How Should Forests Be Characterized in Regard to Human Health? Evidence from Existing Literature

 , ,
, ,  and
and
Abstract
:1. Introduction
- the extent to which forests are studied and described in studies of human health;
- the extent to which patterns can be identified between forest variables and physiological health effects.
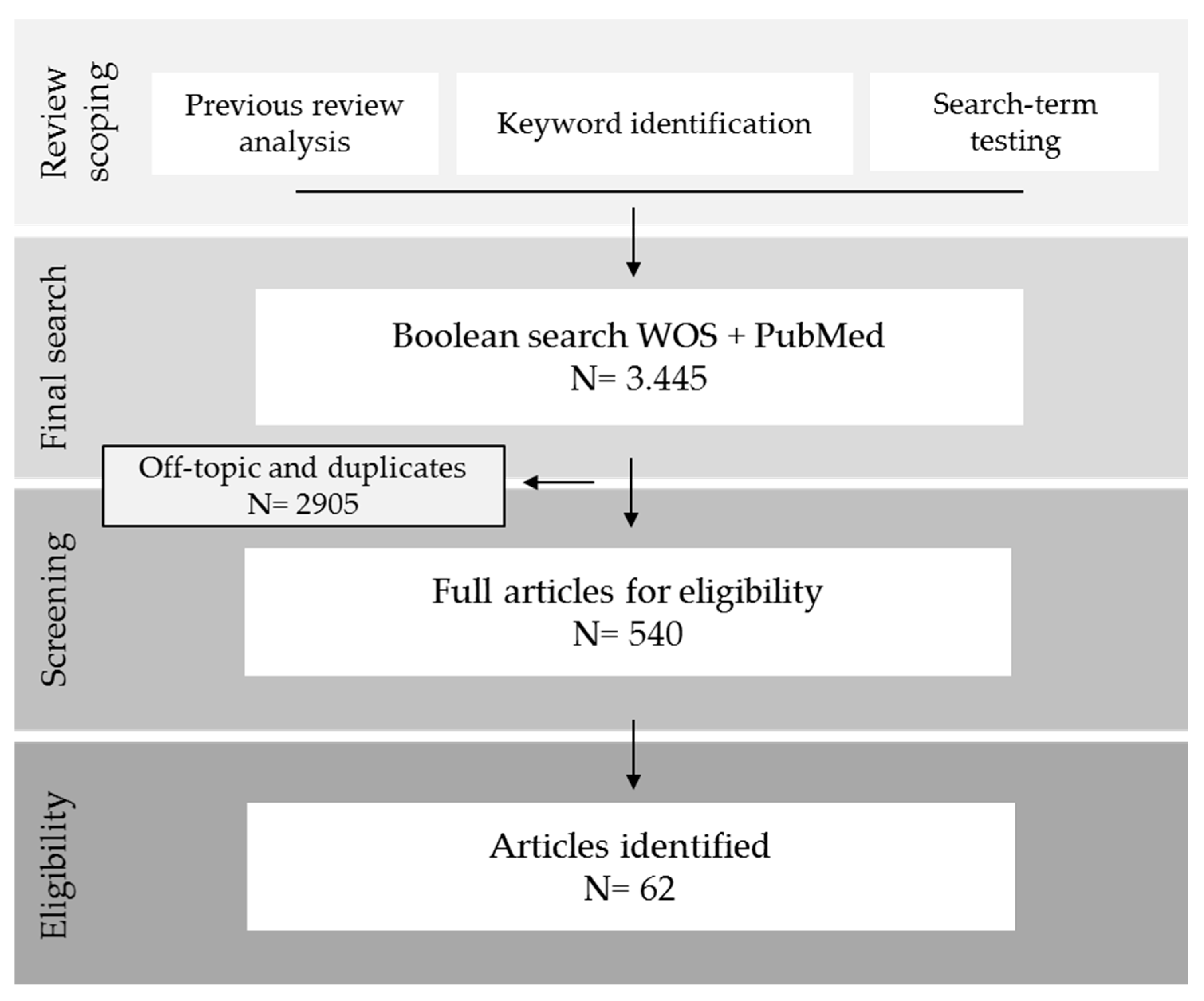
2. Materials and Methods
2.1. Review Scoping
2.2. Searches
2.3. Screening
2.4. Eligibility
- experiments with a real-life exposure to forests;
- experimental studies with humans;
- articles containing quantitative objective measurements of physiological health variables.
2.5. Data Collection
- -
- Article basics: authors, year of publication, title, country where the study was conducted, number of participants and study design. This last item, concerning the methodology used in the study, was further classified into three categories: before-after (B-A) studies, control trials (CTs) (randomized or not) and comparative studies (when different forests or types of groups were compared). This distinction was made to better register the records of health variables for a more comprehensive analysis. Effects before and after forest exposure, between urban and forest environments or even between forest types could thus be compared.
- -
- Exposure characteristics: we suggested the following exposure type classification considering three levels: (a) passive exposure (when participants just stayed in the forest, sitting or viewing the landscape, or passively walked around the forest); (b) active exposure (when participants did any kind of moderate to vigorous-intense physical activity such as running, cycling or any other sport) and (c) pro-active exposure (when the activities and actions conducted could induce mental or physical well-being effects by itself, without necessarily being in the forest, e.g., yoga, meditation). Exposure time was also recorded and ranked in minutes (≤60 min), hours (≤24 h), days (≤365 days) and years (>1 year).
- -
- Forest descriptions: forest information from the articles were gathered and sorted into eight categories: forest type (taken from the species composition or dominance if not explicitly mentioned in the text), abiotic variables measured (e.g., temperature, humidity, light intensity, wind speed), general forest description (referring to any broad information about the forest, such as the surface of the forested area, the conservation status or any geographical information like the altitude), forest species described (tree species composition), forest age, management strategy (any information about the management regime develop in the studied forest), forest variables described (e.g., tree density, biodiversity, BVOCs, vegetation structure, diameter at breast height, basal area) and forest variables measured (if numerical values of the measurements were recorded). All data were gathered into these representative categories of the detail degree of description for a forest ecosystem. We assumed forest type as the broadest description of a forest, and the measurement of a particular forest variable as the most accurate and precise approach for describing a stand.
- -
- Health outcomes: measured health variables were registered for each article. The effects of forests in B-A studies were assessed and classified at four levels: increases (if the value of a variable increased significantly after a visit to the forest), decreases (if the value of a variable decreased significantly after a visit to the forest), non-significant (NS) results after the trial and mixed effects (when changes were significant but increased for some participants while decreased for others). Similarly, the effect of a forest was assessed for CTs and classified as: Higher (if the value of a variable was significantly higher in the forest than the urban group), Lower (if the value of a variable was significantly lower in the forest than the urban group), Non-significant (NS) after the trial and Mixed effects (when changes were significant but were lower for some participants and higher for others). Significant levels were set at p < 0.05. Health variables were not registered if an article did not explicitly present statistical analysis of values before and after exposure or a comparison between the tested environments.
2.6. Data Analysis
3. Results
3.1. General Overview
3.2. Forest Variables
3.3. Health Variables
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Funding
Acknowledgments
Conflicts of Interest
References
- Tsunetsugu, Y.; Park, B.J.; Miyazaki, Y. Trends in research related to “shinrin-yoku” (taking in the forest atmosphere or forest bathing) in Japan. Environ. Health Prev. Med. 2010, 15, 27–37. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Park, B.J.; Tsunetsugu, Y.; Ohira, T.; Kagawa, T.; Miyazaki, Y. Effect of forest bathing on physiological and psychological responses in young Japanese male subjects. Public Health 2011, 125, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Song, C.; Ikei, H.; Miyazaki, Y. Physiological effects of nature therapy: A review of the research in Japan. Int. J. Environ. Res. Public Health 2016, 13, 781. [Google Scholar] [CrossRef] [PubMed]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Kagawa, T.; Miyazaki, Y. The physiological effects of Shinrin-yoku (taking in the forest atmosphere or forest bathing): Evidence from field experiments in 24 forests across Japan. Environ. Health Prev. Med. 2010, 15, 18–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ideno, Y.; Hayashi, K.; Abe, Y.; Ueda, K.; Iso, H.; Noda, M.; Lee, J.-S.; Suzuki, S. Blood pressure-lowering effect of Shinrin-yoku (Forest bathing): A systematic review and meta-analysis. BMC Complement. Altern. Med. 2017, 17, 409. [Google Scholar] [CrossRef] [PubMed]
- Meyer, K.; Bürger-Arndt, R. How forests foster human health–Present state of research-based knowledge (in the field of Forests and Human Health). Int. For. Rev. 2014, 16, 421–446. [Google Scholar] [CrossRef]
- Meyer-Schulz, K.; Bürger-Arndt, R. Les effets de la forêt sur la santé physique et mentale. Une revue de la littérature scientifique. Rev. For. Française 2019, 243, 115–134. [Google Scholar] [CrossRef] [Green Version]
- Antonelli, M.; Barbieri, G.; Donelli, D. Effects of forest bathing (shinrin-yoku) on levels of cortisol as a stress biomarker: A systematic review and meta-analysis. Int. J. Biometeorol. 2019, 63, 1117–1134. [Google Scholar] [CrossRef]
- Hansen, M.M.; Jones, R.; Tocchini, K. Shinrin-yoku (Forest bathing) and nature therapy: A state-of-the-art review. Int. J. Environ. Res. Public Health 2017, 14, 851. [Google Scholar] [CrossRef]
- Morita, E.; Fukuda, S.; Nagano, J.; Hamajima, N.; Yamamoto, H.; Iwai, Y.; Nakashima, T.; Ohira, H.; Shirakawa, T. Psychological effects of forest environments on healthy adults: Shinrin-yoku (forest-air bathing, walking) as a possible method of stress reduction. Public Health 2007, 121, 54–63. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Nakadai, A.; Matsushima, H.; Miyazaki, Y.; Krensky, A.; Kawada, T.; Morimoto, K. Phytoncides (wood essential oils) induce human natural killer cell activity. Immunopharmacol. Immunotoxicol. 2006, 28, 319–333. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Kobayashi, M.; Wakayama, Y.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Shimizu, T.; Kawada, T.; Park, B.J.; et al. Effect of phytoncide from trees on human natural killer cell function. Int. J. Immunopathol. Pharmacol. 2009, 22, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.S.; Lim, Y.R.; Lee, K.; Lee, J.; Lee, J.H.; Lee, I.S. Terpenes from forests and human health. Toxicol. Res. 2017, 33, 97–106. [Google Scholar] [CrossRef]
- Shin, W.S.; Kim, J.; Lim, S.S.; Yoo, R.; Jeong, M.; Park, S. Paradigm shift on forest utilization: Forest service for health promotion in the Republic of Korea. NET J. Agric. Sci. 2017, 5, 53–57. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.; Park, B.J.; Joung, D.; Yeom, D.G.; Koga, S. Healing environments of major tree species in Kyushu University forests: A case study. J. Fac. Agric. Kyushu Univ. 2015, 60, 477–483. [Google Scholar]
- Collaboration for Environmental Evidence. Guidelines for Systematic Review and Evidence Synthesis in Environmental Management. Available online: www.environmentalevidence.org/Documents/Guidelines/Guidelines4.2.pdf (accessed on 5 February 2020).
- Oh, B.; Lee, K.J.; Zaslawski, C.; Yeung, A.; Rosenthal, D.; Larkey, L.; Back, M. Health and well-being benefits of spending time in forests: Systematic review. Environ. Health Prev. Med. 2017, 22, 71. [Google Scholar] [CrossRef]
- Tsunetsugu, Y.; Park, B.-J.; Ishii, H.; Hirano, H.; Kagawa, T.; Miyazaki, Y. Physiological Effects of Shinrin-yoku (Taking in the Atmosphere of the Forest) in an Old-Growth Broadleaf Forest in Yamagata Prefecture, Japan. J. Physiol. Anthropol. 2007, 26, 135–142. [Google Scholar] [CrossRef] [Green Version]
- Joung, D.; Kim, G.; Choi, Y.; Lim, H.; Park, S.; Woo, J.M.; Park, B.J. The prefrontal cortex activity and psychological effects of viewing forest landscapes in Autumn season. Int. J. Environ. Res. Public Health 2015, 12, 7235–7243. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, H.; Song, C.; Ikei, H.; Kagawa, T.; Miyazaki, Y. Analysis of Individual Variations in Autonomic Responses to Urban and Forest Environments. Evid.-Based Complement. Altern. Med. 2015, 2015, 1–7. [Google Scholar] [CrossRef]
- Li, Q.; Morimoto, K.; Nakadai, A.; Inagaki, H.; Katsumata, M.; Shimizu, T.; Hirata, Y.; Hirata, K.; Suzuki, H.; Miyazaki, T.; et al. Forest Bathing Enhances Human Natural Killer Activity and Expression of Anti-Cancer Proteins. Int. J. Immunopathol. Pharmacol. 2007, 20, 3–8. [Google Scholar] [CrossRef]
- Li, Q.; Morimoto, K.; Kobayashi, M.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Shimizu, T.; Li, Y.J.; Wakayama, T.; et al. A forest bathing trip increases human natural killer activity and expression of anti-cancer proteins in female subjects. J. Biol. Regul. Homeost. Agents 2008, 22, 45–55. [Google Scholar]
- Li, Q.; Morimoto, K.I.; Kobayashi, M.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Suzuki, H.; Li, Y.; Wakayama, Y.; et al. Visiting a Forest, but not a City, Increases Human Natural Killer Activity and Expression of Anti-Cancer Proteins cells, and intracellular anti-cancer proteins in lymphocytes. In the present study, we investigated how with a trip to places in a city. Int. J. Immunopathol. Pharmacol. 2008, 21, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Im, S.G.; Choi, H.; Jeon, Y.H.; Song, M.K.; Kim, W.; Woo, J.M. Comparison of effect of two-hour exposure to forest and urban environments on cytokine, anti-oxidant, and stress levels in young adults. Int. J. Environ. Res. Public Health 2016, 13, 625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.J.; Hur, J.; Yang, K.S.; Lee, M.K.; Lee, S.J. Acute Biophysical Responses and Psychological Effects of Different Types of Forests in Patients With Metabolic Syndrome. Environ. Behav. 2018, 50, 298–323. [Google Scholar] [CrossRef]
- Saito, H.; Horiuchi, M.; Takayama, N.; Fujiwara, A. Effects of managed forest versus unmanaged forest on physiological restoration from a stress stimulus, and the relationship with individual traits. J. For. Res. 2019, 24, 77–85. [Google Scholar] [CrossRef]
- Bielinis, E.; Bielinis, L.; Krupińska-Szeluga, S.; Łukowski, A.; Takayama, N. The effects of a short forest recreation program on physiological and psychological relaxation in young polish adults. Forests 2019, 10, 34. [Google Scholar] [CrossRef] [Green Version]
- Yu, C.P.; Lin, C.M.; Tsai, M.J.; Tsai, Y.C.; Chen, C.Y. Effects of short forest bathing program on autonomic nervous system activity and mood states in middle-aged and elderly individuals. Int. J. Environ. Res. Public Health 2017, 14, 897. [Google Scholar] [CrossRef]
- Mao, G.X.; Cao, B.Y.; Yang, Y.; Chen, Z.M.; Dong, J.H.; Chen, S.S.; Wu, Q.; Lyu, X.L.; Jia, B.B.; Yan, J.; et al. Additive benefits of twice forest bathing trips in elderly patients with chronic heart failure. Biomed. Environ. Sci. 2018, 31, 159–162. [Google Scholar]
- Mao, G.; Cao, Y.; Wang, B.; Wang, S.; Chen, Z.; Wang, J.; Xing, W.; Ren, X.; Lv, X.; Dong, J.; et al. The salutary influence of forest bathing on elderly patients with chronic heart failure. Int. J. Environ. Res. Public Health 2017, 14, 368. [Google Scholar] [CrossRef] [Green Version]
- Mao, G.-X.; Cao, Y.-B.; Lan, X.-G.; He, Z.-H.; Chen, Z.-M.; Wang, Y.-Z.; Hu, X.-L.; Lv, Y.-D.; Wang, G.-F.; Yan, J. Therapeutic effect of forest bathing on human hypertension in the elderly. J. Cardiol. 2012, 60, 495–502. [Google Scholar] [CrossRef] [Green Version]
- Wu, Q.; Cao, Y.; Mao, G.; Wang, S.; Fang, Y.; Tong, Q.; Huang, Q.; Wang, B.; Yan, J.; Wang, G. Effects of forest bathing on plasma endothelin-1 in elderly patients with chronic heart failure: Implications for adjunctive therapy. Geriatr. Gerontol. Int. 2017, 17, 2627–2629. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.-W.; Choi, J.-H. The effects of single session forest walking on physiological and psychological state of myocardial infarction patients. J. People Plants Environ. 2019, 22, 109–118. [Google Scholar] [CrossRef]
- Horiuchi, M.; Endo, J.; Takayama, N.; Murase, K.; Nishiyama, N.; Saito, H.; Fujiwara, A. Impact of viewing vs. not viewing a real forest on physiological and psychological responses in the same setting. Int. J. Environ. Res. Public Health 2014, 11, 10883–10901. [Google Scholar] [CrossRef] [Green Version]
- Tsao, T.-M.; Tsai, M.-J.; Hwang, J.-S.; Cheng, W.-F.; Wu, C.-F.; Chou, C.-C.; Su, T.-C. Health effects of a forest environment on natural killer cells in humans: An observational pilot study. Oncotarget 2018, 9, 16501–16511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamaguchi, M.; Deguchi, M.; Miyazaki, Y. The effects of exercise in forest and urban environments on sympathetic nervous activity of normal young adults. J. Int. Med. Res. 2006, 34, 152–159. [Google Scholar] [CrossRef] [PubMed]
- López-Pousa, S.; Bassets Pagès, G.; Monserrat-Vila, S.; de Gracia Blanco, M.; Hidalgo Colomé, J.; Garre-Olmo, J. Sense of well-being in patients with fibromyalgia: Aerobic exercise program in a mature forest—A pilot study. Evid. Based Complement. Altern. Med. 2015, 2015, 614783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolling, A.; Nilsson, H.; Lundell, Y. Stress recovery in forest or handicraft environments—An intervention study. Urban For. Urban Green. 2017, 27, 162–172. [Google Scholar] [CrossRef]
- Sonntag-Öström, E.; Nordin, M.; Lundell, Y.; Dolling, A.; Wiklund, U.; Karlsson, M.; Carlberg, B.; Slunga Järvholm, L. Restorative effects of visits to urban and forest environments in patients with exhaustion disorder. Urban For. Urban Green. 2014, 13, 344–354. [Google Scholar] [CrossRef]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Hirano, H.; Kagawa, T.; Sato, M.; Miyazaki, Y. Physiological effects of Shinrin-yoku (taking in the atmosphere of the forest) using salivary cortisol and cerebral activity as indicators. J. Physiol. Anthropol. 2007, 26, 123–128. [Google Scholar] [CrossRef] [Green Version]
- Sung, J.; Woo, J.M.; Kim, W.; Lim, S.K.; Chung, E.J. The effect of cognitive behavior therapy-based “forest therapy” program on blood pressure, salivary cortisol level, and quality of life in elderly hypertensive patients. Clin. Exp. Hypertens. 2012, 34, 1–7. [Google Scholar] [CrossRef]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Morikawa, T.; Kagawa, T.; Miyazaki, Y. Physiological effects of forest recreation in a young conifer forest in Hinokage Town, Japan. Silva Fenn. 2009, 43, 291–301. [Google Scholar] [CrossRef] [Green Version]
- Sonntag-Öström, E.; Nordin, M.; Dolling, A.; Lundell, Y.; Nilsson, L.; Slunga Järvholm, L. Can rehabilitation in boreal forests help recovery from exhaustion disorder? The randomised clinical trial ForRest. Scand. J. For. Res. 2015, 30, 732–748. [Google Scholar] [CrossRef]
- Song, C.; Ikei, H.; Miyazaki, Y. Sustained effects of a forest therapy program on the blood pressure of office workers. Urban For. Urban Green. 2017, 27, 246–252. [Google Scholar] [CrossRef]
- Jia, B.B.; Yang, Z.X.; Mao, G.X.; Lyu, Y.D.; Wen, X.L.; Xu, W.H.; Lyu, X.L.; Cao, Y.B.; Wang, G.F. Health Effect of Forest Bathing Trip on Elderly Patients with Chronic Obstructive Pulmonary Disease. Biomed. Environ. Sci. 2016, 29, 212–218. [Google Scholar] [PubMed]
- Lee, J.Y.; Lee, D.C. Cardiac and pulmonary benefits of forest walking versus city walking in elderly women: A randomised, controlled, open-label trial. Eur. J. Integr. Med. 2014, 6, 5–11. [Google Scholar] [CrossRef]
- Wang, D.H.; Yamada, A.; Miyanaga, M. Changes in urinary hydrogen peroxide and 8-hydroxy-2′-deoxyguanosine levels after a forest walk: A pilot study. Int. J. Environ. Res. Public Health 2018, 15, 1871. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.T.; Yu, C.P.; Lee, H.Y. The effects of forest bathing on stress recovery: Evidence from middle-aged females of Taiwan. Forests 2018, 8, 403. [Google Scholar] [CrossRef] [Green Version]
- Song, C.; Ikei, H.; Kagawa, T.; Miyazaki, Y. Effects of walking in a forest on young women. Int. J. Environ. Res. Public Health 2019, 16, 229. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Tsunetsugu, Y.; Takayama, N.; Park, B.-J.; Li, Q.; Song, C.; Komatsu, M.; Ikei, H.; Tyrväinen, L.; Kagawa, T.; et al. Influence of forest therapy on cardiovascular relaxation in young adults. Evid.-Based Complement. Altern. Med. 2014, 2014, 1–7. [Google Scholar] [CrossRef]
- Han, J.-W.; Choi, H.; Jeon, Y.-H.; Yoon, C.-H.; Woo, J.-M.; Kim, W. The effects of forest therapy on coping with chronic widespread pain: Physiological and psychological differences between participants in a forest therapy program and a control group. Int. J. Environ. Res. Public Health 2016, 13, 255. [Google Scholar] [CrossRef] [Green Version]
- Hassan, A.; Tao, J.; Li, G.; Jiang, M.; Aii, L.; Zhihui, J.; Zongfang, L.; Qibing, C. Effects of walking in bamboo forest and city environments on brainwave activity in young adults. Evid.-Based Complement. Altern. Med. 2018, 2018, 1–9. [Google Scholar] [CrossRef]
- Lee, J.; Park, B.J.; Tsunetsugu, Y.; Kagawa, T.; Miyazaki, Y. Restorative effects of viewing real forest landscapes, based on a comparison with urban landscapes. Scand. J. For. Res. 2009, 24, 227–234. [Google Scholar] [CrossRef]
- Song, C.; Ikei, H.; Kobayashi, M.; Miura, T.; Li, Q.; Kagawa, T.; Kumeda, S.; Imai, M.; Miyazaki, Y. Effects of viewing forest landscape on middle-aged hypertensive men. Urban For. Urban Green. 2017, 21, 247–252. [Google Scholar] [CrossRef]
- Yu, Y.M.; Lee, Y.J.; Kim, J.Y.; Yoon, S.B.; Shin, C.S. Effects of forest therapy camp on quality of life and stress in postmenopausal women. Forest Sci. Technol. 2016, 12, 125–129. [Google Scholar] [CrossRef]
- Song, C.; Ikei, H.; Kobayashi, M.; Miura, T.; Taue, M.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; Miyazaki, Y. Effect of forest walking on autonomic nervous system activity in middle-aged hypertensive individuals: A pilot study. Int. J. Environ. Res. Public Health 2015, 12, 2687–2699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seo, S.C.; Park, S.J.; Park, C.-W.; Yoon, W.-S.; Choung, J.T.; Yoo, Y. Clinical and immunological effects of a forest trip in children with asthma and atopic dermatitis. Iran. J. Allergy Asthma Immunol. 2015, 14, 28–36. [Google Scholar]
- Mao, G.X.; Lan, X.G.; Cao, Y.B.; Chen, Z.M.; He, Z.H.; LV, Y.D.; Wang, Y.Z.; Hu, X.L.; Wang, G.F.; Yan, J. Effects of short-term forest bathing on human health in a broad-leaved evergreen forest in Zhejiang Province, China. Biomed. Environ. Sci. 2012, 25, 317–324. [Google Scholar]
- Chun, M.H.; Chang, M.C.; Lee, S.J. The effects of forest therapy on depression and anxiety in patients with chronic stroke. Int. J. Neurosci. 2017, 127, 199–203. [Google Scholar] [CrossRef]
- Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; Miyazaki, Y. Physiological and psychological effects of a forest therapy program on middle-aged females. Int. J. Environ. Res. Public Health 2015, 12, 15222–15232. [Google Scholar] [CrossRef] [Green Version]
- Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Takamatsu, A.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; et al. Physiological and psychological effects of forest therapy on middle-aged males with high-normal blood pressure. Int. J. Environ. Res. Public Health 2015, 12, 2532–2542. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Otsuka, T.; Kobayashi, M.; Wakayama, Y.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Li, Y.; Hirata, K.; Shimizu, T.; et al. Acute effects of walking in forest environments on cardiovascular and metabolic parameters. Eur. J. Appl. Physiol. 2011, 111, 2845–2853. [Google Scholar] [CrossRef] [PubMed]
- Stigsdotter, U.K.; Corazon, S.S.; Sidenius, U.; Kristiansen, J.; Grahn, P. It is not all bad for the grey city—A crossover study on physiological and psychological restoration in a forest and an urban environment. Heal. Place 2017, 46, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Ohtsuka, Y.; Yabunaka, N.; Takayama, S. Shinrin-yoku (forest-air bathing and walking) effectively decreases blood glucose levels in diabetic patients. Int. J. Biometeorol. 1998, 41, 125–127. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Otsuka, T.; Kobayashi, M.; Wakayama, Y.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Li, Y.; Hirata, K.; Shimizu, T.; et al. Effects of forest environments on cardiovascular and metabolic parameters. J. Evid.-Based Complement. Altern. Med. 2016, 2016, 1–7. [Google Scholar]
- Bang, K.S.; Lee, I.; Kim, S.; Lim, C.S.; Joh, H.K.; Park, B.J.; Song, M.K. The effects of a campus Forest-Walking program on undergraduate and graduate students’ physical and psychological health. Int. J. Environ. Res. Public Health 2017, 14, 728. [Google Scholar] [CrossRef] [Green Version]
- Park, B.J.; Tsunetsugu, Y.; Ishii, H.; Furuhashi, S.; Hirano, H.; Kagawa, T.; Miyazaki, Y. Physiological effects of Shinrin-yoku (taking in the atmosphere of the forest) in a mixed forest in Shinano Town, Japan. Scand. J. For. Res. 2008, 23, 278–283. [Google Scholar] [CrossRef]
- Ohe, Y.; Ikei, H.; Song, C.; Miyazaki, Y. Evaluating the relaxation effects of emerging forest-therapy tourism: A multidisciplinary approach. Tour. Manag. 2017, 62, 322–334. [Google Scholar] [CrossRef]
- Horiuchi, M.; Endo, J.; Akatsuka, S.; Uno, T.; Hasegawa, T. Influence of forest walking on blood pressure, profile of mood states and stress markers from the viewpoint of aging. J. Aging Gerontol. 2013, 1, 9–17. [Google Scholar] [CrossRef]
- Morita, E.; Imai, M.; Okawa, M.; Miyaura, T.; Miyazaki, S. A before and after comparison of the effects of forest walking on the sleep of a community-based sample of people with sleep complaints. Biopsychosoc. Med. 2011, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Toda, M.; Takeshita, T. The influence of personal patterns of behavior on the physiological effects of woodland walking. Adv. Mind Body Med. 2015, 29, 14–18. [Google Scholar]
- Toda, M.; Den, R.; Hasegawa-Ohira, M.; Morimoto, K. Effects of woodland walking on salivary stress markers cortisol and chromogranin A. Complement. Ther. Med. 2013, 21, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Song, C.; Ikei, H.; Lee, J.; Park, B.-J.; Kagawa, T.; Miyazaki, Y. Individual differences in the physiological effects of forest therapy based on Type A and Type B behavior patterns. J. Physiol. Anthropol. 2013, 32, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horiuchi, M.; Junko, E.; Akatsuka, S.; Hasegawa, T.; Yamamoto, E.; Uno, T.; Kikuchi, S. An effective strategy to reduce blood pressure after forest walking in middle-aged and aged people. J. Phys. Ther. Sci. 2015, 27, 3711–3716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, H.; Song, C.; Ikei, H.; Park, B.J.; Lee, J.; Kagawa, T.; Miyazaki, Y. Population-based study on the effect of a forest environment on salivary cortisol concentration. Int. J. Environ. Res. Public Health 2017, 14, 931. [Google Scholar] [CrossRef] [PubMed]
- Song, C.; Ikei, H.; Miyazaki, Y. Elucidation of a physiological adjustment effect in a forest environment: A pilot study. Int. J. Environ. Res. Public Health 2015, 12, 4247–4255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, B.J.; Jeong, H.; Park, S.; Lee, S. Forest adjuvant anti-cancer therapy to enhance natural cytotoxicity in urban women with breast cancer: A preliminary prospective interventional study. Eur. J. Integr. Med. 2015, 7, 474–478. [Google Scholar] [CrossRef]
- Barnes, M.R.; Donahue, M.L.; Keeler, B.L.; Shorb, C.M.; Mohtadi, T.Z.; Shelby, L.J. Characterizing nature and participant experience in studies of nature exposure for positive mental health: An integrative review. Front. Psychol. 2019, 9, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- An, K.W.; Kim, E.; Jeon, K.S.; Setsu, T. Effects of forest stand density on human’s physiopsychological changes. J. Fac. Agric. Kyushu Univ. 2004, 49, 283–291. [Google Scholar]
- Nazaruk, J.; Borzym-Kluczyk, M. The role of triterpenes in the management of diabetes mellitus and its complications. Phytochem. Rev. 2015, 14, 675–690. [Google Scholar] [CrossRef] [Green Version]
- Gershenzon, J.; Dudareva, N. The function of terpene natural products in the natural world. Nat. Chem. Biol. 2007, 3, 408–414. [Google Scholar] [CrossRef]
- Mewalal, R.; Rai, D.K.; Kainer, D.; Chen, F.; Külheim, C.; Peter, G.F.; Tuskan, G.A. Plant-derived terpenes: A feedstock for specialty biofuels. Trends Biotechnol. 2017, 35, 227–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, D.M.; Gershenzon, J.; Bohlmann, J. Induction of volatile terpene biosynthesis and diurnal emission by methyl jasmonate in foliage of Norway spruce. Plant Physiol. 2003, 132, 1586–1599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.J.; Lu, K.W.; Ma, Y.S.; Tang, N.Y.; Wu, P.P.; Wu, C.C.; Lu, H.F.; Lin, J.G.; Chung, J.G. Alpha-phellandrene, a natural active monoterpene, influences a murine WEHI-3 leukemia model in vivo by enhancing macrophague phagocytosis and natural killer cell activity. In Vivo 2014, 28, 583–588. [Google Scholar] [PubMed]
- Komori, T.; Fujiwara, R.; Tanida, M.; Nomura, J.; Yokoyama, M.M. Effects of citrus fragrance on immune function and depressive states. Neuroimmunomodulation 1995, 2, 174–180. [Google Scholar] [CrossRef]
- Nam, E.-S.; Uhm, D.-C. Effects of Phytoncides Inhalation on Serum Cortisol Level and Life Stress of College Students. Korean J. Adult Nurs. 2008, 20, 697–706. [Google Scholar]
- Sumitomo, K.; Akutsu, H.; Fukuyama, S.; Minoshima, A.; Kukita, S.; Yamamura, Y.; Sato, Y.; Hayasaka, T.; Osanai, S.; Funakoshi, H.; et al. Conifer-derived monoterpenes and forest walking. Mass Spectrom. 2015, 4, A0042. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Reference | (−) Detail of Description (+) | |||||||
|---|---|---|---|---|---|---|---|---|
| Forest Type | Abiotic Variables | Forest Description | Forest Species | Forest Age | Manag. Strategy | Forest Var. Described | Forest Var. Measured | |
| [26] | * | * | * | * | * | * | * | * |
| [25] | * | * | * | * | * | * | * | |
| [27] | * | * | * | * | * | * | * | |
| [28] | * | * | * | * | * | * | * | |
| [29] | * | * | * | * | * | * | ||
| [30] | * | * | * | * | * | * | ||
| [31] | * | * | * | * | * | * | ||
| [32] | * | * | * | * | * | * | ||
| [33] | * | * | * | * | * | * | ||
| [34] | * | * | * | * | * | |||
| [22] | * | * | * | * | * | |||
| [35] | * | * | * | * | * | |||
| [24] | * | * | * | * | ||||
| [36] | * | * | * | |||||
| [23] | * | * | * | * | ||||
| [21] | * | * | * | |||||
| [37] | * | * | * | * | * | * | ||
| [38] | * | * | * | * | ||||
| [39] | * | * | * | * | * | |||
| [18] | * | * | * | * | ||||
| [40] | * | * | * | * | ||||
| [41] | * | * | * | * | ||||
| [42] | * | * | ||||||
| [43] | * | * | * | * | ||||
| [44] | * | * | * | * | ||||
| [45] | * | * | * | * | ||||
| [46] | * | * | * | * | ||||
| [47] | * | * | * | * | ||||
| [48] | * | * | * | * | ||||
| [49] | * | * | * | * | ||||
| [50] | * | * | * | |||||
| [51] | * | * | * | |||||
| [52] | * | * | ||||||
| [53] | * | * | * | |||||
| [54] | * | * | * | |||||
| [55] | * | * | * | |||||
| [56] | * | * | ||||||
| [57] | * | * | * | |||||
| [58] | * | * | ||||||
| [59] | * | * | ||||||
| [60] | * | * | ||||||
| [61] | * | * | ||||||
| [62] | * | * | ||||||
| [63] | * | |||||||
| [64] | * | |||||||
| [4] | * | |||||||
| [65] | * | |||||||
| [66] | * | |||||||
| [2] | * | |||||||
| [67] | * | |||||||
| [68] | ||||||||
| [69] | ||||||||
| [19] | ||||||||
| [70] | ||||||||
| [71] | ||||||||
| [72] | ||||||||
| [73] | ||||||||
| [74] | ||||||||
| [75] | ||||||||
| [20] | ||||||||
| [76] | ||||||||
| [77] | ||||||||
| A | Forest Type | Effect on Diastolic Blood Pressure (DBP) | ||||
| Decrease | NS | Increase | Mixed Effects | Total | ||
| Broad-leaved | - | 1 | - | 1 | 2 | |
| Coniferous | 1 | - | - | - | 1 | |
| Bamboo | 1 | - | - | - | 1 | |
| Mixed | 3 | 6 | - | - | 9 | |
| Total | 5 | 7 | - | 1 | 13 | |
| B | Effect on Systolic Blood Pressure (SBP) | |||||
| Decrease | NS | Increase | Mixed effects | Total | ||
| Broad-leaved | - | 2 | - | - | 2 | |
| Coniferous | 1 | - | - | - | 1 | |
| Bamboo | 1 | - | - | - | 1 | |
| Mixed | 6 | 2 | 1 | - | 9 | |
| Total | 8 | 4 | 1 | - | 13 | |
| A | Forest Type | Effect on Diastolic Blood Pressure (DBP) | ||||
| Lower | NS | Higher | Mixed Effects | Total | ||
| Broad-leaved | 1 | 1 | - | 1 | 3 | |
| Coniferous | 3 | - | - | - | 3 | |
| Bamboo | 1 | - | - | - | 1 | |
| Mixed | 1 | 5 | - | - | 6 | |
| Total | 6 | 6 | - | 1 | 13 | |
| B | Effect on Systolic Blood Pressure (SBP) | |||||
| Lower | NS | Higher | Mixed effects | Total | ||
| Broad-leaved | 1 | 1 | - | 1 | 3 | |
| Coniferous | 1 | 1 | - | - | 2 | |
| Bamboo | - | 1 | - | - | 1 | |
| Mixed | - | 6 | - | - | 6 | |
| Total | 2 | 9 | - | 1 | 12 | |
| A | Forest Type | Effect on Pulse Rate | ||||
| Decrease | NS | Increase | Mixed Effects | Total | ||
| Broad-leaved | - | - | - | 1 | 1 | |
| Mixed | 2 | 3 | 1 | - | 6 | |
| Total | 2 | 3 | 1 | 1 | 7 | |
| B | Lower | NS | Higher | Mixed effects | Total | |
| Broad-leaved | 1 | 1 | - | - | 2 | |
| Coniferous | 1 | - | - | - | 1 | |
| Mixed | 3 | - | - | - | 3 | |
| Total | 5 | 1 | - | - | 6 | |
| A | Forest Type | Effect on Cortisol Levels | ||||
| Decrease | NS | Increase | Mixed Effects | Total | ||
| Broad-leaved | - | 2 | - | - | 2 | |
| Mixed | 2 | - | - | - | 2 | |
| Total | 2 | 2 | - | - | 4 | |
| B | Lower | NS | Higher | Mixed effects | Total | |
| Broad-leaved | 4 | 1 | - | - | 5 | |
| Mixed | 3 | - | - | - | 3 | |
| Total | 7 | 1 | - | - | 8 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bach Pagès, A.; Peñuelas, J.; Clarà, J.; Llusià, J.; Campillo i López, F.; Maneja, R. How Should Forests Be Characterized in Regard to Human Health? Evidence from Existing Literature. Int. J. Environ. Res. Public Health 2020, 17, 1027. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17031027
Bach Pagès A, Peñuelas J, Clarà J, Llusià J, Campillo i López F, Maneja R. How Should Forests Be Characterized in Regard to Human Health? Evidence from Existing Literature. International Journal of Environmental Research and Public Health. 2020; 17(3):1027. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17031027
Chicago/Turabian StyleBach Pagès, Albert, Josep Peñuelas, Jana Clarà, Joan Llusià, Ferran Campillo i López, and Roser Maneja. 2020. "How Should Forests Be Characterized in Regard to Human Health? Evidence from Existing Literature" International Journal of Environmental Research and Public Health 17, no. 3: 1027. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17031027