Micronuclei in Exfoliated Buccal Cells of Children Living in a Cluster Area of Salento (Southern Italy) with a High Incidence of Lung Cancer: The IMP.AIR Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
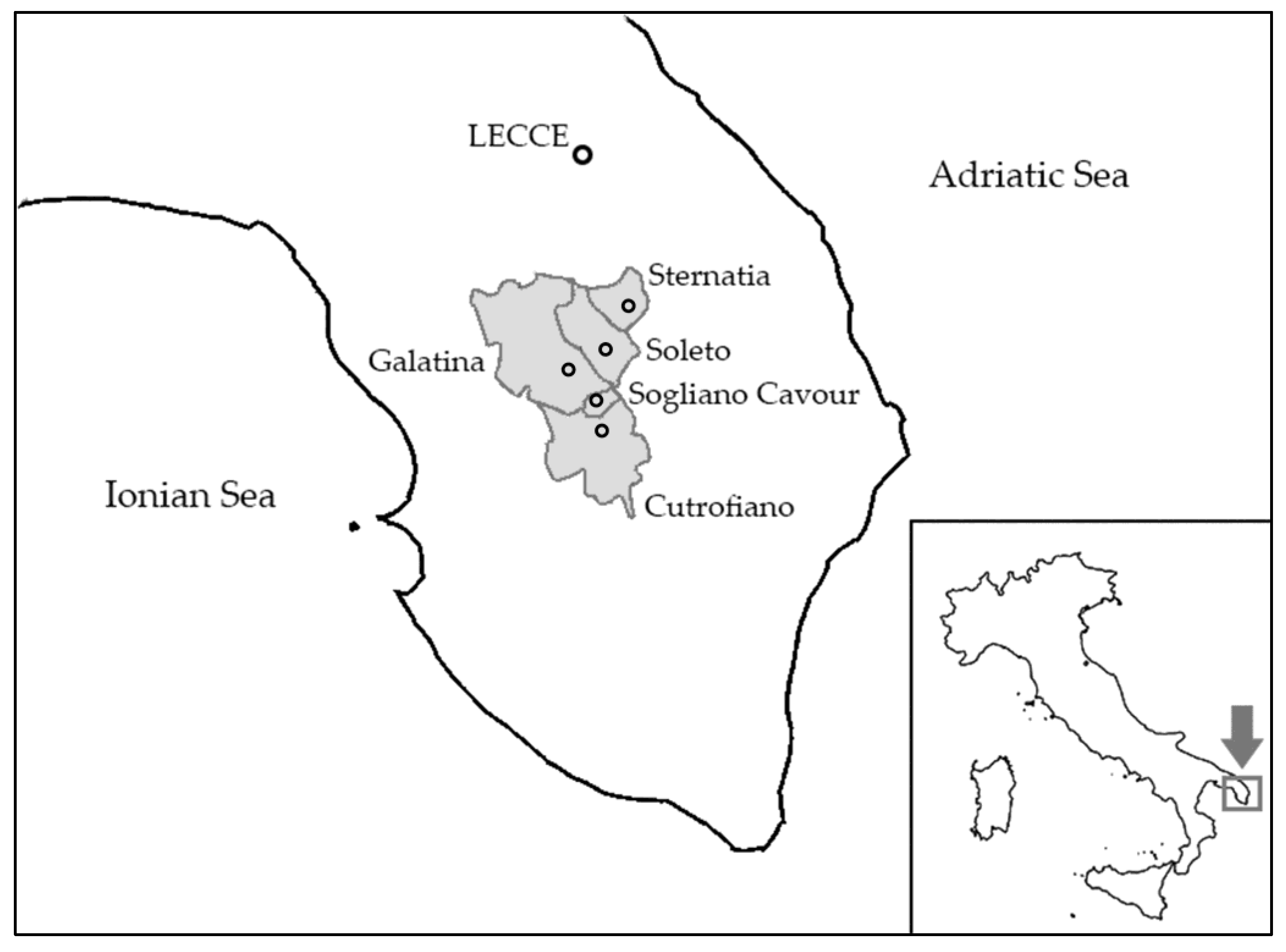
2.1. Study Design
2.2. Recruitment
2.3. Questionnaire Administration
2.4. Collection of Biological Samples
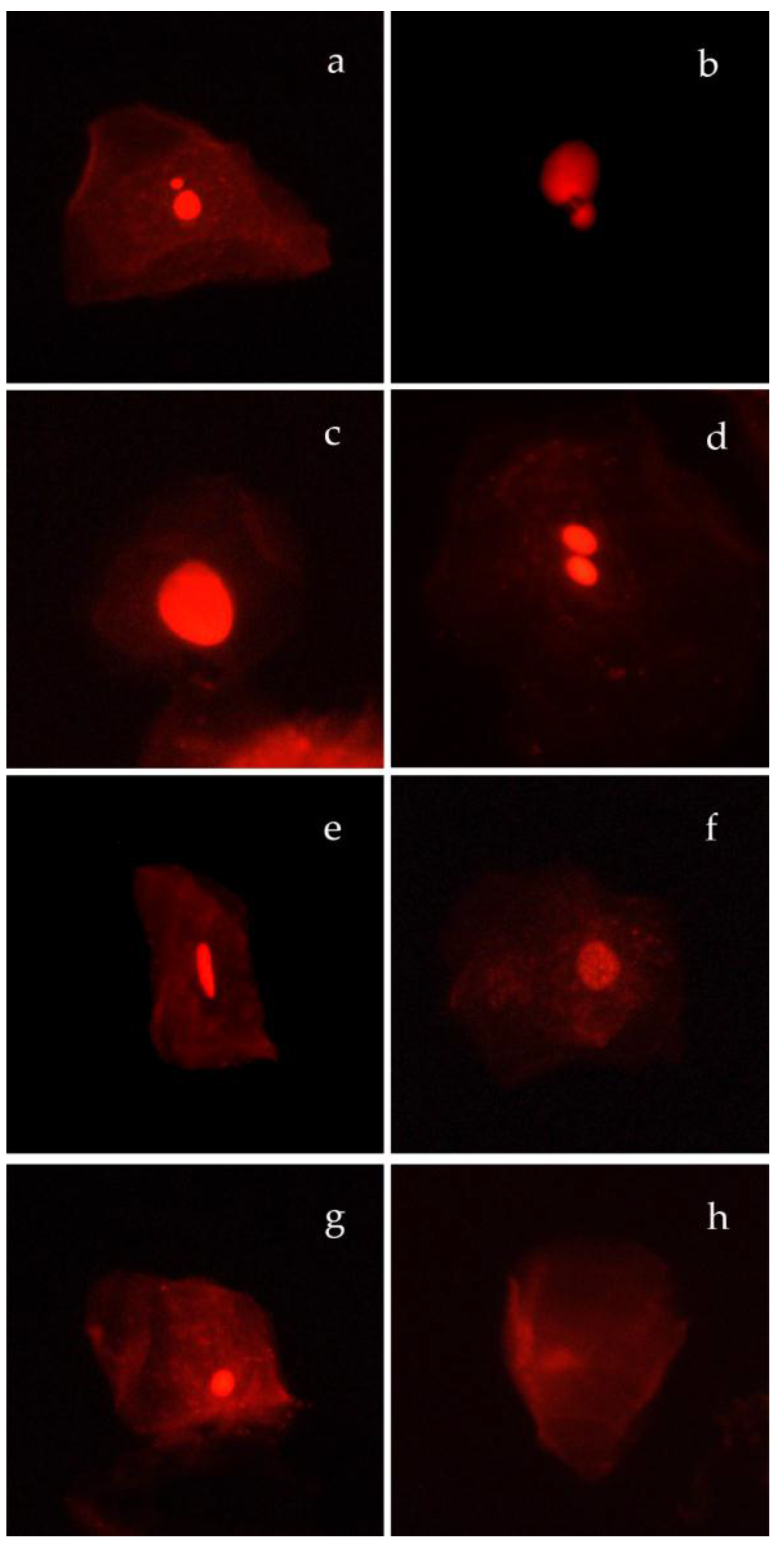
2.5. Buccal Micronucleus Cytome (BMCyt) Assay
2.6. Air Quality
2.7. Data Analysis
2.8. Ethical Aspects
3. Results
3.1. Characteristics of Recruited Children
3.2. Dietary Habits
3.3. Domestic Environment
3.4. Characteristics of Parents
3.5. Air Quality
3.6. The Buccal Micronucleus Cytome (BMCyt) Assay
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Islami, F.; Torre, L.A.; Jemal, A. Global trends of lung cancer mortality and smoking prevalence. Transl. Lung Cancer Res. 2015, 4, 327–338. [Google Scholar] [PubMed]
- Malhotra, J.; Malvezzi, M.; Negri, E.; La Vecchia, C.; Boffetta, P. Risk factors for lung cancer worldwide. Eur. Respir. J. 2016, 48, 889–902. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.M.; Chen, B.J.; Li, W.M.; Jiang, C.W. Risk factors on lung cancer: A meta-analysis. Chin. J. Evid.-Based Med. 2010, 10, 1446–1449. [Google Scholar]
- Kim, C.; Gao, Y.T.; Xiang, Y.B.; Barone-Adesi, F.; Zhang, Y.; Hosgood, H.D.; Ma, S.; Shu, X.O.; Ji, B.T.; Chow, W.H.; et al. Home kitchen ventilation, cooking fuels, and lung cancer risk in a prospective cohort of never smoking women in Shanghai, China. Int J. Cancer 2015, 136, 632–638. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer and World Health Organization. IARC: Outdoor Air Pollution a Leading Environmental Cause of Cancer Deaths. No. 221; World Health Organization: Lyon, France, 2013. [Google Scholar]
- Landrigan, P.J.; Kimmel, C.A.; Correa, A.; Ekenazi, B. Children’s health and the environment: Public health issue and challenges for risk assessment. Environ. Health Perspect. 2004, 112, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Bateson, T.F.; Schwartz, J. Children’s response to air pollutants. J. Toxicol. Environ. Health A 2008, 71, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Grigg, J. Particulate matter exposure in children: Relevance to chronic obstructive pulmonary disease. Proc. Am. Thorac. Soc. 2009, 6, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Wild, C.P.; Kleinjans, J. Children and increased susceptibility to environmental carcinogens: Evidence or empathy? Cancer Epidemiol. Biomark. Prev. 2003, 2, 1389–1394. [Google Scholar]
- Feretti, D.; Ceretti, E.; De Donno, A.; Moretti, M.; Carducci, A.; Bonetta, S.; Marrese, M.R.; Bonetti, A.; Covolo, L.; Bagordo, F.; et al. MAPEC_LIFE study group. Monitoring air pollution effects on children for supporting public health policy: The protocol of the prospective cohort MAPEC study. BMJ Open 2014, 4, e006096. [Google Scholar] [CrossRef]
- Adjiri, A. Identifying and targeting the cause of cancer is needed to cure cancer. Oncol. Ther. 2016, 4, 17–33. [Google Scholar] [CrossRef] [PubMed]
- Thomas, P.; Fenech, M. Buccal micronucleus cytome assay. Methods Mol. Biol. 2011, 682, 235–248. [Google Scholar] [PubMed]
- Bonassi, S.; Ugolini, D.; Kirsch-Volders, M.; Strömberg, U.; Vermeulen, R.; Tucker, J.D. Human population studies with cytogenetic biomarkers: Review of the literature and future prospective. Environ. Mol. Mutagen. 2005, 45, 258–270. [Google Scholar] [CrossRef] [PubMed]
- Samanta, S.; Dey, P. Micronucleus and its application. Diagn. Cytopathol. 2012, 40, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Celik, A.; Kanik, A. Genotoxicity of occupational exposure to wood dust: Micronucleus frequency and nuclear changes in exfoliated buccal mucosa cells. Environ. Mol. Mutagen. 2006, 47, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Holland, N.; Bolognesi, C.; Kirsch-Volders, M.; Bonassi, S.; Zeiger, E.; Knasmueller, S.; Fenech, M. The micronucleus assay in human buccal cells as a tool for biomonitoring DNA damage. The HUMN project perspective on current status and knowledge gaps. Mutat. Res. 2008, 659, 93–108. [Google Scholar] [CrossRef] [PubMed]
- Ceretti, E.; Feretti, D.; Viola, G.C.V.; Zerbini, I.; Limina, R.M.; Zani, C.; Capelli, M.; Lamera, R.; Donato, F.; Gelatti, U. DNA Damage in Buccal Mucosa Cells of Pre-School Children Exposed to High Levels of Urban Air Pollutants. PLoS ONE 2014, 9, e96524. [Google Scholar] [CrossRef] [PubMed]
- Torres-Bugarìn, O.; Fernàndez-Gracìa, A.; Torres-Mendoza, B.M.; Zavala-Aguirre, J.L.; Nava-Zavala, A.; Zamora-Perez, A.L. Genetic profile of overweight and obese school-age children. Toxicol. Environ. Chem. 2009, 91, 789–795. [Google Scholar] [CrossRef]
- Holland, N.; Fucic, A.; Merlo, D.F.; Sram, R.; Kirsch-Volders, M. Micronuclei in neonates and children: Effects of environmental, genetic, demographic and disease variables. Mutagenesis 2011, 26, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Neri, M.; Fucic, A.; Knudsen, L.E.; Lando, C.; Merlo, F.; Bonassi, S. Micronuclei frequency in children exposed to environmental mutagens: A review. Mutat. Res. 2003, 544, 243–254. [Google Scholar] [CrossRef] [PubMed]
- De Donno, A.; Grassi, T.; Ceretti, E.; Viola, G.C.V.; Levorato, S.; Vannini, S.; Salvatori, T.; Carducci, A.; Verani, M.; Bonetta, S.; et al. Air pollution biological effects in children living in Lecce (Italy) by buccal micronucleus cytome assay (the MAPEC_LIFE study). Int. J. Sus. Dev. Plann. 2016, 11, 500–510. [Google Scholar] [CrossRef]
- Wang, J.; Luo, X.; Xu, B.; Wei, J.; Zhang, Z.; Zhu, H. Elevated Oxidative Damage in Kitchen Workers in Chinese Restaurants. J. Occup. Health 2011, 53, 327–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katic, J.; Cemeli, E.; Baumgartner, A.; Laubenthal, J.; Bassano, I.; Stølevik, S.B.; Granum, B.; Namork, E.; Nygaard, U.C.; Løvik, M.; et al. Evaluation of the genotoxicity of 10 selected dietary/environmental compounds with the in vitro micronucleus cytokinesis-block assay in an interlaboratory comparison. Food Chem. Toxicol. 2010, 48, 2612–2623. [Google Scholar] [CrossRef] [PubMed]
- Kapka, L.; Baumgartner, A.; Siwińska, E.; Knudsen, L.E.; Anderson, D.; Mielżyńska, D. Environmental lead exposure increases micronuclei in children. Mutagenesis 2007, 22, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, P.; Wu, J.; Dhillon, V.; Fenech, M. Effect of dietary intervention on human micronucleus frequency in lymphocytes and buccal cells. Mutagenesis 2011, 26, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Bilancia, M.; Fedespina, A. Geographical clustering of lung cancer in the province of Lecce, Italy: 1992–2001. Int. J. Health Geogr. 2009, 8, 40. [Google Scholar] [CrossRef] [PubMed]
- Minelli, G.; Melcarne, A.; Fazzo, L.; Quarta, F.; Golizia, M.G.; De Maria, V.; Rashid, I.; Comba, P.; Conti, S. Il tumore polmonare nella Provincia di Lecce: Analisi di cluster di incidenza e mortalità. In Proceedings of the XVIII Convegno Annuale AIRTUM 2014, Taranto, Italy, 9–11 April 2014; Available online: https://www.scribd.com/document/217461724/XVIII-Convegno-annuale-AIRTUM-Taranto-9–11-aprile-2014-Atti-Definitivo-Web (accessed on 20 June 2018). (In Italian).
- Bagordo, F.; Migoni, D.; Grassi, T.; Serio, F.; Idolo, A.; Guido, M.; Zaccarelli, N.; Fanizzi, F.P.; De Donno, A. Using the DPSIR framework to identify factors influencing the quality of groundwater in Grecìa Salentina (Puglia, Italy). Rend. Lincei 2016, 27, 113–125. [Google Scholar] [CrossRef]
- Miglietta, P.P.; Toma, P.; Fanizzi, F.P.; De Donno, A.; Coluccia, B.; Migoni, D.; Bagordo, F.; Serio, F.A. Grey Water Footprint Assessment of Groundwater Chemical Pollution: Case Study in Salento (Southern Italy). Sustainability 2017, 9, 799. [Google Scholar] [CrossRef]
- Osservatorio Epidemiologico Regionale (OER) Puglia. Tavole Mortalità per Causa. Available online: https://www.sanita.puglia.it/web/oer/mortalita-e-cause (accessed on 11 June 2018). (In Italian).
- Villarini, M.; Levorato, S.; Salvatori, T.; Ceretti, E.; Bonetta, S.; Carducci, A.; Grassi, T.; Vannini, S.; Donato, F.; Bonetta, Si.; et al. Buccal micronucleus cytome assay in primary school children: A descriptive analysis of the MAPEC_LIFE multicenter cohort study. Int J. Hyg. Environ. Health 2018, 221, 883–892. [Google Scholar] [CrossRef] [PubMed]
- Bagordo, F.; De Donno, A.; Grassi, T.; Guido, M.; Devoti, G.; Ceretti, E.; Zani, C.; Feretti, D.; Villarini, M.; Moretti, M.; et al. Lifestyles and socio-cultural factors among children aged 6–8 years from five Italian towns: The MAPEC_LIFE study cohort. BMC Public Health 2017, 17, 233. [Google Scholar] [CrossRef] [PubMed]
- Agenzia Regionale per la Prevenzione e la Protezione dell’Ambiente (ARPA) Puglia. Rapporto Annuale Sulla Qualità dell’aria 2015. Available online: http://www.arpa.puglia.it/web/guest/rapporti_annuali_qa (accessed on 20 July 2018). (In Italian).
- EU, Directive 2008/50/EC of the European Parliament and of the Council of 21 May 2008 on Ambient Air Quality and Cleaner Air for Europe, 2008. EUR-lex. Available online: http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2008:152:0001:0044:EN:PDF (accessed on 18 June 2018).
- Zani, C.; Donato, F.; Grioni, S.; Viola, G.C.V.; Ceretti, E.; Feretti, D.; Festa, A.; Bonizzoni, S.; Bonetti, A.; Monarca, S.; et al. Feasibility and reliability of a questionnaire for evaluation of the exposure to indoor and outdoor air pollutants, diet and physical activity in 6–8-year-old children. Ann. Ig. 2015, 27, 646–656. [Google Scholar] [PubMed]
- Bolognesi, C.; Knasmueller, S.; Nersesyan, A.; Thomas, P.; Fenech, M. The HUMNxl scoring criteria for different cell types and nuclear anomalies in the buccal micronucleus cytome assay—An update and expanded photogallery. Mutat. Res. 2013, 753, 100–113. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Flegal, K.M.; Nicholls, D.; Jackson, A.A. Body mass index cut offs to define thinness in children and adolescents: International survey. BMJ 2007, 335, 194. [Google Scholar] [CrossRef] [PubMed]
- Law, M.R.; Hackshaw, A.K. Environmental tobacco smoke. Br. Med. Bull. 1996, 52, 22–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonassi, S.; Coskun, E.; Ceppi, M.; Lando, C.; Bolognesi, C.; Burgaz, S.; Holland, N.; Kirsh-Volders, M.; Knasmueller, S.; Zeiger, E.; et al. The Human MicroNucleus project on eXfoLiated buccal cells (HUMNxl): the role of life-style, host factors, occupational exposure, health status, and assay protocol. Mutat. Res. 2011, 728, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Huen, K.; Gunn, L.; Duramad, P.; Jeng, M.; Scalf, R.; Holland, N. Application of a geographic information system to explore associations between air pollution and micronucleus frequencies in African American children and adults. Environ. Mol. Mutagen. 2006, 47, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Marcon, A.; Fracasso, M.E.; Marchetti, P.; Doria, D.; Girardi, P.; Guarda, L.; Pesce, G.; Pironi, V.; Ricci, P.; De Marco, R. Outdoor formaldehyde and NO2 exposures and markers of genotoxicity in children living near chipboard industries. Environ. Health Perspect. 2014, 122, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Sisenando, H.A.; Batistuzzo de Medeiros, S.R.; Artaxo, P.; Saldiva, P.H.; Hacon Sde, S. Micronucleus frequency in children exposed to biomass burning in the Brazilian legal amazon region: A control case study. BMC Oral Health 2012, 12, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duan, J.; Tan, J.; Yang, L.; Wu, S.; Hao, J. Concentration, sources and ozone formation potential of volatile organic compounds (VOCs) during ozone episode in Beijing. Atmos. Res. 2008, 88, 25–35. [Google Scholar] [CrossRef]
- Ebi, K.L.; McGregor, G. Climate change, tropospheric ozone and particulate matter, and health impacts. Environ. Health Perspect. 2008, 116, 1449. [Google Scholar] [CrossRef] [PubMed]
- Grassi, T.; De Donno, A.; Bagordo, F.; Serio, F.; Piscitelli, P.; Ceretti, E.; Zani, C.; Viola, G.C.V.; Villarini, M.; Moretti, M.; et al. Socio-Economic and Environmental Factors Associated with Overweight and Obesity in Children Aged 6–8 Years Living in Five Italian Cities (the MAPEC_LIFE Cohort). Int. J. Environ. Res. Public Health 2016, 13, E1002. [Google Scholar] [CrossRef] [PubMed]
- Nardone, P.; Spinelli, A.; Lauria, L.; Buoncristiano, M.; Bucciarelli, M.; Andreozzi, S.; Gruppo OKkio alla SALUTE. Lo stato ponderale dei bambini. Il Sistema di sorveglianza. OKkio alla SALUTE: Risultati 2014; Stituto Superiore di Sanità: Roma, Italy, 2016; Available online: http://www.iss.it/binary/publ/cont/ONLINE_Okkio.pdf (accessed on 12 June 2018). (In Italian)
- Oostindjer, M.; Alexander, J.; Amdam, G.V.; Andersen, G.; Bryan, N.S.; Chen, D.; Corpet, D.E.; De Smet, S.; Dragsted, L.O.; Haug, A. The role of red and processed meat in colorectal cancer development: A perspective. Meat Sci. 2014, 97, 583–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zani, C.; Ceretti, E.; Grioni, S.; Viola, G.C.V.; Donato, F.; Feretti, D.; Festa, A.; Bonizzoni, S.; Bonetti, A.; Monarca, S.; et al. Are 6–8 year old Italian children moving away from the Mediterranean diet? Ann. Ig. 2016, 28, 339–348. [Google Scholar] [PubMed]
- World Health Organization. The World Health Report 2002. Reducing Risk, Promoting Healthy Life; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Sikorska-Jaroszynska, M.H.; Mielnik-Blaszczak, M.; Krawczyk, D.; Nasilowska-Barud, A.; Blaszczak, J. Passive smoking as an environmental health risk factor. Ann. Agric. Environ. Med. 2012, 19, 547–550. [Google Scholar] [PubMed]
- Ferrante, G.; Simoni, M.; Cibella, F.; Ferrara, F.; Liotta, G.; Malizia, V.; Corsello, G.; Viegi, G.; La Grutta, S. Third-hand smoke exposure and health hazards in children. Monaldi Arch. Chest Dis. 2013, 79, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Golley, R.K.; Hendrie, G.A.; Slater, A.; Corsini, N. Interventions that involve parents to improve children’s weight-related nutrition intake and activity patterns—what nutrition and activity targets and behaviour change techniques are associated with intervention effectiveness? Obes. Rev. 2011, 12, 114–130. [Google Scholar] [CrossRef] [PubMed]
- Dziubanek, G.; Marchwińska-Wyrwał, E.; Piekut, A.; Hajok, I.; Bilewicz-Wyrozumska, T.; Kuraszewska, B. Environmental Risks Perception—A Study of the awareness of families to threats in areas with increased health disorders in children. Ann. Agric. Environ. Med. 2013, 20, 555–558. [Google Scholar] [PubMed]
- Carducci, A.; Casini, B.; Donzelli, G.; Verani, M.; Bruni, B.; Ceretti, E.; Zani, C.; Carraro, E.; Bonetta, S.; Bagordo, F.; Grassi, T.; et al. Improving awareness of health hazards associated with air pollution in primary school children: Design and test of didactic tools. Appl. Environ. Educ. Commun. 2016, 15, 247–260. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Units of Measure | Value |
|---|---|---|
| Males | N (%) | 67 (54.9%) |
| Females | N (%) | 55 (45.1%) |
| Born in Italy | N (%) | 121 (99.2%) |
| 6 years old | N (%) | 34 (27.9%) |
| 7 years old | N (%) | 41 (33.6%) |
| 8 years old | N (%) | 47 (38.5%) |
| Average age | years ± standard deviation (SD) | 7.65 ± 0.94 |
| Average weight | kg ± SD | 28.3 ± 7.6 |
| Average height | cm ± SD | 127.2 ± 8.7 |
| Average BMI | kg/m2 ± SD | 17.247 ± 2.892 |
| UW | N (%) | 6 (4.9%) |
| NW | N (%) | 77 (63.1%) |
| OW | N (%) | 21 (17.2%) |
| OB | N (%) | 18 (14.8%) |
| Sports (≥3 times/week) | N (%) | 65 (53.3%) |
| Outdoor sports | N (%) | 38 (31.7%) |
| Swimming | N (%) | 11 (9.0%) |
| Outdoor play (>1 h/day) | N (%) | 85 (69.7%) |
| Food Categories | Average Consumption ± SD (times/week) |
|---|---|
| Bread | 6.97 ± 3.79 |
| Pasta/rice/soups | 10.36 ± 4.66 |
| Pizza and focaccia | 1.70 ± 0.91 |
| Legumes | 0.80 ± 0.73 |
| Vegetables | 9.55 ± 7.88 |
| Potatoes | 1.51 ± 1.30 |
| Fresh fruit | 20.67 ± 23.08 |
| Dried fruit | 1.10 ± 1.56 |
| Red or processed meat | 6.48 ± 3.62 |
| Poultry | 1.83 ± 1.19 |
| Fish | 3.74 ± 2.67 |
| Eggs | 1.33 ± 0.68 |
| Milk and dairy products | 16.42 ± 9.05 |
| Cakes | 14.28 ± 9.37 |
| Snacks | 1.88 ± 1.69 |
| Soft/fizzy drinks | 5.13 ± 6.64 |
| Olive oil 1 | 7.97 ± 4.31 |
| Butter 2 | 1.05 ± 1.85 |
| Variable | N (%) |
|---|---|
| Fried foods | 111 (91.0) |
| Wood-fired pizza | 97 (79.5) |
| Barbecued foods (wood/charcoal) | 72 (59.0) |
| Foods cooked on the griddle | 59 (48.4) |
| Toasted bread | 45 (36.9) |
| Smoked foods | 23 (18.9) |
| Variable | N (%) |
|---|---|
| Residence in high-traffic areas | 34 (27.9%) |
| Residence near roads with high traffic of heavy vehicles | 19 (15.7%) |
| Fuel used for heating | |
| Methane gas | 107 (82.3%) |
| Wood | 12 (9.2%) |
| Diesel | 5 (3.8%) |
| Electricity | 5 (3.8%) |
| Fuel used for cooking | |
| Methane gas | 121 (91.0%) |
| Electricity | 9 (6.8%) |
| Wood | 3 (2.3%) |
| Presence of fireplace | 61 (50.0%) |
| Presence of gas boiler inside home | 4 (3.3%) |
| Living with smokers inside the dwelling | 25 (20.5%) |
| Frequent staying in the kitchen during food cooking | 23 (19.2%) |
| Cooking on the griddle/barbecue | 83 (68.6%) |
| Use of solvents for hobbies | 2 (1.6%) |
| Variable | Mother N (%) | Father N (%) |
|---|---|---|
| Born in Italy | 110 (90.2%) | 112 (92.6%) |
| High school education or greater | 86 (70.5%) | 72 (59.5%) |
| Employment rate | 58 (47.5%) | 106 (91.4%) |
| Smoking habits | 15 (12.3%) | 47 (38.8%) |
| Variable | PM2.5 (µg/m³) | NO2 (µg/m³) | CO (mg/m³) | SO2 (µg/m³) | O3 * (µg/m³) |
|---|---|---|---|---|---|
| Annual mean | 17.2 | 11.4 | 0.51 | 4.23 | 103.3 |
| Maximum 24-h mean value | 60.2 | 29.3 | 1.3 | 8.48 | 166 |
| Biomarkers (‰) 1 | IMP.AIR Study 2 | Lecce (MAPEC_LIFE Study) 3 [33] |
|---|---|---|
| MNC | 0.49 ± 0.65 | 0.24 ± 0.32 * |
| NBUD | 0.10 ± 0.33 | 0.09 ± 0.26 |
| BC | 1.70 ± 1.72 | 0.19 ± 0.41 * |
| BNC | 2.73 ± 1.79 | 3.26 ± 1.88 |
| CCC | 51.20 ± 17.97 | 26.60 ± 18.59 * |
| KHC | 8.50 ± 5.74 | 13.29 ± 13.90 * |
| PYK | 0.64 ± 1.00 | 0.11 ± 0.31 * |
| KYL | 16.00 ± 4.76 | 28.62 ± 21.05 * |
| Independent Variables | OR | CI (95%) | p-Value |
|---|---|---|---|
| Male | 0.802 | 0.293–0.195 | 0.667 |
| Obesity | 3.849 | 1.140–12.994 | 0.030 |
| Residence in high traffic areas | 1.624 | 0.539–4.897 | 0.389 |
| Use of fireplace (>8 days/month) | 3.585 | 0.724–17.756 | 0.118 |
| Red or processed meat consumption (>4 times/week) | 3.622 | 1.154–11.365 | 0.027 |
| Vegetables consumption (>3 times/week) | 0.378 | 0.122–1.175 | 0.093 |
| Sport (≥3 times/week) | 0.692 | 0.241–1.982 | 0.492 |
| Father with high school diploma | 0.873 | 0.308–2.478 | 0.799 |
| Mother with high school diploma | 1.672 | 0.462–6.043 | 0.433 |
| Smoking father | 0.955 | 0.346–2.637 | 0.929 |
| Smoking mother | 5.511 | 1.156–26.274 | 0.032 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Idolo, A.; Grassi, T.; Bagordo, F.; Panico, A.; De Giorgi, M.; Serio, F.; Guido, M.; Piscitelli, P.; De Filippis, G.; Raho, A.; et al. Micronuclei in Exfoliated Buccal Cells of Children Living in a Cluster Area of Salento (Southern Italy) with a High Incidence of Lung Cancer: The IMP.AIR Study. Int. J. Environ. Res. Public Health 2018, 15, 1659. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081659
Idolo A, Grassi T, Bagordo F, Panico A, De Giorgi M, Serio F, Guido M, Piscitelli P, De Filippis G, Raho A, et al. Micronuclei in Exfoliated Buccal Cells of Children Living in a Cluster Area of Salento (Southern Italy) with a High Incidence of Lung Cancer: The IMP.AIR Study. International Journal of Environmental Research and Public Health. 2018; 15(8):1659. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081659
Chicago/Turabian StyleIdolo, Adele, Tiziana Grassi, Francesco Bagordo, Alessandra Panico, Mattia De Giorgi, Francesca Serio, Marcello Guido, Prisco Piscitelli, Giovanni De Filippis, Annamaria Raho, and et al. 2018. "Micronuclei in Exfoliated Buccal Cells of Children Living in a Cluster Area of Salento (Southern Italy) with a High Incidence of Lung Cancer: The IMP.AIR Study" International Journal of Environmental Research and Public Health 15, no. 8: 1659. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081659