative Study of Patients’ and Health Professionals’ Perspectives. Health Expect. 2019, 22, 1285–1293. [Google Scholar] [CrossRef] [PubMed]
- Szu, L.Y.; Tsao, L.I.; Chen, S.C.; Ho, M.L. Self-Participation Experiences among Well-Adapted Hemodialysis Patients. Healthcare. 2021, 9, 1742. [Google Scholar] [CrossRef] [PubMed]
- Szu, L.Y.; Chang, C.H.; Hsieh, S.I.; Shih, W.M.; Huang, L.M.; Tsai, M.C.; Tseng, S.M. Factors Related to Quality of Life of Hemodialysis Patients during the COVID-19 Pandemic. Healthcare. 2023, 11, 1155. [Google Scholar] [CrossRef] [PubMed]
- Pett, M.A.; Lackey, N.R.; Sullivan, J.J. Making Sense of Factor Analysis: The Use of Factor Analysis for Instrument Development in Health Care Research; SAGE Publications: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Song, Y.C.; Lin, C.C. The Development and Testing of a New Hemodialysis Self-Management Instrument. J. Nurs. Healthc. Res. 2009, 5, 51–59. [Google Scholar]
- Curtin, R.B.; Johnson, H.K.; Schatell, D. The Peritoneal Dialysis Experience: Insights from Long-Term Patients. Nephrol. Nurs. J. 2004, 31, 615–624. [Google Scholar] [PubMed]
- Santos, P.R.; Capote, J.R.F.G.; Filho, J.R.M.C.; Ferreira, T.P.; Filho, J.N.G.; Oliveira, S.S. Religious Coping Methods Predict Depression and Quality of Life among End-stage Renal Disease Patients Undergoing Hemodialysis: A Cross-sectional Study. BMC Nephrol. 2017, 18, 197. [Google Scholar] [CrossRef] [PubMed]
- Al-Ghabeesh, S.H.; Alshraifeen, A.A.; Saifan, A.R.; Alnuaimi, K.M.; Masalha, H.A. Spirituality in the Lives of Patients with End-stage Renal Disease: A Systematic Review. JSTOR 2018, 57, 2461–2477. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Factors and Items (Cronbach’s α) | Pattern Matrix | Structure Matrix | Corrected Item-Total Correlation |
|---|---|---|---|
| Perceptions of Hemodialysis (α = 0.812) | |||
| Factor 1: Atmosphere during hemodialysis (α = 0.910) | |||
| 6. The friendly dialysis environment makes me feel warm inside. | 0.882 | 0.882 | 0.826 |
| 7. I have a pleasant time with my hemodialysis partners. | 0.865 | 0.863 | 0.801 |
| 8. I will refer to the experience of hemodialysis partners and learn about the life of self-care and dialysis. | 0.829 | 0.829 | 0.770 |
| 5. For my unfulfilled wish, I will continue to receive hemodialysis. | 0.778 | 0.778 | 0.749 |
| 4. In order to love my loved relatives or friends, I will continue to undergo hemodialysis. | 0.756 | 0.758 | 0.732 |
| Factor 2: Negative emotions during hemodialysis (α = 0.836) | |||
| 2. I need to rely on others to become a burden on my family and feel worthless. | 0.842 | 0.843 | 0.735 |
| 1. I feel sad and worthless. | 0.826 | 0.826 | 0.723 |
| 3. I feel discriminated against and feel worthless. | 0.719 | 0.719 | 0.650 |
| Initial Eigenvalues | Extraction Sums of Squared Loadings | |||||
|---|---|---|---|---|---|---|
| Factor | Total | % of Variance | Cumulative % | Total | % of Variance | Cumulative % |
| Scale of Perceptions of Hemodialysis | ||||||
| Factor 1: Atmosphere during hemodialysis | 3.71 | 46.40 | 46.40 | 3.40 | 42.48 | 42.48 |
| Factor 2: Negative emotions during hemodialysis | 2.26 | 28.30 | 74.70 | 1.91 | 23.86 | 66.34 |
| Scale of Self-Participation in Hemodialysis | ||||||
| Factor 1: Creating a new life | 13.81 | 47.61 | 47.61 | 13.42 | 46.28 | 46.28 |
| Factor 2: Implementation of self-care | 2.45 | 8.45 | 56.06 | 2.09 | 7.22 | 53.50 |
| Factor 3: Adjusting and facing hemodialysis | 1.32 | 4.56 | 60.62 | 0.90 | 3.09 | 56.59 |
| Factor 4: Active sharing and shared decisions | 1.04 | 3.60 | 64.22 | 0.67 | 2.32 | 58.91 |
| Factors and Items (Cronbach’s α) | Pattern Matrix | Structure Matrix | Corrected Item-Total Correlation |
|---|---|---|---|
| Self-Participation in Hemodialysis (α = 0.959) | |||
| Factor 1: Creating a new life (α = 0.927) | |||
| 28. I can develop interests in life. | 0.976 | 0.948 | 0.886 |
| 27. I can find the fun in my life. | 0.957 | 0.932 | 0.878 |
| 29. I can generate positive energy. | 0.853 | 0.902 | 0.852 |
| 22. I can actively attend outdoor activities or social events to adjust the dialysis schedule. | 0.543 | 0.734 | 0.733 |
| 24. I can find fun in my life or through outdoor activities. | 0.543 | 0.774 | 0.768 |
| 26. I can arrange my transportation to and from the dialysis unit. | 0.498 | 0.606 | 0.593 |
| 21. I can handle the negative emotions caused by dialysis. | 0.375 | 0.704 | 0.697 |
| Factor 2: Implementation of self-care (α = 0.902) | |||
| 16. I can check the bleeding (bruise) at the blood vessel and the infectious signs (for example redness, swelling, hotness, pain, etc.) at the injection site after hemodialysis. | 0.939 | 0.850 | 0.776 |
| 17. I can feel the care and respect for the medical staff. | 0.769 | 0.754 | 0.698 |
| 14. I can choose a suitable medical care strategy when I feel sick. | 0.731 | 0.836 | 0.799 |
| 12. I can check for blood flow vibration or sizzling sound in the hemodialysis vessels. | 0.723 | 0.697 | 0.632 |
| 13. I am confident that I can deal with physical discomfort after hemodialysis, such as palpitations, dizziness, cramps, itchy skin, etc. | 0.621 | 0.786 | 0.771 |
| 18. I gradually returned to the living conditions and work I used to have before hemodialysis. | 0.426 | 0.610 | 0.609 |
| 6. I can deal with the pain caused by needles in my way. | 0.373 | 0.634 | 0.605 |
| 10. I can prepare the supplies needed and food and recreation for myself before hemodialysis. | 0.369 | 0.637 | 0.622 |
| 15. I can accept advice or assistance from other hemodialysis patients to adjust my hemodialysis life. | 0.352 | 0.629 | 0.617 |
| Factor 3: Adjusting and facing the dialysis life (α = 0.893) | |||
| 7. When I don’t want to exercise because busy or tired, I can still exercise because of hemodialysis. | 0.814 | 0.679 | 0.610 |
| 8. I can adjust the water intake and diet based on the amount of fluid removal each time. | 0.742 | 0.817 | 0.758 |
| 5. I can force myself to do the things that are beneficial for hemodialysis. | 0.725 | 0.682 | 0.634 |
| 9. I can try various methods to satisfy the desire for water intake and a normal diet. | 0.650 | 0.786 | 0.728 |
| 2. I can adjust my diet and medicine at home and social events based on the blood laboratory report. | 0.632 | 0.750 | 0.719 |
| 3. I can adjust to the original lifestyle due to the hemodialysis life. | 0.540 | 0.754 | 0.730 |
| 4. I can seek spiritual sustenance such as religious beliefs and good relationships, and I can face hemodialysis positively. | 0.457 | 0.653 | 0.629 |
| 1. I can encourage myself to handle the life changes after hemodialysis. | 0.433 | 0.695 | 0.673 |
| 11. I can pay attention to the setting and blood pressure data on the hemodialysis machine. | 0.379 | 0.475 | 0.454 |
| Factor 4: Active sharing and shared decisions (α = 0.858) | |||
| 20. I treat medical staff or relatives and friends as people to talk to about life and disease-related issues. | 0.772 | 0.787 | 0.728 |
| 25. I can actively seek help from others. | 0.738 | 0.817 | 0.729 |
| 23. I can discuss with the medical staff or decide the treatment I’m expecting. | 0.698 | 0.783 | 0.711 |
| 19. I’m willing to share the experience of hemodialysis life and help other hemodialysis patients. | 0.506 | 0.707 | 0.647 |
| Factor | F1 | F2 | F1 | F2 | F3 | F4 |
|---|---|---|---|---|---|---|
| Scale of Perceptions of Hemodialysis | ||||||
| Factor 1: The atmosphere during hemodialysis | 1.00 | |||||
| Factor 2: The negative emotions during hemodialysis | −0.04 | 1.00 | ||||
| Scale of Self-Participation in Hemodialysis | ||||||
| Factor 1: Creating a new life | −0.18 ** | 0.38 ** | 1.00 | |||
| Factor 2: Implementation of self-care | −0.29 ** | 0.27 ** | 0.64 ** | 1.00 | ||
| Factor 3: Adjusting and facing hemodialysis life | −0.24 ** | 0.25 ** | 0.64 ** | 0.80 ** | 1.00 | |
| Factor 4: Active sharing and shared decisions | −0.27 ** | 0.20 ** | 0.77 ** | 0.65 ** | 0.59 ** | 1.00 |
| Factor | Grand Mean (SD) | Item | Mean (SD) |
|---|---|---|---|
| Scale of Perceptions of Hemodialysis | |||
| Factor 1: The atmosphere during hemodialysis | 5.21 (6.05) | 5 | 1.04 (1.21) |
| Factor 2: The negative emotions during hemodialysis | 10.14 (2.56) | 3 | 3.38 (0.33) |
| Scale of Self-Participation in Hemodialysis | |||
| Factor 1: Creating a new life | 18.72 (7.27) | 7 | 2.67 (1.04) |
| Factor 2: Implementation of self-care | 27.00 (7.37) | 9 | 3.00 (0.82) |
| Factor 3: Adjusting and facing hemodialysis life | 24.64 (7.70) | 9 | 2.74 (0.86) |
| Factor 4: Active sharing and shared decisions | 10.53 (4.16) | 4 | 2.63 (1.04) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szu, L.-Y.; Hsieh, S.-I.; Shih, W.-M.; Tsai, M.-C.; Tseng, S.-M. The Scale of Perceptions and Self-Participation in Hemodialysis: Development and Psychometric Evaluation. Healthcare 2023, 11, 3072. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11233072
Szu L-Y, Hsieh S-I, Shih W-M, Tsai M-C, Tseng S-M. The Scale of Perceptions and Self-Participation in Hemodialysis: Development and Psychometric Evaluation. Healthcare. 2023; 11(23):3072. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11233072
Chicago/Turabian StyleSzu, Li-Yun, Suh-Ing Hsieh, Whei-Mei Shih, Mei-Chu Tsai, and Su-Mei Tseng. 2023. "The Scale of Perceptions and Self-Participation in Hemodialysis: Development and Psychometric Evaluation" Healthcare 11, no. 23: 3072. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11233072